insight - Sankara Nethralaya Files/in072003.pdf · insight Vol. XXI No. 2 JULY 2003 ... Residents...
22
in sight Vol. XXI No. 2 JULY 2003 Scientific Journal of MEDICAL & VISION RESEARCH FOUNDATIONS 18, COLLEGE ROAD, CHENNAI - 600 006, INDIA Editorial Perspective — Intraocular lens power calculations after corneal refractive surgery — Srinivas K Rao Diplopia management with Fresnel prisms - a clinical experience — Dharani R, Meenakshi S, Jayarajini S, Sumita Agarkar and Sujatha Guha Needle Stick Injuries — A Mahalingam and P Suresh Kumar MUSCLE PUZZLE — Aarti Kabra and S. Meenakshi Last Page - Optical Coherence Tomography in Macular Disorders — Sachin Kabra and Pratik Ranjan Sen OCT picture of normal macula showing various layers of retina.
Transcript of insight - Sankara Nethralaya Files/in072003.pdf · insight Vol. XXI No. 2 JULY 2003 ... Residents...

insightVol. XXI No. 2 JULY 2003
Scientific Journal ofMEDICAL & VISION RESEARCH FOUNDATIONS
18, COLLEGE ROAD, CHENNAI - 600 006, INDIA
Editorial
Perspective — Intraocular lens power calculations after corneal refractive surgery— Srinivas K Rao
Diplopia management with Fresnel prisms - a clinical experience — Dharani R,Meenakshi S, Jayarajini S, Sumita Agarkar and Sujatha Guha
Needle Stick Injuries — A Mahalingam and P Suresh Kumar
MUSCLE PUZZLE — Aarti Kabra and S. Meenakshi
Last Page - Optical Coherence Tomography in Macular Disorders— Sachin Kabra and Pratik Ranjan Sen
OCT picture of normal macula showing various layers of retina.

26
Errors in DBR calculation can lead to disastrous results. This can leadto a situation that is difficult to explain away as a known complication andis one that is fraught with legal implications. The chances of such an errorincreases manifold in a patient who has undergone prior refractive surgery.Factors such as pre refractive surgery refractive error, error that has beencorrected with the refractive surgery, current refractive status of the eye areall factors having an implication in DBR calculation of these patients. Inaddition, these patients are who had undergone refractive surgery in the firstplace to get rid of their glasses and are unlikely to be happy if made to wearthick lenses once again after cataract surgery. We have an article in thePerspective section of this issue of Insight addressing this very importantissue.
Another area of concern for all medical professionals is the risk of beinginfected through a needle prick injury - something most of us would havebrushed aside as innocuous in the pre HIV days. An interesting article in thisissue gives us guidelines to prevent such an accident and also outlines whatto do next if such an accident were to occur.
Despite the availability of multiple modes to image the fundus such asthe indirect ophthalmoscope, fundus camera, fluorescein and indocyaninegreen angiograms, none could give us an in vivo histopathological section,that is until the OCT. The basics of the OCT, indications for its use inevaluation of fundus disorders are detailed in the last page of this issue.
Dr Mahesh P Shanmugam
Editor
EDITORIAL
CME PROGRAMMES FOR THE SILVER JUBILEE YEAR 2003
This Academic Year being the “Silver Jubilee Year” of Sankara Nethralaya attractsspecial significance and importance. Apart from the continuous efforts directed towardsimprovement of Patient’s Care and Patient’s Education on prevention and cure, thefoundation has also lined up various CME Programmes for Ophthalmologists andOptometrists for updating their skill and knowledge.
Sl.No. Topics Date1. Vitreo-retina 24th, 25th & 26th July 2003
2. Glaucoma 6th & 7th December 2003
The programmes are aimed to provide continuing medical education to the practisingOphthalmologists, Residents in Ophthalmology and to the Optometrists.
FOR MORE DETAILS, PLEASE CONTACT
Mr. N. SivakumarThe Academic Officer — SANKARA NETHRALAYA
18, College Road, CHENNAI – 600 006
Fax: 91-44-8254180 Email: [email protected]

27
Perspective:
Intraocular lens power calculations aftercorneal refractive surgerySrinivas K Rao
would result in an equivalent error in IOLpower, while a 0.33 mm error in axial lengthdetermination would cause a 1 D error in IOLpower in an eye of average axial length. Ineyes shorter than 22 mm, the magnitude ofthe error in IOL power estimation wouldincrease.
In RK, deep incisions in the peripheralcornea allow the intraocular pressure to shiftthe peripheral cornea outwards, resulting ina flattening of the central corneal curvature.There is thus, no tissue removal in thisprocedure, unlike in PRK and LASIK, in whichthe excimer stromal ablation results in tissueremoval from the central cornea. In the latterprocedures, tissue removal would depend onthe amount of myopic correction attempted.Based on a rule-of-thumb that 1 D ofrefractive correction requires the removal of10 µm of central corneal tissue, a 12 Dcorrection would require the removal of about120 µm of corneal tissue. Since mostauthorities consider 12 D the upper limit forsafe myopic refractive surgery, it is unlikelythat greater tissue removal would be seen inmost of these patients. Axial lengthmeasurement using non-contact ultrasoundtechniques and the IOL master, which usesthe principle of optical coherence, woulddetect this amount of tissue loss, whenmeasuring the axial length. Contactultrasound techniques may not have thesensitivity to detect this change and hencemay be a source of error in IOL powercalculations. This should lead to a 0.3 to 0.5Derror in IOL power estimation. Studies of IOLpower calculation in eyes that have undergonecorneal refractive surgery have however,indicated that most of the error that occursresults from inaccurate estimation of thecorneal power.
Cataract surgery has evolvedtremendously in the past few decades and iscurrently considered a refractive procedurewith most patients expecting excellent unaidedvision following the procedure. Present daytechniques of phacoemulsification, whichdisturb the corneal contour minimally andensure in-the-bag intraocular lens (IOL)placement in a consistent fashion, havecontributed to such results. An improvedunderstanding of the methods used for IOLpower calculation and the precision of currenttechnologies used to measure axial length andcorneal curvature has also contributed to theincreased accuracy of cataract surgery.
Another procedure, which has gainedtremendous popularity in recent years, isexcimer laser corneal refractive surgery andit is currently the second most commonlyperformed ocular surgical procedure. Althoughlaser in situ keratomileusis (LASIK) is themost advocated procedure, a large number ofpatients have undergone photorefractivekeratectomy (PRK) and radial keratotomy (RK)in the past. Most of these refractive procedureshave been performed in patients in theirsecond to fourth decades, and as theseindividuals age they will need cataract surgeryas well. However, initial attempts resulted inpoor refractive predictability following cataractsurgery in these eyes. The purpose of thisarticle is to highlight the reasons for suchpoor outcomes, and to review the methodsdescribed to overcome these problems.
The problem
The two most important measurementsthat aid accurate IOL power calculation arethe axial length of the eye and the cornealcurvature. Their importance is highlighted bythe fact that an error of 1 D in keratometry

