Insulin response in bulimia nervosa as a marker of nutritional depletion
8
Insulin Response in Bulimia Nervosa as a Marker of Nutritional Depletion Janice Russell Michael Hooper Glenn Hunt (Accepted 29 August 1995) Objective: The aim of this provocation study was to examine insulin, glucose, and cortisol levels in response to a glucose load in bulimia nervosa patients and to relate this to behavior, treatment status, and depressive symptomatology. Method: A 3-hr glucose tolerance test was performed in 15 female patients and in 4 controls. Tests were performed at different stages of treatment and following documented engagement in the patient’s usual or previous reper- toire of bulimic behaviors in the 24 hr prior to testing. Insulin, glucose, and cortisol levels were assayed at baseline and at 30-min intervals following the glucose load. Presence or absence of significant depressive symptomatology was ascertained. Results: Three patterns of insulin response were identified: (1) an exaggerated response, (2) a normative response which resembled that of healthy controls, and (3) a blunted pattern. A reciprocal relationship between peak insulin and mean cortisol levels was seen with higher depression scores associated with blunted insulin response. Patients whose response was exaggerated binged and vomited relatively infrequently and were of stable weight. The insulin response of success- fully treated patients, abstinent from binging and vomiting for 4 weeks, was similar to that of normal controls. A blunted response occurred in patients who binged and vomited more frequently, whose weight was unstable, and whose baseline eating was chaotic or nonexistent. Discussion: The exaggerated insulin response was seen as a physiological adaptation to intermittent starvation reversible with treatment, while the blunted insulin response associated with higher cortisol levels was seen to result from more constant nutritional deprivation secondary to greater disturbance of behavior. 0 1996 by John Wiley & Sons, Inc. Janice Russell, M.B.B.S., M.D.(Syd.), F.R.A.C.P., F.R.A.N.Z.C.P., M.F.C.P., is Senior Lecturer in the Department of Psychiatry, University of Sydney and Repatriation General Hospital, Concord, New South Wales (NSW), and Director, Eating Disorders Unit, Northside Clinic, Greenwich, NSW. Michael Hooper, M.B.B.S., F.R.A.C.P., is Staff Specialist and Head of the Department of Endocrinology, Repatriation General Hospital, Concord, NSW. Glenn Hunt, B.A., M.Sc., Ph.D.(Syd.), is Research Fellow, Department of Psychiatry, University of Sydney, and Director, Psychopharmacology Laboratory, Repatriation General Hospital, Concord, NSW. Address reprint requests to Dr. )anice Russell, Room 8, Clinical Sciences, Repatriation General Hospital Concord, Hospital Rd, Concord, NSW, 2139 Australia. Some of these data were presented at the 17thCongress of Collegium Internationale Neuro-Psychopharmacolgi- cum Kyoto, Japan, September 10-14, 1990. lnternationa1)ournal of fating Disorders, Vol. 20, No. 3, 307-31 3 (1996) 0 1996 by John Wiley & Sons, Inc. CCC 0276-3478/96/030307-07
-
Upload
janice-russell -
Category
Documents
-
view
216 -
download
2
Transcript of Insulin response in bulimia nervosa as a marker of nutritional depletion

Insulin Response in Bulimia Nervosa as a Marker of Nutritional Depletion
Janice Russell Michael Hooper
Glenn Hunt
(Accepted 29 August 1995)
Objective: The aim of this provocation study was to examine insulin, glucose, and cortisol levels in response to a glucose load in bulimia nervosa patients and to relate this to behavior, treatment status, and depressive symptomatology. Method: A 3-hr glucose tolerance test was performed in 15 female patients and in 4 controls. Tests were performed at different stages of treatment and following documented engagement in the patient’s usual or previous reper- toire of bulimic behaviors in the 24 hr prior to testing. Insulin, glucose, and cortisol levels were assayed at baseline and at 30-min intervals following the glucose load. Presence or absence of significant depressive symptomatology was ascertained. Results: Three patterns of insulin response were identified: ( 1 ) an exaggerated response, (2) a normative response which resembled that of healthy controls, and (3) a blunted pattern. A reciprocal relationship between peak insulin and mean cortisol levels was seen with higher depression scores associated with blunted insulin response. Patients whose response was exaggerated binged and vomited relatively infrequently and were of stable weight. The insulin response of success- fully treated patients, abstinent from binging and vomiting for 4 weeks, was similar to that of normal controls. A blunted response occurred in patients who binged and vomited more frequently, whose weight was unstable, and whose baseline eating was chaotic or nonexistent. Discussion: The exaggerated insulin response was seen as a physiological adaptation to intermittent starvation reversible with treatment, while the blunted insulin response associated with higher cortisol levels was seen to result from more constant nutritional deprivation secondary to greater disturbance of behavior. 0 1996 by John Wiley & Sons, Inc.
