Integrated TB-HIV care from a - KNCV Tuberculosefonds · TB and HIV • WORLDWIDE – 35 500 000...
30
Reinout van Crevel Radboud umc, Netherlands [email protected] Integrated TB-HIV care from a clinician’s perspective
Transcript of Integrated TB-HIV care from a - KNCV Tuberculosefonds · TB and HIV • WORLDWIDE – 35 500 000...

Reinout van CrevelRadboud umc, Netherlands
Integrated TB-HIV care from a clinician’s perspective

My perspective
Academic clinician• Internist - infectious disease specialist• responsible for HIV in my hospital (660 pts)• 1 of 2 TB coordinators in my hospital• University lecturer
Researcher• ‘Global Health and Infectious Diseases’• TB (mostly in Indonesia, Romania)
– TB-diabetes; TB meningitis; MDR/WGS; LTBI and transmission – basic sciences (immunology, ‘omics’) and clinical-operational research
• HIV (<< than TB)– Quality of HIV care in Netherlands and Indonesia

TB and HIV• WORLDWIDE
– 35 500 000 people infected with HIV
– 13% co-infected with TB
– 1 600 000 died in 2012 (4.5%)
– 25% of AIDS deaths are TB related
• EUROPE (2014)
– 33.000 TB, 65% HIV tested, 5% positive
– 78% new HIV, 22% known
– 42% IDU
– More MDR-XDR (RR 2-3)
– Less treatment success (58% vs 84%)
vd Werf, AIDS, 2016

HIV epidemic is changing (especially in W-Europe)
• Becoming a chronic disease
• Higher CD4 at time of diagnosis
• Very effective treatment, (very) few deaths
• More non-communicable co-morbidity
• HIV-prevention is not keeping up
• Therefore: focus on detection and treatment of early HIV (to reduce transmission and incidence)

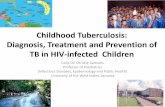
TB in HIV: presentation dependent on CD4
CD
4+
T-ce
lls
1000
800
600
400
200
0years
(classical) Pulmonary TB
Non-cavitary PTB; extrapulmonary TB,
Disseminated TB

Difficult diagnosis
– Dutch man, frequent travel to Asia
– Chronic non-responsive pneumonia
– Referred to pulmonologist
– Broncho-alveolar lavage: M. tuberculosis
– Tested for HIV: positive
– Referred to HIV physician: CD4 160 cells
All TB patients should be tested for HIV!

27 year old South African musician
• Visiting the Netherlands
• Sent to hospital with cough
• At emergency room: mouth mask
• 3 hours later. Xpert TB: positive
• Rifampicin resistant: MDR-TB
• Newly diagnosed HIV; CD4 140
Besides HIV-testing: infection prevention and rapid drug-resistance testing!

Combined treatment

RT
Provirus
ProteinsRNA
RNA
RT
Protease
Inhibitors
(n=10) *
Reverse
transcriptase
Inhibitors
(n=8+4) *RNA
RNA
DNA
DNA
DNA
Anti-retroviral treatment (ART) for HIV
Integrase
Inhibitors
(n=3) *
Entry blockers
(n=2) *
Reversetranscriptase
integrase
protease
* Available in the Netherlands

Treatment of TB - HIV
• Toxicity
• Resistance
• Interactions
• IRIS
• Timing ART in new HIV

Our Dutch patient
– 4 weeks after TB treatment (HRZE), start of ART
– Combination treatment: combivir, Efavirenz
– First: aggression, mood swings. Efavirenz?
– Then: anemia. Zidovudine?
– Then: decreased kidney function: tenofovir?
– Then: severe hypersensitivity reaction: abacavir!
– …
Drug-toxicity can be a big problem limitingtreatment options

12
Toxicity to HIV medication
Toxic epidermic necrolysis(TEN)
= severe Stevens-Johnson
With permission

TB-HIV; more and overlapping toxicity
TB-medication HIV-medication
hepatotoxicity INH, PZA, Rifampin Nevirapine (NVP), efavirenz(EFV), all protease inhibitors (PIs)
Skin rash INH, PZA, Rifampin NVP, EFV, abacavir, .. all others
Leukopenia, anemia Rifampin zidovudin
Neuropathy INH Nucleoside reverse transcriptase inhibitors (NRTIs)
Artralgia, myopathy PZA, rifabutin Tenofovir, integrase-remmers
fever INH, rifampicine Abacavir, …
More drug-toxicity in HIV, especially with low CD4

Interactionsrifampicin
HIV patients often on other co-medication

refugees – sometimes difficult coordination
– TB spondylitis, HIV (120 CD4 cells), hepatitis B
– first TB treatment HRZE
–2 mths later: ART (truvada, efavirenz)
–HIV-genotyping: EFV resistance
– Efavirenz replaced by lopinavir/ritonavir
–Rifampicine to rifabutin (300 mg / day), because rifabutin has fewer interactions
–Moved by Dutch immigration service

7 weeks later (another hospital)
– Severe polyarthralgia, nausea
– Leukopenia, thrombocytopenia
– fever
– Painful eye
– Vision loss
Rifabutin toxicity due to interaction with ritonavir!
Combined treatment more challenging when multiple doctors involved
Slit lamp:Hypopyonuveitis.