28
uses for image formation. This results in anunderestimation of the IOL power and apostoperative hyperopic refractive error. Thisis the main source of error in eyes that haveundergone RK. In PRK and LASIK, in additionto this error, the alteration in the relationshipbetween the anterior and posterior cornealsurfaces introduces a second error whencorneal power is calculated from the measuredradius of curvature.
The solution(s)1. Corneal topography - The explanation
in the previous paragraph indicates whystandard keratometry results in poor refractiveoutcomes after IOL implantation in eyes thathave had corneal refractive surgery. Most ofthe currently available computerized video-keratography units provide color-coded mapsof corneal power distribution. The basicprinciples adopted by the Placido-baseddevices remain very similar to those in manualkeratometers. Hence they are subject to theinaccuracies described earlier. However, inpost-RK eyes, some degree of accuracy canbe attained by ignoring the simulatedkeratometry values provided by the machine(measured from a 3 mm zone), and derivingthe value from the center of the zone offlattening indicated in the topographic map.This is more accurate since these devices usedata from more points on the corneal surface,including the cornea within the 3 mm zonemeasured by the keratometer. This methodwould not however be useful in eyes that havehad excimer surgery, due to the inaccuracyin conversion mentioned earlier.
2. The History method - This methodderives the post-refractive surgerykeratometric value from the pre- and postsurgery refractive data of the patient. Thiscan be explained with the help of an example,
Data
Preoperative refraction = - 8 D
Preoperative keratometry = 44 D
Refractive correction attempted = - 8 D
Post-LASIK refraction = - 1 D
Standard keratometry makes certainassumptions regarding corneal shape. Thecornea is considered a regular sphero-cylindrical surface, and the measurement ofits curvature is derived from points situatedon a central circle which is about 3 mm indiameter. Since the central cornea within thiszone is considered to be a spherical surface,this measurement is assumed to represent thepower distribution within this area and at thecorneal apex. Since keratometers use thereflection of a target from the anterior cornealsurface, what is measured is the curvature ofthe anterior corneal surface. Refraction at theposterior corneal surface results in a negativepower, and the overall power of the cornea isthe algebraic sum of these two components.Since the posterior corneal power cannot bemeasured using standard keratometrictechniques, manufacturers use a modificationin the refractive index of the cornea to accountfor this factor. Hence, most keratometers usea corneal refractive index of 1.376 instead ofthe true value of 1.3375. This allows aconversion of the measured radius ofcurvature of the anterior surface to the totalpower of the cornea. For this assumption tobe valid however, a constant relationshipbetween the anterior and posterior cornealsurfaces is assumed. This assumption isviolated in excimer refractive surgery, in whichtissue is removed from the anterior cornealsurface. This would therefore, further affectthe accuracy of conversion of the measuredanterior radius of curvature into corneal powerin such eyes.
Since the shape of the cornea afterrefractive surgery, be it RK or excimer surgeryis oblate - meaning that there is a negativeshape factor or central flattening, measure-ment of the paracentral cornea results in anerroneously steeper value for the centralcorneal power. This error is enhanced by thefact that the flat post-refractive surgery corneareflects the target of the keratometer from alarger central area. Thus, after RK and excimersurgery for myopia, the measured cornealpower in the 3 to 4 mm zone is steeper thanthat in the central cornea, which the patient

29
allows refraction and the patient has a best-corrected visual acuity of at least 6/18 (toensure that the refraction is accurate). If thecataract is very dense or total, and accuraterefraction is not possible, or if the visualacuity in the cataractous eye cannot beimproved beyond 6/24, then the accuracy ofthis method is open to question.
4. Intraoperative retinoscopy - In thistechnique, cataract surgery is completed andretinoscopy is performed intraoperatively inthe aphakic eye. From the aphakic refraction,the IOL power can be determined.Alternatively, the IOL chosen can be implantedand then retinoscopy is performed, althoughIOL exchange would be necessary if there wasa significant error. It would also be necessaryto consider the loss of aseptic technique thatmay occur during this intraoperativemaneuver. Lastly, this technique would beinappropriate in eyes that have had refractivesurgery for hyperopia as even minorinaccuracies in the working distance duringretinoscopy could result in serious errors inIOL power.
5. The DBR method - This is the mostrecently described method, and in thisapproach, preoperative patient data isessential. When the patient presents forrefractive surgery, in addition to refractionand keratometry, the axial length is alsomeasured and the IOL power required foremmetropia is calculated. Following refractivesurgery, the stable refractive error prior toonset of cataract is determined and the changein refraction effected by the surgical procedureis calculated. This can be explained with theaid of the following example,
DataPreoperative refraction = - 5.25 DPreoperative keratometry = 46.2 DAxial length = 25.0 mmIOL power for emmetropia
= 16.8 D (A constant 118.0)
Refractive correction attempted = - 5.25 DPost-treatment refraction = Plano
Calculations
Refractive error corrected = 7 D
Hence, post-LASIK keratometry= (44 - 7) = 37D
This method uses the post-treatmentrefractive error of the patient, prior to thedevelopment of the cataract. This is usuallyobtained one month after LASIK, whenrefractive stability has been attained. Sincethe change in refractive error is the directresult of the corneal alterations produced bythe surgical procedure, it is logical to derivethe final corneal power by subtracting therefractive change attained from the pre-treatment refractive error. Although thismethod works fairly well, it requires accessto patient data in the pre- and early post-treatment periods. Details of the surgicalprocedure, including the correction attemptedare also important.
3. The Hard contact lens method - Inthis technique, a hard contact lens of knownbase curve is placed on the eye with lenschanges, and refraction is performed. Thesubjective refraction with the contact lens inplace is compared with the refraction obtainedwithout the contact lens. These values areused to derive the corneal power, using thefollowing relationship,
Keratometry (D) = Contact lens base curve(D) + contact lens power (D) + (refractionwith the contact lens) - (refraction withoutthe contact lens)
The rationale of this method can be betterexplained with an example. If refractionwithout the contact lens (base curve 38 D) is- 5.0 D, and with the contact lens in place isplano, it means that the cornea underlyingthe lens is steeper than the contact lens by 5D. Hence the corneal power would be contactlens power plus 5 D (assuming that thecontact lens power was zero). Thus,
Keratometry= 38 + 0 + (0) - (- 5) = 38 + 5 = 43 D
This method is advantageous because itdoes not require access to patient data.However, it is accurate only if the cataract

