Insulin
29
INSULIN
-
Upload
university-of-the-east-ue -
Category
Documents
-
view
88 -
download
0
Transcript of Insulin
INSULIN
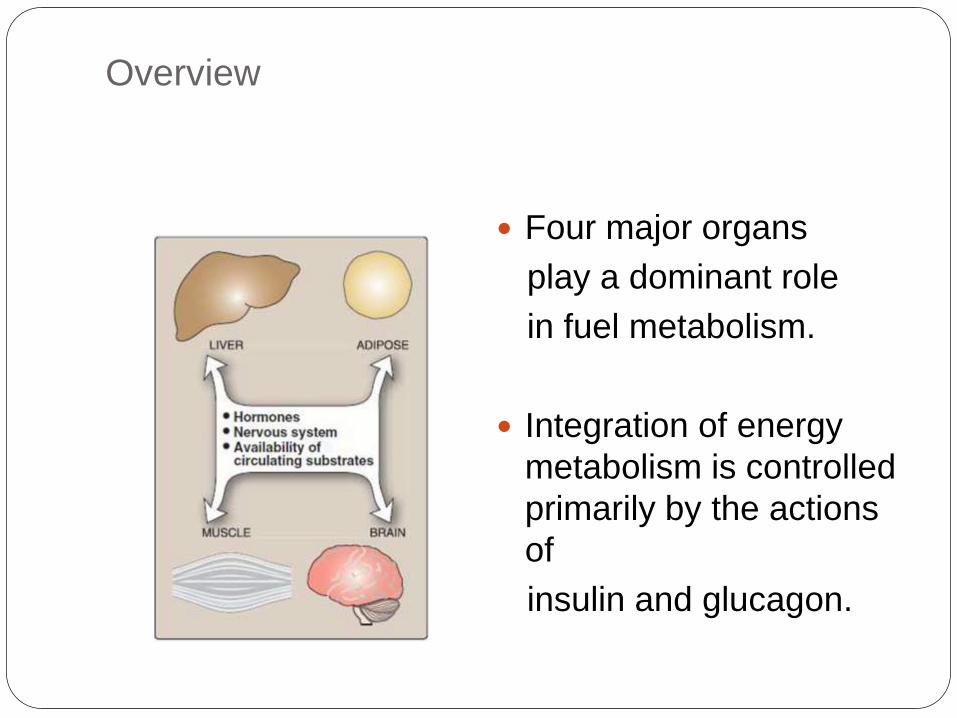
Overview
Four major organs
play a dominant role
in fuel metabolism.
Integration of energy
metabolism is controlled
primarily by the actions
of
insulin and glucagon.
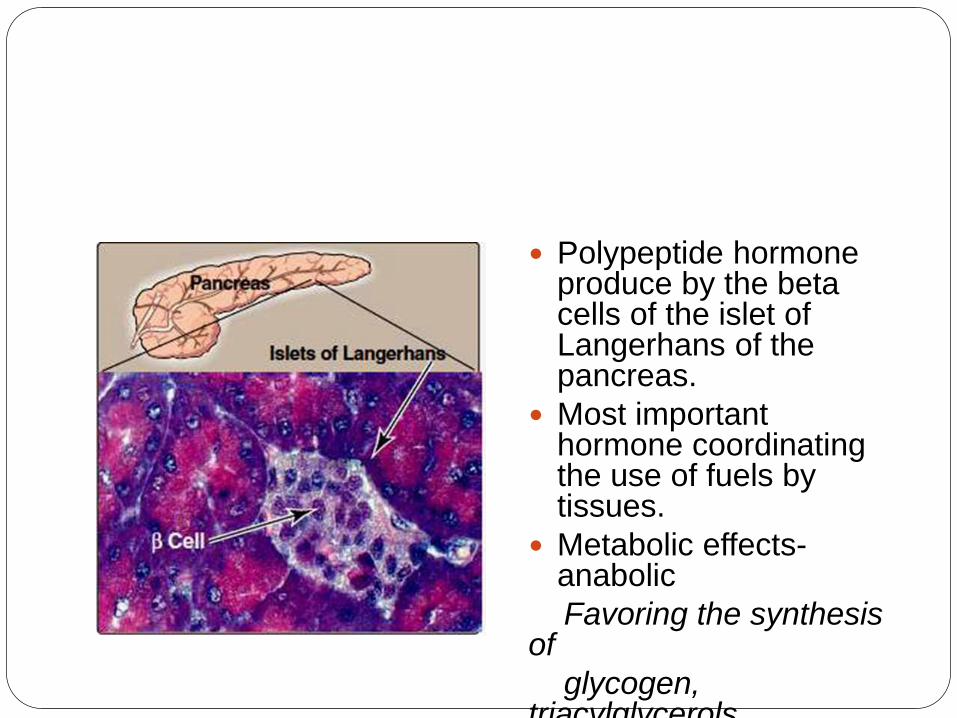
Polypeptide hormone produce by the beta cells of the islet of Langerhans of the pancreas.
Most important hormone coordinating the use of fuels by tissues.
