Innovative Strategies Strive Bundled Payment Success ... Vest_Innovative... · Innovative...
42
Innovative Strategies Strive Bundled Payment Success Avoiding Readmissions and Adverse Outcomes
Transcript of Innovative Strategies Strive Bundled Payment Success ... Vest_Innovative... · Innovative...

Innovative Strategies Strive Bundled Payment Success
Avoiding Readmissions and Adverse Outcomes
SIGNATURE MEDICAL GROUPAwardee Convener CMS Bundled Payments for Care Improvement (BPCI)
Convener for Largest Orthopedic Bundled Payment Initiative
Managing over $1.3B in annual spend

Signature Episode Management History• BPCI Awardee Convener
• Began development in 2011• Scaled from
• 6 provider groups, 80 physicians and $25 million in Medicare spend to• 60 provider groups, 2,000 physicians and $1.3 billion in Medicare spend in• 12 months
• Maternity Care Home• Missouri statewide program serving 2,000+ Medicaid moms (2013)
• Commercial bundled payments in orthopedics• Episode focus
• Historical - Orthopedic and Maternity Care• Comprehensive episode management (operational strategy)
• Medical and surgical episodes (episode/disease state agnostic)• Medicare, Medicaid, Medicare Advantage and commercial (payer agnostic)• Pre-admission, acute and post-acute management (savings agnostic)
Confidential and Proprietary