Janice Russell, M.B.B.S., M.D.(Syd.), F.R.A.C.P., F.R.A.N.Z.C.P., M.F.C.P., is Senior Lecturer in the Department of Psychiatry, University of Sydney and Repatriation General Hospital, Concord, New South Wales (NSW), and Director, Eating Disorders Unit, Northside Clinic, Greenwich, NSW. Michael Hooper, M.B.B.S., F.R.A.C.P., is Staff Specialist and Head of the Department of Endocrinology, Repatriation General Hospital, Concord, NSW. Glenn Hunt, B.A., M.Sc., Ph.D.(Syd.), is Research Fellow, Department of Psychiatry, University of Sydney, and Director, Psychopharmacology Laboratory, Repatriation General Hospital, Concord, NSW. Address reprint requests to Dr. )anice Russell, Room 8, Clinical Sciences, Repatriation General Hospital Concord, Hospital Rd, Concord, NSW, 2139 Australia.
Some of these data were presented at the 17th Congress of Collegium Internationale Neuro-Psychopharmacolgi- cum Kyoto, Japan, September 10-14, 1990.
lnternationa1)ournal of fating Disorders, Vol. 20, No. 3, 307-31 3 (1996) 0 1996 by John Wiley & Sons, Inc. CCC 0276-3478/96/030307-07

308 Russell, Hooper, and Hunt
Studies performed so far have demonstrated normal and in some cases elevated insulin levels in patients suffering from bulimia nervosa (Schweiger et al., 1987; Casper, Paddy, Jaspar, & Rubenstein, 1988; Kaye, Gwirtsman, & George, 1989; Russell, Hooper, Storlien, & Smythe, 1989). These variable findings can be explained on the basis of differing provoca- tion agents, for example, varying glucose loads or test meals, bulimic behaviors on the day or days prior to testing, and the longer-term nutritional state. The latter would be expected to be determined by the usual pattern of bulimic behavior, size and frequency of binges and vomits, occurrence of fasting, the energy content of the usual diet, meal architecture, chronicity, and the effects of any treatment. The relationship of depressive symptoms and/or syndromes and elevated cortisol levels in patients with bulimia nervosa has been noted (Levy, Dixon, & Stern, 1989; Fichter, Pirke, Pollinger, Wolfram, & Brun- ner, 1990).
The aim of this study was to examine insulin, glucose, and cortisol levels in response to a standardized glucose load in patients suffering from bulimia nervosa and to relate this to their usual combination of bulimic behaviors, depressive symptomatology, and treatment status.
METHODS
Subjects were all female and met criteria for bulimia nervosa outlines in the Diagnostic and statistical manual of mental disorders at entry into the study (American Psychiatric Associa- tion, 1980, 1987). The group included newly diagnosed outpatients, relapsed patients, those completing inpatient treatment with successful and unsuccessful outcomes, and recovered, improved, stable, and recidivist outpatients. All patients had been in treatment with the first author for periods of 1 month to 3 years and all had made logs of their eating/weight losing behaviors during the period of treatment. The study was approved by the Ethics Committee of the Mt. St. Margaret Private Hospital, Ryde, N.S.W., and written informed consent was given by all participants.