Metabolic effects-anabolic
Favoring the synthesis of
glycogen, triacylglycerols
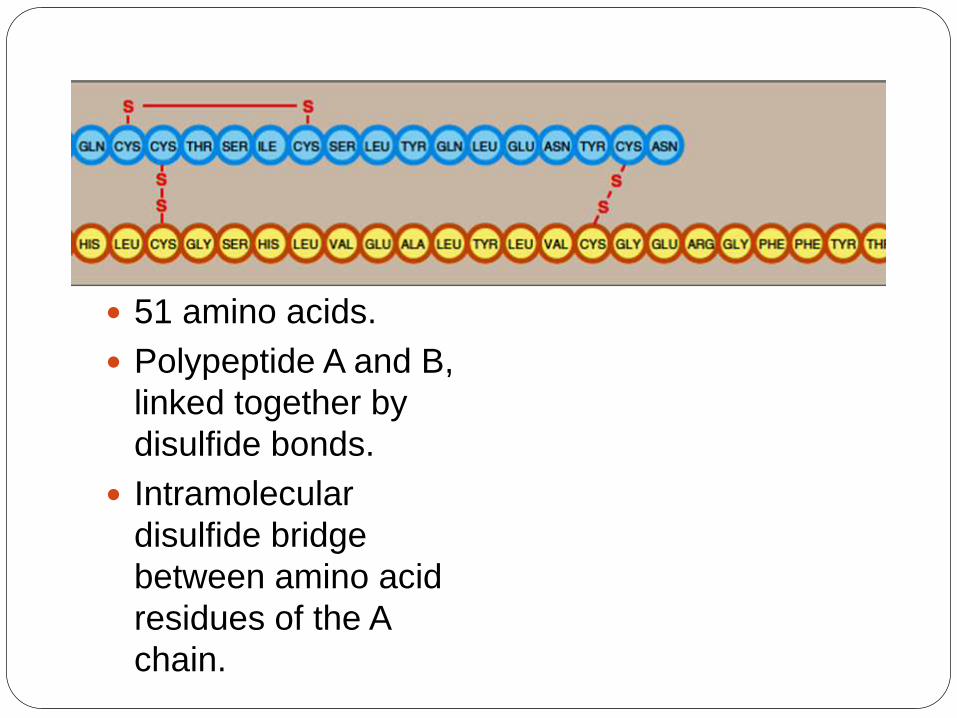
51 amino acids.
Polypeptide A and B,
linked together by
disulfide bonds.
Intramolecular
disulfide bridge
between amino acid
residues of the A
chain.
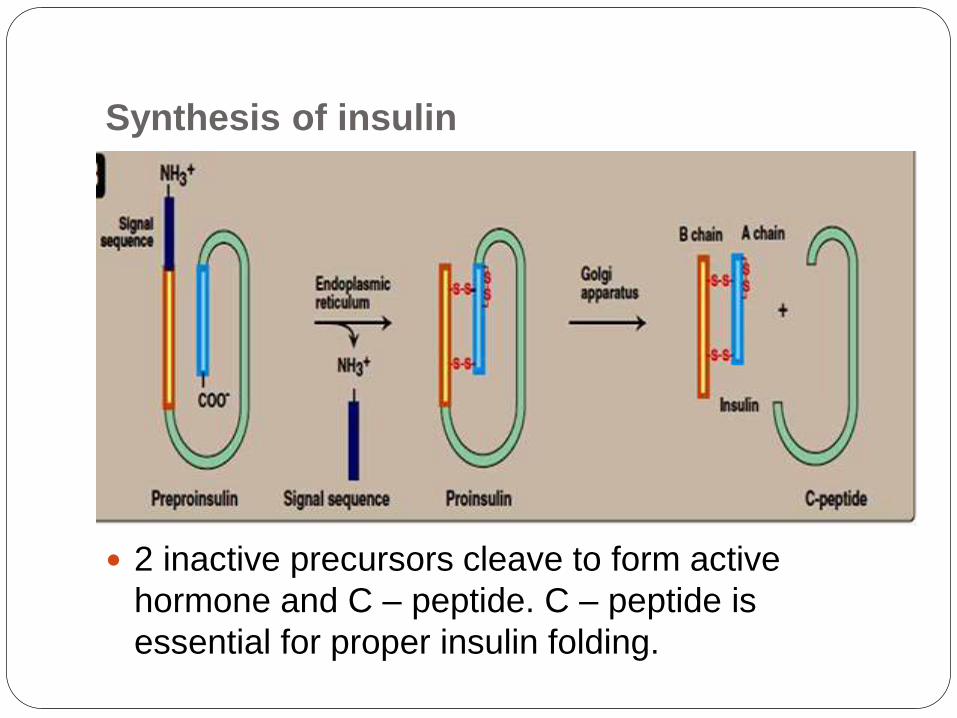
Synthesis of insulin
2 inactive precursors cleave to form active
hormone and C – peptide. C – peptide is
essential for proper insulin folding.
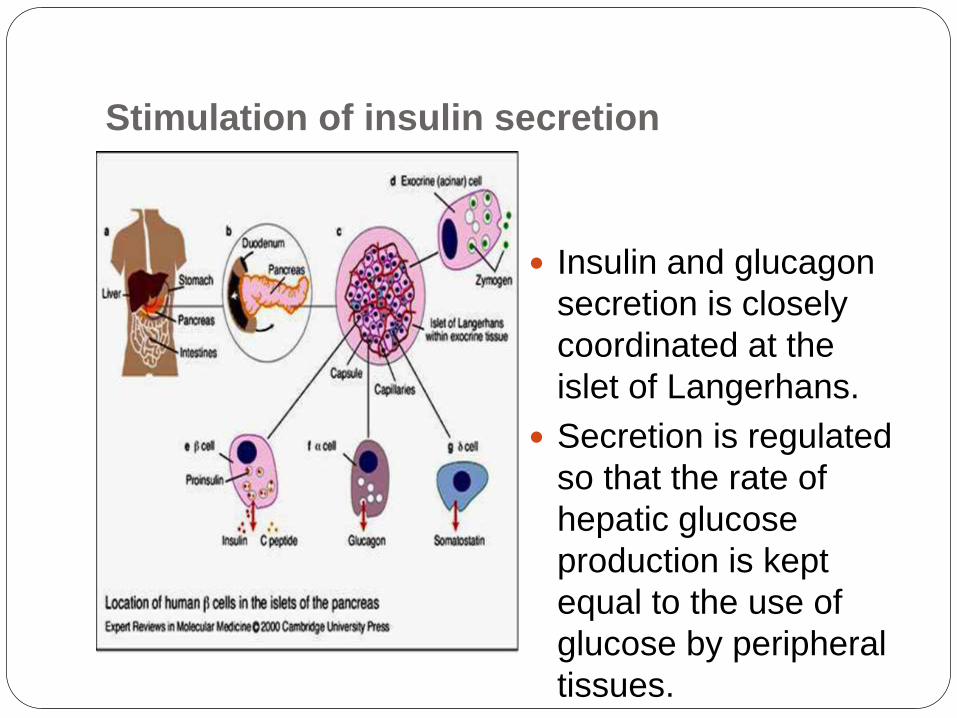
Stimulation of insulin secretion
Insulin and glucagon
secretion is closely
coordinated at the
islet of Langerhans.