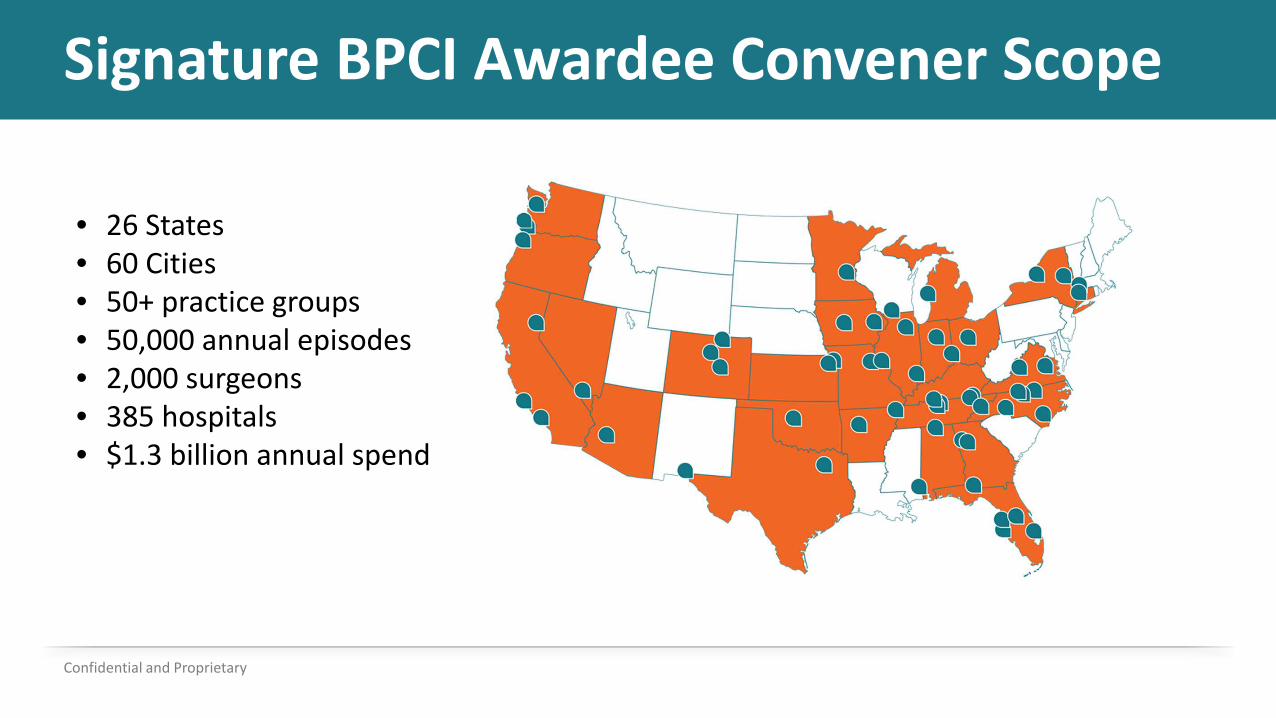
Signature BPCI Awardee Convener Scope
Confidential and Proprietary
• 26 States• 60 Cities• 50+ practice groups• 50,000 annual episodes• 2,000 surgeons• 385 hospitals• $1.3 billion annual spend
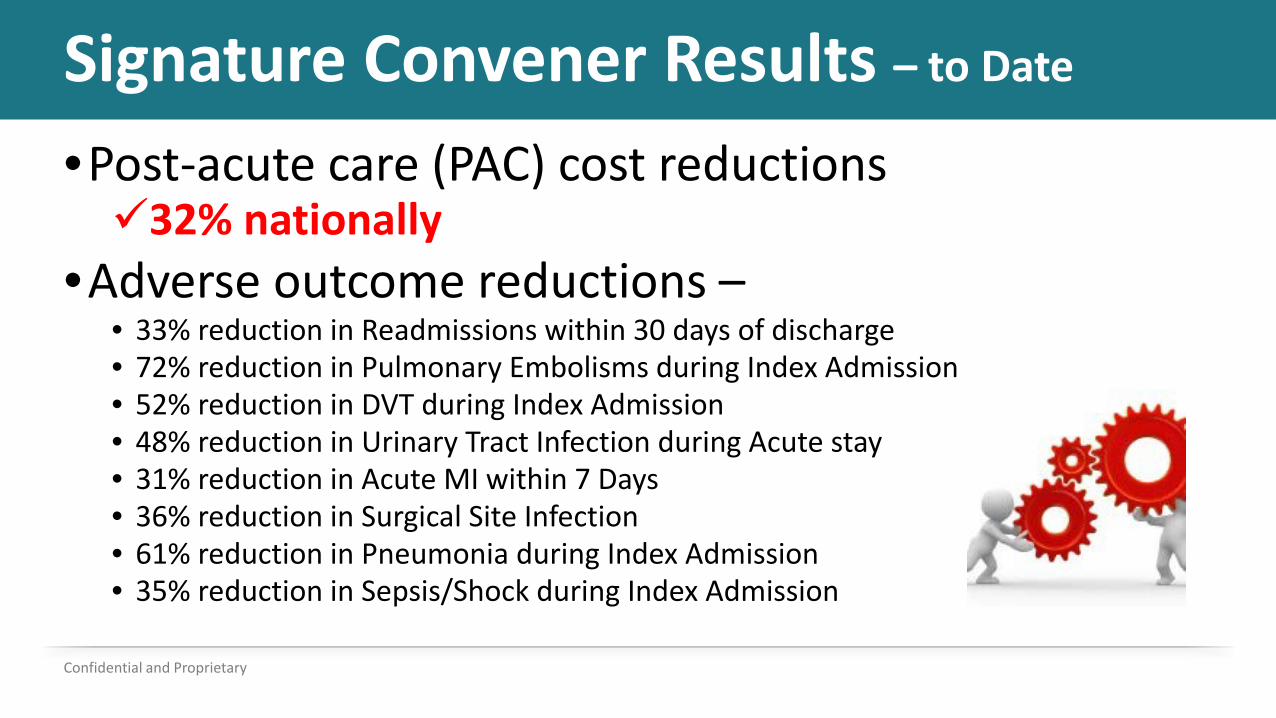
Signature Convener Results – to Date
•Post-acute care (PAC) cost reductions 32% nationally
•Adverse outcome reductions –• 33% reduction in Readmissions within 30 days of discharge• 72% reduction in Pulmonary Embolisms during Index Admission• 52% reduction in DVT during Index Admission• 48% reduction in Urinary Tract Infection during Acute stay• 31% reduction in Acute MI within 7 Days• 36% reduction