A 3-hr glucose tolerance test using a 100-g glucose load was performed. Patients were asked to engage in their usual combination of bulimic behaviors on the day prior to testing (even if they had been abstinent from such behaviors in recent weeks). This was documented in food and behavior logs which they were asked to keep for a minimum of 3 days. On the day prior to testing, they fasted from 9 p.m., came to the laboratory at 8 a.m. the following morning, were weighed and measured, then rested for 45 min when an intravenous (IV) cannula was inserted. Subjects were instructed to drink only water prior to testing. Blood was taken at baseline and at 30-min intervals for 3 hr. Analyses for glucose, insulin, and cortisol were performed (see below). Patients were asked to refrain from taking laxatives or any other medication for at least 1 week prior to testing; exceptions being continuation of therapeutic dose of mianserin in one case, thyroxine replacement in another, and an oral contraceptive in three patients who were taking these on a regular basis.
A similar glucose tolerance test was performed in 4 nondieting female medical students who completed food logs for 3 days before testing, and were interviewed to exclude past or current eating disorder and excessive alcohol use.
Plasma glucose was measured with an automatic analyzer by the glucose oxidase method. Serum insulin was measured by a double antibody radioimmunoassay (Phar- macia) and serum cortisol by a single antibody radioimmunoassay (Amerlex).

Insulin a n d Nutrit ional Depletion 309
A variety of depression inventories and rating scales were used to assess the level of depressive symptomatology : the Beck Depression Inventory (BDI; Kendall, Hollon, Beck, Hammen, & Ingram, 1983, the self-report symptom rating scale devised by the Center for Epidemiological Studies (CES-D; Weissman, Sholomsakas, Pottenger, Prusoff, & Locke, 1977), and the 24-Item Hamilton Rating Scale for Depression (HRSD; Hamilton, 1960). Patients were merely ascertained to be at or above cutoff for the particular instrument (i.e., indicative of significant depressive symptomatology) or below cutoff (i.e., no significant depressive symptomatology). Cutoff scores used were 16,30, and 12 for CES-D, BDI, and HRSD, respectively (Hamilton, 1960; Weissman et al., 1977; Kendall et al., 1987).
Patients were grouped according to insulin response. Frequency and type of habitual bulimic behaviors were documented from information contained in food logs and clinical records. Treatment status and behavior, mean cortisol levels, and depression scores were related to insulin responses.
Statviewt" and Cricket Graph'" statistical and graphics packages were used with analyses of variance (ANOVAs), Scheff's Test, and Fisher's Exact Test to ascertain the significance of changes between and within groups. Significance was ascribed at p values less than .05.
RESULTS
Fifteen female patients and 4 controls were tested. Mean age of the controls was 21 years and mean body mass index (BMI) was 21.5. Two patients were retested following 8 weeks of inpatient treatment. Patients ranged in age from 19 to 41 years, with a mean of 24.5 years. BMI range was 16-25; mean was 21.5. Three months earlier, one patient whose BMI was 16 had had a BMI of 20; her weight had been unstable for 5 years and she engaged in frequent binging and vomiting. On retesting her weight had normalized. Another patient was alleged to have had a BMI of 16 some months prior to testing, but was tested at a BMI of 22.
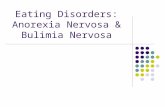
Three different patterns of insulin response to the glucose load were observed (Fig. 1). These were (1) an insulin response (N = 4) similar to that of normal controls (N = 4), (2) an exaggerated insulin response (N = 4), and (3) a blunted insulin response (N = 9).
Cmax insulin in the first group was 75-101 mU/L and that of controls 93-162 mU/L with a single peak. Secondary peaks were seen only in the group with the highest Cmax of 110-206 mU/L. In contrast, a blunted response with little discernible insulin peak, that is, between 24 and 53 mUI/L, was demonstrated in 7 patients for whom hospitalization was recommended and in 2 of these who were retested following inpatient treatment. There was a significant difference ( p = .OOl) between groups and within groups with respect to mean and maximum insulin response, that is, the blunted insulin response group differed from the other three groups which did not differ significantly from each other.