30
result in more accurate refractive outcomesfollowing cataract surgery and IOLimplantation, in patients who have hadcorneal refractive surgery.
References
1. Celikkol L, Pavlopoulos G, Weinstein B,Celikkol G, Feldman S. Calculation ofintraocular lens power after radialkeratotomy with computerized video-keratography. Am J Ophthalmol 1995;120:739-50.
2. Holladay JT. Consultations in refractivesurgery. Refract Corneal Surg 1989;5:203.
3. Hoffer KJ. Intraocular lens powercalculation for eyes after refractivekeratotomy. J Refract Surg 1995; 11:490-3.
4. Feiz V, Mannis MJ, Garcia-Ferrer F,Kandavel G, Darlington JK, Kim E, CasparJ, Wang JL, Wang W. Intraocular lenspower calculation after laser in situkeratomileusis for myopia and hyperopia.Cornea 2001;20:792-7.
5. Seitz B, Langenbucher A. Intraocular lenspower calculation in eyes after cornealrefractive surgery. J Refract Surg 2000;16:349-61.
Since there has been a 5.25 D change inrefraction at the spectacle plane followingsurgery (12 mm vertex distance), the IOLinside the eye should have its power increasedby an equivalent amount, for the post-refractive surgery eye to attain emmetropia.It is also calculated that for every diopter ofchange in IOL power, only 0.7 D of change inrefraction at the spectacle plane will beachieved.
Calculations
5.25 D change at the spectacle plane= 5.25 / 0.7
= 7.5 D change at the IOL plane
IOL power for emmetropia= 16.8 D + 7.5 D = 24.3 D
This technique also requires access topre- and post-operative patient data. Sincethis is a common requirement for many ofthe techniques described above, it is importantfor refractive surgeons to maintain detailedrecords. It may also be prudent to provide allpatients undergoing refractive surgery with acopy of the relevant data, in case theyapproach another ophthalmologist for cataractsurgery. Attention to the above details andadoption of the techniques described can
SANKARA NETHRALAYACHENNAI
SIR RATAN TATA TRUST COMMUNITYOPHTHALMOLOGY FELLOWSHIP PROGRAMME
August / October / December 2003CATARACT MICROSURGERY FELLOWSHIP (Basic & Advanced) - 2months duration.A registered Medical Practitioner with Post Graduate Diploma or Degree in Ophthalmologycan apply.
Bio DataProvide all useful information about yourself in plain paper and send it to theundersigned.
InterviewCandidates called for interview need to appear for MCQ / personal interview at theirown cost. Rush application indicating the batch required. Fordetails write to :
Academic Officer, MEDICAL RESEARCH FOUNDATION , 18, College Road,Chennai - 600 006. Fax : 044-28254180 e-mail : [email protected]
Bio Data & Application can be faxed or e-mailed or sent by speed post.
31
Diplopia is one of the most troublesomevisual symptoms that a patient canexperience, as it interferes with the ability toperform any visual task. Ocular misalignmentis the commonest cause of binocular diplopia.
Fresnel prisms are excellent option fornon-surgical management of diplopia 1-4. Wepresent three cases of ocular misalignmentleading to diplopia, which was relieved withFresnel prisms.
Case 1
An 18-year-old male reported with ahistory of blunt trauma in right eye with avisual acuity of 3/60 and <N36. The visualacuity was 6/6 and N6 in the left eye. Anteriorsegment was normal in both eyes, except forangle recession in superior and nasalquadrants in the right. Fundus examinationshowed a partial rhegmatogenous retinaldetachment in right eye for which the patientunderwent scleral buckling.
Post operatively, visual acuity improvedto 6/12; N6 with myopic correction, but thepatient was complaining of binocular diplopia.Extra ocular movements were full in both eyes.Alternate prism cover test revealed rightexotropia of 45-prism dioptres. The patientunderwent squint surgery following whichthere was a residual exotropia of 30-prismdioptres. This undercorrection may sometimesbe seen in sensory strabismus. The patientwas referred to Orthoptic clinic for trial ofFresnel prism.
On trial, diplopia was minimized with 20-prism dioptres. After adequate adaptation withprism for fusion in free space patient wasfitted with 20-prism dioptres as Fresnel prismin right eye and was advised to come for afollow up after 3 months.
Diplopia management with Fresnel prisms -a clinical experienceDharani R, Meenakshi S, Jayarajini S, Sumita Agarkar and Sujatha Guha
Follow up
At 10 months follow-up, the patient wasusing Fresnel prism without any diplopia oreyestrain. On examination, his visual acuitywas 6/18, N6 in right eye and 6/6, N6 in lefteye. Cover test revealed exophoria for distanceand orthophoria for near.
Case 2
A 31-year-old male reported with ahistory of blunt trauma to the right eye witha visual acuity of perception of light withinaccurate projection. The visual acuity was6/9 and N6 in the left eye. Anterior segmentexamination revealed traumatic rupture oflens, corneal tear and edema and hyphemain right eye and the patient underwentprimary wound repair and lensectomy.
Post-operatively visual acuity improvedto 6/24 with aphakic correction. The patientwas fitted with semi soft contact lens, whichimproved visual acuity to 6/9. However patientwas complaining of diplopia with contact lens.Extra ocular movements were full in both eyes.Alternate prism cover test revealed rightexotropia of 20-prism dioptres and hypotropiaof 2-prism dioptres this cause of which wassensory. Patient was referred to Orthopticclinic for a trial of Fresnel prism.
On trial, diplopia was minimized with 15-prism dioptres base in. After adequateadaptation with prism for fusion in free space,patient was fitted with 15-prism dioptres basein as Fresnel prism in right eye and wasadvised to come for a follow up after 3 months.
Follow up
At 3 months follow-up, the patient wasusing Fresnel prism without any difficulty.On examination, the visual acuity was 6/9and N6 in right eye and 6/6 and N6 in left

32
The major disadvantages are blurring ofvision, decreased contrast sensitivity due toscattering of light, colored fringes, visibilityof the grooves, discoloration and peeling ofprism membrane7 from the glasses. Contrastsensitivity function is reduced for all spatialfrequencies, to a greater degree at higherspatial frequencies 7.
The main advantages of Fresnel prismsare reduced weight (approximately 1mmthickness), large diameter (67 mm), which canfit into any frame shape and ease ofapplication. Fresnel prisms producesubstantially less horizontal and verticalmagnification of objects and less curvature ofvertical lines 8. On comparison withconventional prisms, visually insignificantdifference has been reported for asymmetrichorizontal magnification and change of verticalmagnification with horizontal angle8.
None of our patients complained ofblurred vision since the Fresnel prism wasfitted in front of the non-dominant eye, sothat clear vision was maintained through thebetter eye. One patient (case 2) complained ofscattering of light in outdoors and two patients(case 1 and case 3) complained of discolorationof prism membrane. One patient (case 2)reported that the grooves were noticeable byothers. None of the patients complained ofcolored fringes or peeling of the prismmembrane.
Conclusion
Fresnel prisms can be considered as ashort term or long-term treatment option fordiplopia and are more successful in achievingsingle binocular vision in cases where surgerymay not be beneficial.
References
1. M Flanders, N Sarkis. Fresnel membraneprisms: clinical experience. Can JOphthalmol 1999; 34: 335-40.
2. S M Brown. Fresnel prism treatment ofsensory exotropia with restoration ofsensory and motor fusion. J CataractRefract Surg 1999; 25: 441-443.
eye. Cover test revealed exophoria for distanceand orthophoria for near.
Case 3A 47-year old man reported with
decreased vision in left eye. On examinationthe visual acuity was 6/9 and N8 in right eyeand perception of light with inaccurateprojection in left eye. Anterior segments werenormal in both eyes. Fundus examinationrevealed partial rhegmatogenous retinaldetachment in left eye. The patient underwentscleral buckling which was uneventful.
Post-operatively the visual acuityimproved to 6/18 and N8 in left eye, but thepatient complained of binocular diplopia fordistance and near. Alternate prism cover testrevealed left exotropia of 12-prism dioptresand hypotropia of 20-prism dioptres. Thepatient was referred to optometry clinic forprescription of Fresnel prism. On trial, thepatient was able to fuse diplopic images with10-prism dioptres base in and 15-prismdioptres base down. The patient wasprescribed with 10-prism dioptres base in asground in prism and 15-prism dioptres baseup as Fresnel prism in left eye.
Follow up
At 10 months follow up, the patient wassuccessfully using the Fresnel prism fordistance and was keen on Fresnel prism fornear vision. On examination, the visual acuitywas 6/9 and N8 in right eye and 6/18 andN6 in left eye. Prism bar cover test revealedorthophoria for distance and 10 prism dioptresof left hypotropia. The patient was prescribedwith 10-prism dioptres base up for near.
Discussion
Fresnel prisms are reasonable permanenttreatment option for diplopia managementwhen large prisms cannot be incorporated inspectacles. Fresnel prisms can be prescribedin sector, often referred to as sectorapplication of Fresnel prism in cases ofincomitant deviations, when the magnitudeof deviation is expected to change withtime5,6,7 .