in Surgical Site Infection• 61% reduction in Pneumonia during Index Admission• 35% reduction in Sepsis/Shock during Index Admission
Confidential and Proprietary
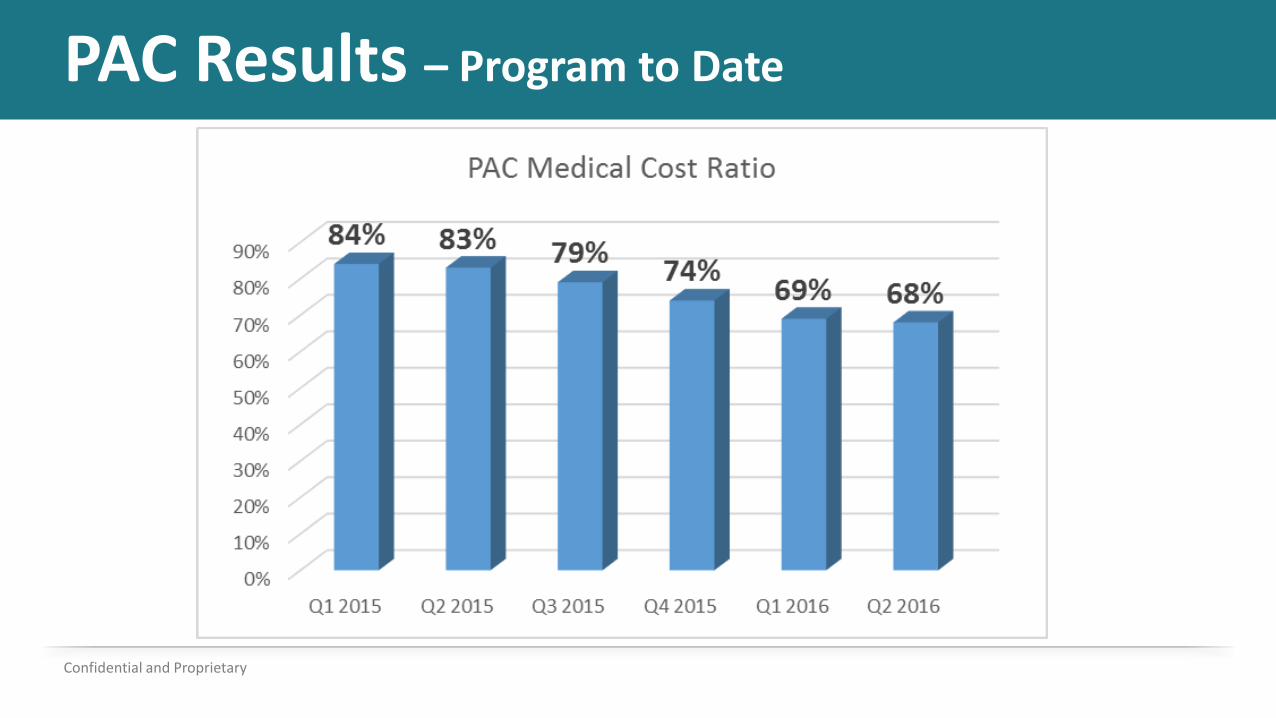
PAC Results – Program to Date
Confidential and Proprietary
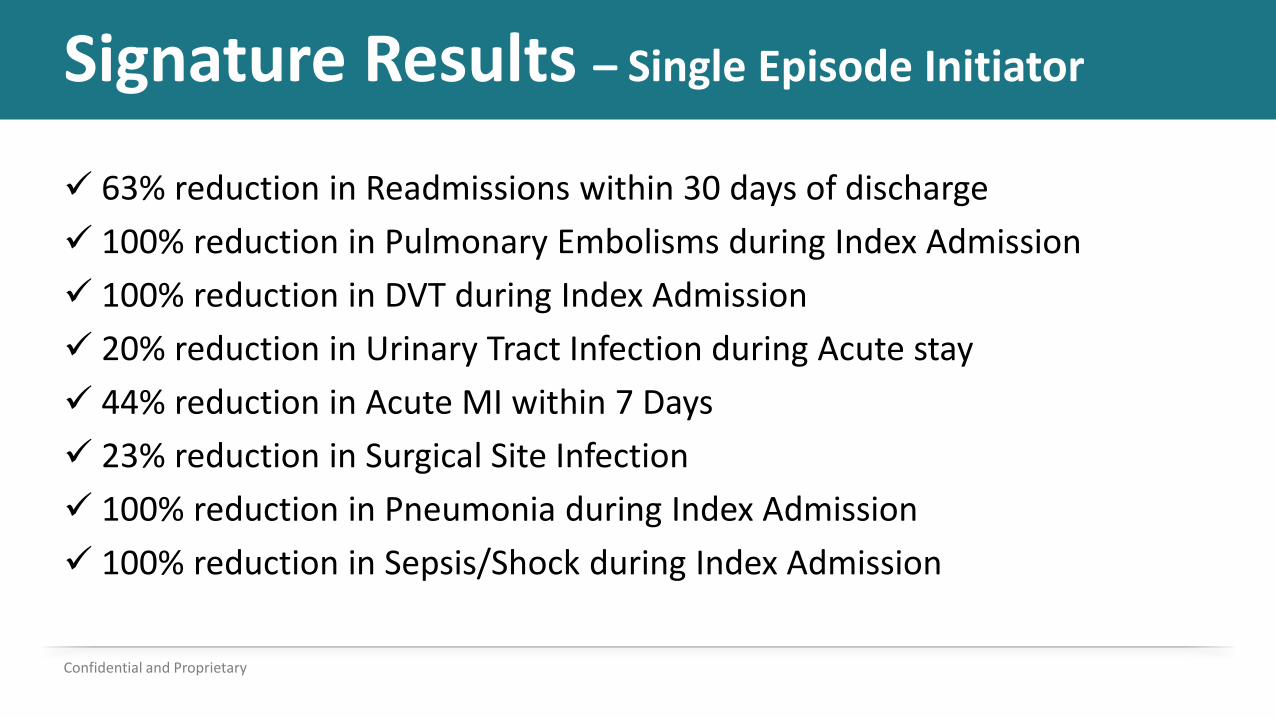
Signature Results – Single Episode Initiator
Confidential and Proprietary
63% reduction in Readmissions within 30 days of discharge 100% reduction in Pulmonary Embolisms during Index Admission 100% reduction in DVT during Index Admission 20% reduction in Urinary Tract Infection during Acute stay 44% reduction in Acute MI within 7 Days 23% reduction in