

INSIDE OPERATIONAL EXCELLENCE AWARDS INSIDE FCS ......14 Toward Operational Excellence Honorees...
40
Dr. Ryan Olson directs uniquely positioned pathology laboratory Delivering Results INSIDE OPERATIONAL EXCELLENCE AWARDS » INSIDE FCS VOLUNTEERING » C.A.R.E. VALUES Summer 2015
Transcript of INSIDE OPERATIONAL EXCELLENCE AWARDS INSIDE FCS ......14 Toward Operational Excellence Honorees...

Summer 2015 1
Dr. Ryan Olson directs uniquely positioned
pathology laboratory
DeliveringResults
INSIDE OPERATIONAL EXCELLENCE AWARDS » INSIDE FCS VOLUNTEERING » C.A.R.E. VALUES
Summer 2015

2 FCS The Magazine
5202 Paylor Lane | Sarasota, FL 34240 | (855) 585-5433
Fighting cancer is a long journey. Florida Cancer Specialists Foundation helps make the road a little easier.
We deeply care about our patients and their struggles. Florida Cancer Specialists Foundation was created to help patients who need financial assistance while undergoing treatment. The Foundation allows those fighting their battle with cancer to concentrate on recovery rather than their overdue rent, mortgage, electric or water bill.
Please visit our website for ways to donate. Florida Cancer Specialists Foundation is a 501(c)(3) non-profit organization.
Foundation.FLCancer.comFoundation
A cancer diagnosis changes everything.

Summer 2015 3
summer 2015contents
in this issue
DEPARTMENTS 6 FCS News
18 Get to Know Dr. Spitz
30 FCS Events
33 C.A.R.E./CORE Values
38 Radar Screen
SPOTLIGHT 8 Research Spotlight: DR. RYAN OLSONLab director places premium on service.
12 Office Spotlight: WEST PALM BEACHFacility favors interdisciplinary approach.
24 Nurse Spotlight: DONNA OTTCaregiver closely connects with patients.
36 Doctor Spotlight: DR. MAEN HUSSEINInvestigator’s work fueled by optimism.
FEATURES14 Toward Operational ExcellenceHonorees foster continuing improvement.
26 Rx to the RescuePharmacy manages growing drug portfolio.
34 FCS Volunteer ProgramLittle things make big difference to patients.
Featured Nurse: Donna Ott is one-third of a three-nurse team at FCS’s Wellington office. “We have to work effectively together,” she says. “We support and reassure each other. We are family.”
5202 Paylor Lane | Sarasota, FL 34240 | (855) 585-5433
Fighting cancer is a long journey. Florida Cancer Specialists Foundation helps make the road a little easier.
We deeply care about our patients and their struggles. Florida Cancer Specialists Foundation was created to help patients who need financial assistance while undergoing treatment. The Foundation allows those fighting their battle with cancer to concentrate on recovery rather than their overdue rent, mortgage, electric or water bill.
Please visit our website for ways to donate. Florida Cancer Specialists Foundation is a 501(c)(3) non-profit organization.
Foundation.FLCancer.comFoundation
A cancer diagnosis changes everything.

4 FCS The Magazine
PHYSICIAN LEADERSHIPPRESIDENT
WILLIAM N. HARWIN, M.D. ASSISTANT MANAGING PARTNER,
DIRECTOR, EXECUTIVE BOARD STEPHEN V. ORMAN, M.D.
MEDICAL DIRECTOR MARK S. RUBIN, M.D.
SCIENTIFIC DIRECTOR OF CLINICAL RESEARCH, DIRECTOR, DRUG DEVELOPMENT PROGRAM
LOWELL L. HART, M.D.DIRECTOR OF RESEARCH OPERATIONS
ROBERT C. WHORF, M.D.
EXECUTIVE MANAGEMENTCHIEF EXECUTIVE OFFICER
BRAD PRECHTL CHIEF FINANCIAL OFFICER
LIBBY SLATERCHIEF OPERATING OFFICER
TODD SCHONHERZGENERAL COUNSEL
TOM CLARK CHIEF MARKETING & SALES OFFICER
SHELLY GLENNCHIEF HUMAN RESOURCES OFFICER
SHARON DILL SENIOR VICE PRESIDENT, RADIATION/RADIOLOGY
AND PARTNERSHIP SERVICES ED MERCADO
VICE PRESIDENT OF REVENUE CYCLE SARAH CEVALLOS
VICE PRESIDENT OF CLINIC FINANCIAL SERVICES CHRISTINA SIEVERT
SENIOR MANAGEMENTRAY BAILEY
JEREMY BEHLING JENNIFER BRYAN
LOIS BROWN MELODY CHANG
DAVID CURRY RICH DYSON JEFF ESHAM
MICHAEL ESSIK INGA GONZALEZ KATIE GOODMAN
CHRISTOPHER HOUSER SUE KEARNEY
LOIS POEL JEFFREY RUBIN
TARA RUSKA DENICE VEATCH
SAMANTHA WATKINS
When Brad Prechtl spoke, you could hear a pin drop. We were in Orlando at the lovely but dated Dolphin Hotel in a large, dim and cool ballroom. Brad was on stage as part of a three person panel invited by The Community Oncology Alliance to discuss the topic of merging one oncology practice into another.
The other two guests were nice, but the audience was hungry for information and they clearly recognized that Brad was the only person up there who could answer their questions from a perspective of successful experience.
How do you value the hard assets of the practice? What percentage of cash flow is drugs? What percentage is the “other stuff?” What is the fate of the loyal employees of the practice? What about employed physicians? Can you stop doctors from arguing?
There were about 500 people in the ballroom and they hung on Brad’s every word. FCS is the largest privately owned oncology practice in the country, and the folks there at the Dolphin really wanted to know how this was accomplished.
Brad did a great job. He answered the questions with as much candor and detail as he could, but I could tell that the audience wanted more: more detail, more “numbers.” Oncologists love formulas and regimens, they wanted the “NCCN regimen” for practice merging.
If they were listening carefully, they would have heard the secret. Brad often credited his excellent teams of support staff. He has his executive team, then there is the merger team, the clinical excellence team, the executive physician team, and on and on. Another way of saying team is to say: the people. So the deep secret of FCS success is actually very simple: the energy and intellect and good will of the people who work here. Like you.
We hope that you enjoy discovering more about these people in these pages of the summer edition of FCS the Magazine.
All the best,
Scott Tetreault,Editor, FCS the Magazine
Message from
Scott Tetreault
editor'sletter
FCSTHE MAGAZINE
DESIGNED AND PRODUCED BY
IN PARTNERSHIP WITH

Summer 2015 5
We Support the Health of your PracticeWith the Same Dedication that You Support Your Patients
Your number one priority is the health of your patients. With the changing healthcare landscape, our number one priority is the business health of your practice.
Dedicated exclusively to the viability of community oncology, ION Solutions provides contracting, technology, education and advocacy support that ensures you have the tools to run your practice both efficiently and effectively. With the practice support of ION Solutions, you can navigate this changing environment and focus on providing quality care for your patients.
To learn how ION Solutions enables community oncology practices to improve operational efficiency, financial performance and quality of care, contact your Strategic Account Manager or visit IONonline.com.
To experience ION Solutions advocacy support, visit ourcommunitycounts.org.

6 FCS The Magazine
FCSnews
✚ INVERNESS SOUTH OFFICE HOSTS RIBBON CUTTING AND TOUR OF NEW FACILITY
Florida Cancer Specialists physicians and staff welcomed community leaders and patients to a ribbon-cutting ceremony at the Inverness South office on April 8, 2015. The event celebrated the opening of the second Florida Cancer Specialists location in Inverness, Florida, which provides added convenience for patients in Citrus County.
Among those in attendance at the Inverness South ribbon cutting (left to right): Jeff Rubin, senior director of operations; Shelly Glenn, chief marketing and sales officer; Julie Anning, physician liaison; Servillano E. Dela Cruz Jr., medical oncologist; William V. Harrer, III, medical oncologist; Anthony Klement, medical assistant; Stephanie Alawee, registered nurse; Jennifer Petellat, patient services specialist; Jaimee Gordon, patient services specialist; Darlana Martin, financial counselor; Christine Soldo, registered nurse; Chris Hightower, office manager; Karen Genzardi, head nurse; Sherree Scriven, patient services specialist; Tiffany Anthony, medical assistant.
✚ FCS ANNOUNCES NOMINEES FOR LEUKEMIA & LYMPHOMA SOCIETY’S MAN/WOMAN OF THE YEAR
Florida Cancer Specialists & Research Institute (FCS) is pleased to announce that Drs. Beth Byron, Todd Gersten and Anjan J. Patel and Physician Liaison Danielle Spears have been nominated by local Florida chapters of the Leukemia & Lymphoma Society (LLS) as Man/Woman of the Year for 2015. After an intensive nominating and vetting process, these four outstanding community leaders accepted the challenge to engage in a spirited competition to raise funds for blood cancer research and earn the coveted title of “Man/Woman of the Year.” Danielle Spears won Leukemia & Lymphoma Society's Woman of the Year for Central Florida.
✚ CONSTRUCTION BEGINS ON NEW $10M CANCER FACILITY IN GAINESVILLEState-of-the-Art Facility Will Be Located Adjacent to North
Florida Regional Cancer CenterFlorida Cancer Specialists & Research Institute launched a new
$10 million construction project at a groundbreaking ceremony in Gainesville on March 18. The 25,000-square-foot facility will offer patients added convenience and access to a broad range of cancer services. According to Florida Cancer Specialists CEO Brad Prechtl, the center will house the clinical practice and research operations in Gainesville under one roof in a building connected to the North Florida Regional Cancer Center. The facility will replace FCS’s current 13,000-square-foot building in Gainesville, where they have practiced since 2011. FCS will be in full operation at its current location — 1147 NW 64th Terrace — during the construction.
The rendering depicts the new Florida Cancer Specialists & Research Institute in Gainesville, located adjacent to the North Florida Regional Medical Center. Florida Cancer Specialists physicians pictured (from left to right): Manuel de la Puerta, M.D., medical oncologist; Peter Acs, M.D., Ph.D., medical oncologist; Laura C. Dickerson, M.D., medical oncologist; Lucio Gordan, M.D., medical oncologist; Andres Bhatia, M.D., medical oncologist.

Summer 2015 7
✚ U.S. REP. RICHARD NUGENT AND MAYOR KENT GUINN ATTEND OCALA RIBBON CUTTING
Florida Cancer Specialists physicians and staff welcomed Congressman Richard Nugent and Ocala Mayor Kent Guinn, as well as patients and their families, to a ribbon-cutting ceremony at the Ocala office on Feb. 26. The event celebrated the expansion of the office to provide greater comfort and state-of-the-art services for patients in Marion County.
Among those in attendance at the Ocala location ribbon-cutting (left to right): Shelly Glenn, chief marketing and sales officer; Sandy Brooks, physician liaison; Mirna Cortez, billing; Dr. Vipul Patel, medical oncologist; Paige Morris, RN-nurse specialist; Michelle Guess, ARNP; Bradley Prechtl, chief executive officer; Peggy Hinman, RN-head nurse; Rachel Lefkowitz, office manager; Lisa Matos, MA; Dr. Patrick Acevedo, medical oncologist; Terri Ertley, pharmacy tech; Reina Goenaga, RN; Mary Cordier, PSS; Monica Peterkin, MA; Dr. Imad El-Jassous, medical oncologist; Jeff Rubin, senior regional director; Max Gibbons, PSS.
✚ WASHINGTON POST ARTICLE FEATURES DR. ANDY LIPMAN ON PATIENT EMPATHY
As an Oncology Fellow at Tufts/New England Medical Center in Boston, Dr. Andy Lipman learned a simple yet powerful truth: Never answer a patient’s feeling with a fact. That’s a lesson he takes to heart every day in his medical practice in Naples, Florida, as a partner with Florida Cancer Specialists. In an article published by the Washington Post, Lipman writes, “Clinical empathy was once dismissively known as ‘good bedside manner’ and traditionally regarded as far less important than technical acumen. But a spate of studies in the past decade has found that it is no mere frill. Increasingly, empathy is considered essential to establishing trust, the foundation of a good doctor-patient relationship.” Lipman reports that studies have linked empathy to greater patient satisfaction, better outcomes, decreased physician burnout and a lower risk of malpractice suits and errors.
✚ FLORIDA CANCER SPECIALISTS’ PHYSICIAN NAMED FLASCO PRESIDENT
Dr. Michael Diaz Assumes Leadership of Statewide Cancer Advocacy Organization
Florida Cancer Specialists & Research Institute (FCS) is pleased to announce that Michael Diaz, M.D., a member of the FCS Executive Board, was named president of the Florida Society of Clinical Oncology (FLASCO) at the organization’s Spring Conference and Annual Meeting, held in early April in Orlando. Known as the “Voice of Oncology in Florida,” FLASCO is a statewide 501(c)(3) nonprofit organization committed to facilitating and promoting multidisciplinary efforts to improve patient care in Florida. FLASCO also promotes excellence in care of patients afflicted with cancer and hematologic disorders and leads efforts to respond to policies and legislation that threaten to compromise patient access to quality cancer care.
✚ FLORIDA CANCER SPECIALISTS WELCOMES DR. MIGUEL PELAYODr. Pelayo to See Patients in Sarasota County
Florida Cancer Specialists & Research Institute (FCS) is pleased to announce that Miguel Pelayo, M.D., has joined the practice. He began seeing patients
at the Lakewood Ranch office on March 16. Commented FCS CEO Bradley Prechtl, “Dr. Pelayo will be able to add more convenience and expanded services for our patients in our Lakewood Ranch office. He received numerous awards and recognition during his years of training and we are very pleased to have him join the FCS family.” Originally from Miami, Florida, Dr. Pelayo has lived and studied in Florida for most of his life. During his internship and residency at the University of South Florida/H. Lee Moffitt Cancer Center in Tampa, he was chosen consecutively as Internal Medicine Intern of the Year, Outstanding Resident and Internal Medicine Resident of the Year.
✚ DR. ERNESTO BUSTINZA-LINARES JOINS FLORIDA CANCER SPECIALISTS
Physician Trained at MD Anderson to Practice in Central Florida
Florida Cancer Specialists & Research Institute (FCS) is pleased to welcome Ernesto Bustinza-Linares, M.D., to the practice. Dr. Bustinza-Linares has had training at M.D. Anderson and is seeing patients at the Deland, Lake Mary and Orange City office locations in Central Florida. Recognized for his avid interest in research, Dr. Bustinza-Linares has presented his findings at several statewide and national meetings of noted organizations such as the American College of Physicians, the American Medical Association and the American Society of Clinical Oncology. Dr. Bustinza-Linares’ areas of research interest include targeted therapies, breast cancer and GI malignancies. He has been practicing in Florida since 2011 and currently resides in Lake Mary.
✚ FCS PLEASED TO ADD TWO DOCTORS WITH STRONG INTEREST IN RESEARCH
Drs. Dandamudi and Patel Will See Patients in Brooksville, New Port Richey and Spring Hill
Florida Cancer Specialists & Research Institute (FCS) is pleased to announce that Uday Dan-damudi, M.D., and Shilen Patel, M.D., have joined the practice and will be seeing patients in the Brooksville, New Port Richey and Spring Hill FCS cancer centers, respectively. Dr. William Harwin, founder and president of FCS, said, “We are delighted to welcome Drs. Dandamudi and Patel to Florida Cancer Specialists. Both physicians come to us with excellent credentials, and each has a strong interest in clinical research. These two outstanding physicians will be able to add more convenience and expanded services for our patients in our Brooksville, New Port Richey and Spring Hill locations.” FCS CEO Bradley Prechtl added, “Dr. Dandamudi has broad experience in both hospital and private practice; Dr. Patel received several awards and recognition during his years of training and taught Oncology/Hematology Fellows at one of the leading cancer centers in the United States. We are very pleased to have both of them join the FCS family.”
FCSnews
8 FCS The Magazine