Analysis of clinical records and food logs prior to testing (which most often reflected usual bulimic behavior) revealed common features in the behavior and treatment status of patients within insulin-response groups. Patients of stable weight who were binging and vomiting less than five times a day on average and who fasted or ate abstemiously between binges had the greatest insulin response. A blunted response was seen in the 3 patients who binged and vomited 10-20 times a day, whose weight had been unstable, and who had just been admitted to the hospital. A similar response (but slightly less blunted) was seen in 6 patients (including 2 of the previous 3 patients who were retested following inpatient treatment during which their compliance had been poor). These pa- tients were considered to be partially treated but were continuing to binge and vomit,

31 0 Russell, Hooper, and Hunt
Insulin following glucose load
* b&ve5 T - treated --P-
+ 150
100
50
0
b&v>lO partial treated Healthy controls
9:OO 9:30 1O:OO 10:30 11 :00 11 :30 12:OO
Clock Tim
Figure 1. Insulin levels (mU/L) at 30-min intervals in response to a 100-g glucose load given at 9:OO a.m. comparing five groups of subjects. Open circles indicate patients who binged and vomited less than five times a day (N = 4). Closed diamonds indicate successfully treated patients who had abstained from binging and vomiting for approximately 4 weeks (N = 4). Open squares indicate severely ill patients who binged and vomited 10-20 times a day (N = 3). Open diamonds indicate patients who had partially responded to treatment and were binging and vomiting 5-10 times a day. Large open squares indicate normal controls (N = 4).
albeit less often with an average frequency of 5-10 episodes per day. The patients whose insulin response resembled that of normals had all been successfully treated, 3 as inpatients and 1 as an outpatient and all had refrained from engaging in bulimic behavior for approximately 4 weeks before testing.
Differences in cortisol levels between groups achieved statistical significance which was attributable to lower levels in the patients who binged and vomited less frequently and
Peak Insulin 81 Mean Cortisol
Treatment Group
Figure 2. Peak insulin (mU/L) and mean cortisol levels (mmol/L) in four groups of bulimic patients following a 100-g glucose load given at 9 a.m. with 30-min sampling for 3 hr. From left to right: less than five binge and vomit episodes per day (N = 4), no binge and vomit episodes for 4 weeks following successful treatment (N = 4), 5 to 10 binge and vomit episodes per day after partially successfully treatment (N = 6), more than 10 binge and vomit episodes per day, that is, severely ill patients prior to admission to hospital (N = 3).

Insulin and Nutritional Depletion 31 1
whose insulin levels were higher ( p = .038). A significant change in levels within all groups over the 3-hr time course was demonstrated which was due to normal diurnal decrement. A reciprocal relationship between group mean cortisol levels and mean Cmax insulin levels was seen, that is, low cortisols were associated with higher insulin levels and vice versa (Fig. 2).
Differences between and within bulimic groups for glucose were not significant, al- though there was a trend for levels to be slightly higher in the partially treated and frequent bingers and vomiters. Despite the low insulin levels of patients in these groups, glucose levels did not reach levels seen in diabetic patients and in most cases had returned to baseline levels at the conclusion of testing.
Although the method of ascertainment of depressive ”caseness” is far from optimal and the low numbers precluded statistical analysis, the results supported a relationship between higher levels of depressive symptomatology, lower peak insulin levels, higher cortisol levels, and more disordered eating behavior.
DISCUSSION
The main finding of this limited study were the differences in insulin responses and cortisol levels between groups which differed in terms of frequency and nature of bulimic behaviors and/or treatment response. The method of testing in this study used the double provocation of the patient’s usual bulimic behaviors in the preceding 24 hr as well as a larger standard oral glucose load. This would seem to be an appropriate, albeit controver- sial, way of ensuring that patients are in a relatively similar state with respect to the day- to-day behavioral variability of bulimia nervosa. This type of investigative strategy has been supported by Johnson, Jarrell, Chupurdia, and Williamson (1994). Furthermore, engagement in bulimic behavior is self-perpetuating so that understanding of the metabolic changes at this point (i.e., following bulimic behavior, fasting, and a large carbohydrate load) would appear to be more relevant than when nutrition has been relatively normal.