Secretion is regulated
so that the rate of
hepatic glucose
production is kept
equal to the use of
glucose by peripheral
tissues.
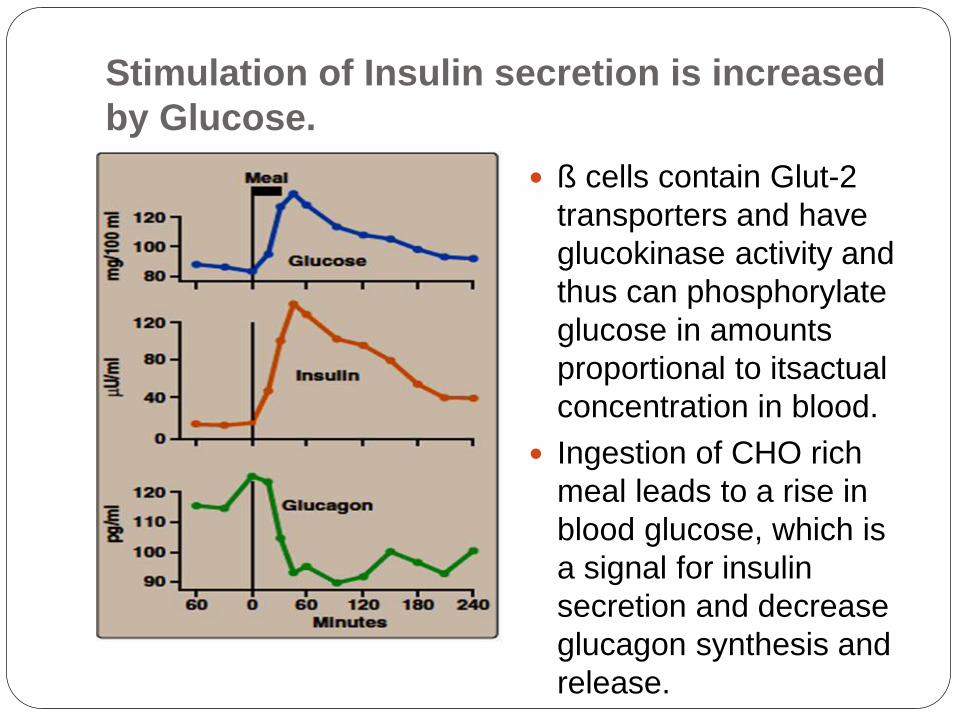
Stimulation of Insulin secretion is increased
by Glucose.
ß cells contain Glut-2
transporters and have
glucokinase activity and
thus can phosphorylate
glucose in amounts
proportional to itsactual
concentration in blood.
Ingestion of CHO rich
meal leads to a rise in
blood glucose, which is
a signal for insulin
secretion and decrease
glucagon synthesis and
release.
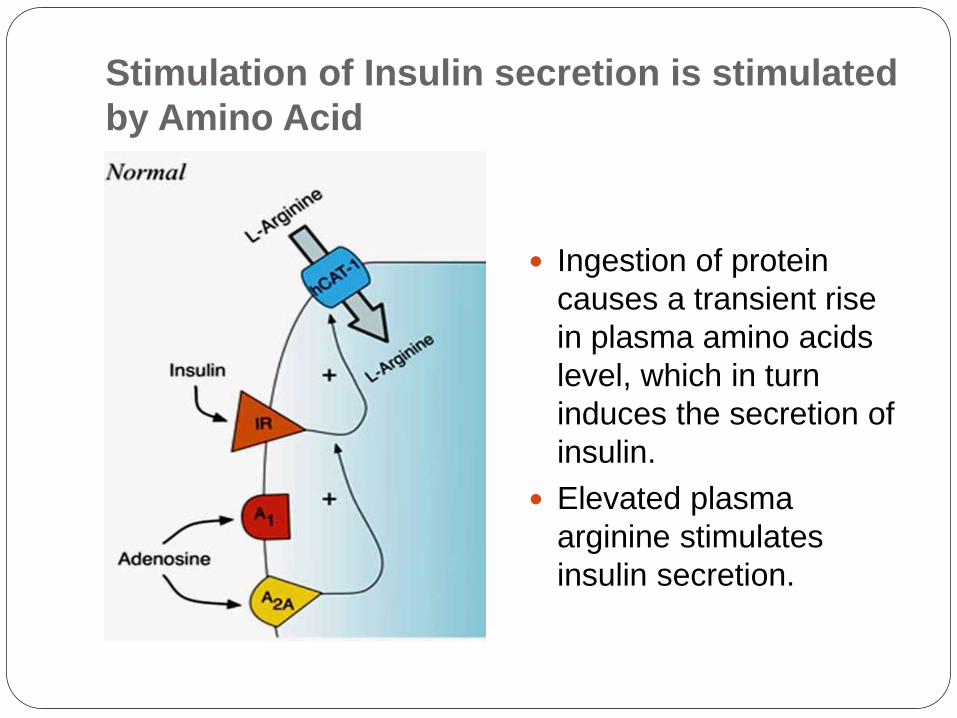
Stimulation of Insulin secretion is stimulated
by Amino Acid
Ingestion of protein
causes a transient rise
in plasma amino acids
level, which in turn
induces the secretion of
insulin.
Elevated plasma
arginine stimulates
insulin secretion.
Stimulation of Insulin secretion increased by
Gastro- Intestinal hormones.
Cholecytoskinin and gastric-inhibitory peptide increased insulin secretion.
