Continuum Biomechanics of Soft Tissue: Successes and Challenges

1
Integrated tissue biology, biomechanics
and digital diagnosis for non-surgical treatment
Kee-Joon Lee, DDS, PhD
Department of Orthodontics,
Yonsei University College of Dentistry
Envelop of discrepancy
Orthognathic surgery is indicated for severe skeletal discrepancy beyond the limit of orthodontic camouflage in a non-growing patient (Proffit, Contemporary orthodontcs)

2
Class III Mn prognathism Q) Can we move mandible
‘backward’ without surgery?
We know it is impossible,
but…
Surgery? (22Y F)
Clue 2-1) Upper ant. axis affects posterior occlusion
Ideal
OB/OJ

3
Clue 2-2) Lower ant. axis affects posterior occlusion
Ideal
OB/OJ
Clue) incisor axes affect posterior occlusion
Translation Valladares et al. 2014
Lingual tipping
2D VTO: Class II/III compensation
Class II compensation
U1: Translation~root movement
L1: Intrusion+ controlled tipping
(no flaring!!!)
6/6: Anchor loss or distalization
Class III compensation
U1: Minor retraction
L1: Translation~root movement
U6: anchor loss?
L6: Distalization?
Occlusal
Plane

4
Clue 1. Soft
tissue
Understanding the soft tissue…
•1. The thicker, the dumber (refractory)
•Lower lip>Upper lip>Buccal cheek
•2. Facial change after camouflage?
•Class III > Class II > Asymmetry
•2. DDX between rest & active
•(1) Midline at rest & action (philtrum deviation)
•(2) Nasolabial fold at rest & action
• Hypothesis – bodily movement may induce more dramatic soft tissue change esp in the lower lip?

5
Clue 2. Mechanics
Summary: appliance construction (modified shape-
driven approach) Angle Orthod 2014
Kee’s protocol Bodily retraction
• Miniscrew (low buccal), long hook
• Anterior torque (++)
• Moderate retraction force (150-200g) renewal 4-6wks
Indication
Incisor axis normal
Incisor exposure normal
Incompetency (+-)

6
Clue 3. Biology
Young 3D Young 7D Young 14D
force
Adult 7D Adult 14D
Skerry et al. J. Bone Miner. Res 1989;4:783-788. Klein-Nulend et al. FASEB J;1995:441-445. Cowin et al. J of Biomech Eng ;1991:191-197
Summary)
1. Bone formation on the lateral surface may precede bone resorption
on the ‘pressure’ side PDL
2. Coronal/middle 1/3 bone response may differ from apical 1/3 region
3. Bone formation via ‘light force technology’ may be realistic in young
patients, but not in adults.

7
Clue 4. Airway & function

8
Class II Mn retrognathism Q) Can we move mandible
‘forward’ without surgery?
We know it is impossible,
but…
Comparison 2017-10-16
Incompetency exaggerates protrusive profile / Mn retrusion
Ob Oris: Lip pursing
Mentalis: Chin flattening
Zmi LLS
LLSAN

9
Q) Vertical control of maxilla via total
arch intrusion?
Vertical closure Restriction
of suture growth
Dentoalveolar intrusion
Predictability Poor Good
(WITH MINISCREW)
Stability Questioned Relatively stable?
Dermaut et al. Eur J Orthod 1992 “Orthopedic effect on the maxilla could not be established.”
Orton et al. Eur J Orthod 1992 “Maxiallry restraint -No significant change in the anterior facial
height.”
Sugawara et al.Int J Adult Orthod Orthognat Surg 2002 “SAS would be a valid modality to
intrude mandibular molars”
Cr
Cr
Single miniscrew
Dual miniscrews
Cres of
Mx. dentition
Distalization and rotation
Vertical reduction (-)
Distalization and intrusion
Vertical reduction (+) (p<0.05)
2.41mm
1.56mm
1.29mm 0.49 mm
2.91mm
1.40mm
1.83mm
0.84mm
Q) Effect of
dual miniscrews
on vertical
dimension (in
non-ext model)?
• Vertical angle up to 45dgr: minimal buccal tipping of molars (no palatal miniscrew)
• Vertical angle > 45dgr: significant buccal tipping of molars (+ palatal miniscrew)
• Rotation is related to the relative position of force vector