Surgical Site Infection 100% reduction in Pneumonia during Index Admission 100% reduction in Sepsis/Shock during Index Admission
Myths
1) Volume creates savingsi. Episode annual growth per physician (all episodes) = 1.1%ii. Episode annual growth per physician (lower joints) = 3%
2) Patient population difference3) High benchmarks for success4) Provider size matters
Confidential and Proprietary
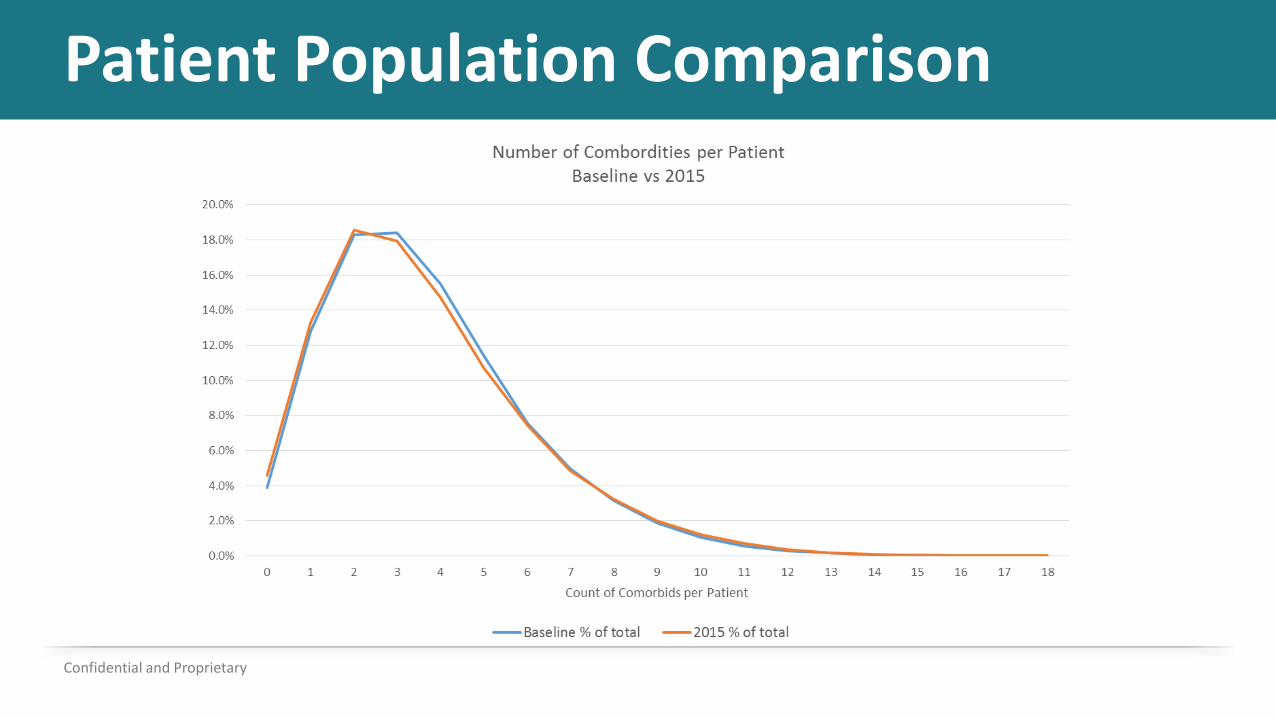
Patient Population Comparison
Confidential and Proprietary
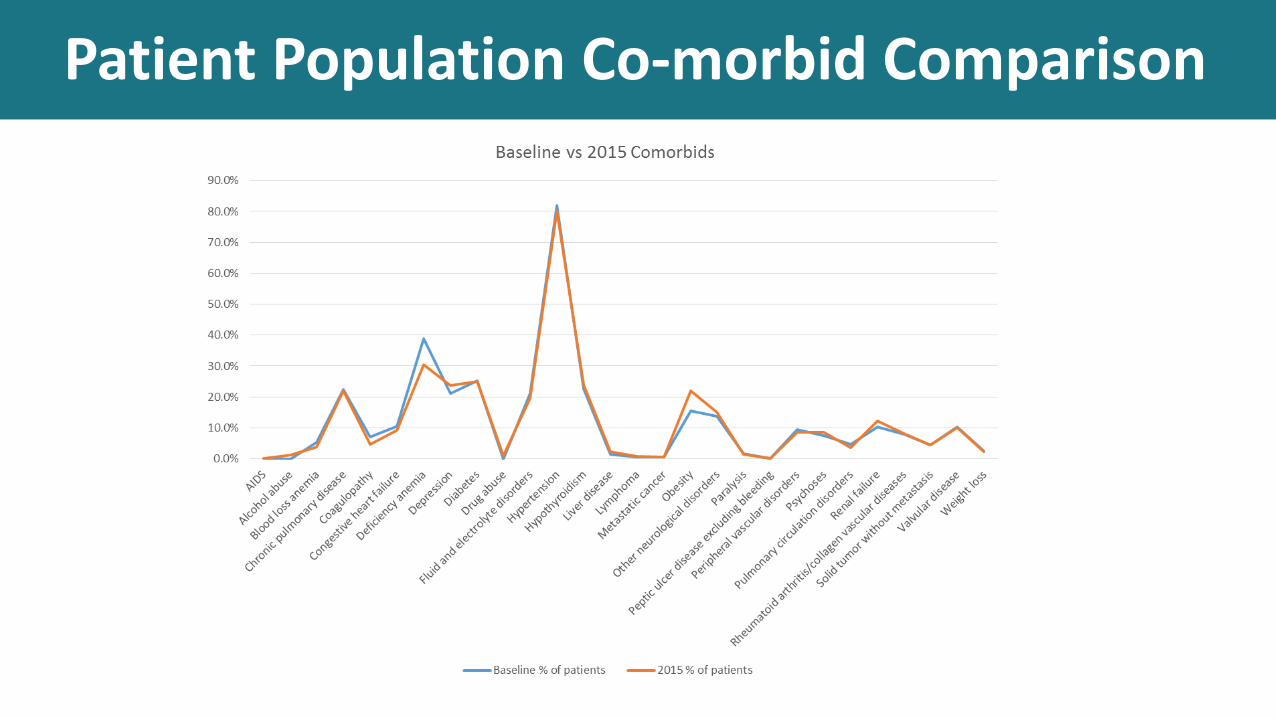
Patient Population Co-morbid Comparison
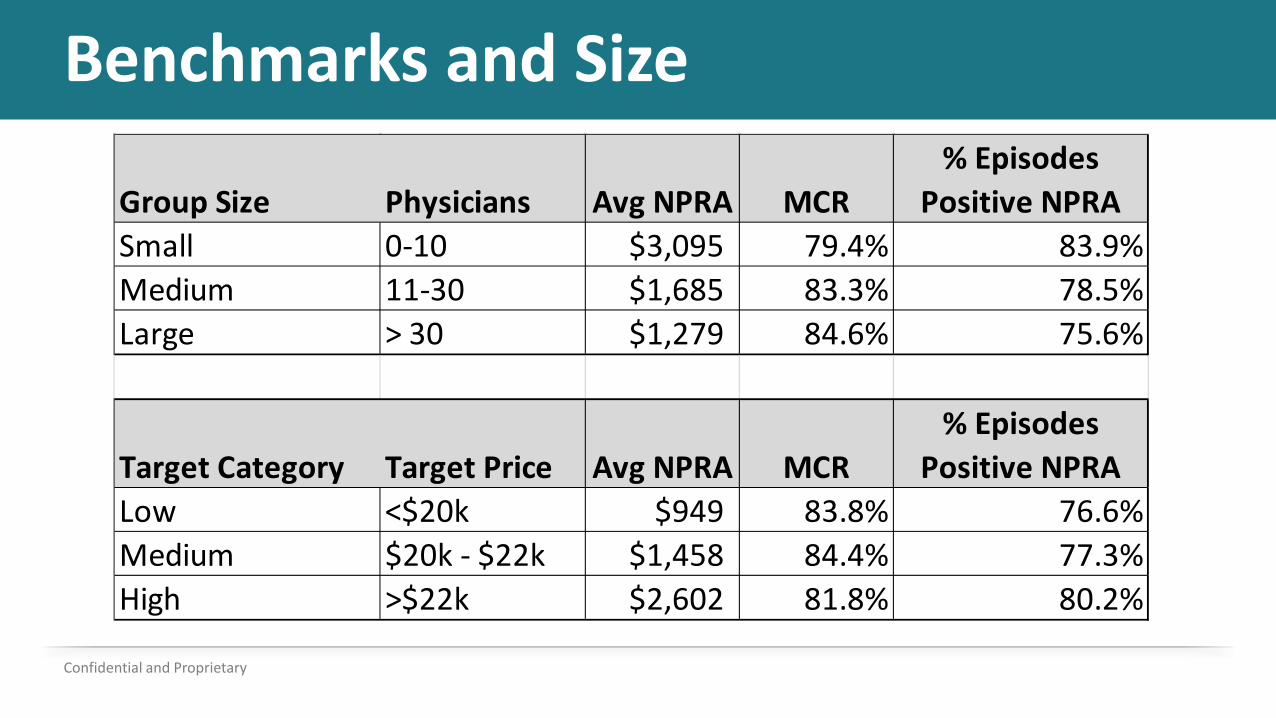
Benchmarks and Size
Confidential and Proprietary