Released from SI in response to oral glucose and cause anticipatory rise in insulin levels.
This may account for the fact that the same amount of glucose given orally induces a much greater secretion of insulin that is given

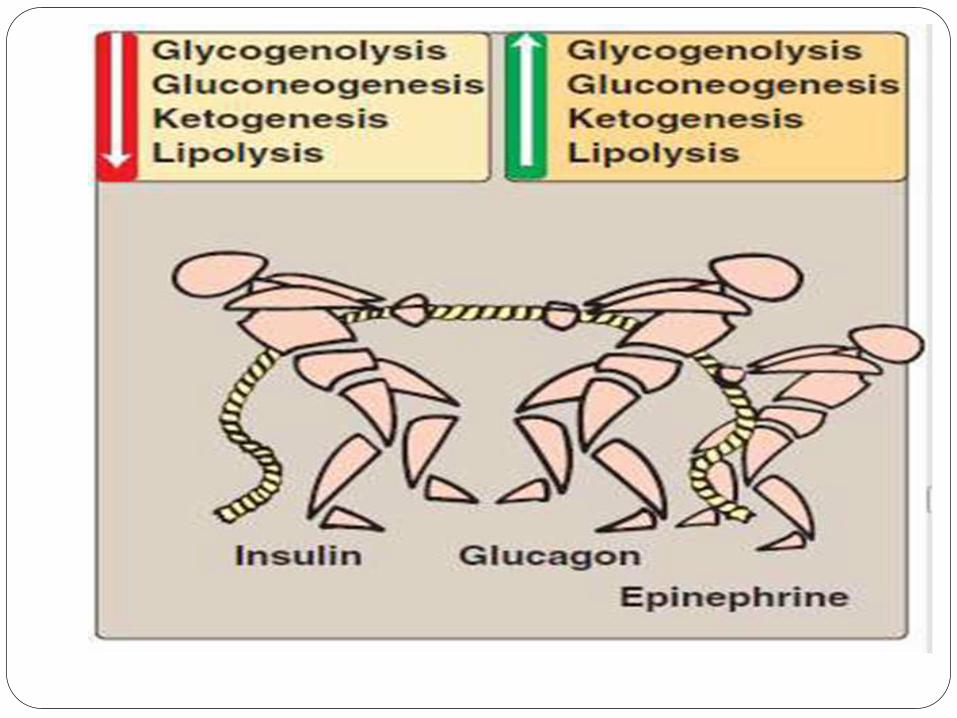
Inhibition of insulin secretion: Epinephrine.
Scarcity of dietary fuels and during the period of stress,
Direct effect on energy metabolism
causing glycogenolysisand
Gluconeogenesis,
Can override the normal glucose-
stimulated release of insulin,
In emergency situation, the sympathetic nervous system largely replaces the plasma glucose concentration as the controlling influence over ß cells Secretion.
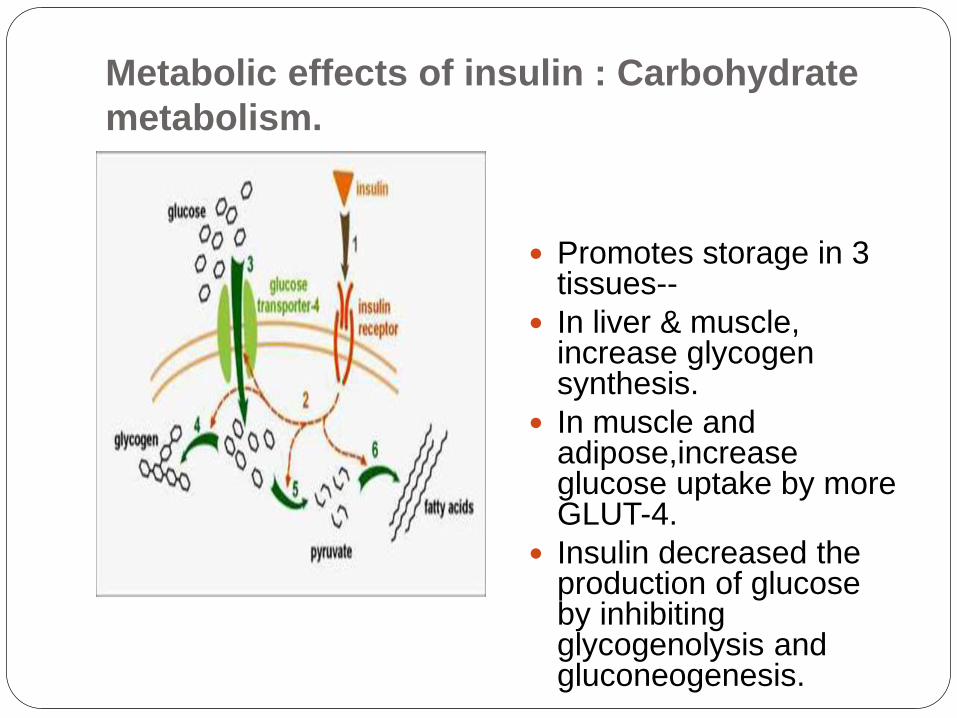
Metabolic effects of insulin : Carbohydrate
metabolism.
Promotes storage in 3 tissues--
In liver & muscle, increase glycogen synthesis.
In muscle and adipose,increaseglucose uptake by more GLUT-4.