10
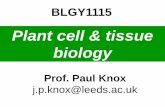
Cres of total arch??
Figure 7. Positions of the centers of resistance. A, The center of resistance of the 4 mandibular anterior
teeth; B, the center of resistance of the 6 mandibular anterior teeth; C, the center of resistance of the
complete mandibular dentition.
Korean J Orthod. 2017 Jan;47(1):21-30
Finite-element analysis of the center of resistance of the mandibular dentition
A-Ra Jo, Sung-Seo Mo, Kee-Joon Lee, Sang-Jin Sung, and Youn-Sic Chun
Gwang-Mo Jeong, Sang-Jin Sung, Kee-Joon Lee, Youn-Sic Chun, Sung-Seo Mo. Kor J Orthod 2009:39;83-94
Cres of total arch??
Force system for total arch intrusion
1. Vertical vector should be set close to the Cres of total arch.
2. Bimaxillary force vectors and/or dual miniscrews may be reliable.
3. Torque-on-the-wire for incisor control (10dgr)
?
?
?

11
Hypothesis: for ‘pure vertical’ discrepancy!!!!!!!!!!
• 3D total intrusion reduction AFH reduction
incompetency
• 2-3mm TAI (Max) + 1-2mm TAI (Man) (+ lip ‘draping’)
= 3-5 mm correction only?
• What if normal soft tissue growth is combined???
• TAI in grower (fast and effective TAI)???????????
Superimposition(Initial / Deb / fu) 12-14Y M
Autorotation during growth peak???
ANB 1.3 -0.7 -1.0
MP angle 34.030.3 25.8
AFH 130.1 127.7 128
Superimposition
Mn ‘advancement growth’ 8mm

12
AFH 2mm increased
MP angle 1dgr reduced
Suggestion: 4D Semi-early treatment
• Gray area between growth spurt and growth cessation!!!
• Middle school active orthodontics for vertical issue
Advantage of early correction? KJ’s suggestion
• … Based on soft tissue paradigm…
Category Author Conclusion KJ’s suggestion
Biological rationale D Carlson Suggestion of gene-based approach
Alveolar movement for skeletal change
Tx timing and outcome H Pancherz Negative Positive via 4D concepts (Less non-invasive tx)
Class II WR Proffit JFC Tulloch
Negative Positive via 4D total arch intrusion
Skeletal open bite (high angle)
JD English Inconclusive Positive via 4D total arch intrusion
Open bite PA Shapiro Yes but not stable Positive via 4D intrusion
Impacted incisors A Becker Active orthodontics>waiting
4D Yonsei guided eruption

13
Transverse correction for asymmetry
Transverse problem
Camouflage
CR CR
CR CR
U-L CRe difference = -8.7 Req Exp. = +7.5
X +1.0 55.5
Surgery
46.8
54.5
Δ IMW @Cres= -7.5 Req Exp. = +6.5mm
T/S 21 T/S 40 Initial
2M

14
what to extract?
#44 Extraction #47 or #48 Extraction
Initial
Debond
Shift from surgery non-surgery
Initial Debond

15
2018-04-11 2018-02-22
CBCT comparison
CBCT comparison;
frontonasal disjunction!!!

16
*What leads to surgery :
- TVL to Pog’+++ (average to low angle, ‘no rotation’)
- Insufficient ‘U zone’
*For successful camouflage
- Elimination of incompetency
- U1 translation>>tipping
- Total intrusion
- ‘More than’ A type anchorage
*For successful surgery
- Elimination of perinasal depression
- adequate jaw(esp Mx) rotation
- maximum decompensation
In Class II…
*What leads to surgery
- TVL to Pog’ +++
-L1 linguoversion
*What leads to camouflage
- IMPA relatively high
- chin+lower lip protrusion
*For successful surgery
- IMPA << L1 to Facial plane/TVL
- Variation in U1 consideration: MARPE
In Class III…

17
Summary : KJ protocol for Class III / asymmetry
•1. Early transverse correction to secure perm teeth eruption - MARPE>> RPE
•2. Minimum/moderate protraction (avoid creation of incompetency!!!)
•- Low angle: RPE, High angle: MARPE
•3. Growth observation / maintenance of transverse
-re-RPE if indicated
-Please, do not ext L4!!!
•4. Phase II: Early phase II in case of high angle / incompetency
-OGS if not camouflageable (pt’s perception)
-Non surgery via Total arch intrusion (in case of incompetency)
-Non surgery via ext L4 & L1 translation (in case of A-P problem+minor protrusion)
Thanks for your
attention!!!
Acknowledgement
Pf. YJ Choi
Dr. CB Park
Dr. JH Chun
Dr. HK Hong
Dr. Amanda Cunha