Elevated insulin levels were also demonstrated in response to a balanced test meal in bulimia nervosa patients (Schweiger et al., 1987) and were seen to represent a metabolic response to intermittent starvation. Other parameters of starvation have been reported in normal-weight bulimic patients, namely, elevated ketones, depressed triiodothyronine levels, and impaired orthostatic responsivity (Pahl et al., 1985). The finding of impaired glucose tolerance and increased secretion of insulin is supported by earlier studies in acute experimental starvation and anorexia nervosa during refeeding (Unger, Eisentrant, & Madison, 1963). However, Johnson et al. (1994) found no evidence for an exaggerated cephalic phase insulin secretion in 8 bulimic patients. Reduction of insulin potentiation following nutritional rehabilitation was demonstrated in a previous study which included the treated inpatients reported here (Russell et al., 1989). Relative hyperinsulinemia in response to a glucose load following engagement in bulimic behavior might defend against intermittent starvation by increasing appetite and, by the lipotrophic action of insulin, promoting weight maintenance despite variable levels of nutrition. This contrasts with the blunted and reduced insulin response seen in the more behaviorally disordered pa- tients. Unlike the first group, these vomited frequently both in absolute terms and relative to binge episodes whilst their baseline eating was chaotic or nonexistent. Thus their degree of nutritional deprivation was likely to have been greater as evidenced by the inability to maintain normal weight in the most severely ill of the group.

31 2 Russell, Hooper, and Hunt
Glucose tolerance was mildly impaired in bulimic patients as a group and compared to controls, although there was no difference between bulimic groups which is surprising in view of the differences in insulin response. Diminished insulin secretion may have reflected greater depletion of total body potassium which has been shown to impair glucose tolerance and insulin release (Rowe, Tobin, Rosa, & Andres, 1980) and which has been demonstrated in patients suffering from bulimia and anorexia nervosa (Pirke et al., 1986) presumably on the basis of nutritional deprivation, purgation, and loss of lean body mass. Normal extracellular potassium levels in the patients reported here may not adequately reflect the total body or pancreatic intracellular situation. Johnson et al. (1994) reported hypoglycemia immediately following purging and suggested this as a perpetuat- ing factor in the occurrence of binge-purge cycles. However, elevations in insulin and glucose levels similar to those of normals (and of our patients on the day after bulimic behavior) were noted following a subsequent meal which was not purged.
Lower plasma cortisol levels have been previously demonstrated in some of the patients reported have following engagement in bulimic behavior (Russell et al., 1989) and were seen to be related to ingested carbohydrates, an effect reported in animal studies and linked to reduction of catecholamine levels and the perception of stress (Smythe, Brad- shaw, & Vining, 1983). In this study, however, it can be seen that the relationship between insulin and cortisol was reciprocal with blunted insulin response being associated with higher cortisol levels, and low cortisol levels with high and normal insulin levels. In this respect, severely ill patients with bulimia nervosa may be similar to patients with anorexia nervosa in whom low insulin levels and elevated cortisol levels have been reported (Kiriike et al., 1990).
Higher levels of depressive symptomatology were seen in association with higher cortisol levels. Both could arise as an effect of nutritional deprivation alone, rather than elevated cortisols being associated with primary depressive disorder and bulimic behavior arising as a symptom of this. The consensus of opinion is that bulimia nervosa is a primary condition and not a form of depressive disorder (Levy et al., 1989).
In summary, this study has demonstrated a blunted insulin response in a subgroup of patients suffering from bulimia nervosa. This most likely reflects a greater degree of nutritional depletion in patients who engage more frequently in bulimic behaviors, particu- larly vomiting, and in whom there may be no more nutrition between episodes of binge eating. Higher cortisol levels and depression scores are also likely to be related to this cause.
Thanks are due to the staff of the eating Disorder Units of the former Mt. St. Margret Hospital and the Northside Clinic, to the nursing and technical staff of the Endocrine Ward Concord Hospital, and to Professors Peter Beumont and Leonard Storlien for their valued assistance.
REFERENCES
American Psychiatric Association. (1980). Diagnostic and sfatistical manual ofniental disorders (3rd ed.). Washington,
American Psychiatric Association (1987). Diagnostic and statistical manual of mental disorders (3rd Rev: ed.).