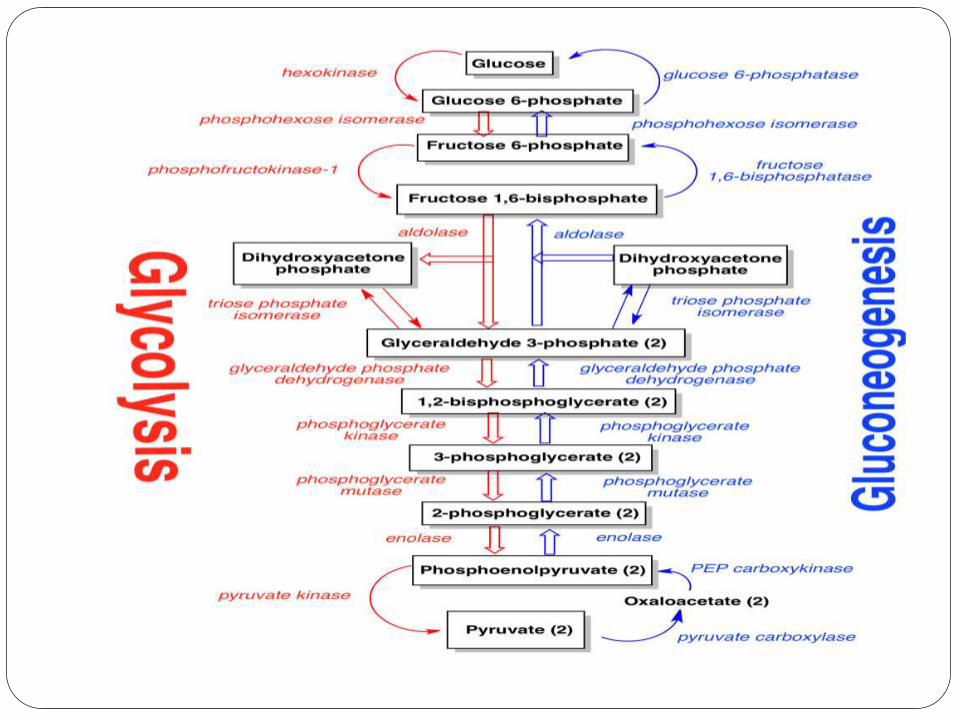
Insulin decreased the production of glucose by inhibiting glycogenolysis and gluconeogenesis.
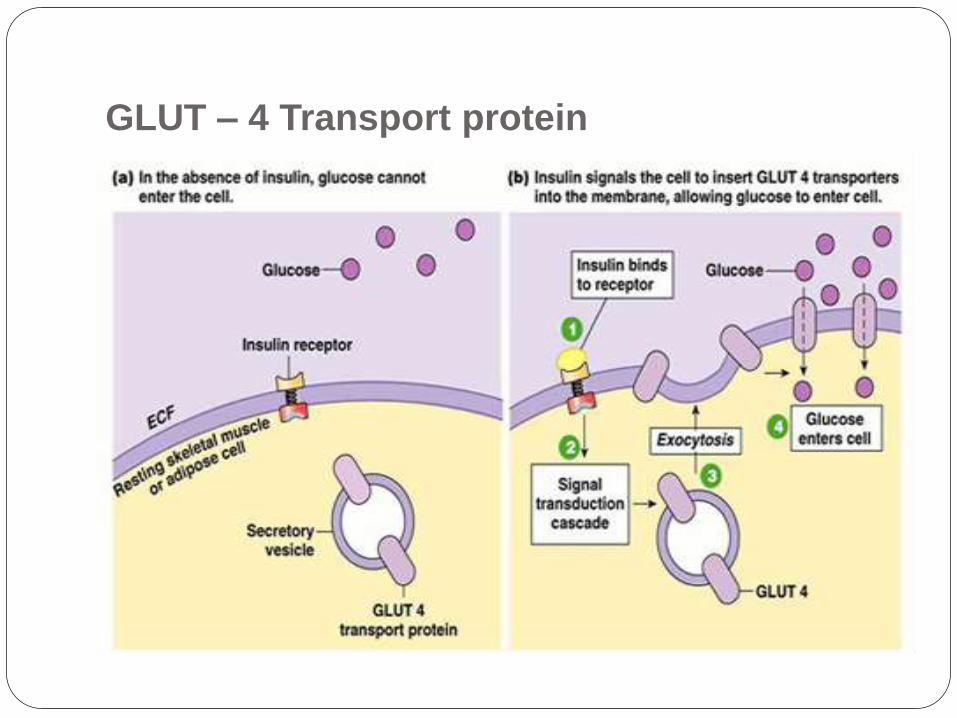
GLUT – 4 Transport protein
Metabolic effects of insulin- lipid
metabolism
Decrease TAG
degradation.
Insulin inhibits hormone
sensitive lipase ,
Increaes TAG
synthesis.
Insulin increases
transport and
metabolism of glucose
into adipocytes
providing substrate for
glycerol -3- phosphate
for TAG synthesis.
Also increases the
lipoprotein lipase,thus
providing fatty acids for
Metabolic effects of insulin : Protein
synthesis.
Insulin stimulates the entry of amino acids into
cells, and protein synthesis through activation of
factors required for translation.
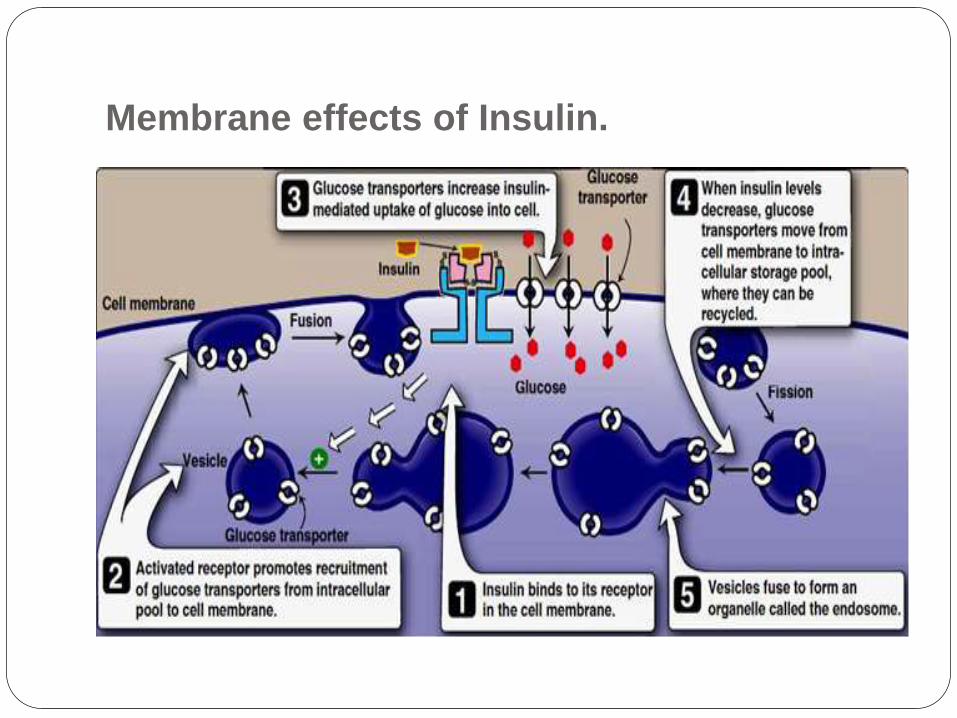
Membrane effects of Insulin.