33
3. J Wylie, M Henderson et al., Persistentbinocular diplopia following cataractsurgery: etiology and management. Eye1994; 8 (5): 543-6.
4. D A Bader. Fresnel prism for constantdiplopia. Am J Optom Physiol Opt 1983 ;60 (5): 410-1.
5. J M Sinelli, M X Repka. Prism treatment ofincomitant horizontal deviations. AmOrthopt J. 1996; 46: 123-26.
6. B J Kushner. Management of diplopia
limited to down gaze. Arch Ophthalmol.1995; 113 (11): 1426-30.
7. Cotter S A, Frantz K A. Practicalconsiderations in prism implementation.Cotter S A and London R (ed): In Clinicaluses of prism 1st ed. St. Louis: Mosby;1995: 64-71.
8. A J Adams, R J Kapash and E Barkan.Optical performance and optical propertiesof Fresnel membrane prisms. Am J OptomArch Am Acad Optom 1971; 48: 289-297.
AN APPEALA lot of things in this world depend on money - security, shelter, education and evenhealth. But at Nethralaya, money has ceased to be a pre-requisite for sight.Day after day, year after year, Nethralaya treats hundreds of patients absolutely freeof cost and gives them back their sight. Treatment is provided free of cost to allpatients with a monthly income below Rs.1,750/-.Yet there is no discrimination between the free patient and the one who pays. Apartfrom the treatment, food, medicines and travel expenses are absolutely free.Those free patients depend on Nethralaya, and Nethralaya depends on you.So, come and join the OPHTHALMIC MISSION TRUST.For questions about tax exempt status and contributions, please contact:
Mr S V Acharya,Treasurer
Ophthalmic Mission Trust Inc. (OM Trust)14613, Pommel Drive, Rockville,
MD 20850, U.S.A.Phone: (301)251 0378
INTERNET e-mail : [email protected]
For those of you in India and elsewhere, please contact:Dr S S Badrinath,
President & ChairmanSankara Nethralaya
(UNIT OF MEDICAL RESEARCH FOUNDATION)18 College Road, Chennai 600 006
Phone: 826 1265, 827 1616Fax: (044) 825 4180, 821 0117
INTERNET e-mail : [email protected] US UP ON THE WEB at http://www.sankaranethralaya.org
http://www.omtrust.orgGIVE ONLINE @ www.icicicommunities.org
COME, GIVE THE GIFT OF SIGHT
34
Needle Stick InjuriesA Mahalingam and P Suresh Kumar
Introduction:
Needle stick injuries are wounds causedby needles that accidentally puncture theskin. Needle stick injuries are a hazard forpeople who work with hypodermic syringesand other needle equipment. These injuriescan occur at any time when people use,disassemble, or dispose needles. When notdisposed properly, needles can becomeconcealed in linen or garbage and injure otherworkers who encounter them unexpectedly. Aneedle stick injury can be a devastating event.Although the risk of contracting blood-bornepathogen is low, the psychological trauma thatfollows the injury can be disabling in certainsituations.
Hazards of Needlestick InjuriesAccidental punctures by contaminated
needles can inject hazardous fluids into thebody through skin. There is potential forinjection of hazardous drugs, but injection ofinfectious fluids, especially blood, is by farthe greatest concern. Even small amounts ofinfectious fluid can spread certain diseaseseffectively. The pathogens that pose the mostserious health risks arel Hepatitis B virus (HBV)l Hepatitis C virus (HCV)l Human immuno deficiency virus (HIV)
Needle stick injuries have transmittedmany other diseases involving viruses,bacteria, fungi, and other microorganisms tohealth care workers and laboratoryresearchers in rare, isolated events.
How Do Needlestick Injuries Occur?
Several studies show that needles causeinjuries at every stage of their use,disassembly, or disposal. But there isdisagreement as to why the accidents are socommon among health care workers or whysimple solutions fail to solve the problem.
Nursing and laboratory staff usuallyexperience 30 to 50 percent of all injuriesduring clinical procedures. Equipment design,nature of the procedure, condition of work,staff experience, recapping, and disposal hasall been mentioned as factors that influencethis occurrence.
1. Equipment Design:
Safer innovative devices using protectedneedle devices or needle-free systems withself-sealing ports would alleviate many ofthese injuries. There is accumulatingevidence suggesting that syringes withsafety features reduce needle stick injuries.
2. Nature of Procedure:
l while withdrawing a needle from anuncooperative patient
l a needle out of the rubber stopper of avacuum tube which can jab the hand in arebound reflex
Injuries commonly occur when workers tryto do several things at the same time,especially while disassembling or disposingoff needles.
3. Conditions of Work:
Work conditions that might contribute toan increase in the number of needle stickinjuries include:
l staff reductions where nurses, laboratorypersonnel and students assume additionalduties
l difficult patient care situations inemergency conditions
l working at night with reduced lighting.
4. Staff Experience:
New staff or students tend to have moreneedle stick injuries than experienced staff.
35
5. Recapping:
Recapping can account for 25 to 30 percentof all needle stick injuries of nursing andlaboratory staff. Often, it is the single mostcommon cause. It is extremely dangerousto hold a needle in one hand and attemptto cover it with a small cap held in theother hand. Injuries occur three differentways:
l the needle misses the cap and accidentallyenters the hand holding it
l the needle pierces the cap and enters thehand holding it
l the poorly fitting cap slips off of a recappedneedle and the needle stabs the hand.
6. Improper Disposal:
Virtually all needle stick injuries ofdomestic and conservancy staff are fromneedles that have either been lost in theworkplace or thrown into regular garbage.Janitors and garbage handlers can alsoexperience needle stick injuries or cutsfrom “sharps” when handling trash thatcontains needles or scalpels. This can beattributed to forgetfulness or lack ofmotivation or training on the part of peoplewho work with and dispose off needles.Inconvenient disposal systems alsocontribute to these incidents. Maintenancestaffs have also experienced needle stickinjuries when they clean ducts or otherareas with their hands and fond hiddenneedles and syringes. These injuriesusually happen when the maintenancestaffs reach into areas they cannot see andare not wearing leather gloves.
How to Prevent Needlestick Injuries?
Preventing needle stick injuries is themost effective way to protect workers fromthe infectious diseases that needle stickaccidents transmit. A comprehensive needlestick injury prevention program wouldinclude:
1. Employee Training & Education:
Proper education of employees about the
importance of following universalprecautions, using disposal methods,including recommended disposalcontainers, prompt emptying of disposalcontainers before they overflow and usingpreventive devices are essential elementsof a program to minimize the needle stickinjuries. Specifically, the training programsshould address:
l risk of injury
l potential hazards
l recommended precautions for use anddisposal of needles
l procedures for reporting injuries
l the importance of hepatitis B vaccinationwhere appropriate.
The effectiveness of the training should beassessed on their understanding andknowledge, observing actual practice andmonitoring the frequency of incidents.
2. Recommended Guidelines:
The following guidelines deal specificallywith needle safety:
l needles, scalpel blades and other sharpinstruments- workers should considerthese as potentially infectious andhandle them with care to preventaccidental injuries
l disposable needles and syringes, scalpelblades, and other sharp items- workersshould place these in puncture-resistantcontainers located near the area of use.They should avoid overfilling thecontainers because accidental needlestick injuries may occur
l recapping- workers should not recapneedles by hand or purposely bend,break, or remove them from disposablesyringes or otherwise manipulate themby hand.
3. Safe Recapping Procedures:
In situations where recapping is considerednecessary, safe approaches should befollowed. Workers should never move an