Group Size Physicians Avg NPRA MCR% Episodes
Positive NPRASmall 0-10 $3,095 79.4% 83.9%Medium 11-30 $1,685 83.3% 78.5%Large > 30 $1,279 84.6% 75.6%
Target Category Target Price Avg NPRA MCR% Episodes
Positive NPRALow <$20k $949 83.8% 76.6%Medium $20k - $22k $1,458 84.4% 77.3%High >$22k $2,602 81.8% 80.2%
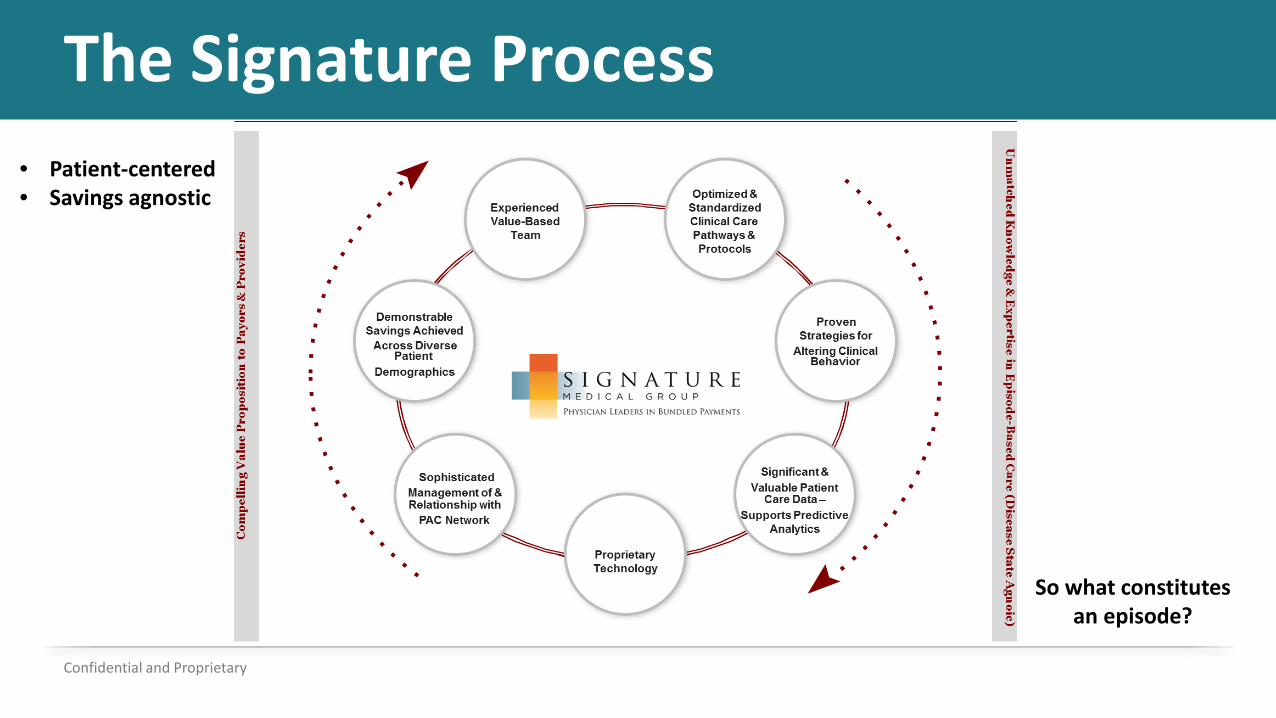
The Signature Process
Confidential and Proprietary
So what constitutes an episode?
• Patient-centered• Savings agnostic
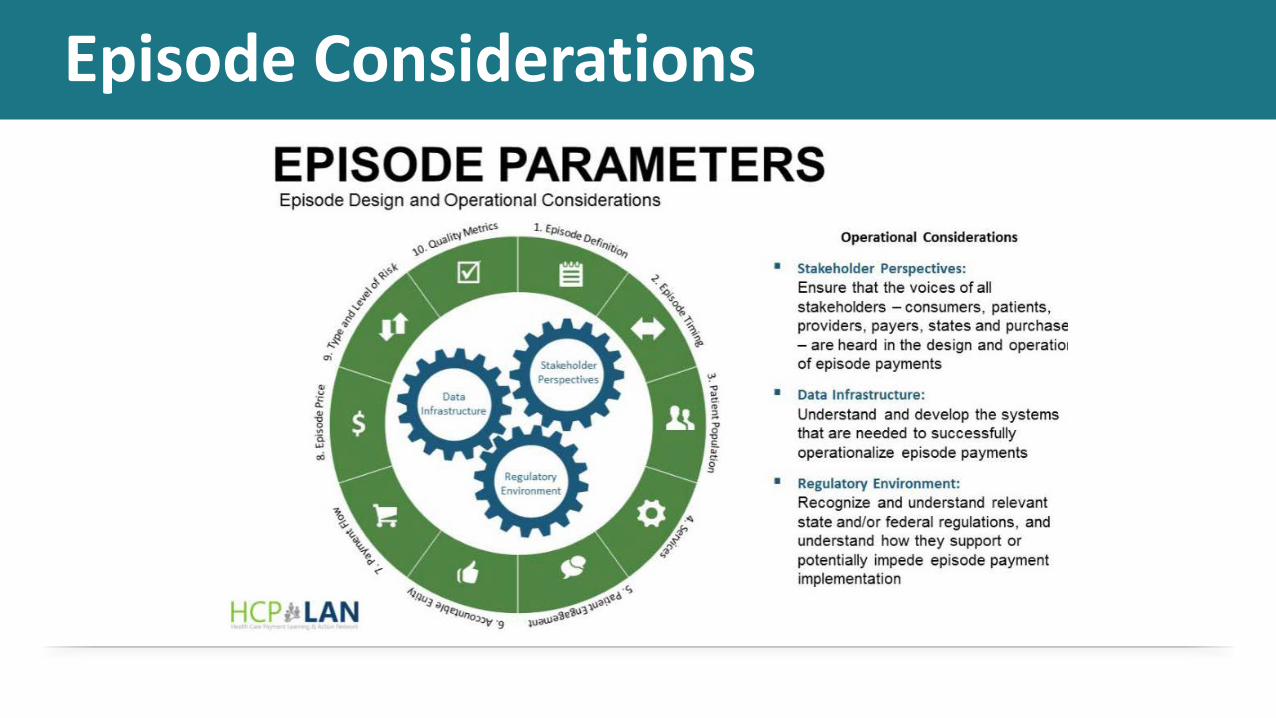
Episode Considerations
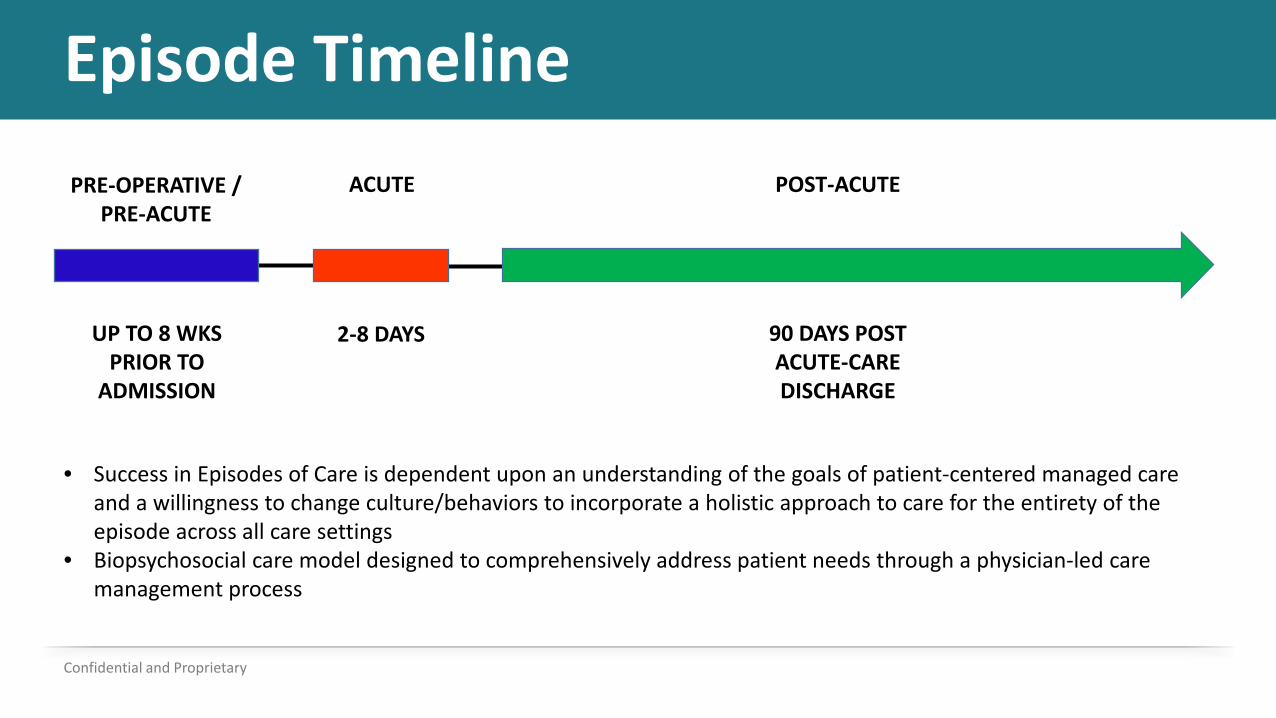
Episode Timeline
Confidential and Proprietary
PRE-OPERATIVE / PRE-ACUTE
ACUTE POST-ACUTE