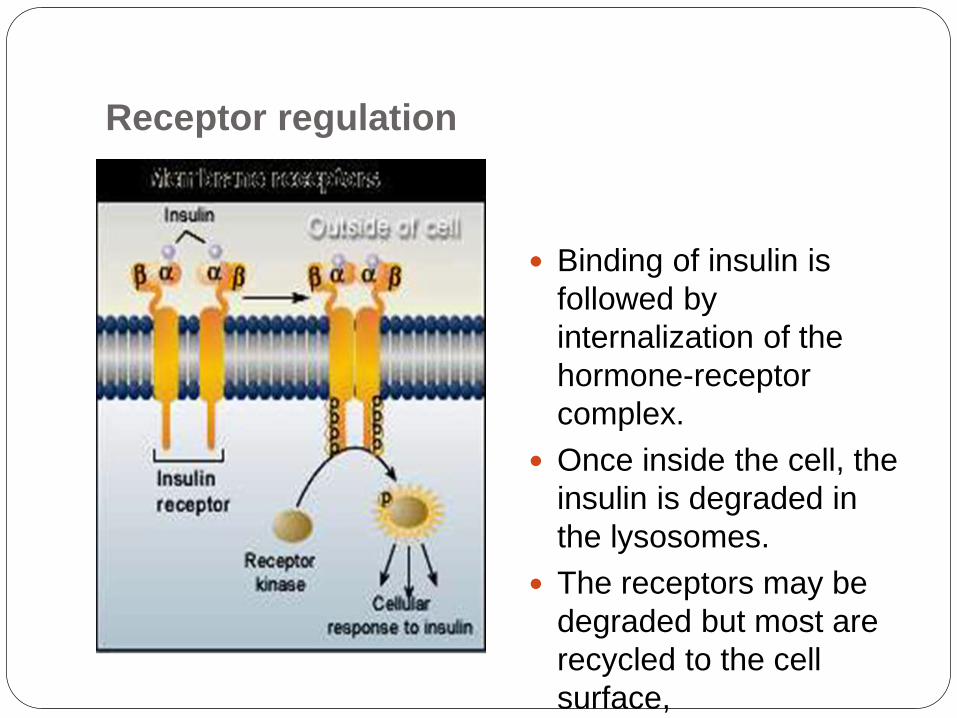
Receptor regulation
Binding of insulin is
followed by
internalization of the
hormone-receptor
complex.
Once inside the cell, the
insulin is degraded in
the lysosomes.
The receptors may be
degraded but most are
recycled to the cell
surface,
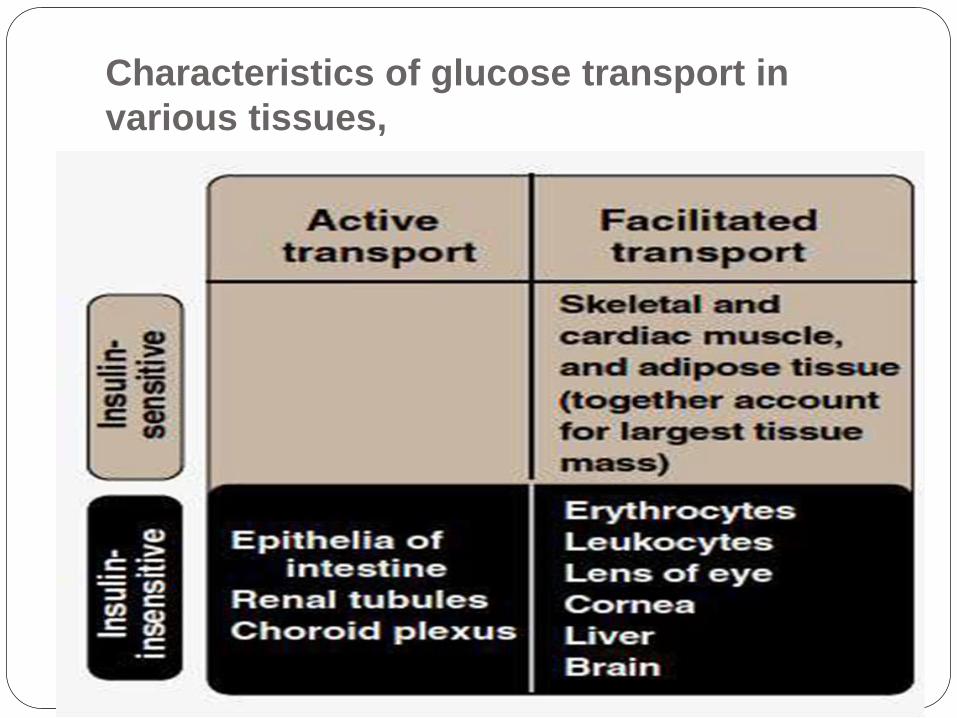
Characteristics of glucose transport in
