Integrated Framework for Reducing Racial and Ethnic Disparities in the Quality of Health Care...
21
Integrated Framework for Reducing Racial and Ethnic Disparities in the Quality of Health Care Marshall H. Chin, MD, MPH, and Don Goldmann, MD University of Chicago, Institute for Healthcare Improvement
-
Upload
ralph-norton -
Category
Documents
-
view
224 -
download
0
Transcript of Integrated Framework for Reducing Racial and Ethnic Disparities in the Quality of Health Care...

Integrated Framework for Reducing Racial and Ethnic Disparities in the Quality of
Health Care
Marshall H. Chin, MD, MPH, and Don Goldmann, MD
University of Chicago, Institute for Healthcare Improvement

Roadmap
Context and problems in current efforts to reduce disparities in health care quality
Conceptual models for reducing disparities
Evidence on disparity interventions
6 key components for reducing disparities
Implications for funders
Exercise: Advice to AHRQ

Promising Time
Increased public awareness of disparities
Health reform legislation will increase collection of race, ethnicity, and language data
Increased motivation for providers and health care organizations to address disparities
An opportunity to move from description and complaint to action

Problems and Gaps
Lots of research on the magnitude of disparities, but relatively little work on interventions to reduce disparities
Many providers, organizations, and policy makers do not know where to start to reduce disparities
Despite language encouraging proposals on vulnerable populations, many public and private funders receive few applications

Models, Models, Models
Models can inform approaches to disparities, but….
Models must be customized to address the unique underlying causes of disparities directly, but….
Customized solutions are sparse, therefore….
The nation’s research agenda must be directed at testing interventions that address disparities specifically

Level of Engagement Model• Patient/Person• Provider• Microsystem - small unit of care delivery• Organizations that house or support
microsystems• Communities and regions that span care
delivery, prevention, and health promotion for populations
• Environment of policy, payment, regulation, accreditation
Based on Berwick, Health Affairs 2002;21:n. 3

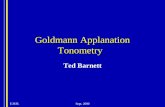
Informed,ActivatedPatient
ProductiveInteractions
Prepared,ProactivePractice Team
Functional and Clinical Outcomes
DeliverySystemDesign
Decision Support
ClinicalInformation
Systems
Self-Management
Support
Health System
Resources and Policies
Community
Organization of Health Care
Wagner
Planned Care Conceptual Model

Finding Answers: Disparities Research for Change
www.SolvingDisparities.org
New IOM Framework
Crosscutting
Dimensions
EQUITY
VALUE
Components of Quality Care
Type of Care
Chronic condition management
Acute
Treatment
Preventive
Care
Effectiveness
Safety
Timeliness
Patient/family-centeredness
Care Coordination
Health Systems Infrastructure Capabilities
Access
Efficiency
Crosscutting
Dimensions
EQUITY
VALUE
Components of Quality Care
Type of Care
Chronic condition management
Acute
Treatment
Preventive
Care
Effectiveness
Safety
Timeliness
Patient/family-centeredness
Care Coordination
Health Systems Infrastructure Capabilities
Access
Efficiency

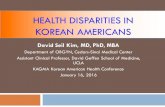
RWJF Finding AnswersConceptual Model
Chin et al. Med Care Res Rev 2007; 64:7S-28S
Provider
Patient
Policy / Payment / Regulation / Accreditation
Health CareOrganization
Person
Community
Process
Outcomes
Access

Systematic Reviews
Reviewed 200+ articles
Condition-specific Cardiovascular disease
Diabetes
Depression
Breast cancer
Cross-cuttingCultural leverage
Pay-for-performance incentives
FAIR Database

Common Successful Interventions from Systematic Reviews
Multifactorial interventions that address multiple leverage points along a patient’s pathway of care
Culturally tailored QI more than generic QI
Nurse-led interventions with multidisciplinary teams and close tracking and monitoring of patients
Chin MH, et al. Med Care Res Rev 2007; 64:7S-28S.

Review of Pediatric Literature (Asthma, Immunizations)
Measure and improve structural aspects of care experience that impact outcomes
Incorporate families into interventions
Integrate non-health care partners into QI interventions
Chin MH, et al. Pediatrics 2009;124 (Suppl 3):S224-S236.

Lessons from RWJF Finding Answers: Disparities
Research for Change Grantees
Knowledge/attitude interventions helpful but not sufficient
Providing disparity data helpful but not sufficient
Context and tailoring are critical
Multifactorial, multitarget interventions
Intervention & the process of implementation
Buy-in, incentives, sustainability, system

Integral Components of Systems Approach to Reducing Disparities
1) Examine your performance data stratified by insurance status, race/ethnicity, language, and socioeconomic status.
2) Get training for your staff to work effectively with diverse populations.
3) Make reduction of inequities in care for vulnerable populations an integral component of quality improvement efforts.
Chin MH. Ann Intern Med 2008; 149:206-208.

Systems Approach - 2
4) Provide models of care and infrastructural support to enable organizations to improve the quality of care for vulnerable patients.
5) Align incentives to reward providers and health care organizations for providing high quality care to vulnerable populations.
6) Allocate more resources for the uninsured with chronic diseases.

Implications for FundersMove beyond asking applicants simply to show that they have included “priority populations” in their research plan
Ask all quality of care applicants to address specifically how they will reduce known disparities or gaps discovered in the course of the work– Include a measurement plan that stratifies data
appropriately
Design an overall portfolio of grants and grantees that addresses improving outcomes and reducing gaps in diverse populations and settings
Reward applicants who address equity issues

Spheres of Influence for Disparity Interventions
Patient/person
Provider
Microsystem
Health care delivery organization
Community and region
Policy, payment, regulation, accreditation
Which spheres are you addressing or plan to address in your comprehensive, multifactorial approach to reducing an equity gap ?

Example - Care Coordination for Chronically Ill Patients
Patient: engagement, empowerment, mobilization
Provider: engagement, training in health literacy and cultural competency
Microsystem: teamwork, communication, QI, practice redesign, stratified data and real time feedback

Care Coordination for Chronically Ill Patients - 2
Health care delivery organization: communication, coordination, support for patients and families across the continuum, tele-health and monitoring, focus on value and longer term fiscal horizon
Community: activation, mobilization of non-medical resources and supports, attention to social capital and environment
Policy – alignment of incentives and payment to promote the above actions

Exercise: Advice to AHRQ
Request For Applications– Think of your research area– Pick one of the 6 spheres of influence– Write a research question you’d like to be a priority
area for the RFA for your research area in that sphere of influence
– If time, write questions for other spheres
To reduce disparities in health care quality, what else might AHRQ do, in addition to directing and supporting research on specific topics?

Spheres of Influence for Disparity Interventions
Patient/person
Provider
Microsystem
Health care delivery organization
Community and region
Policy, payment, regulation, accreditation