Summer 2015 9
If you put Dr. Ryan Olson’s life under a microscope, you’d see it multiplying exponentially. The 40-year-old hemato-pathologist from San Diego is the medical director of the Florida Cancer Specialist & Research Institute’s fast-growing
pathology lab in Fort Myers … and a first-time father of twins. Together, Drs. Olson and Mohammad Abuel Haija, along with laboratory managers Dr. Li, Silvia Fernandez, Kim Fortunato and Lisa Toomer, have overseen the lab’s development since 2011. In just four years, it has grown more than four-fold from a staff of six to greater than 24 hematopathologists, technologists, managers and assistants. Combined with the Central Lab, these testing facili-ties occupy 10,000 square feet of space devoted to state-of-the-art technology, which attracts some of the nation’s brightest minds.
Pathology Lab Passes the TestFacility has seen rapid growth BY ZANDRA WOLFGRAM
RESEARCH SPOTLIGHT
The pathology lab launched flow cytometry (laser-based cell testing) in 2010, but soon after Olson and Haija, who also is a hematopatholo-gist, came aboard in 2011, they set out to ex-pand the lab’s testing capabilities. Today, they include histology (examining cells on slides), immunohistochemistry (protein expression by antibody-assisted histology) and FISH (fluores-cent in situ hybridization) testing — a cytoge-netic technique used to detect and localize the presence or absence of specific DNA sequences on chromosomes at the molecular level.
“Really, the testing we do involves different ways of looking at the same tissue, kind of like
looking at different sides of the same coin on the same sample,” Olson explains.
Olson says the type of testing the lab per-forms does not depart much from that of other hospital or reference laboratories, but unique advantages result from the fact that the lab and its staff are seamlessly integrated into FCS’s daily operation.
“The biggest advantage to this lab is the highly personal communication with the on-cologists we serve,” Olson says. “Knowing us personally, having us on call 24/7 by text, cell and email is great for them.
“From a pathologist’s perspective, person-ally knowing the doctors who are requesting

10 FCS The Magazine
RESEARCH SPOTLIGHT
the tests and having access to all the patient’s health information cannot be overstated. No-where have I worked with such direct access to patient information and familiarity with the clinical oncologists. When I sign out a bone marrow biopsy, I know exactly where it was drawn, by whom, the reasons why and, most importantly, the clinical issue in question.”
Last year, Olson and his team processed nearly 5,000 bone marrow biopsies. To put this in perspective, Albany Medical Cen-ter, where Olson trained and completed his residency and fellowship, performed approxi-mately 600 per year. “I’ve been in practice five years now and I’ve performed about as many bone marrow reports as my mentor who has been in practice for over 15 years,” he says. “There are few, if any, places with such an op-portunity for a hematopathologist.”
Being a physician himself, Olson can clearly relate to the 160 medical oncologists he serves. “A pathologist is a doctor’s doctor, and our job at the lab is to serve and support them to give them what they need to support and serve their patients,” he says.
Recently, the College of American Patholo-gists (CAP) inspection gave the lab a perfect review. Olson is proud that the lab earned this “gold standard” certification and is quick to share the credit for the exponential growth and unprecedented volume with the entire lab team and Dr. William Harwin. “This lab wouldn’t be where it is without this incomparable team, and it certainly would not be pos-sible without the absolute and unequivocal support and leadership of Dr. Harwin,” Olson says.
Director of Compliance and Ancillary Services Sue Kearney is an ardent supporter, too. As someone driven by bottom line results, she knows first hand what the labs mean to the company’s bottom line. “The more testing we can do internally, the greater the benefit for our patients and for FCS. We’ve come a long way,” she says.
Running a fast-paced, high-volume lab isn’t for every pathologist. “There is a joke about pathologists that we don’t want to see patients and
I’ve been in practice five years now and I’ve performed about as many bone marrow reports as my mentor who has been in practice for over 15 years … There are few, if any, places with such an opportunity for a hematopathologist.”— DR. RYAN OLSON

Summer 2015 11
we work in a dark room all alone,” Ol-son says. “I don’t want that at all. I love my job, because I love working with other people.” And surely, the lab staff enjoys working with Olson because he is a strong team leader and effective communicator.
Although he did not initially intend to go into pathology when entering
Albany Medical College, Olson fell in love with the field during his third year of medical school and hasn’t looked back since. “Pathology is a tre-mendously fascinating field where you are always on the cutting edge,” he says. “Every time there is a new test, we’re always right there learning it, driving it and understanding it.”
Olson lives just a five-minute drive from the “gem of a lab” in which he works. “FCS built the lab with our direction, allowed us to hire spec-tacular personnel and gave us the freedom to run it. So yes, I pinch my-self all the time. This is absolutely a dream job, and I feel like a kid on a playground.”
And with the arrival of his new twin babies, he just may mean that literally!
State-of-the-art equipment is an indispensable part of FCS’s “gem of a lab” in Fort Myers. But what sets it apart for other testing laboratories, say Dr. Ryan Olson, is the extraordinarily close communication between lab staff and the oncologists they serve.

12 FCS The Magazine
The walk up to the FCS West Palm Beach facility is lined with palm trees and colorful flowers, leading to a beautiful façade that echoes both modernity and, somehow, permanence.
It’s a fitting contrast for this South Florida facility. Inside those doors, modern medicine meets decades’ worth of experience in treating cancer patients.
Lois Brown is the regional director for the West Palm Beach facility, also known as “Flagler,” (its street address). The Flagler office is unrivaled among cancer programs in the community because of its multi-disciplinary, comprehensive and integrated approach to treatments, and its access to the most advanced therapies available.
“Flagler offers a full spectrum of services all under one roof,” Brown explains. “We provide the most advanced cancer treatment in a caring and compassionate setting that helps patients and their families face the challenges of cancer.”
What began originally as the Helen and Harry Gray Cancer Institute, a part of the local hospital, became in 2003 the Palm Beach Cancer Institute. In June 2013, the facility merged with Florida Cancer Specialists and became a flagship center in the FCS portfolio.
The FCS Flagler location has a well-earned reputation of being a leading provider of cancer care in Palm Beach County. It is led by 16 dedicated physicians and a team of 65 employees.
Brown has been with the Flagler office since 2000. Today, she oversees the Flagler facility, along with five other locations in Vero Beach, Sebastian, Palm Beach Gardens, Atlantis and Wellington.
Accounting for just the Flagler facility, the physicians saw 1,800 new patients and over 19,000 total patient encounters in 2014.
“Our facility is an integral part of the community,” Brown says. Being a steadfast presence — even through growth and transition — is what makes FCS Flagler stand out.
TREATING THE WHOLE PATIENTThe facility offers unique provider services through Sari Center ranging from Integrated Cancer Care to Interventional Radiology. Some of
the specialized services available include genetic screenings by a highly trained genetic counselor and integrative oncology services that treat the whole body, not just the disease. Dietary services, therapeutic massage, yoga, acupuncture and counseling are some of the integrative oncology services that are offered at the FCS Flagler location.
In addition, physicians at the Flagler center provide a variety of specialized treatments for patients with cancer.
Dr. Gerald Zemel is an interventional radiologist, a highly trained physician who specializes in minimally invasive, targeted treatments for cancer and other diseases. Dr. Zemel uses image-guided technologies, such as CT, MRI, ultrasound and fluoroscopy, to place a catheter inside
the body and treat patients. As an alternative to open surgery, interventional radiology procedures can reduce risk, pain and recovery time for patients.
Dr. Howard Goodman is a gynecologic oncologist at FCS Flagler. In addition to the surgical management of women with gynecologic cancer, he performs all aspects of complex gynecologic surgery, pelvic reconstruction, advanced laparoscopy and robotic surgery.
Dr. Carisa Pearce is a specialist in both cancer rehabilitation and interventional pain management.
Her goals are to reduce pain and improve function and quality of life for patients. By prescribing a treatment plan that may include physical therapy, psychotherapy, injection therapy or rehabilitation techniques, Dr. Pearce is able to lessen some of the side effects that can occur as a result of cancer treatment.
Many of these traditional and complementary specialties help lift patients’ spirits, as well as elevate their bodies’ response to intervention and treatment. This commitment to the whole patient is the foundation of the FCS Flagler facility.
Like all FCS facilities, Flagler actively participates in clinical trial research to evaluate promising new therapies, investigational drugs and other treatment methods. Currently, the FCS Flagler cancer center is the only site in the state of Florida that is participating in a unique tumor cell vaccine trial for high-risk ovarian cancer.
Modern Medicine Meets Time-Tested CareFCS Flagler in West Palm Beach is a highly respected cancer center where patients get top-notch advanced care in a family-friendly setting BY TISHA CREWS KELLER
WEST PALM BEACH1309 N. Flagler Drive West Palm Beach, FL 33401Phone: (561) 366-4100
OFFICE SPOTLIGHT

Summer 2015 13
GIVING BACK IN MORE WAYS THAN ONEMost Florida Cancer Specialists employees view treating cancer patients as a calling, rather than just a job. Leaders like Lois Brown ensure that staff spirits remain upbeat and community involvement is high. Brown also points to the FCS/C.A.R.E. Values, which encourage giving back and striving to provide excellence in all that we do. To that end, FCS Flagler stands out just as much for its community involvement as it does for its medical expertise.
The physicians take time to give talks at local events about cancer care, prevention and provider support. Clinical symposiums are a mainstay on the FCS Flagler calendar. There is also a long tradition of raising awareness and funding for local charitable causes, especially those related to cancer.
Recently, Drs. Elizabeth Byron and Todd Gersten were nominated for Leukemia & Lymphoma Society’s Man and Woman of the Year. Both physicians have a passion and dedication to their patients and feel it is a great opportunity to come together with our employees, patients and people in the community to raise money for a great cause. This community outreach event included several fundraisers, a celebrity bartending event (with docs pouring drinks!), a vendor fair and T-shirt sales for Team Byron and Team Gersten.
The two physicians’ goal for the 10-week fund raising program was to raise $20,000 for the Leukemia & Lymphoma Society; to date, they have raised more than $75,000.
It’s this excitement for doing “good” that infuses the FCS Flagler team with a level of care and caring that the patients instinctively feel when they come for treatment. It also encourages staff members to go the extra mile and treat patients as if they are family members.
Strong teamwork and high job satisfaction are the hallmarks of FCS cancer Centers, and Flagler is no exception.
As professionals, the staff has the medical knowledge to provide world-class care. As a community and a team, they truly care about the people who they see so frequently and at such a vulnerable time.
“Caring and compassion is the number one attribute of our employees,” Brown explains. The physicians and staff strive to maintain an atmosphere where compassion for the patient accompanies the best cancer care found anywhere. Patients are, truly, at the heart of everything we do here.”
For the staff at FCS Flagler in West Palm Beach, there is only one acceptable approach to patient care: All in. The team is characterized by genuine care and compassion for patients, strong teamwork and high job satisfaction levels. Says regional director Lois Brown, “Patients are at the heart of everything we do.”