Combining HIV drugs with TB drugs
• Rifampicin* + double dose dolutegravir
• Rifampicin + efavirenz
• If protease inhibitors are needed: rifabutin
Avoid:
• Rifampicin + Protease inhibitors, etravirine, elvitegravir/cobistat, NVP, rilpivirine, TAF
* As part of standard TB treatment

Other drug-interactions
• Bedaquiline– 50% lower with efavirenz,
– 25% higher with protease inhibitors
• Delamanid; probably no interactions with rifamp
• Other co-medication– with rifampicin
– With HIV drugs (protease inhibitors, efavirenz, nevirapine, dolutegravir, …)

Paradoxical worsening
• Our African musician
• Recent abdominal TB
• Now pulmonary TB (MDR)
• CD4 140, ART (Atripla) 5 wk na start TB
• 2 weeks later: fever and ileus
• ultrasound: necrotising abdominal lymphnodes

“immuun reconstitutie inflammatory syndrome“ (IRIS)
What else can cause fever in such a patient?
drug fever, other infections, lymphoma etc


Our African patient.. more complications
• ileus (due to enlarged lymphnodes)• IRIS: prednisone 3 months• Good response to ART, HIV-RNA < after 3 mths, CD4 up• Nephrotic syndrome, renal failure• Severe hepatotoxicity• Transfusions: severe hemolytic anemia and trombocytopenia• Switches /interruptions TB treatment..• Hospitalised throughout this course in TB sanatorium
• seizure 3,5 mths after start of cART

3 months later: Seizure -IRIS again

Risk factors IRIS
• low CD4, rapid rise after start ART
• Short interval between start TB drugs and ART
• Extrapulmonary (disseminated) TB
• High load M. tuberculosis
• for TB meningitis: more if culture-positive or more neutrophils in cerebrospinal fluid
Lai – Eur J Imm 2013; Marais – Clin Inf Dis 2014

Quick start of ART ~ more IRIS
0
10
20
30
40
50
60
70
80
90
< 1 mnd 1-2 mnd 2-3 mnd 3-4 mnd > 4 mnd
% m
et T
B-I
RIS
Time between start TB-therapy and start ART
Meintjes G, Lancet ID 2008
N=162 ART-naïeve patients South Africa;
CD4 < 100

Timing ART after start of TB
– Balance risk of IRIS with risk of progression of HIV (deathdue to other infections)
– Many trials compared early and late ART after TB therapy
– Overall: no benefit from starting early, except for CD4<50
– My take on this: • screen aggressively for other infections
(cryptococcal meningitis, CMV retinitis)
• Delay ART to 4-8 weeks after start of TB treatment, depending on TB severity, TB treatment response, toxicity etc

Two kinds of TB-IRIS
TB treatment
ART
ART
Clinical worsening TB becauseof immune reconstitution = paradoxical IRIS
Increased inflammation tosubclinical TB because of immune reconstitution = ‘unmasking’ IRIS
Active TB
No sign of TB before
ART

Unmasking IRIS can help TB diagnosis
– Jamaican man, 28 years
– Known HIV, treated in Jamaica
– 2 years ART; treatment interruptions
– No symptoms, 80 CD4 cells
– Resistant virus. Start 2nd line ART
– 3 weeks later:
– Fluctuating cervical mass
– AFB and Xpert-positive (MDR..)
– TB-lymphadenitis

TB/LTBI - guideline for HIV physicians Netherlands
• Have a low threshold for screening for active TB, – especially with low CD4 and in individuals from medium/high TB incidence
– Also in the first months after start of ART (‘unmasking TB’)
• Do not screen for LTBI in Dutch / people from low-endemic settings, unless they have had obvious TB exposure (eg having lived in Africa)
• Screen individuals from medium / high TB incidence settings and others with significant TB exposure for LTBI (using IGRA and/or TST), and provide IPT for those positive
• Consider empiric TB-prophylaxis or repeating screening if significant risk of LTBI (eg sub-Saharan Africa) and CD4s < 200

Integrated management & service delivery
• Multidiciplinary (HIV, TB, lab, municipal health service..)
• known HIV - coordination by HIV physician with advise from TB phsyician
• TB diagnosed first – coordination first with TB physician, gradual transfer to HIV care
• HIV care centralised
• HIV-TB care centralised in TB low-endemic settings
• Situation different in W-Europe and E-Europe (for HIV and TB)• Trans-European partnerships?• Registration? Like Dutch HIV monitoring?