various tissues,
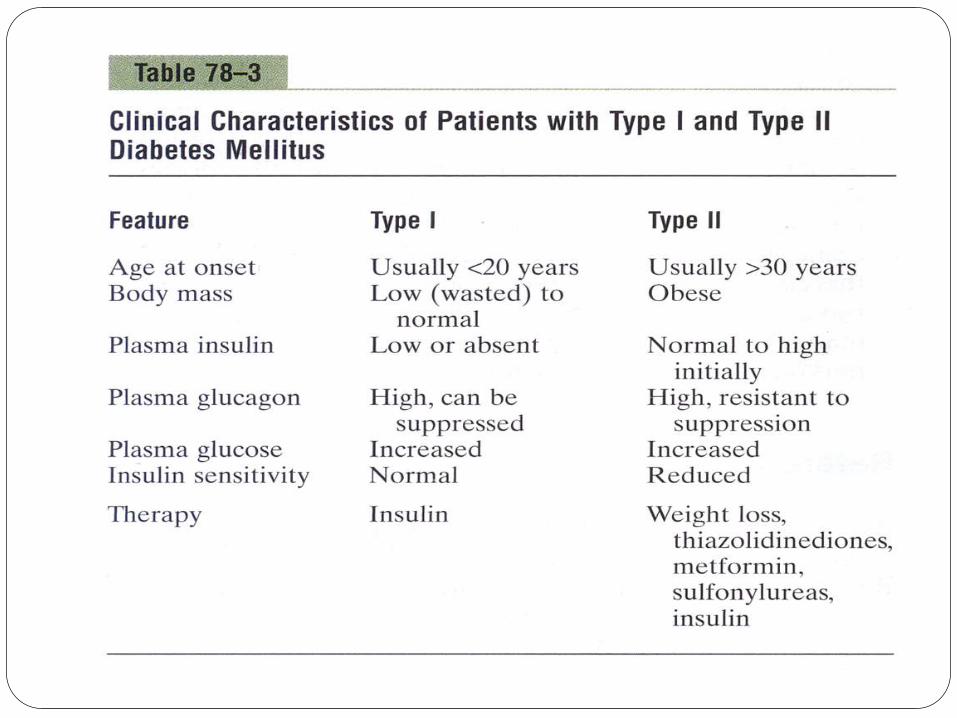
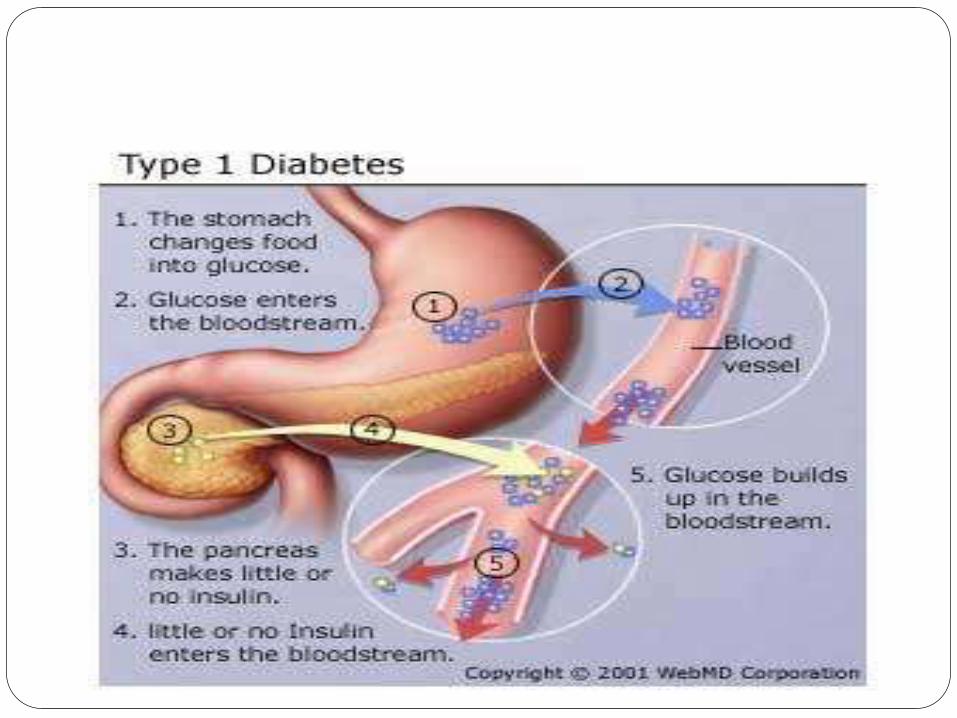
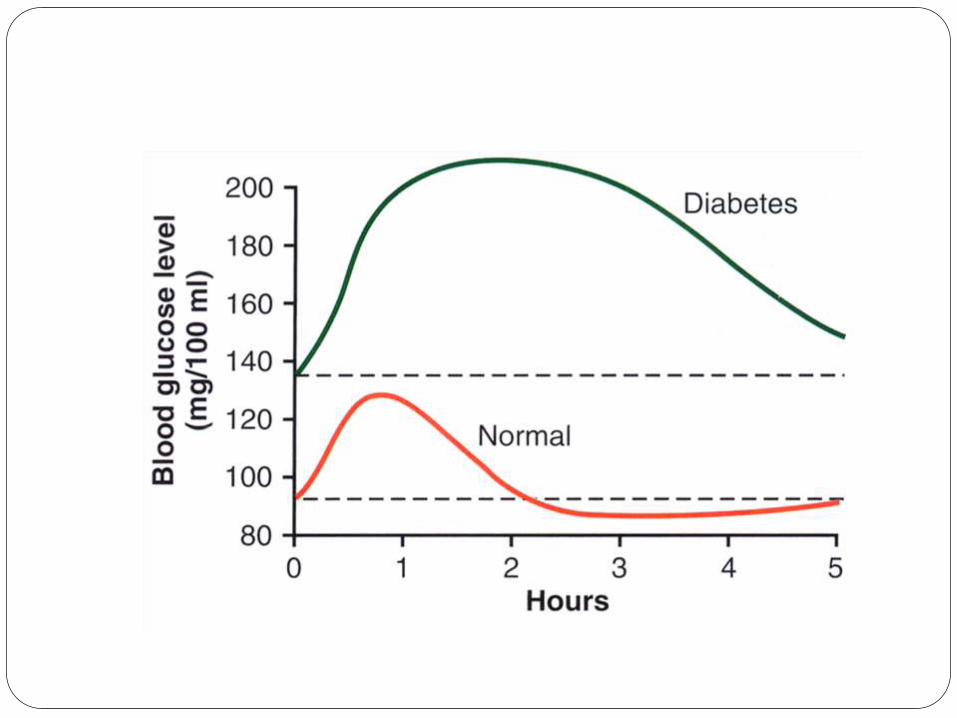
Diabetes Mellitus
Type I
Insulin dependent
Juvenile onset
Causes--
-Increased blood glucose (300-1,200 mg/100ml)
-Increased blood fatty acids and cholesterol
-Protein depletion
Treated with insulin injections