14 FCS The Magazine
OPERATIONAL EXCELLENCE AWARDS
The Operational Excellence Program is a strategic initiative that focuses on three key measures: growth, productivity and service. Aligning each of these areas with operational goals ensures that FCS employees are working together toward the same objectives.
Since its inception, over 60 employees from a variety of departments and across the network have been recognized as those who provide outstanding service and demonstrate their dedication to consistent improvement within their teams and areas of responsibility.
Since the program was instituted at FCS in late 2013, over 300 Standard Operating Procedures (SOPs) have been developed that have resulted in a savings for the company of over $3 million to date. Building on that initial success, COO Todd Schonherz and his team recently introduced a new initiative, Lean Six Sigma, to an inaugural class of 30 practice leaders who were trained during a five-day intensive course. Lean Six Sigma provides a set of tools and techniques for process improvement that helps identify and resolve problems and other complex issues.
Jeremy Behling, vice president of operations, said, “Lean Six Sigma is a tool in your toolbox. It’s a way of looking at a problem or process and provides you a methodology that helps you identify, measure and analyze it, so that it can be corrected and reduce the risk of it reoccurring. I use it as a leadership methodology to create cross-functional teams to ensure that everyone has a seat at the table when we are considering how to improve something; it’s bigger than any one particular person or department.”
Behling anticipates that it will take three to six months to implement new processes and begin tracking improvement. He emphasizes that Lean Six Sigma is not a “band-aid” approach that only provides a temporary fix. Rather, it is a strategic methodology that requires a team effort and seeks to realize true and lasting change and improvement. In 2014, the Operational Excellence Program focused on standardization. This year is a year of taking action and implementing change; 2016 will be a year focusing on results.
Behling added, “During 4th quarter 2015, we are planning to implement an Idea Site, through which employees can make suggestions to improve the overall experience at FCS. We are very excited about gathering ideas on a company-wide basis on how to improve our business.”
COO Schonherz noted that the Lean Six Sigma process would be taught to additional employees in months to come, creating teams that will be empowered to identify and rectify problems in their areas of responsibility. Eventually, this team approach will guide a cultural shift towards continuous improvement throughout the entire organization.
Toward Operational
ExcellenceInitiatives improve
patient satisfaction
BY ELAINE GANICK
There are currently six project areas on which the Lean Six Sigma leaders are focusing:
1. Improving patient satisfaction
2. Reducing patient wait times
3. Improving prescription time-to-fill within Rx to Go
4. Reducing radiology leakage/increasing the number of patients getting PET/CT through FCS
5. Improving overall travel management/reducing travel expenses
6. Improving first pass rate for insurance claims/reducing denials so claims are paid on first pass

Summer 2015 15
2014 OPERATIONAL EXCELLENCE AWARD WINNERS
1. Marina Garza, OM; Todd Schonherz, COO; Maria Damiani-Johnson; and Lois Poel, RD
2. Jeremy Behling, VP Operations, Jill Daniels and Christina Sievert, VP Managed Care
3. Jeff Rubin, Sr. Director Operations; Dr. Marte; Todd Schonherz, COO; Joyce Diele; Dr. Ball; Joan Harris, Sr. Office Manager; and Dr. Alemar
4. Todd Schonherz, COO, Magda Melchert, MD, Julio Lautersztain, MD, Michelle Yoder and Sam Watkins, RD
5. Todd Schonherz, COO; Jeff Rubin, Sr. Director Operations; Dr. Rao; Lane Hallewell, RN; Ellen Bishop; Angie Thorn, MA; Dr. Fonseca; and Karen Jacques-Huntley, ARNP
6. Inga Gonzalez, RD; Todd Schonherz, COO; Amanda Bass; Jennifer Baptiste, HN; Annie Pigue, Sr. Office Manager; and Dr. Hussein
7. Debbie Mabry, Office Manager, and Haley Barber
1.
3.
5.
7.
2.
4.
6.
Maria Damiani-Johnson, Patient Services Specialist at Naples Goodlette office
Joyce Diele, Patient Services Specialist at Mease/Clearwater office
Ellen Bishop, Patient Services Specialist at Lecanto office
Haley Barber, Patient Services Specialist at Tallahassee North
Jill Daniels, Financial Counselor at North Port office
Michelle Yoder, Patient Services Specialist at Tampa Cancer Center
Amanda Bass, Patient Services Specialist at Tavares office

16 FCS The Magazine
8.
10.
12.
14.
9.
11.
13.
15.
Sharon Martinez, Patient Services Specialist at Atlantis/JFK office
Clara Hernandez, Recruiter at Corporate office
Marge Cooke, Systems Admin at Gateway office
Exsa Guzman , Lead Medical Assistant at Broadway office
Jennifer Jessee, Patient Services Specialist at Port Orange office
Colleen Hendricks, Financial Counselor Support Supervisor at Metro office
Kara Sammons, Supervisor Pharm Tech at Corporate office
Jan Montag, Registered Nurse at Venice Healthpark
2014 OPERATIONAL EXCELLENCE AWARD WINNERS

Summer 2015 17
8. Dr. Byron, Dr. Peles, Sharon Martinez, Todd Schonherz, COO, and Lois Brown, RD
9. Inga Gonzalez, RD, Jennifer Jessee, Dr. Doughney, Susan Price, SOM, and Todd Schonherz, COO
10. Dr. Harwin, Clara Hernandez and Brad Prechtl, CEO11. Christina Sievert, VP Managed Care, and Colleen Hendricks12. Brad Prechtl, CEO; Marge Cooke; Sarah Cevallos, VP Revenue Cycle;
and Todd Schonherz, COO13. Katherine Hogan, Pharmacy Manager; Kara Sammons; and Ray Bailey,
Director of Pharmacy14. Lois Poel, RD; Malbery (Betty) Carrion, MA; Todd Schonherz, COO;
Alma Medina, FC; Dee Steeb, PA; Dr. Rodriguez; Sharon Dill, CHRO; Ann Marie Cannistraci Sr., OM; and Esbeyde Guzman
15. Todd Schonherz, COO, Jan Montag and Jeremy Behling, VP Operations
16. Dr. Chamberlain; Andrea Bolivar, Office Manager; Jeff Rubin, Sr. Director Operations; Christopher Thibodaux; Todd Schonherz, COO; and Dr. Luong
17. Todd Schonherz, COO; Dr. Fink; Jenneth Montesino and Sam Watkins, RD
18. Samantha Osteen, RN; Jeff Rubin, Sr. Director Operations; and Brad Prechtl, CEO
19. Michelle Falardeau, Head Nurse; Lourdes Castro; Dr. Gousse; Todd Schonherz, COO; Kristy Meeks, Asst. Office Manager; and Inga Gonzalez, RD
20. Lois Brown, RD; Dr. Gersten, Manouchka Mildor, RN; Dr. Harris; and Todd Schonherz, COO
21. Helen Dantuma, Head Nurse; Todd Schonherz, COO; Ashley Rollins; Dr. Thaper; and Jennifer Gadsden, Asst. Office Manager
16.
18.
20.
17.
19.
21.
Christopher Thibodaux, Lead Medical Assistant at St. Petersburg office
Samantha Osteen, Registered Nurse at Inverness office
Manouchka Mildor, Registered Nurse at Wellington office
Jenneth Montesino, Clinical Assistant at Tampa Cancer Center
Lourdes Castro, Medical Assistant at Altamonte Springs office
Ashley Rollins, Licensed Practical Nurse at Leesburg South
2014 OPERATIONAL EXCELLENCE AWARD WINNERS

18 FCS The Magazine
Dr. Spitz has been practicing in Palm Beach for 27 years and agreed to answer our compelling questions.Where did you graduate from high school? I am a proud alumni of Far Rockaway High School. Go Seahorses!
Where did you take your wife on your first date together? I don’t really remember. I do remember our second date, though. I fell asleep! Residency-call fatigue will do that.
Where did the two of you go for your most recent date? We recently vacationed in the Bahamas.
What specialty would you be in if not oncology? If I weren't practicing oncology, I would definitely specialize in rheumatology.
Favorite superhero from Marvel’s Avengers? Thor.
Favorite sports team? Yankees.
Favorite movie? The “Bourne” film series.
What is currently taking up space on your DVR? Nothing, believe it or not. I don’t really record any TV shows.
Apple or Android? Apple.
Do you have any four-legged companions at home? Yes — a shih-tzu named Ziggy.
Would you rather drive a 1965 Ferrari 500 Superfast or 1969 L88 Corvette? The Corvette.
Go-to happy hour drink? Vodka martini.
Q&A Profileget to know your doctor
Dr. Daniel L. Spitz graduated from the Medical University of South Carolina College of Medicine in 1980 and has been practicing oncology in West Palm Beach for 27 years. Left: Dr. Spitz in his free time with Ziggy the shih-tzu.
The Man Behind the Lab CoatDr. Daniel Spitz answers some of our questions BY DR. SCOTT TETREAULT

Summer 2015 19
Save the Date2015 FCS Nursing & Pharm-Tech Conference
Date: Saturday, September 26, 2015
Time: 8:30 AM - 4:30 PM
Registration & Continental Breakfast: 8:30 AM - 8:55 AM
Place: MOSI Museum 4801 E. Fowler Avenue Tampa, Florida 33617
Designed exclusively for FCS RNs, LPNs and Pharm-techs, this conference is a great opportunity to learn from expert speakers and
network with colleagues within your FCS Family.
Conference details and registration information will be available in the next few months.
We hope to see you there!
Prom
oting Health, Hope and
Hea
ling
Togeth
er As a Team