36
exposed needle tip towards an unprotectedhand.
a. Single-Handed Scooping
Recapping can be safe when people laythe cap on a flat surface and scoop itonto the tip of a syringe held in onehand. They must keep the free handaway from the sheath and well behindthe exposed needle.
b. Recapping Devices
Several devices are available forrecapping needles safely. Some devicespermit single-handed recapping byparking a needle cap on a flat surface.Other devices are designed to protectthe hand that holds the cap during two-handed recapping procedures.
4. Effective Disposal Systems:
An effective system for disposing off usedneedles is crucial to preventing needle stickinjuries. Having disposal containers readilyavailable can greatly reduce the concernfor recapping needles. Workers shouldplace needles in wide-mouth, puncture-proof containers. Locating disposalcontainers specifically where needles haveto be disposed safely without recapping andreplacing the containers before they arecompletely filled and making sure that thecontainers are sealed, collected, anddisposed of in accordance with localregulations for biomedical waste would bean ideal way of disposing off used needles.All staff should report every incident inwhich they find needles left at the bedsideor thrown into the regular garbage.Through careful selection of sharpsdisposal products, (access design, size,etc.), their appropriate placement withinall healthcare settings, and with certainsafe disposal practices for Health CareWorkers and facilities, risk of sharps injurycan be reduced. The risk of needle stickscan be reduced by using new sharps wastetreatment technologies near the point ofuse, or sharps collection followed bytreatment in an on-site non-incineration
technology, or sharps collection andtransport to an off-site treatment facility.
5. Safer Needle Devices:
Safer needle devices have built-in safetycontrol devices, such as those that use aself-sheathing needle, to help preventinjuries before, during, and after usethrough safer design features. There aredifferent types of safety features that areavailable for safer needle devices such as:
¡ Passive safety features: remain in effectbefore, during and after use.
¡ Active devices: require the worker toactivate the safety mechanism.
¡ Integrated safety design: have a safetyfeature that is built in as an integralpart of the device and cannot beremoved. This design feature is usuallypreferred.
¡ Accessory safety devices: have safetyfeatures that are external to the deviceand must be carried to, or betemporarily or permanently fixed to, thepoint of use. This design is dependenton employee compliance and accordingto some researchers, is less desirable.
Desirable Characteristics of Safety Devicesshould include:
¡ The device is needle less.
¡ The safety feature is an integral part ofthe device.
¡ The device is easy to use and practical.
¡ The device performs reliably.
¡ The safety feature cannot be deactivatedand remains protective through disposal.
¡ The devices work effectively and reliably,and are acceptable to the health careworker, and do not adversely affectpatient care.
The immediate measures to be taken after anoccupational exposure are as follows:
l Use soap and water to wash any wound orskin site that came into contact with

37
as PEP found that the risk of HIV infectionwas reduced by approximately 81%. Althoughthe efficacy of combination regimens for PEPis unknown, combination drug regimens arecurrently recommended for PEP. This isbecause they are more potent and may bemore effective against drug-resistant strains.
Possible side effects of PEP
Information about the toxicity ofantiretroviral drugs in persons without HIVinfection is limited. Health care workers whoare given PEP need to be monitored for drugtoxicity at baseline (on starting PEP), and twoweeks after therapy begins. They should beadvised to report acute illness and symptomssuch as back or abdominal pain, pain orurination, blood in the urine, increased thirstand frequent urination. If these symptomsare reported, they must be evaluatedimmediately.
Nausea and diarrhoea often occur duringthe course of treatment. Prescribingantimotility and/or antiemetic agents or othermedications for specific symptoms may enablethe exposed health care worker to completePEP without changing the regimen.
What additional advice should the exposedhealth care worker be given?
Exposed health care worker should avoidbehaviors that carry a risk of secondarytransmission of HIV for the duration of thefollow-up period. This is especially true forthe first 6 to 12 weeks after exposure, whenseroconversion is most likely to occur:
The exposed health care worker shouldbe advised on the following:
l Sexual abstinence
l Use of condoms to prevent sexualtransmission and pregnancy
l Not to donate blood, plasma, organs, tissueor semen
l HIV and some drugs used in therapy canpass through breast milk. Considerdiscontinuing breast-feeding, particularlyafter high-risk exposures.
infected blood or fluid.
l Flush exposed mucous membranes withwater.
l Irrigate an open wound with sterile salineor disinfected infection.
l Eyes should be irrigated with clear water,saline or sterile eye irrigates.
l Report to the concern authority
l Counseling
l Use antiretroviral therapy in case of HIVneedle stick injuries
Post-exposure prophylaxis in HIV needlestick injuries
l The term “Post-exposure prophylaxis” (PEP)refers to the treatment of occupationalexposures using anti-retroviral therapy.The rational is that antiretroviral treatment,which is started immediately after exposureto HIV, may prevent HIV infection.
Current guidelines for PEP
The currently recommended guidelinesstate that
l Therapy should be recommended afterexposure.
l All regimens must include zidovudine.
l Therapy should be initiated within one totwo hours of exposure.
l If the source patient's HIV status isunknown, decision to give PEP should betaken on a case-to-case basis.
l Follow-up counseling and HIV testingshould be carried out periodically for atleast 6 months (i.e. at baseline, 6 weeks,12 weeks and 6 months). It is estimatedthat 95% of health care workers seroconvertwithin 6 months of exposure.
Efficacy of PEP regimensStudies conducted in animals and in
humans prove the efficacy of PEP regimens.Zidovudine has been the most widely studiedagent for prophylaxis. A retrospective studyof health care workers who used zidovudine