2-8 DAYS 90 DAYS POST ACUTE-CARE DISCHARGE
UP TO 8 WKS PRIOR TO
ADMISSION
• Success in Episodes of Care is dependent upon an understanding of the goals of patient-centered managed care and a willingness to change culture/behaviors to incorporate a holistic approach to care for the entirety of the episode across all care settings
• Biopsychosocial care model designed to comprehensively address patient needs through a physician-led care management process
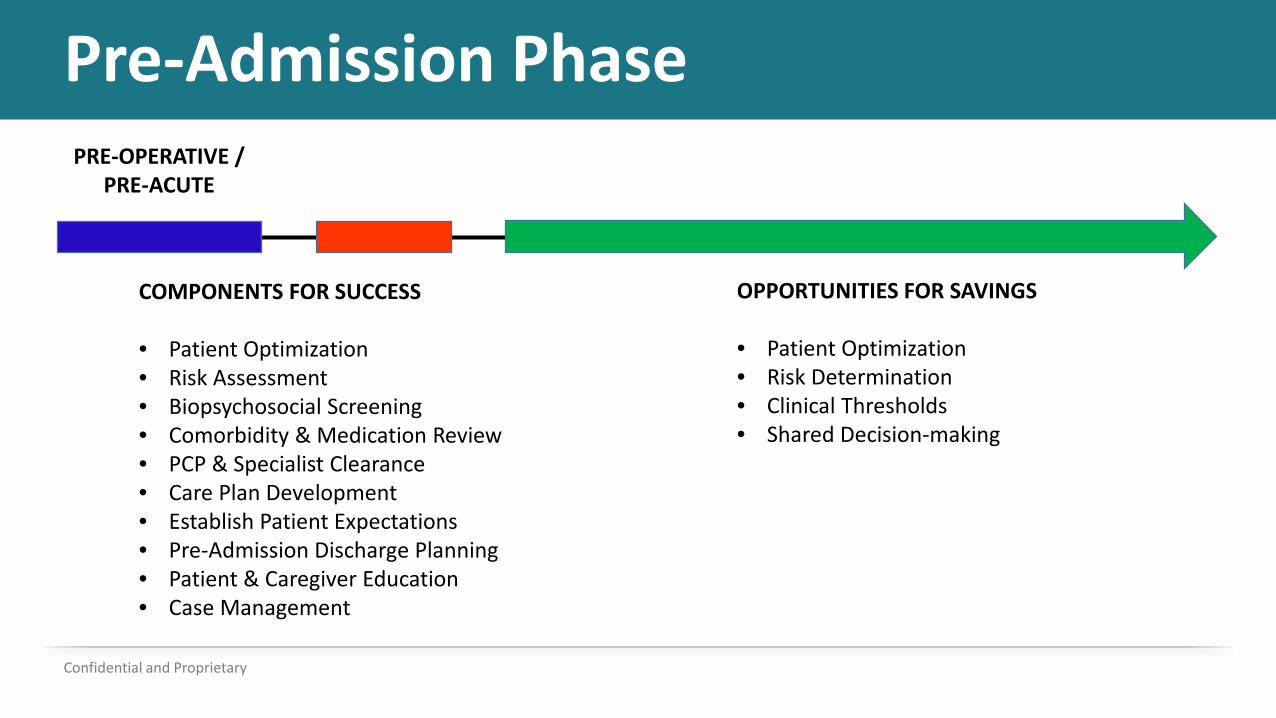
Pre-Admission Phase
Confidential and Proprietary
COMPONENTS FOR SUCCESS