Increases risk of heart disease and stroke
Can cause acidosis and coma
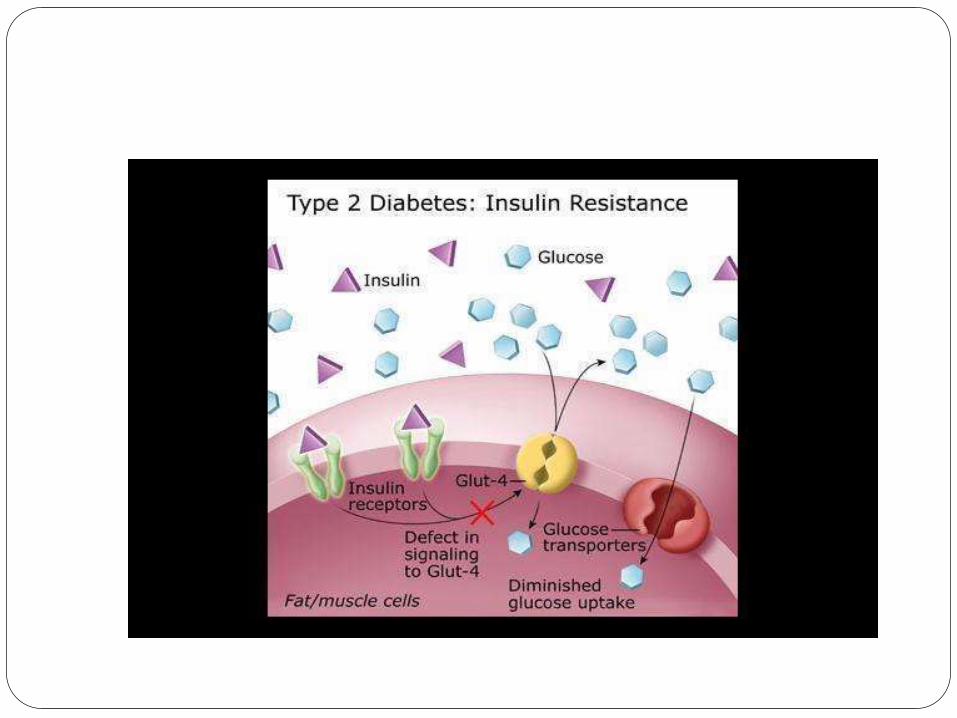
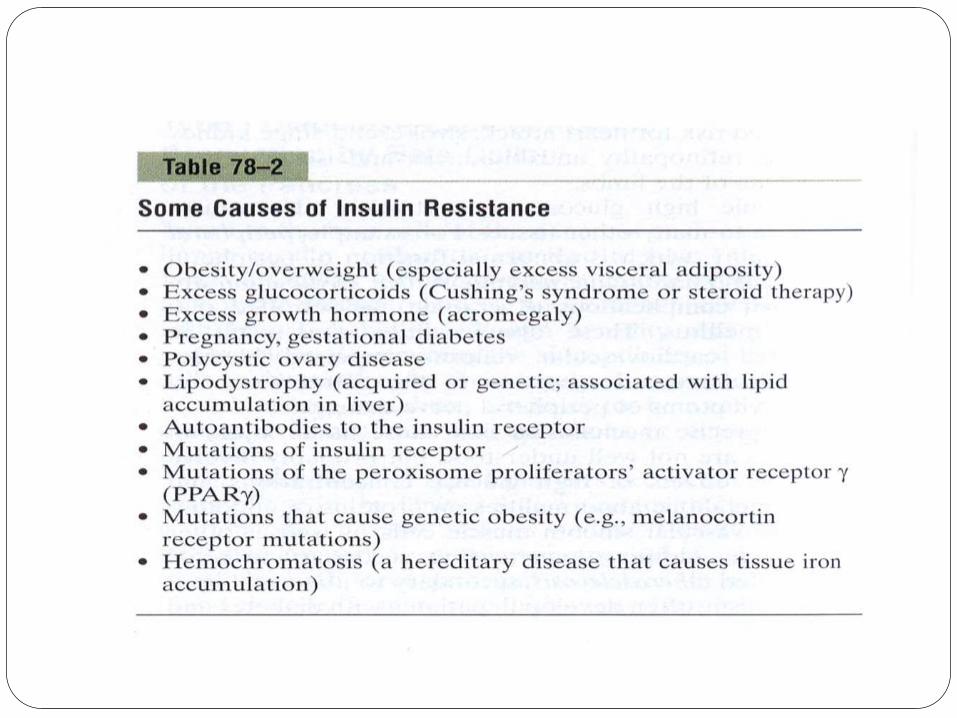
Type II
Non-insulin dependent.
Results from insulin insensitivity.
Elevated insulin levels.
Associated with obesity.
Can lead to insulin dependent form.
Treated with weight loss, diet restriction, exercise
and drugs.

THANK YOU!!!