20 FCS The Magazine
THIS SUPPLEMENT IS SPONSORED AND CO-DEVELOPED BY TAKEDA. PARTICIPANT RECEIVED COMPENSATION FOR TIME AND INPUT.
Treatment sequencing in multiple myeloma: understanding the role of VELCADE® (bortezomib) from initial therapy to retreatmentMultiple myeloma is a complex disease requiring a long-term treatment strategy. Although the disease remains incurable, the advent of novel therapies has led to improved outcomes. However, this places more emphasis on the role of treatment sequencing than ever before. Takeda spoke with Shachar Peles, MD, from Florida Cancer Specialists and Research Institute to learn more about his approach to treatment sequencing with VELCADE (bortezomib), from initial therapy to retreatment.
Indication and Important Safety Information for VELCADE® (bortezomib)
INDICATION
VELCADE (bortezomib) is indicated for the treatment of patients with multiple myeloma.
CONTRAINDICATIONSVELCADE is contraindicated in patients with hypersensitivity (not including local reactions) to bortezomib, boron, or mannitol, including anaphylactic reactions. VELCADE is contraindicated for intrathecal administration. Fatal events have occurred with intrathecal administration of VELCADE.
▼ Peripheral neuropathy: Manage with dose modification or discontinuation. Patients with preexisting severe neuropathy should be treated with VELCADE only after careful risk-benefit assessment.▼ Hypotension: Use caution when treating patients taking anti-hypertensives, with a history of syncope, or with dehydration.▼ Cardiac toxicity: Worsening of and development of cardiac failure has occurred. Closely monitor patients with existing heart disease or risk factors for heart disease.▼ Pulmonary toxicity: Acute respiratory syndromes have occurred. Monitor closely for new or worsening symptoms.▼ Posterior reversible encephalopathy syndrome: Consider
MRI imaging for onset of visual or neurological symptoms; discontinue VELCADE if suspected.
▼ Gastrointestinal toxicity: Nausea, diarrhea, constipation, and vomiting may require use of antiemetic and antidiarrheal medications or fluid replacement.▼ Thrombocytopenia or Neutropenia: Monitor complete blood
counts regularly throughout treatment.▼ Tumor lysis syndrome: Closely monitor patients with high tumor burden.▼ Hepatic Toxicity: Monitor hepatic enzymes during treatment. ▼ Embryo-fetal risk: Women should avoid becoming pregnant while being treated with VELCADE. Advise pregnant women of potential embryo-fetal harm.
Please see Important Safety Information on this page and Brief Summary for VELCADE adjacent to this advertisement.
▼ Closely monitor patients receiving VELCADE in combination with strong CYP3A4 inhibitors. Avoid concomitant use of strong CYP3A4 inducers. ▼ Patients with diabetes may require close monitoring of blood
glucose and adjustment of anti-diabetic medication.
ADVERSE REACTIONS: ▼ Previously Untreated Multiple Myeloma:
In the phase 3 study of VELCADE administered intravenously with melphalan and prednisone (MP) vs MP alone, the most commonly reported adverse reactions (ARs) were thrombocytopenia (48% vs 42%), neutropenia (47% vs 42%), peripheral neuropathy (46% vs 1%), nausea (39% vs 21%), diarrhea (35% vs 6%), neuralgia (34% vs <1%), anemia (32% vs 46%), and leukopenia (32% vs 28%).
▼ Relapsed MM: In the phase 3 study of VELCADE (bortezomib) administered intravenously vs dexamethasone, the most commonly reported ARs were nausea (52% vs 9%), diarrhea (52% vs 11%), fatigue (39% vs 25%), peripheral neuropathies (35% vs 4%), thrombocytopenia (33% vs 3%), constipation (30% vs 8%), vomiting (29% vs 3%), and anorexia (21% vs 2%). The most commonly reported serious ARs were diarrhea (3%), dehydration, herpes zoster, pyrexia, nausea, vomiting, dyspnea, and thrombocytopenia (2% each) in the VELCADE treatment group and pneumonia (4%), hyperglycemia (3%), pyrexia, and psychotic disorder (2% each) in the dexamethasone treatment group.
WARNINGS, PRECAUTIONS, DRUG INTERACTIONS AND USE IN SPECIFIC POPULATIONS
“ Retreatment with VELCADE demonstrated an additional benefit with no evidence of cumulative toxicities.”
Shachar Peles, MDWest Palm Beach, JFK
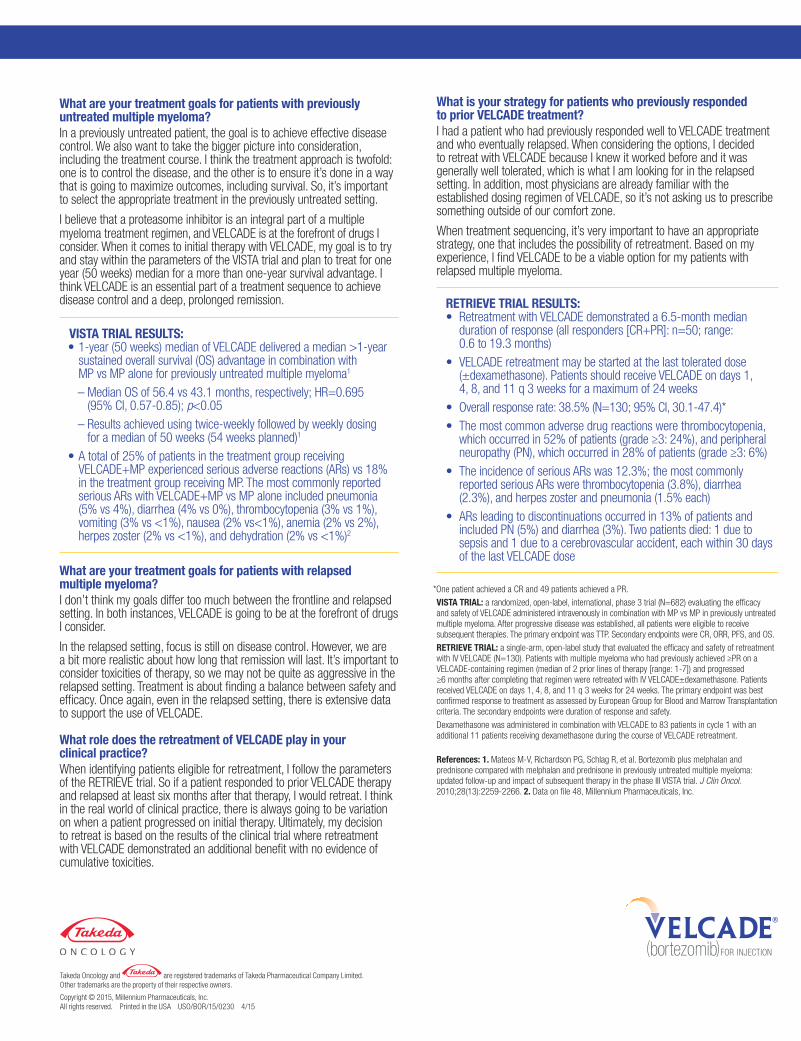
What are your treatment goals for patients with previously untreated multiple myeloma?In a previously untreated patient, the goal is to achieve effective disease control. We also want to take the bigger picture into consideration, including the treatment course. I think the treatment approach is twofold: one is to control the disease, and the other is to ensure it’s done in a way that is going to maximize outcomes, including survival. So, it’s important to select the appropriate treatment in the previously untreated setting.
I believe that a proteasome inhibitor is an integral part of a multiple myeloma treatment regimen, and VELCADE is at the forefront of drugs I consider. When it comes to initial therapy with VELCADE, my goal is to try and stay within the parameters of the VISTA trial and plan to treat for one year (50 weeks) median for a more than one-year survival advantage. I think VELCADE is an essential part of a treatment sequence to achieve disease control and a deep, prolonged remission.
What are your treatment goals for patients with relapsed multiple myeloma?I don’t think my goals differ too much between the frontline and relapsed setting. In both instances, VELCADE is going to be at the forefront of drugs I consider.
In the relapsed setting, focus is still on disease control. However, we are a bit more realistic about how long that remission will last. It’s important to consider toxicities of therapy, so we may not be quite as aggressive in the relapsed setting. Treatment is about finding a balance between safety and efficacy. Once again, even in the relapsed setting, there is extensive data to support the use of VELCADE.
What role does the retreatment of VELCADE play in your clinical practice?When identifying patients eligible for retreatment, I follow the parameters of the RETRIEVE trial. So if a patient responded to prior VELCADE therapy and relapsed at least six months after that therapy, I would retreat. I think in the real world of clinical practice, there is always going to be variation on when a patient progressed on initial therapy. Ultimately, my decision to retreat is based on the results of the clinical trial where retreatment with VELCADE demonstrated an additional benefit with no evidence of cumulative toxicities.
*One patient achieved a CR and 49 patients achieved a PR.
VISTA TRIAL: a randomized, open-label, international, phase 3 trial (N=682) evaluating the efficacy and safety of VELCADE administered intravenously in combination with MP vs MP in previously untreated multiple myeloma. After progressive disease was established, all patients were eligible to receive subsequent therapies. The primary endpoint was TTP. Secondary endpoints were CR, ORR, PFS, and OS.
RETRIEVE TRIAL: a single-arm, open-label study that evaluated the efficacy and safety of retreatment with IV VELCADE (N=130). Patients with multiple myeloma who had previously achieved ≥PR on a VELCADE-containing regimen (median of 2 prior lines of therapy [range: 1-7]) and progressed ≥6 months after completing that regimen were retreated with IV VELCADE±dexamethasone. Patients received VELCADE on days 1, 4, 8, and 11 q 3 weeks for 24 weeks. The primary endpoint was best confirmed response to treatment as assessed by European Group for Blood and Marrow Transplantation criteria. The secondary endpoints were duration of response and safety.
Dexamethasone was administered in combination with VELCADE to 83 patients in cycle 1 with an additional 11 patients receiving dexamethasone during the course of VELCADE retreatment.
References: 1. Mateos M-V, Richardson PG, Schlag R, et al. Bortezomib plus melphalan and prednisone compared with melphalan and prednisone in previously untreated multiple myeloma: updated follow-up and impact of subsequent therapy in the phase III VISTA trial. J Clin Oncol. 2010;28(13):2259-2266. 2. Data on file 48, Millennium Pharmaceuticals, Inc.
Takeda Oncology and are registered trademarks of Takeda Pharmaceutical Company Limited. Other trademarks are the property of their respective owners.
Copyright © 2015, Millennium Pharmaceuticals, Inc. All rights reserved. Printed in the USA USO/BOR/15/0230 4/15
What is your strategy for patients who previously responded to prior VELCADE treatment? I had a patient who had previously responded well to VELCADE treatment and who eventually relapsed. When considering the options, I decided to retreat with VELCADE because I knew it worked before and it was generally well tolerated, which is what I am looking for in the relapsed setting. In addition, most physicians are already familiar with the established dosing regimen of VELCADE, so it’s not asking us to prescribe something outside of our comfort zone.
When treatment sequencing, it’s very important to have an appropriate strategy, one that includes the possibility of retreatment. Based on my experience, I find VELCADE to be a viable option for my patients with relapsed multiple myeloma.
DOCTOR SPOTLIGHT
VISTA TRIAL RESULTS: • 1-year (50 weeks) median of VELCADE delivered a median >1-year
sustained overall survival (OS) advantage in combination with MP vs MP alone for previously untreated multiple myeloma1
– Median OS of 56.4 vs 43.1 months, respectively; HR=0.695 (95% CI, 0.57-0.85); p<0.05
– Results achieved using twice-weekly followed by weekly dosing for a median of 50 weeks (54 weeks planned)1
• A total of 25% of patients in the treatment group receiving VELCADE+MP experienced serious adverse reactions (ARs) vs 18% in the treatment group receiving MP. The most commonly reported serious ARs with VELCADE+MP vs MP alone included pneumonia (5% vs 4%), diarrhea (4% vs 0%), thrombocytopenia (3% vs 1%), vomiting (3% vs <1%), nausea (2% vs<1%), anemia (2% vs 2%), herpes zoster (2% vs <1%), and dehydration (2% vs <1%)2
RETRIEVE TRIAL RESULTS: • Retreatment with VELCADE demonstrated a 6.5-month median
duration of response (all responders [CR+PR]: n=50; range: 0.6 to 19.3 months)
• VELCADE retreatment may be started at the last tolerated dose (±dexamethasone). Patients should receive VELCADE on days 1, 4, 8, and 11 q 3 weeks for a maximum of 24 weeks
• Overall response rate: 38.5% (N=130; 95% CI, 30.1-47.4)* • The most common adverse drug reactions were thrombocytopenia,
which occurred in 52% of patients (grade ≥3: 24%), and peripheral neuropathy (PN), which occurred in 28% of patients (grade ≥3: 6%)
• The incidence of serious ARs was 12.3%; the most commonly reported serious ARs were thrombocytopenia (3.8%), diarrhea (2.3%), and herpes zoster and pneumonia (1.5% each)
• ARs leading to discontinuations occurred in 13% of patients and included PN (5%) and diarrhea (3%). Two patients died: 1 due to sepsis and 1 due to a cerebrovascular accident, each within 30 days of the last VELCADE dose
PRODUCT REVIEW
Summer 2015 21
THIS SUPPLEMENT IS SPONSORED AND CO-DEVELOPED BY TAKEDA. PARTICIPANT RECEIVED COMPENSATION FOR TIME AND INPUT.
Treatment sequencing in multiple myeloma: understanding the role of VELCADE® (bortezomib) from initial therapy to retreatmentMultiple myeloma is a complex disease requiring a long-term treatment strategy. Although the disease remains incurable, the advent of novel therapies has led to improved outcomes. However, this places more emphasis on the role of treatment sequencing than ever before. Takeda spoke with Shachar Peles, MD, from Florida Cancer Specialists and Research Institute to learn more about his approach to treatment sequencing with VELCADE (bortezomib), from initial therapy to retreatment.
Indication and Important Safety Information for VELCADE® (bortezomib)
INDICATION
VELCADE (bortezomib) is indicated for the treatment of patients with multiple myeloma.
CONTRAINDICATIONSVELCADE is contraindicated in patients with hypersensitivity (not including local reactions) to bortezomib, boron, or mannitol, including anaphylactic reactions. VELCADE is contraindicated for intrathecal administration. Fatal events have occurred with intrathecal administration of VELCADE.
▼ Peripheral neuropathy: Manage with dose modification or discontinuation. Patients with preexisting severe neuropathy should be treated with VELCADE only after careful risk-benefit assessment.▼ Hypotension: Use caution when treating patients taking anti-hypertensives, with a history of syncope, or with dehydration.▼ Cardiac toxicity: Worsening of and development of cardiac failure has occurred. Closely monitor patients with existing heart disease or risk factors for heart disease.▼ Pulmonary toxicity: Acute respiratory syndromes have occurred. Monitor closely for new or worsening symptoms.▼ Posterior reversible encephalopathy syndrome: Consider
MRI imaging for onset of visual or neurological symptoms; discontinue VELCADE if suspected.
▼ Gastrointestinal toxicity: Nausea, diarrhea, constipation, and vomiting may require use of antiemetic and antidiarrheal medications or fluid replacement.▼ Thrombocytopenia or Neutropenia: Monitor complete blood
counts regularly throughout treatment.▼ Tumor lysis syndrome: Closely monitor patients with high tumor burden.▼ Hepatic Toxicity: Monitor hepatic enzymes during treatment. ▼ Embryo-fetal risk: Women should avoid becoming pregnant while being treated with VELCADE. Advise pregnant women of potential embryo-fetal harm.
Please see Important Safety Information on this page and Brief Summary for VELCADE adjacent to this advertisement.
▼ Closely monitor patients receiving VELCADE in combination with strong CYP3A4 inhibitors. Avoid concomitant use of strong CYP3A4 inducers. ▼ Patients with diabetes may require close monitoring of blood
glucose and adjustment of anti-diabetic medication.
ADVERSE REACTIONS: ▼ Previously Untreated Multiple Myeloma:
In the phase 3 study of VELCADE administered intravenously with melphalan and prednisone (MP) vs MP alone, the most commonly reported adverse reactions (ARs) were thrombocytopenia (48% vs 42%), neutropenia (47% vs 42%), peripheral neuropathy (46% vs 1%), nausea (39% vs 21%), diarrhea (35% vs 6%), neuralgia (34% vs <1%), anemia (32% vs 46%), and leukopenia (32% vs 28%).
▼ Relapsed MM: In the phase 3 study of VELCADE (bortezomib) administered intravenously vs dexamethasone, the most commonly reported ARs were nausea (52% vs 9%), diarrhea (52% vs 11%), fatigue (39% vs 25%), peripheral neuropathies (35% vs 4%), thrombocytopenia (33% vs 3%), constipation (30% vs 8%), vomiting (29% vs 3%), and anorexia (21% vs 2%). The most commonly reported serious ARs were diarrhea (3%), dehydration, herpes zoster, pyrexia, nausea, vomiting, dyspnea, and thrombocytopenia (2% each) in the VELCADE treatment group and pneumonia (4%), hyperglycemia (3%), pyrexia, and psychotic disorder (2% each) in the dexamethasone treatment group.
WARNINGS, PRECAUTIONS, DRUG INTERACTIONS AND USE IN SPECIFIC POPULATIONS
“ Retreatment with VELCADE demonstrated an additional benefit with no evidence of cumulative toxicities.”
Shachar Peles, MDWest Palm Beach, JFK
What are your treatment goals for patients with previously untreated multiple myeloma?In a previously untreated patient, the goal is to achieve effective disease control. We also want to take the bigger picture into consideration, including the treatment course. I think the treatment approach is twofold: one is to control the disease, and the other is to ensure it’s done in a way that is going to maximize outcomes, including survival. So, it’s important to select the appropriate treatment in the previously untreated setting.
I believe that a proteasome inhibitor is an integral part of a multiple myeloma treatment regimen, and VELCADE is at the forefront of drugs I consider. When it comes to initial therapy with VELCADE, my goal is to try and stay within the parameters of the VISTA trial and plan to treat for one year (50 weeks) median for a more than one-year survival advantage. I think VELCADE is an essential part of a treatment sequence to achieve disease control and a deep, prolonged remission.
What are your treatment goals for patients with relapsed multiple myeloma?I don’t think my goals differ too much between the frontline and relapsed setting. In both instances, VELCADE is going to be at the forefront of drugs I consider.
In the relapsed setting, focus is still on disease control. However, we are a bit more realistic about how long that remission will last. It’s important to consider toxicities of therapy, so we may not be quite as aggressive in the relapsed setting. Treatment is about finding a balance between safety and efficacy. Once again, even in the relapsed setting, there is extensive data to support the use of VELCADE.
What role does the retreatment of VELCADE play in your clinical practice?When identifying patients eligible for retreatment, I follow the parameters of the RETRIEVE trial. So if a patient responded to prior VELCADE therapy and relapsed at least six months after that therapy, I would retreat. I think in the real world of clinical practice, there is always going to be variation on when a patient progressed on initial therapy. Ultimately, my decision to retreat is based on the results of the clinical trial where retreatment with VELCADE demonstrated an additional benefit with no evidence of cumulative toxicities.
*One patient achieved a CR and 49 patients achieved a PR.
VISTA TRIAL: a randomized, open-label, international, phase 3 trial (N=682) evaluating the efficacy and safety of VELCADE administered intravenously in combination with MP vs MP in previously untreated multiple myeloma. After progressive disease was established, all patients were eligible to receive subsequent therapies. The primary endpoint was TTP. Secondary endpoints were CR, ORR, PFS, and OS.
RETRIEVE TRIAL: a single-arm, open-label study that evaluated the efficacy and safety of retreatment with IV VELCADE (N=130). Patients with multiple myeloma who had previously achieved ≥PR on a VELCADE-containing regimen (median of 2 prior lines of therapy [range: 1-7]) and progressed ≥6 months after completing that regimen were retreated with IV VELCADE±dexamethasone. Patients received VELCADE on days 1, 4, 8, and 11 q 3 weeks for 24 weeks. The primary endpoint was best confirmed response to treatment as assessed by European Group for Blood and Marrow Transplantation criteria. The secondary endpoints were duration of response and safety.
Dexamethasone was administered in combination with VELCADE to 83 patients in cycle 1 with an additional 11 patients receiving dexamethasone during the course of VELCADE retreatment.
References: 1. Mateos M-V, Richardson PG, Schlag R, et al. Bortezomib plus melphalan and prednisone compared with melphalan and prednisone in previously untreated multiple myeloma: updated follow-up and impact of subsequent therapy in the phase III VISTA trial. J Clin Oncol. 2010;28(13):2259-2266. 2. Data on file 48, Millennium Pharmaceuticals, Inc.
Takeda Oncology and are registered trademarks of Takeda Pharmaceutical Company Limited. Other trademarks are the property of their respective owners.
Copyright © 2015, Millennium Pharmaceuticals, Inc. All rights reserved. Printed in the USA USO/BOR/15/0230 4/15
What is your strategy for patients who previously responded to prior VELCADE treatment? I had a patient who had previously responded well to VELCADE treatment and who eventually relapsed. When considering the options, I decided to retreat with VELCADE because I knew it worked before and it was generally well tolerated, which is what I am looking for in the relapsed setting. In addition, most physicians are already familiar with the established dosing regimen of VELCADE, so it’s not asking us to prescribe something outside of our comfort zone.
When treatment sequencing, it’s very important to have an appropriate strategy, one that includes the possibility of retreatment. Based on my experience, I find VELCADE to be a viable option for my patients with relapsed multiple myeloma.
DOCTOR SPOTLIGHT
VISTA TRIAL RESULTS: • 1-year (50 weeks) median of VELCADE delivered a median >1-year
sustained overall survival (OS) advantage in combination with MP vs MP alone for previously untreated multiple myeloma1
– Median OS of 56.4 vs 43.1 months, respectively; HR=0.695 (95% CI, 0.57-0.85); p<0.05
– Results achieved using twice-weekly followed by weekly dosing for a median of 50 weeks (54 weeks planned)1
• A total of 25% of patients in the treatment group receiving VELCADE+MP experienced serious adverse reactions (ARs) vs 18% in the treatment group receiving MP. The most commonly reported serious ARs with VELCADE+MP vs MP alone included pneumonia (5% vs 4%), diarrhea (4% vs 0%), thrombocytopenia (3% vs 1%), vomiting (3% vs <1%), nausea (2% vs<1%), anemia (2% vs 2%), herpes zoster (2% vs <1%), and dehydration (2% vs <1%)2
RETRIEVE TRIAL RESULTS: • Retreatment with VELCADE demonstrated a 6.5-month median
duration of response (all responders [CR+PR]: n=50; range: 0.6 to 19.3 months)
• VELCADE retreatment may be started at the last tolerated dose (±dexamethasone). Patients should receive VELCADE on days 1, 4, 8, and 11 q 3 weeks for a maximum of 24 weeks
• Overall response rate: 38.5% (N=130; 95% CI, 30.1-47.4)* • The most common adverse drug reactions were thrombocytopenia,
which occurred in 52% of patients (grade ≥3: 24%), and peripheral neuropathy (PN), which occurred in 28% of patients (grade ≥3: 6%)
• The incidence of serious ARs was 12.3%; the most commonly reported serious ARs were thrombocytopenia (3.8%), diarrhea (2.3%), and herpes zoster and pneumonia (1.5% each)
• ARs leading to discontinuations occurred in 13% of patients and included PN (5%) and diarrhea (3%). Two patients died: 1 due to sepsis and 1 due to a cerebrovascular accident, each within 30 days of the last VELCADE dose