38
2. William Sharney, Hand book of ModernHospital Safety, Lewis publishers, USA1999: 253-378.
3. Edwards C R W, Bouchier I A D, HaslettC, Chilvers E R, Davidson's Principles &Practice of Medicine, 17th Edition,Churchill Livingstone, UK 1995 : 89.
4. David Greenwood, Richard C B Slack,John Forrest Peutherer, MedicalMicrobiology, 14th Edition, ChurchillLivingstone, UK, 1992:637-38.
Suggested Browsing:
1. http://www.australianprescriber.com
2. http://www.ofaaa.bc.ca
3. http://www.lambtonhealth.on.ca
4. http://www.cdc.gov
5. http://www.medscape.com
CONCLUSIONS
Needle stick injuries are an importantand continuing cause of exposure to seriousand fatal diseases among health care workers.Greater collaborative efforts by all teammembers are needed to prevent needle stickinjuries and the tragic consequences that canresult. Such efforts are best accomplishedthrough a comprehensive program thataddresses institutional, behavioral and devicerelated factors that contribute to theoccurrence of needle stick injuries in healthcare team. Critical to the effort are theelimination of needle bearing devices wheresafe & effective alternative are available andthe development, evaluation and use of needledevices with safety features.
Suggested Reading:
1. Biswas J, Ocular Lesions in AIDS In India,(Ist ed), Sankara Nethralaya, Chennai,2001:42-49
Basic and expanded post exposure prophylaxis regimens

39
MUSCLE PUZZLEAarti Kabra and S. Meenakshi
Patient no: 1: (figure 1a, 1b, 1c, 1d )
Fig.1a Fig.1b
Fig.1c Fig.1d
This is a 42 year old patient presenting with progressive inward turning of left eye
H/O Scleral Buckling in left eye 10 yrs back.
Vision: OD: 6/24, N6
OS: HMCF, < N36
Refraction: OD: - 21.00 DS
OS: - 22.00 DS/ -1.00 DC @ 90
Ocular motility : 30 LET (Hirschberg's test) with bilateral abduction deficit
40
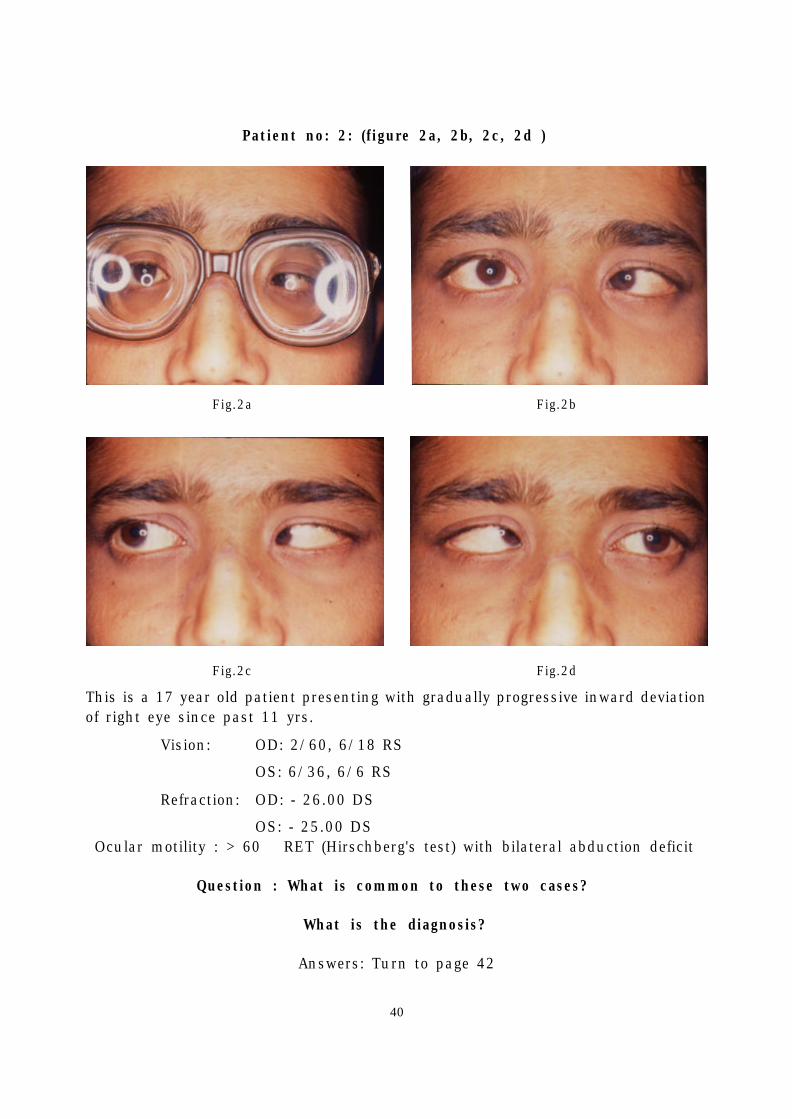
Patient no: 2: (figure 2a, 2b, 2c, 2d )
Fig.2a Fig.2b
Fig.2c Fig.2d
This is a 17 year old patient presenting with gradually progressive inward deviationof right eye since past 11 yrs.
Vision: OD: 2/60, 6/18 RS
OS: 6/36, 6/6 RS
Refraction: OD: - 26.00 DS
OS: - 25.00 DSOcular motility : > 60 RET (Hirschberg's test) with bilateral abduction deficit
Question : What is common to these two cases?
What is the diagnosis?
Answers: Turn to page 42

41
Registration fee details
Delegates – Rs 1500/-
#PGs – Rs 750/-
Foreign delegates – US $100
Last Date for Registaration :31-10-2003
Late fee for Registration
Delegates – Rs 2000/-
#PGs – Rs 1000/-
@ Registration forms are available on linefor print atwww.sankaranethralaya.org andwww..ekalavya.org
# PGs need to send proof of postgraduatestatus
Mailing address :
Dr B ShanthaMedical Research Foundation18, College Road,Chennai, TamilNaduPhone:28271616 Ext. 1434Fax:044-28254180email: [email protected]: http://www.sankaranethralaya.org,
http://www.ekalavya.org
FACULTYInternationalDr Ivan Goldberg (Australia)Dr Jost B Jonas (Germany)Dr Michal Schwartz (Israel)Dr Steve Seah & Team (Singapore)
NationalDr G Chandra Shekar (Hyderabad)Dr Pradeep Vyas (Jalna)Dr Prafulla Sarma (Guwahati)Dr Ramanjit Sihota (New Delhi)Dr S Ramakrishnan (Tirunelveli)Dr Vinay Nangia (Nagpur)
SN Faculty
HIGHLIGHTS
Newer imaging tools - Where to use them?
Newer medications – How do we use them?
Neuroprotection – Is it here?
Angle Closure glaucoma – What is new?
Case discussions
Symposium on Epidemiology
Posters from participants
Note: Abstracts for poster presentationsin the CME may be sent by email in thefollowing format :
Title, Aim, Methods, Results andConclusion (150 words).
Last date 31 -10 - 2003.
GLAUCOMA 2003 UPDATEDear Colleagues,
Cutting edge research in glaucoma has produced a plethora of new diagnostictechniques and therapeutic options. One question about this bewildering assortmentof tests and drugs is their relevance to clinical practice. We have national andinternational experts with experience in these fields to put things in perspective at ourCME programme on 6th and 7th December 2003.
We invite you to block your calendar this December and join us in Chennai for anupdate.
Dr B Shantha, Organising Secretary