Casper, R. C., Paddy, G. N., Jaspar, J. B., & Rubenstein, A. H. (1988). Hormone and metabolite plasma levels
Fichter, M. M., Pirke, K.-M., Pollinger, J., Wolfram, G., & Bruner, E. (1990). Disturbance in the hypothalamo-
Hamilton, M. (1960). A rating scale of depression. Journal of Neurology, Nerirosirrgery and Psychiatry, 23, 56-62.
DC: Author.
Washington, DC: Author.
after oral glucose in bulimia and healthy controls. Biological Psychiatry, 24, 663-674.
pituitary-adrenal and other neuroendocrine axes in bulimia. Biological Psychiatry, 27, 1021-1037.

insulin and Nutritional Depletion 31 3
johnson, W. G., Jarrell, M. P., Chupurdia, K. M., & Williamson, D. A. (1994). Repeated binge/purge cycles in bulimia nervosa: Role of glucose and insulin. International Journal of Eating Disorders, 15, 331-341.
Kaye, W. H., Gwirtsman, H. E., & George, D. T. (1989). The effect of bingeing and vomiting on hormonal secretion. Biological Psychiatry, 25, 768-780.
Kendall, P. C., Hollon, S. D., Beck, A. T., Hammen, C. L., & lngram, R. E. (1987). Issues and recommendations regarding use of the Beck Depression Inventory. Cognitive Therapy and Research, 11, 289-299.
Kiriike, N., Nishiwalu, S., Nagata, T., Okuno, Y., Yamada, J., Tanaka, S., Fujiii, A., & Kawakita, Y . (1Y90). Insulin sensitivity in patients with anorexia nervosa and bulimia. Acta Psychiatrica Scandinauica, 81, 236-239.
Levy, A. B., Dixon, K. N., & Stern, S. L. (1989) How are depression and bulimia related? American Ioiirnal of Psychiatry, 146, 162-169.
Pahl, J., Pirke, K.-M., Schweiger, U., Warnhoff, M., Gerlinghoff, M., Brinkmann, W., Berger, M., & Krieg, C. (1985). Anorectic behaviour, mood and metabolic and endocrine adaptation to starvation in anorexia nervosa during inpatient treatment. Biological Psychiatry, 20, 874-887.
Pirke, K.-M., Pahl, J., Schweiger, U., Munzing, W., Lang, l'., & Bull, U. (1986). Total body potassium, intracellular potassium and body composition in patients with anorexia nervosa during refeeding. International journal of Eating Disorders, 5, 357-364.
Rowe, J. W., Tobin, J. D., Rosa, R. M., & Andres, R. (1980). Effect of experimental potassium depletion on glucose and insulin metabolism. Metabolism, 29, 498-502.
Russell, J., Hooper, M., Storlien, L., & Smythe, G. A. (1989). Insulin, glucose and cortisol levels in bulimia: Effect of treatment. International journal of Eating Disorders, 8, 635-646.
Schweiger, U., Poellinger, J., Laessle, R., Wolfram, G., Fichter, M. M., & Pirke, K.-M. (1987). Altered insulin response to a balanced test meal in bulimic patients. International journal of Eating Disorders, 6, 551-556.
Smythe, G. A., Bradshaw, J. E., & Vining, R. F. (1983). Hypothalamic monoamine control of stress induced adrenocorticotropin release in the rat. Endocrinology, 113, 1062-1071.
Unger, R. H., Eisentraut, A. M., &Madison, L. L. (1963). The effects of total starvation upon the levels of glucagon and insulin in man. Journal of Clinical Investigation, 42, 1031-1039.
Weissman, M. A., Sholomsakas, D., Pottenger, M., Prusoff, B. A., & Locke, B. Z. (1977). Assessing depressive symptoms in five psychiatric populations: A validation study. American journal of Epidemiology, 206, 203-214.











![Bulimia Nervosa[1]](https://static.fdocuments.in/doc/165x107/577d29fe1a28ab4e1ea86b11/bulimia-nervosa1.jpg)