22 FCS The Magazine
(Continued on next page)
Brief Summary
INDICATION:VELCADE® (bortezomib) for Injection is indicated for the treatment of patients with multiple myeloma.CONTRAINDICATIONS: VELCADE is contraindicated in patients with hypersensitivity (not including local reactions) to bortezomib, boron, or mannitol, including anaphylactic reactions. VELCADE is contraindicated for intrathecal administration. Fatal events have occurred with intrathecal administration of VELCADE.WARNINGS AND PRECAUTIONS: Peripheral Neuropathy: VELCADE treatment causes a peripheral neuropathy that is predominantly sensory; however, cases of severe sensory and motor peripheral neuropathy have been reported. Patients with pre-existing symptoms (numbness, pain, or a burning feeling in the feet or hands) and/or signs of peripheral neuropathy may experience worsening peripheral neuropathy (including ≥Grade 3) during treatment with VELCADE. Patients should be monitored for symptoms of neuropathy, such as a burning sensation, hyperesthesia, hypoesthesia, paresthesia, discomfort, neuropathic pain or weakness. In the Phase 3 relapsed multiple myeloma trial comparing VELCADE subcutaneous vs intravenous, the incidence of Grade ≥2 peripheral neuropathy events was 24% for subcutaneous and 39% for intravenous. Grade ≥3 peripheral neuropathy occurred in 6% of patients in the subcutaneous treatment group, compared with 15% in the intravenous treatment group. Starting VELCADE subcutaneously may be considered for patients with pre-existing or at high risk of peripheral neuropathy.Patients experiencing new or worsening peripheral neuropathy during VELCADE therapy may require a decrease in the dose and/or a less dose-intense schedule. In the VELCADE vs dexamethasone phase 3 relapsed multiple myeloma study, improvement in or resolution of peripheral neuropathy was reported in 48% of patients with ≥Grade 2 peripheral neuropathy following dose adjustment or interruption. Improvement in or resolution of peripheral neuropathy was reported in 73% of patients who discontinued due to Grade 2 neuropathy or who had ≥Grade 3 peripheral neuropathy in the phase 2 multiple myeloma studies. The long-term outcome of peripheral neuropathy has not been studied in mantle cell lymphoma.Hypotension: The incidence of hypotension (postural, orthostatic, and hypotension NOS) was 8%. These events are observed throughout therapy. Caution should be used when treating patients with a history of syncope, patients receiving medications known to be associated with hypotension, and patients who are dehydrated. Management of orthostatic/postural hypotension may include adjustment of antihypertensive medications, hydration, and administration of mineralocorticoids and/or sympathomimetics.Cardiac Toxicity: Acute development or exacerbation of congestive heart failure and new onset of decreased left ventricular ejection fraction have occurred during VELCADE therapy, including reports in patients with no risk factors for decreased left ventricular ejection fraction. Patients with risk factors for, or existing, heart disease should be closely monitored. In the relapsed multiple myeloma study of VELCADE vs dexamethasone, the incidence of any treatment-related cardiac disorder was 8% and 5% in the VELCADE and dexamethasone groups, respectively. The incidence of adverse reactions suggestive of heart failure (acute pulmonary edema, pulmonary edema, cardiac failure, congestive cardiac failure, cardiogenic shock) was ≤1% for each individual reaction in the VELCADE group. In the dexamethasone group, the incidence was ≤1% for cardiac failure and congestive cardiac failure; there were no reported reactions of acute pulmonary edema, pulmonary edema, or cardiogenic shock. There have been isolated cases of QT-interval prolongation in clinical studies; causality has not been established.Pulmonary Toxicity: Acute Respiratory Distress Syndrome (ARDS) and acute diffuse infiltrative pulmonary disease of unknown etiology, such as pneumonitis, interstitial pneumonia, and lung infiltration have occurred in patients receiving VELCADE. Some of these events have been fatal. In a clinical trial, the first two patients given high-dose cytarabine (2 g/m2 per day) by continuous infusion
with daunorubicin and VELCADE for relapsed acute myelogenous leukemia died of ARDS early in the course of therapy. There have been reports of pulmonary hypertension associated with VELCADE administration in the absence of left heart failure or significant pulmonary disease. In the event of new or worsening cardiopulmonary symptoms, consider interrupting VELCADE until a prompt, comprehensive, diagnostic evaluation is conducted.Posterior Reversible Encephalopathy Syndrome (PRES): Posterior Reversible Encephalopathy Syndrome (PRES; formerly termed Reversible Posterior Leukoencephalopathy Syndrome (RPLS)) has occurred in patients receiving VELCADE. PRES is a rare, reversible, neurological disorder, which can present with seizure, hypertension, headache, lethargy, confusion, blindness, and other visual and neurological disturbances. Brain imaging, preferably MRI (Magnetic Resonance Imaging), is used to confirm the diagnosis. In patients developing PRES, discontinue VELCADE. The safety of reinitiating VELCADE therapy in patients previously experiencing PRES is not known.Gastrointestinal Toxicity: VELCADE treatment can cause nausea, diarrhea, constipation, and vomiting, sometimes requiring use of antiemetic and antidiarrheal medications. Ileus can occur. Fluid and electrolyte replacement should be administered to prevent dehydration. Interrupt VELCADE for severe symptoms.Thrombocytopenia/Neutropenia: VELCADE is associated with thrombocytopenia and neutropenia that follow a cyclical pattern, with nadirs occurring following the last dose of each cycle and typically recovering prior to initiation of the subsequent cycle. The cyclical pattern of platelet and neutrophil decreases and recovery remain consistent in the studies of multiple myeloma with no evidence of cumulative thrombocytopenia or neutropenia in the treatment regimens studied. Monitor complete blood counts (CBC) frequently during treatment with VELCADE. Measure platelet counts prior to each dose of VELCADE. Adjust dose/schedule for thrombocytopenia. Gastrointestinal and intracerebral hemorrhage has occurred during thrombocytopenia in association with VELCADE. Support with transfusions and supportive care, according to published guidelines. In the single-agent, relapsed multiple myeloma study of VELCADE versus dexamethasone, the mean platelet count nadir measured was approximately 40% of baseline. The incidence of bleeding (≥Grade 3) was 2% in the VELCADE arm and was <1% in the dexamethasone arm.Tumor Lysis Syndrome: Tumor lysis syndrome has been reported with VELCADE therapy. Patients at risk of tumor lysis syndrome are those with high tumor burden prior to treatment. Monitor patients closely and take appropriate precautions.Hepatic Toxicity: Cases of acute liver failure have been reported in patients receiving multiple concomitant medications and with serious underlying medical conditions. Other reported hepatic reactions include hepatitis, increases in liver enzymes, and hyperbilirubinemia. Interrupt VELCADE therapy to assess reversibility. There is limited re-challenge information in these patients.Embryo-fetal Risk: Pregnancy Category D. Women of reproductive potential should avoid becoming pregnant while being treated with VELCADE. Bortezomib administered to rabbits during organogenesis at a dose approximately 0.5 times the clinical dose of 1.3 mg/m2 based on body surface area caused post-implantation loss and a decreased number of live fetuses.ADVERSE REACTIONS: In the phase 3 VELCADE+melphalan and prednisone study in previously untreated multiple myeloma, the safety profile of VELCADE administered intravenously in combination with melphalan/prednisone is consistent with the known safety profiles of both VELCADE and melphalan/prednisone. The most commonly reported adverse reactions (≥10%) in this study (VELCADE+melphalan and prednisone vs melphalan and prednisone) were thrombocytopenia (48% vs 42%), neutropenia (47% vs 42%), peripheral neuropathy (46% vs 1%), nausea (39% vs 21%), diarrhea (35% vs 6%), neuralgia (34% vs <1%), anemia (32% vs 46%), leukopenia (32% vs 28%), vomiting (26% vs 12%), fatigue (25% vs 14%), lymphopenia (23% vs 15%), constipation (23% vs 4%), anorexia (19% vs 6%), asthenia (16% vs 7%), pyrexia (16% vs 6%), paresthesia (12% vs 1%), herpes zoster (11% vs 3%), rash (11% vs 2%), abdominal pain upper (10% vs 6%), and insomnia (10% vs 6%).
T:7”
T:10
”
VEL214CDNY7541_E_Master_BS_7x10_April_r2_FSU.indd 1 4/23/15 3:19 PM