42
Esotropia has been described inassociation with high myopia. It can presentin various forms. It can be comitant orincomitant.
1) Acquired Strabismus fixus has beendescribed in conjunction with highmyopia. 1
The postulated theory suggests that thereis fibrosis of the medial rectus musclesecondary to lateral rectus paralysis. Theinvolved eye is fixed in the adductedposition and cannot be moved. This canreach extreme form in which the corneaalso is not seen in the palpebral fissure.Forced Duction Test helps in diagnosis.
Management:
Complete disinsertion of the medial rectusmuscle(s) along with resection of the lateralrectus muscle and recession of theconjunctiva and the Tenon's capsule.
2) Another form of strabismus with highmyopia is the Heavy eye syndrome , whichconsists of a slow progressive developmentof esotropia and hypotropia. 2 Downwarddisplacement of the lateral rectus has beennoted in these eyes. It is thought to be dueto scleral ectasia, which causes a downslipof the muscle in relation to the globe. Thiscauses a depressing effect. This can beconfirmed by MRI scan.3
Management:Supratransposition of the resected lateralrectus muscle along with recession of
ANSWER: Esotropia and high myopia with abduction deficit
Fig. 1a, Fig. 2a: Patient is wearing high minus glasses
Fig. 1b, Fig. 2b: Primary gaze showing large esotropia
Fig. 1c, Fig. 2c: Right gaze - limitation of abduction in the right eye
Fig. 1d, Fig. 2d: Left gaze - limitation of abduction in the left eye
Esotropia in High Myopiamedial rectus muscle has been described.This can be augmented with scleral fixationof the transposed muscle with silicon loop.4
But the results are not satisfying.
3) Progressive strabismus in the form ofrestrictive motility disturbances has beendescribed in high myopia. Various causesspeculated include:
1. Disproportion between the size of theorbit and the enlarged or elongatedmyopic globe and contact between theelongated globes and the orbital wallsand apices of the orbit.5
2. Compression of the lateral rectus againstthe lateral orbital wall by an enlargedglobe.
3. Progressive fibrosis, myopathy, ormyositis
4) Acute Acquired Comitant Esotropia 6 hasalso been described with myopia. This iscalled as the Bielschowsky type and isassociated with high myopia and constantdeviation both for distance and near. Thesepatients usually begin with a small angleand gradually progress to a large deviation.However there is no evidence of lateralrectus paralysis. Some of these cases maydemand neuroimaging to rule out anyintracranial pathology.
Theories proposed for this type are:
1. Increased tone of medial rectus muscle
2. Direct damage to the lateral rectus muscle.

43
Management:
Surgery is usually effective in re-establishing good binocular function.
References:
1. Prakash P, Gupta NK, Menon V, ChandraM: Myopic strabismus fixus convergens.Indian J Ophthalmol 1989; 37: 24 - 26.
2. Aydin P, Kansu T, Sanac AS: High myopiacausing bilateral abduction deficiency. JClin Neuro Ophththalmol 1992; 12: 163 -165.
3. Krzizok T, Kaufmann H, Traupe H:Elucidation of restrictive motility in highmyopia by magnetic resonance imaging.Arch Ophthalmol 1997; 115: 1019 - 1027.
4. Krzizok T, Kaufmann H, Traupe H: Newerapproach to strabismus surgery in highmyopia. Br. J Ophthalmol 1997; 81: 625- 630.
5. Demer JL, Noorden Von GK: High myopiaas an unusual cause of restrictive motilitydisturbance. Surv Ophthalmol 1989; 33:281 - 284.
6. Creig S Hoyt, William V Good: Acute onsetconcomitant esotropia: when is it a sign ofserious neurological disease? Br JOphthalmol 1995; 79: 498 - 501.
(contd. from page 46)
Assessment of retinal architecturerequires knowledge of the OCT features of anormal eye. It is illustrated in figure 1. Ahighly reflective red layer present inferiorly,corresponds to the retinal pigment epithelium(RPE) and choriocapillaris. The contrastbetween this red layer and neural retinacreates a reproducible boundary for measure-ment of neurosensory retinal thickness. Thedark layer immediately anterior to the RPE /choriocapillaris represents the photoreceptorouter segment. The middle retinal layersexhibit moderate backscattering. Retinalblood vessels are noted by their shadowingof deeper retinal structures. The retinal nervefibre layer corresponds to a bright redreflective layer at the inner retinal margin.The vitreoretinal interface is well defined dueto contrast between the non-reflectivevitreous and the backscattering retina. Weakreflections appear from the deep choroid andthe sclera due to signal attenuation.
The data management system stores theinformation for future reference. OCT softwarepackage includes 18 scan acquisitionprotocols and 18 analysis protocols. Togetherthey help us analyze the optic disc, the retinalnerve fiber layer and the macula with a singleinstrument. Thus OCT facilitates evaluationof both glaucoma and vitreoretinal diseases.
OCT is useful for detecting andmonitoring a variety of diseases, including.vitreomacular traction syndrome, macularhole, retinoschisis, macular edema, centralserous chorioretinopathy, subretinal neo-vascularization, age-related maculopathy. 3
The tomographic information provided byOCT has lead to a better understanding ofthe pathogenesis of macular hole formation.OCT is effective in distinguishing full-thickness macular holes from partial-thickness holes, macular pseudoholes, andcysts.4 OCT is useful in staging macular holesto identify potential surgical candidates. It canmeasure the diameter of macular hole, whichcan influence the post surgical outcome. Inaddition, hole resolution and macularthickness can be measured after surgery. OCT

44
is also useful to evaluate the vitreofovealinterface in patients' fellow eye and is ableto detect small (150 microns) separations ofthe posterior hyaloid from the retina.
OCT is useful for the diagnosis andquantitative characterization of epiretinalmembranes.5 The structural assessment ofthe macula is useful in the preoperative andpostoperative evaluation of epiretinalmembrane surgery. OCT can differentiatebetween the focally adherent membranes fromglobally adherent membranes. Globallyadherent membranes are associated withfeatures like macular pseudohole, a differencein optical reflectivity between the membraneand retina, and/or a visible membrane tuftor edge. Quantitative measurements and theassessment of membrane adherence with OCTmay be useful in characterizing the surgicalprognosis of eyes with an epiretinal
membrane.
OCT is a useful tool for evaluating,documenting and monitoring macular edema6
with a very high degree of accuracy. It issensitive to the small changes in retinalthickness. Macular edema is detected on OCTas intraretinal; areas of decreased reflectivityand retinal thickening. The various patternsdetected are - diffuse spongy type of edema,cystoid macular edema and neurosensoryretinal detachment. OCT is capable ofdetecting an early positive response tophotocoagulation for macular edema. 6
OCT has been used to evaluate variousfindings associated with ARMD7. It is helpfulin quantitatively evaluating subretinal andintraretinal fluid, assessing possible subfovealinvolvement of neovascularization, and inmonitoring CNV before and after laserphotocoagulation. Choroidal neovasculari
FIG.1- OCT picture of normal macula showing various layers of retina.