Summer 2015 23
Takeda Oncology and are registered trademarks of Takeda Pharmaceutical Company Limited.Other trademarks are the property of their respective owners.
Copyright © 2014, Millennium Pharmaceuticals, Inc.All rights reserved. Printed in the USA USO/BOR/14/0015 11/14
In the phase 3 study of VELCADE® (bortezomib) administered intravenously vs dexamethasone in relapsed multiple myeloma, the most commonly reported adverse reactions (>20%) were nausea (52% vs 9%), diarrhea (52% vs 11%), fatigue (39% vs 25%), peripheral neuropathies (35% vs 4%), thrombocytopenia (33% vs 3%), constipation (30% vs 8%), vomiting (29% vs 3%), and anorexia (21% vs 2%). The most commonly reported serious adverse reactions were diarrhea (3%), dehydration, herpes zoster, pyrexia, nausea, vomiting, dyspnea, and thrombocytopenia (2% each) in the VELCADE treatment group and pneumonia (4%), hyperglycemia (3%), pyrexia, and psychotic disorder (2% each) in the dexamethasone treatment group.In the phase 3 VELCADE subcutaneous vs intravenous study in relapsed multiple myeloma, safety data were similar between the two treatment groups. The most commonly reported adverse reactions (≥10%) in this study were peripheral neuropathy NEC (37% vs 50%), thrombocytopenia (30% vs 34%), neutropenia (23% vs 27%), neuralgia (23% vs 23%), anemia (19% vs 23%), diarrhea (19% vs 28%), leukopenia (18% vs 20%), nausea (16% vs 14%), pyrexia (12% vs 8%), vomiting (9% vs 11%), asthenia (7% vs 16%), and fatigue (7% vs 15%). The incidence of serious adverse reactions was similar for the subcutaneous treatment group (20%) and the intravenous treatment group (19%). The most commonly reported SARs were pneumonia and pyrexia (2% each) in the subcutaneous treatment group and pneumonia, diarrhea, and peripheral sensory neuropathy (3% each) in the intravenous treatment group.In a single-arm, open-label study of retreatment with intravenous VELCADE in relapsed multiple myeloma, the most common adverse drug reaction was thrombocytopenia, which occurred in 52% of patients (grade ≥3: 24%). Peripheral neuropathy was experienced by 28% of patients (grade ≥3: 6%). The incidence of serious adverse reactions was 12.3%; the most commonly reported serious adverse reactions were thrombocytopenia (3.8%), diarrhea (2.3%), and herpes zoster and pneumonia (1.5% each).DRUG INTERACTIONS: Bortezomib is a substrate of cytochrome P450 enzyme 3A4, 2C19 and 1A2. Co-administration of ketoconazole, a strong CYP3A4 inhibitor, increased the exposure of bortezomib by 35% in 12 patients. Monitor patients for signs of bortezomib toxicity and consider a bortezomib dose reduction if bortezomib must be given in combination with strong CYP3A4 inhibitors (eg, ketoconazole, ritonavir). Co-administration of omeprazole, a strong inhibitor of CYP2C19, had no effect on the exposure of bortezomib in 17 patients. Co-administration of rifampin, a strong CYP3A4 inducer, is expected to decrease the exposure of bortezomib by at least 45%. Because the drug interaction study (n=6) was not designed to exert the maximum effect of rifampin on bortezomib PK, decreases greater than 45% may occur. Efficacy may be reduced when VELCADE is used in combination with strong CYP3A4 inducers; therefore, concomitant use of strong CYP3A4 inducers is not recommended in patients receiving VELCADE. St. John’s wort (Hypericum perforatum) may decrease bortezomib exposure unpredictably and should be avoided. Co-administration of dexamethasone, a weak CYP3A4 inducer, had no effect on the exposure of bortezomib in 7 patients. Co-administration of melphalan-prednisone increased the exposure of bortezomib by 17% in 21 patients. However, this increase is unlikely to be clinically relevant.USE IN SPECIFIC POPULATIONS:Nursing Mothers: It is not known whether bortezomib is excreted in human milk. Because many drugs are excreted in human milk and because of the potential for serious adverse reactions in nursing infants from VELCADE, a decision should be made whether to discontinue nursing or to discontinue the drug, taking into account the importance of the drug to the mother.Pediatric Use: The safety and effectiveness of VELCADE in children has not been established.Geriatric Use: No overall differences in safety or effectiveness were observed between patients ≥age 65 and younger patients receiving VELCADE; but greater sensitivity of some older individuals cannot be ruled out.Patients with Renal Impairment: The pharmacokinetics of VELCADE
are not influenced by the degree of renal impairment. Therefore, dosing adjustments of VELCADE are not necessary for patients with renal insufficiency. Since dialysis may reduce VELCADE concentrations, VELCADE should be administered after the dialysis procedure. For information concerning dosing of melphalan in patients with renal impairment, see manufacturer’s prescribing information.Patients with Hepatic Impairment: The exposure of bortezomib is increased in patients with moderate and severe hepatic impairment. Starting dose should be reduced in those patients.Patients with Diabetes: During clinical trials, hypoglycemia and hyperglycemia were reported in diabetic patients receiving oral hypoglycemics. Patients on oral antidiabetic agents receiving VELCADE treatment may require close monitoring of their blood glucose levels and adjustment of the dose of their antidiabetic medication.OVERDOSAGE:There is no known specific antidote for VELCADE overdosage. In humans, fatal outcomes following the administration of more than twice the recommended therapeutic dose have been reported, which were associated with the acute onset of symptomatic hypotension and thrombocytopenia. In the event of an overdosage, the patient’s vital signs should be monitored and appropriate supportive care given.PATIENT COUNSELING INFORMATIONAdvise patients to contact their physicians if they experience the following symptoms:Dehydration/Hypotension, such as dizziness, light-headedness or fainting spells, or muscle cramps. Cardiac: swelling of feet, ankles, or legs, or other heart-related problems.Respiratory: shortness of breath, cough, or other lung problems.Hepatic: jaundice or right upper abdominal pain.Dermal: rash, severe injection-site reactions, or skin pain. Discuss the option for antiviral prophylaxis for herpes virus infection.Peripheral Neuropathy and Nervous System, such as new or worsening tingling, numbness, pain, a burning feeling in the feet or hands, or weakness in the arms or legs. Advise patients to contact their physicians if they experience symptoms possibly indicative of PRES or PML such as convulsion, persistent headache, reduced eyesight, blurred vision, confusion, lethargy, altered ability to think, or difficulty walking.Other: increase in blood pressure, bleeding, fever, constipation, or decreased appetite.In addition, counsel patients on the following:Pregnancy/Nursing: Advise patients to use effective contraceptive measures to prevent pregnancy during treatment with VELCADE. Instruct them to report pregnancy to their physicians immediately. Advise patients that they should not receive VELCADE while pregnant or breast-feeding. If a patient wishes to restart breast-feeding after treatment, she should be advised to discuss the appropriate timing with her physician.Concomitant Medications: Advise patients to speak with their physicians about any other medication they are currently taking.Diabetic Patients: Advise patients to check their blood sugar frequently if using an oral antidiabetic medication and to notify their physicians of any changes in blood sugar level.Ability to Drive or Operate Machinery or Impairment of Mental Ability: Advise patients not to drive or operate machinery if they experience fatigue, dizziness, syncope, or orthostatic/postural hypotension.
Please see full Prescribing Information for VELCADE at VELCADE-hcp.com.
Brief Summary (cont’d)
T:7”
T:10
”
VEL214CDNY7541_E_Master_BS_7x10_April_r2_FSU.indd 2 4/23/15 3:19 PM

24 FCS The Magazine
Donna Ott’s decision to pursue a career in nursing placed her on a path that led her away from a small factory town in western Massachusetts.

Summer 2015 25
Growing up in a small, working-class town in western Massachusetts, Donna Ott prepared to follow in the footsteps of most of her friends and family and planned to roll up her sleeves at the Spalding sporting goods factory.
But fate had other plans for the shy 17-year-old. The factory raised the minimum age for workers to 18 making Ott ineligible for employment. So, the high school junior tried her hand at waitressing. When that didn’t pan out, she took a job as a nurse’s aide in a total-care nursing facility and instantly knew that working with patients was her destiny.
“Though I had to do it all, including changing bed spans and everything else, I fell in love with the patients, taking care of them and trying to make a difference,” Ott, who is now 50, says with just a hint of a Northeastern accent.
She worked during high school and continued after graduation in order to save money for college to pursue a degree in nursing. After she got her diploma from Holyoke Community College, she left her hometown of Chickopee in 1990 and headed south to Florida. She landed in Wellington and relished having a fresh start in life as a new bride.
She began working at the Palm Beach Cancer Institute. Eventually, it merged with Florida Cancer Specialists & Research Institute in June 2013. Always the optimist, Ott, working as a charge nurse, knew that change would bring opportunity, and she embraced the big merger and her new nursing role with FCS. “I saw the need and I knew where health care was going and knew it would be good,” she says.
During 25 years as a registered nurse, Ott has experienced moments when she thought she might want to make a change, but she says there was always one thing that kept her going: the patients.
“I have known some of my patients for 16 years now,” she says. “Some of them are Facebook friends, some have my cell number, we’re that close,” she says. One female patient in her 50s with metastatic breast cancer followed Ott to the FCS Wellington office after the merger.
Though she has only worked with FCS for two years, the transition to the team seemed seamless. Ott had known many of the physicians, including Elisabeth McKeen and James Harris for 25 years — pretty much the span of her entire career.
Ott is part of a three-nurse team at Wellington. The close-knit relationships among FCS staff are a key to the team’s success, according
to Ott. “We’re so small, we have to work effectively together,” she says. “We support and reassure each other. We are family.”
Beyond her regular nursing responsibilities, Ott is actively involved in several cancer-related annual events such as Relay for Life and Making Strides. She also gets a chance to use her experience and leadership skills by serving on the 21-member FCS Clinical Directions Team (CDT) committee. “We develop SOPs, troubleshoot problems, discuss current issues and listen to feedback,” she explains. “As a spokesperson, my role is to roll out that information throughout the six offices in the Southeast region.”
Ott has been a member of the Oncology Nursing Society for a number of years and this year is looking forward to deepening her knowledge by attending the 40th annual Nursing Congress in Orlando.
“I am really looking forward to it,” she says. “I am excited and hoping to learn more about trends in genetics this year.”
She’s also looking forward to another change. The Wellington office will move to a newer building where FCS will occupy the entire floor, making it possible to expand from 13 chemo chairs to 22.
“I’m thrilled,” Ott exclaimed. “It’s only a mile away, but it’s a big deal for all of us.”
Ott contends that working as a caregiver has made her more compassionate. “When I started as a teenager, I was clueless about aging,” she confessed. “Working in nursing and health care has given me a different perspective. People go through life not appreciating things, but our cancer patients help us keep that in sharp focus every day.”
When she is tempted to complain about a bad hair day, she thinks of her patients who are happy just to have hair. “How can I complain?” she reflects. “Being a nurse helps me be grateful for all I have and to remember every day that life is precious.”
It’s been 25 years since Ott relocated to the Sunshine State for a fresh start. Five years ago, with two grown children, she ventured into another new adventure: a second marriage to her husband, Michael Ott.
At her home in Royal Palm Beach, Ott enjoys quiet pursuits — gardening and hiking. “But when I’m at work I’m very outgoing with everyone,” she says.
This career caregiver has aced nursing.
Nursing Brings Donna Ott Out of Her ShellCareer has spanned 25 years BY ZANDRA WOLFGRAM
NURSE SPOTLIGHT

26 FCS The Magazine
FEATURE
FCS’s Rx to Go is committed to delivering the latest oral oncology medications to patients.
Summer 2015 27
Rx to the RescueIn-house pharmacy center plays integral role to treating patients while delivering to FCS bottom line BY ZANDRA WOLFGRAM
You know, they make a pill for that … Oncology is targeting cancer with
unprecedented oral drug therapies. Today, nearly 25 percent of cancer
drugs are available in a pill form. With the FDA’s fast-track approvals for drugs showing clear promise, there have been as many as 35 new drugs come to market in the last several years — more than ever before. More drugs mean more options for patients, but it also means more to manage for Florida Cancer Specialists & Research Institute (FCS)’s Rx to Go pharmacy center.
Located in Fort Myers within the corporate offices of FCS, Rx To Go, led by pharmacist Ray Bailey, is a specialty oral oncology pharmacy focused on delivering newer oral oncology medications to FCS patients.
“I have the vision, but my team does all the hard work,” Bailey says in an effort to give credit where it is due.
The 50-member Rx to Go oncology pharmacy team, whose day-to-day operation is managed by Katherine Hogan, RPh, Pharmacy Manager; Natasha Khrystolubova, RPh, BCOP, Clinical Coordinator; Jackie Jimenez-Capote, RPhT, Manager of Financial Services; and Kara Sammons, RPhT, Supervisor of Pharmacy Technicians,; all play a vital role in FCS.
Cancer drugs can be hard to get. That’s where Rx to Go comes to the rescue. “The secret is we are part of the FCS practice, so our pharmacists have access to our patient’s EMR (electronic medical record), so we have all the pathology and doctor notes to print out and send to the insurance companies to expedite things,” Bailey explains.
Cancer drugs are also expensive. Bailey estimates that on average typical cancer-fighting drugs cost $6,000 to $11,000 a month. Being able to write a prescription doesn’t matter if the patient cannot afford it. Once again, Rx to Go steps up with a four-member financial team specially trained to provide assistance with insurance qualifications and co-pays, making it easier to navigate paperwork and meet insurance requirements.
“Prior to us being here, patients were frustrated because they would go to the local drug store and the pharmacy wouldn’t have the drugs, and then they would try to figure out where to go, such as a specialty pharmacy. If they were available and they ran the claim, they were often not affordable for the patient forcing them to go without,” Bailey says.
In addition to delivering medications throughout the state of Florida to FCS patients’ homes, Rx to Go is licensed in an additional 30 or so states, so patients can continue to receive their medication while traveling.
As more drugs are prescribed, Rx to Go plays a critical clinical role in patient care. “There are benefits to oral drugs compared to having an IV administered, but there are pitfalls when you give patients pills — and they don’t take them. So it’s our job to help patients manage their medications. We do that by creating a customized care plan for each patient.”
And then there are side effects. “We tell our patients everything to expect, talk about pre-medicating, how to manage side effects. Patients need to understand that although they are taking pills it is still their chemotherapy regimen and they have to take the medication as prescribed for it

28 FCS The Magazine
to be effective for them. Helping our patients understand and getting them to buy-in to the value of the therapy is our most important role,” Bailey says.
Since it opened in 2008, Rx to Go has become an integral part of FCS’s treatment program and a successful internal business. With Bailey at the helm since 2009, the internal pharmacy center has become the central repository for all FCS patients’ drugs. The pharmacy also upgraded to a software system better suited for a high touch specialist pharmacy. Those changes have helped Rx to Go expand to a formulary of approximately 60 drugs. Nearly 250 prescriptions are processed daily resulting in an annual revenue stream of $200 million.
With an eye on industry trends, Bailey has helped to design a new 12,000 square-foot state-of-the-art pharmacy to be completed in August 2015. “We’re braced for more drugs and more growth,” he says.
But Bailey isn’t sitting idly by. You can find this 30-plus year veteran of the pharmacy industry out and about calling on insurance and pharmaceutical companies in an effort to
leverage FCS’s success story. “Explaining why and how our model works for our patients helps to make sure we get access to drugs and ensure payers allow us to bill,” he says. “If you don’t get out there and advocate for your pharmacy, no one knows what you do or what your capabilities are.”
Bailey’s palm-pressing efforts have worked. With support from FCS founder and president William Harwin, M.D., — who originated the idea of an in house pharmacy — FCS was able to get Blue Cross/Blue Shield of Florida, Aetna, Inc. and Cigna on board with more to come. “There are several national plans and PBMs that we are not going to give up on,” Bailey says.
With a dedicated team, updated software and state-of-the-art facilities, Rx to Go is well positioned to help FCS keep its competitive advantage in community oncology care. “We are a practice that doesn’t cut any corners,” Bailey says. “We are going to exhaust all options as best we can; that’s what cancer is all about. And right now our patients demand nothing less.”
We are a practice that doesn’t cut any corners. We are going to exhaust all options as best we can; that’s what cancer is all about. And right now our patients demand nothing less.”— RAY BAILEY, RX TO GO
FEATURE
Pharmacist Ray Bailey leads the Rx to Go management team.

Summer 2015 29

30 FCS The Magazine
FCSevents
1. NAPLES RELAY FOR LIFE Pictured (L to R): Pam White, Virginia Panek, Barb Scott, Sara Fernandez, Judi Thompson Marina Garza, Becky Kendall, Maria Johnson, Nancy Bowers, Lois Poel, Paula Zuluaga and Rosemarie Sudano2. CAPE CORAL RELAY FOR LIFE Pictured (L to R): Dr. Faithlore Gardner and Dr. Michael Raymond
3. TALLAHASSEE RELAY FOR LIFE Pictured (L to R): Cheryl Holm and Letitia Owens4. INVERNESS, CITRUS COUNTY RELAY FOR LIFE Pictured (L to R): Servillano Dela Cruz, MD-CRV/IVS; Christine Soldo, RN-CRV; Karen Genzardi, RN-IVS; William Harrer, MD-IVS/CRV; Brooke Boleware, FC-INV; Julie Anning, RN BA PL; Theresa Simms, FC-INV; Dallas Thacker, MA-IVS; and Chris Hightower, OM-CRV/IVS
5. NEW PORT RICHEY RELAY FOR LIFE Pictured (L to R): Margaret Galon, Peggy Dinsmore, Joan Covell, Ester Bernardo, Skyshane Mustian, Jody Colwell and McKenna Colwell6. VERO BEACH RELAY FOR LIFE Pictured (L to R): Katrina Thompson, OM; Dr. Raul Storey; Malia Keen, Head Nurse; Jane Anderson, RN; and Devin Jenkins
1. 2.
3. 4.
5. 6.

Summer 2015 31
FCSevents
7. TALLAHASSEE WOMEN OF INTEREST LUNCHEON Pictured (L to R): Physician Liaison Sandra Brooks, Congresswoman 2nd District of Florida Gwen Graham and Tallahassee Office Manager Deborah Mabry8. GRACEFUL ART OF SENIOR CARE GALA Congratulations to Dr. Geetha Kamath on receiving the Bon Secours Health System
Good Help Award. Pictured (L to R): First Row — Veronika Beard, Pat Drogon, Dr. Geetha Kamath and Susan Easter; Second Row — Danielle Carlton, Jaynita Paragi, Josephine McDougall, Dr. Jay Kamath and Claudia Rosa.9. HUMANITARIAN WORK IN HAITI After three years of hard work, the community center in Haiti, overseen by Dr. Ralph Gousse, is open and functioning well. The community
center serves young boys and girls — teaching English, sewing, cooking, arts, crafts and more. The next area of focus will include dental hygiene for all the children.10. FCS ANNIVERSARIES Pictured (L to R): Jeff Rubin and Evelyn Deaton both celebrate 25 years with FCS — congratulations and thank you for all of your outstanding work over the years!
7. 8.
10.
9.

32 FCS The Magazine
11. THE LAST DAY OF CHEMO TREATMENT Pictured (L to R): Dr. Andres Bhatia and patient Margret Weeks celebrating in Gainesville. 12. FCS PHYSICIANS PANEL IN TAMPA WITH DR. OZ SPONSORED BY ABC-TV Pictured (L to R): Kerry Chamberlain, DO; FCS Physician Liaison
Monica Clark; Dr. Mehmet Oz; Gail Wright, MD; and FCS Physician Liaison Manager Maria Ramos-Person. 13. INAUGURAL GREEN BELT CLASS Pictured (L to R): First Row — Jackie Jimenez Capote, Melody Chang, Melisa Chandler, Katie Goodman and Chelsea Jones. Second Row — Kathy Hogan, Tiffany Bauman, Sarah
Cevallos, Alison Murty, Sam Watkins, Inga Gonzales, Kim Delgado, Lois Brown, Kristi McComack, Annie Pigue, Tara Ruska, David Curry, KK Moore and Libby Slater. Third Row — Gary MacDougall, Eric Grindstaff, Christina Sievert, Chris Houser, Jeff Rubin, Jeff Esham, Jeremy Behling and Todd Schonherz
11. 12.
13.
FCSevents

Summer 2015 33
FCSc.a.r.e/core values
Early in April, the Leadership Team proudly launched the FCS C.A.R.E./CORE Values Program. At FCS, core values shape the culture and define the character of our company; core values guide how we behave
and conduct ourselves with patients and with one another. The FCS core values were developed as a result of an extensive discussion and examination of our corporate culture.
The core values of an organization are those fundamental beliefs that guide our internal conduct, as well as our relationships with the outside world. At Florida Cancer Specialists, core values shape the culture and define the character of our company; core values guide how we behave and conduct ourselves with patients and each other. The core values were renamed as our “C.A.R.E.” Values to better reflect the guiding principles in which we believe.
CONTINUOUSLY SUPPORT THE PATIENTOur team delivers results by providing compassionate oncology and hematology services with continued focus on the patient.
ALWAYS DO THE RIGHT THINGWe are committed to personal excellence, accountability and integrity. We abide by the highest regulatory standards, perform in the most ethical manner and take responsibility for our actions.
RESPECTFULLY ENGAGEWe foster positive relationships, encourage diversity of thought and promote trust among our teams and customers. We encourage healthy debate and respect the thoughts and opinions of others. We believe that the talents, skills and expertise of our people are our most important assets.
EXCEED EXPECTATIONSWe strive to provide excellence in all that we do. We create a standard of caring that goes above and beyond while embracing change in support of continuous improvement for our patients.
HOW CAN YOU EMBODY THE C.A.R.E. VALUES?Never stop asking questions. What are some ways that you, as an individual, can support patients? When there are differing opinions among employees, how can you encourage healthy debate and still
ensure that all employees are respectful of one another? These core values help define FCS, and they start with each and every employee and volunteer.
Please continue to consider and use these C.A.R.E./CORE VALUES to enhance your relationships with your team members, physicians, vendors and, most importantly, with our patients. By personally demonstrating our C.A.R.E./CORE Values in everything you do, you help educate patients about Florida Cancer Specialists and represent the mission, vision and the very heart of our organization.
Florida Cancer Specialists C.A.R.E. About Their PatientsFor FCS, caring is a core value BY ELAINE GANICK
Daytona Beach Cancer Center and New Smyrna Beach Cancer Center staff members promoting FCS C.A.R.E. Values. Pictured (L to R): First Row: Jessica Muh, Mary Carn and Gina Helsel; Second Row: Pam Venneri, Kim Heller and Adam Helsel

34 FCS The Magazine
“If you want others to be happy, practice compassion. If you want to be happy, practice compassion.” — Dalai Lama
Akind word, a little snack, a fluffed-up pillow … sometimes it’s the little things that make a big difference. Especially to anyone who is not
feeling well and perhaps even more so to someone undergoing cancer therapy treatment.
Lifelong volunteer Val Vance understands this better than most. And this is precisely why Florida Cancer Specialists Foundation selected this tireless 60-something last December to lead the charge as its volunteer program manager out of the Foundation’s Sarasota office.
Though she has actively served such deserving national causes as the American Cancer Society, the Alzheimer’s Foundation and the American Red Cross for many years, volunteerism isn’t all Vance brings to her new hands-on leadership job role. As a 25-year retired veteran of S.C. Johnson Wax company, Val is no stranger to team building, large-scale company rollouts and project management. Though the Michigan native confesses she had a little initial trepidation about working daily with oncology patients, she soon overcame that uneasiness.
“When I got there it was so uplifting and warm. It really wasn’t anything like what I expected,” Vance says.
Founded in January 2011, Florida Cancer Specialists Foundation is dedicated to providing non-medical support (up to $1,500) for qualifying cancer patients undergoing treatment. This could mean help with a mortgage payment, car payment and utility bills. The volunteer program Vance leads does background checks on all applicants and immerses qualified volunteers in targeted training to ensure all of the patients the
program touches receive consistent, quality care administered by compassionate providers.
“This program is not only in line with FCS Foundation’s mission, but it supports FCS C.A.R.E. values, the first of which is to ‘continuously support the patient,’ ” Vance stresses.
The volunteers are designed to be a helpful extension of the Florida Cancer Specialists & Research Institute (FCS) health care staff, and so far the reaction is positive. “It’s a very good program,” says Donna Ott, a charge nurse in the Wellington office in Palm Beach County. “Our patients love it. And for us to have someone there to get them what they need it’s a big help. A lot of the volunteers have been through cancer and so they know what the patients are going through, which is always helpful.”
In just four months Vance has rolled up her sleeves and gotten right down to business. She saw to the opening of six FCS patient support program facilities and expanded the program to a core of 25 specially trained volunteers.
Like many other areas of FCS, expansion is on the horizon. “We are projected to open another 12 to 15 sites and grow to 40 volunteers by the end of July 2015,” Vance says.
There are established volunteer programs at FCS offices in West Palm Beach, Tampa and Bradenton West, one newly opened in Bonita Springs and three more planned for Clearwater, Port Charlotte and Fort Myers and Naples West. Many offices are beginning to request the program, but for now, Vance says the site locations are selected based on where the patient volume and need is greatest.
‘Volunteering is For Everyone’Val Vance Leads FCS Volunteer Program BY ZANDRA WOLFGRAM
VOLUNTEER PROGRAM