45
OCT enables unprecedented visualizationof intraretinal morphologic features andtherefore has the potential to contribute to abetter understanding of ocular pathogenesis,as well as to enhance the sensitivity andspecificity for early ophthalmic diagnosis andto monitor the efficacy of therapy.
References:1. Hee MR, Baumal CR, Puliafito CA.Optical
coherence tomography of the humanretina. Arch Ophthalmol 1995; 113:325-332.
2. Puliafito CA, Hee MR, Lin CP et al,Imaging of macular diseases with opticalcoherence tomography, Ophthalmology1995; 102(2): 217-29.
3. Drexler W, Sattmann H, Hermann B et al,Enhanced visualization of macularpathology with the use of ultra high-resolution optical coherence tomography.Arch Ophthalmol 2003; 121(5): 695-706.
4. Hee MR, Puliafito CA, Wong C et al,Optical coherence tomography of macularholes. Ophthalmology 1995; 102(5): 748-56.
5. Wilkins JR, Puliafito CA, Hee MR et al,Characterization of epiretinal membranesusing optical coherence tomography.Ophthalmology 1996; 103(12): 2142-51.
6. Rivellese M, George A, Sulkes D et al,Optical coherence tomography after laserphotocoagulation for clinically significantmacular edema. Ophthalmic Surg Lasers2000; 31(3): 192-7.
7. Hee MR, Baumal CR, Puliafito CA et al,Optical coherence tomography of age-related macular degeneration andchoroidal neovascularization. Ophthal-mology 1996; 103(8): 1260-70.
INSIGHT & EYELIGHTS are now available on line athttp://www.sankaranethralaya.org/publication.htm
zation is evident in the tomograms as athickening and fragmentation of a reflectivelayer, which corresponded to the retinalpigment epithelium and choriocapillaris. Ithas the potential to accurately define theboundaries in a subset of angiographicallyoccult CNV. Classic CNV presents with well-defined boundaries on OCT, whereas occultCNV had a variable cross-sectionalappearance. Pigmentary changes, soft drusen,and detachments of the neurosensory retinaand retinal pigment epithelium all havedistinct presentations on OCT. However it isdifficult to detect CNV beneath serouspigment epithelial detachments.
OCT can diagnose and objectivelyquantify the height of neurosensorydetachment in central serous chorio-retinopathy (CSR). It can accurately detectchanges in the height of detachment on followup visits. OCT is effective in distinguishingretinoschisis from retinal detachment. OCTimages of retinoschisis show a splitting ofthe neurosensory retina. The OCT images ofretinal detachment show separation of full-thickness neurosensory retina from theretinal pigment epithelium band. OCT candetect intraretinal separation of the detachedretina after retinal detachment inrhegmatogenous retinal detachment. It is oneof the factors associated with poor vision inrhegmatogenous retinal detachment.
Thus OCT has a great potential as adiagnostic and research tool. However it hasits own limitations in presence of mediaopacities like vitreous haemorrhage, cornealedema and dense cataract, which attenuatethe incident and reflected light.
PLEASE LOOK US UP ON THE WEB athttp://www.sankaranethralaya.org
Please forward your correct address with your E-mail address if any,to enable us to update our address data base.

Editor : Dr Mahesh P Shanmugam 46 For Private Circulation Only
(contd. on page 43)
Last Page
Optical Coherence Tomography inMacular DisordersMahesh Shanmugam, Sachin Kabra and Pratik Ranjan Sen
A near-infrared light beam (820 nm) isprojected onto the retina from a superluminescent diode. An infrared camera isused to view the fundus and probe beamlocation. The light beam is reflected at theboundaries of tissues with different opticalproperties. The echo time delays of lightreflected from the retina and reference mirrorare compared. The interferometer combinesthe reflected light pulses from the retina andthe reference mirror to create theinterference, which is measured by aphotodetector. The interfer-ometer electroni-cally detects, collects, processes and storesthe echo delay patterns from the retina.Multiple data points are integrated toconstruct a cross sectional image of retinalanatomy. The resultant OCT image of opticalreflectivity is displayed in false color scale. Itrepresents the degree of back-scattering fromtissues at different depths in the retina. Darkcolors such as blue and black representregions of minimal relative optical reflectivity,while bright colors such as red and whiterepresent regions of high optical reflectivity.The coherence length of the light sourcedefines the longitudinal resolution of the OCT,which is about 10 microns. The transverseresolution is determined by multiple factors,including the probe beam diameter and theseparation of individual A scans, and isupto13 microns.
The fundus view provided by traditionalophthalmoscopy is excellent. Techniques likefluorescein angiography, ultrasound andscanning laser ophthalmoscopy provides uswith additional details such as functional andanatomical integrity of the retina and otherstructures of the fundus. However currentdiagnostic instruments lack sufficientresolution to provide useful cross-sectionalimages of retinal structure. High frequencyultrasound has resolution to about 20 micronsbut cannot be applied to posterior segmentdue to limited penetration. Ocular aberrationsand the maximum entrance pupil diameter ofthe eye limit the longitudinal resolution ofconfocal imaging techniques such as scanninglaser ophthalmoscopy to 300 microns. Opticalcoherence tomography (O.C.T.) is a novelnoninvasive, noncontact-imaging modality,which produces high depth resolution (10microns) cross-sectional tomographs ofretina.1-3
OCT is a computer assisted precisionoptical instrument that works by a techniqueknown as low-coherence interferometry. Theprinciple of operation of interferometry issimilar to ultrasound, except that it uses lightrather than sound. The principle difference isthat the speed of light is nearly a million timesfaster than the speed of sound. The differencepermits measurement of structures anddistances on the <10-micron scale, versus the100-micron scale for ultrasound.
This issue of Insight is sponsored by:Rampion Eyetech Pvt. Ltd., Kalash, New Sharda Mandir Road, Paldi, Ahmedabad - 380 007Apex Laboratories Pvt. Ltd ., 44, Gandhi Mandapam Road, Kotturpuram, Chennai - 600 085Pharmacia & Upjohn India Pvt. Ltd., SCO 27, Sector 14, Gurgaon 122 001, HaryanaWarren Pharmaceuticals Ltd., 2/10, Joti Wire House, Veera Desai Road, Andheri (W), Mumbai - 400 053
Medical & Vision Research Foundations thank the above sponsors for their generosity.