Summer 2015 35
Each volunteer program site launch is about a four to six-week process and includes a two- to three-hour training orientation.
For Vance, the personal reward from giving has always been worth the time and effort expended. “Volunteering has truly changed my life,” Vance says. “It’s a wonderful way to give back to your community and the patients we serve … a smile, a warm welcome or blanket might be just the thing that makes a patient feel special and cared for that day.”
Vance finds volunteering gives her added energy to enjoy favorite activities, including traveling, boating, sailing and spending time with her two dogs, Bailey and P.K., and her 14 grandchildren.
“I like to say volunteering is for everyone,” Vance says. And if that doesn’t work. She pulls out the dog-eared article she likes to reference on the first day of orientation and lets the facts speak for themselves. “It’s proven that volunteers live longer,” she says with a laugh. “So there really is no downside to it.”
Turns out she’s right. According to an extensive review of multiple studies conducted at the University of Exeter Medical School published in August 2013, people who volunteered on average lived up to 20 percent longer, sometimes more. The studies further showed they were also healthier and happier.
For those who would like to live longer and feel better by lending a hand, there are plenty of ways to do it. In addition to the FCS Foundation patient support program, the Foundation office could use help with administrative duties, patient casework and maintaining the website. You can also help out at a special event or show your support by making a corporate, individual or in-kind donation to the FCS Foundation.
For upcoming events and more information on the patient support volunteer program, visit Foundation.FLCancer.com. To contact the Volunteer Program Office, call (941) 677-7191 or email [email protected].
An FCS volunteer chats with a patient at the Tampa Care Center. Volunteers find that they are energized by the
experience of brightening patients’ days.
TOP: An FCS volunteer chats with a patient at the Tampa Care Center. Volunteers find that they are energized by the experience of brightening patients’ days. CENTER There is evidence to suggest that volunteers live longer. FCS Foundation volunteers wouldn’t disagree. BOTTOM: Volunteers, including Gloria Winston, comfort both patients and their family members.

36 FCS The Magazine
Dr. Maen Hussein is a busy man. From the looks of it, he barely has time to sleep, let alone run a thriving practice and give back heavily to his community. However, this husband and father of two rambunctious boys never misses a beat.
At home and on the job, his passion is clear.Hussein is a specialist in hematology and oncology at the FCS Villages
location in Lady Lake. From this central point, he sees patients in Tavares and Leesburg. In all, that’s between 700-800 patient encounters per month. In addition, he is the principal investigator for lung cancer and other clinical trials at the FCS location.
FINDING HIS PASSIONHailing from Jordan, Hussein attended medical school at the University of Jordan, then completed his residency in Rhode Island and a fellowship at St. Louis University to hone his skill. In his early medical school days, he would have been the last person to believe that oncology would be his passion.
“I hated oncology in medical school,” Hussein remembers. “It was the last year of medical school when I became fascinated by how people survived cancer.”
Listening to him talk about cancer gives even the biggest skeptic hope. Perhaps through his own research, Hussein has come to believe that the 21st century will be the “Cancer Century.” That is, the time when modern medicine tames this devastating disease.
“Communicable diseases used to kill millions of people,” he explains, “but after discovering antibiotics, they are no longer death sentences — they are highly treatable.”
In the same way, Hussein likens coming advances in cancer treatment and care to a communicable disease that can be cured.
It’s this access to groundbreaking research that truly fuels Hussein’s fire for his profession. As a principal investigator, he is able to provide patients with promising drug therapies that can dramatically affect their disease. Most do better than expected with these experimental protocols.
Hussein’s excitement is evident when he explains how coming therapies may be able to starve cancer — or turn its switch “off” and halt the disease. Understanding how a patient’s own immune system can be stimulated to kill cancer is a particular interest for this oncology-averse medical student turned researcher.
In fact, Hussein co-authored an abstract that was presented at the American Society of Clinical Oncology (ASCO) annual meeting in Chicago this past summer.
ENRICHING HIS FAMILYHussein is passionate about his family and their role in the community. His wife, a nursing clinical instructor and hospice professional who will complete her studies this fall to become a nurse practitioner, and their two boys live in Leesburg. Zachariah is 11 and Zade is 9. The entire family enjoys physical activity, exploring the world and community service.
Hussein played soccer during his undergraduate days, and his finesse for the game was handed down to his sons. Now, he assists in coaching Zachariah’s travel soccer team and also plays adult soccer league at the YMCA.
In a few months, Hussein’s passion for soccer and his leadership vision will culminate in The Villages Cup, a nationwide soccer tournament with 80 competing teams from all over the U.S. FCS is the main sponsor of the tournament, and Hussein is working closely with organizers.
The family also enjoys Boy Scouts together — Hussein is on the local board — and traveling both the U.S. and internationally. They love to water ski, snow ski and swim. Together, the four have explored Norway, London, Colorado, upstate New York, the Florida Keys and most every other Florida location in between.
Not to mention Legoland; Hussein and his sons are avid Lego fans and collectors.
“We have over 300 Lego sets in our house,” he says. “Some of them are still too old for my sons, so we are keeping them in boxes until they are ready. We’ve made Lego models of the Pirates of the Caribbean ‘Black Pearl,’ the Harry Potter Hogwarts castle, the Millennium Falcon (from Star Wars) and more.”
“I’ve seen every kids’ movie in the last five years,” Hussein laments. “But I focus on my family because I want them to remember that I was around — so they will remember me when they get older!”
GIVING BACK — A WAY OF LIFEHussein’s wife got him involved in the Leesburg Hospital Community Clinic, a free clinic where she volunteers. He now sees patients free of
Paying It ForwardDr. Maen Hussein leads by example when it comes to community investment BY TISHA CREWS KELLER
DOCTOR SPOTLIGHT
COUR
TESY
OF
DR. M
AEN
HUS
SEIN

Summer 2015 37
charge for blood disorders and cancer complications. Through FCS’s generosity, Hussein is able to help qualified patients at his main office using resources the company sets aside for the medically needy.
Asked why he gives back so much to his community, Hussein easily answers. He believes that helping the community is really a way of helping his family.
“I do many charity events, through work and personally,” he explains. “Whether it’s the Boys and Girls Club locally or the Florida Cancer Foundation statewide, these are great causes.
“Things like the Boys and Girls Club get kids off the streets and involved in something productive — and that makes my community a better, safer, more wonderful place. That’s good for me and my family.”

38 FCS The Magazine
I spent three days at the Community Oncology Alliance (COA) Meeting in Orlando recently. Once upon a time, COA was a tiny organization, cobbled together in crisis as Congress was contemplating the major changes to the oncology delivery system for Medicare in the early 2000s. These changes eventually became the Medicare Modernization Act in 2003.
Back then, the community oncologist, the one who provides “world class medicine, hometown care,” was either completely misunderstood by policymakers or worse, understood to deliver poor quality at high prices. The challenge of the oncologists joining COA was enormous: convince every stakeholder in cancer care that we deliver the highest quality cancer care in the world to the greatest number of patients in the most cost-effective way possible.
I’m happy to report that after years of doing the heavy lifting of research and education that it took to refute the negative perceptions, COA has been successful. There isn’t one major gathering of thought leaders or policymakers or payers in the cancer policy world that doesn’t put COA on the top of the invitation list. I’m proud of the role that the FCS doctors have played in this organization with their consistent support.
As I sat there in the ballroom on the last day, it struck me that, going forward, everyone in the room can do better: doctors, payers and even patients. Thankfully, we have gone beyond yelling at each other and impugning each other’s motives. All players would benefit from a little introspection.
DOCTORSWhen we discuss improving the quality of cancer care, doctors tune out because they are all perfect. Everyone thinks that his or her quality is as high as it can possibly be, so what’s the point of going down this road? But a little humility would help here. The insurers would tell you, if they could tell you, that there is way too much variation in how we do things. So, for curable diseases (adjuvant breast, adjuvant colon, DLCL, etc.), we all open the standard recipe book and use the exact same regimens. There isn’t much variation there. The differences between docs are seen in use of growth factors and in radiology services, particularly scans done as part of “surveillance” on patients who are probably already cured. One of the heads of BCBS said that in their recent review (unpublished of course) 80 percent of breast cancer patients with tumors
less than 1cm, (node negative) were getting PET scans done at diagnosis. All those physicians ordering those PETs would tell you that they are high quality physicians.
In incurable diseases, the variations in practice patterns are huge. I recently was asked for a second opinion on a breast cancer patient. The doctor treating her in Georgia had started Avastin with chemotherapy at a time when Avastin had this FDA indication. But then when the chemo agents failed her, he kept the Avastin going and going and going for over three years while cycling through different chemo drugs. Payers are not impressed with this degree of quality.
There are many other areas for improvement on our part, but the final point I would make is that not once ever have I heard an oncologist ever admit out loud, after a patient passes away, that maybe, just maybe, the patient received too many lines of therapy — too much chemo. We all use just the right amount of chemo, not too much, not too little. In contrast, I have had many family members tell me later that if they could do it over again, they would have advocated for their loved one for earlier hospice care.
PAYERSNow we are on familiar ground, we all know the payers have to do better. But doctors would do well to remember that the old axiom that patients hate their insurance companies is just a myth. They actually love their insurance companies and trust their insurance company’s judgment on what care is necessary and what care is not. The data clearly shows that the pendulum has swung from when patients felt that insurance companies withheld needed stuff, to now, where patients look more skeptically at their doctor when he orders something that is not covered. Anecdotally, doctors have a tendency to remember the one or two patients who appeal to the insurance company when something is denied, but the rule, rather than the exception, is that patients are pretty passive and just want the correct treatment without a mailbox full of bills. The insurance companies have done a great job of marketing their brand, and the sad fact is that they are trusted more often than you are when there is a conflict. But they need to look at all the costs of cancer care and realize that drugs are only 27 percent. Almost half the cost is ER visits and hospitalizations. The recent United pilot study should teach them that the quality goes up, the costs come down and the patient
is more satisfied if payers work with us to keep patients in their community oncology offices and not in 340B centers and academic centers. By concentrating on drug margins they have pushed practices out of business and raised their own costs. We are not the enemy; cancer is the enemy, and we are the army that has to fight it. We need to be respected, and we need the proper weapons.
PATIENTSI know, this is heresy. Patients are victims and have no role in raising the quality of their own care, and the finances of cancer care are far too intimidating and complex for them to have a say or get involved. Your father’s generation may have fit that description but not the new digital patients. They have a right to expect full and transparent information about their diagnosis, treatment options, and, yes, all toxicities of those treatments, even the economic toxicity. But patients really need to know crucial facts that influence their care, and one of the most fundamental is the proper goal of their treatment plan. In a recent NEJM study (Weeks et al.), 60 percent of stage IV lung cancer patients at Dana Farber thought that their treatment would be “curative.” This is at Harvard where the doctors are actually all perfect. So patients need a better understanding of curable situations versus incurable ones. It is OK to pray for miracles, but if we base our treatment plan on miracles then there simply will not be any limits to what treatments patients will subject themselves to. There won’t be any reason not to get a second and third and fourth opinion at expensive and prestigious academic centers so that every conceivable drug or surgery can be administered before death. “Patient Advocates” need to resist the temptation to be “radical treatment advocates.” Instead of the friends and family undermining the trust that the patient has in the health care team, they should be humble, as we all should, and learn about hospice and palliative care and they should accept that in all cases, modern cancer treatment does have limits and can be harmful if given beyond futility.
The change in tone of all the stakeholders at the COA meeting from “I’m OK, you are not” to “we all have to work together” was a great thing to see. New payment models that stress outcomes and not procedures are already here, and we will see many different flavors in the coming years. And the future will be better, if we believe that we can all do better.
Everyone Can Do Better BY DR. SCOTT TETREAULT
what's on your radar?the radar screen

Summer 2015 39
Additional information will be available on our website www.ResearchToPractice.com later this summer.
This daylong program will feature 16 renowned clinical investigators specializing in specific tumor types and use an informal, conversational style to review many of the year’s newest and most important data sets in a multitude of different cancers, including breast cancer, gastrointestinal cancers, genitourinary cancers, lung cancer, skin cancer, Hodgkin and non-Hodgkin lymphoma and multiple myeloma.
Neil Love, MD and Research To Practice will be back at this year’s FCS Clinical Summit
SAVE THE DATE — Saturday, October 24, 2015
Sponsored by:
Research To Practice is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians.
A Regional Symposium Focused on the Application of Emerging
Research Information to the Care of Patients with Common Cancers
This activity is being hosted in association with
YiR-FCS_15_Orlando-AD_vFINAL2fr.indd 1 5/18/15 10:07 AM


