• Patient Optimization• Risk Assessment• Biopsychosocial Screening• Comorbidity & Medication Review• PCP & Specialist Clearance• Care Plan Development• Establish Patient Expectations• Pre-Admission Discharge Planning• Patient & Caregiver Education• Case Management
OPPORTUNITIES FOR SAVINGS
• Patient Optimization• Risk Determination• Clinical Thresholds• Shared Decision-making
PRE-OPERATIVE / PRE-ACUTE
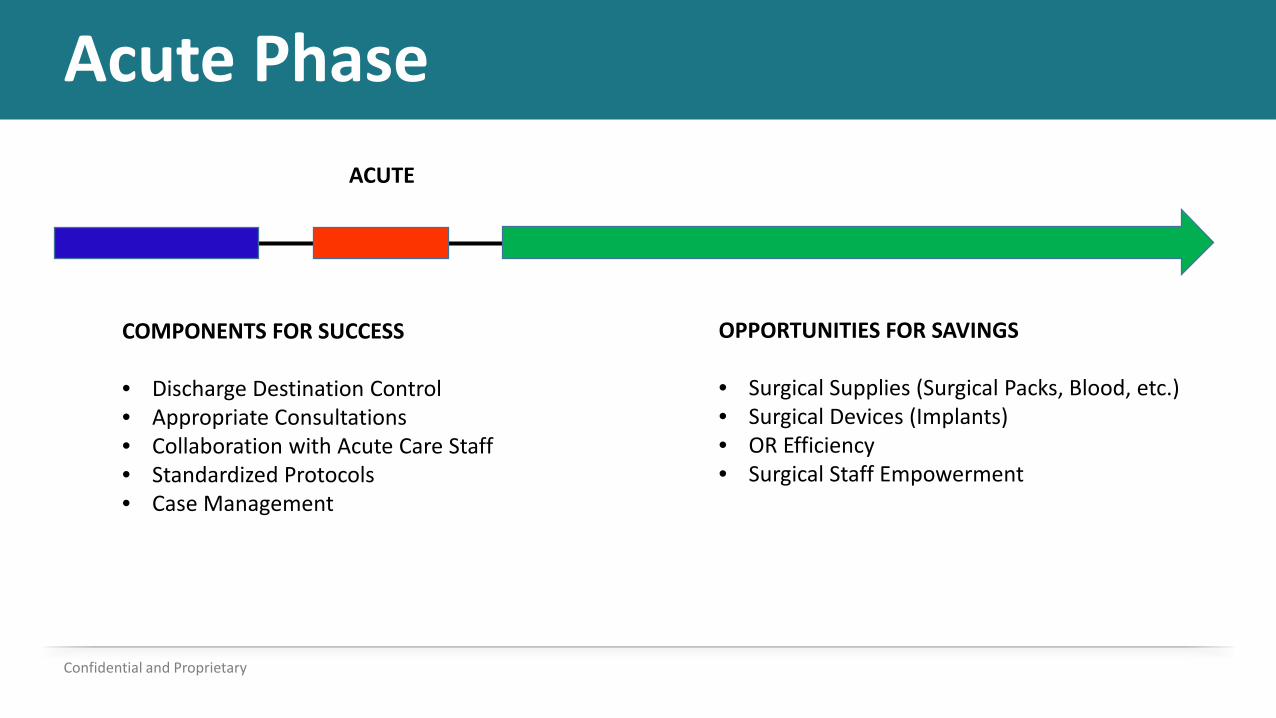
Acute Phase
Confidential and Proprietary
COMPONENTS FOR SUCCESS
• Discharge Destination Control• Appropriate Consultations• Collaboration with Acute Care Staff• Standardized Protocols• Case Management
OPPORTUNITIES FOR SAVINGS
• Surgical Supplies (Surgical Packs, Blood, etc.)• Surgical Devices (Implants)• OR Efficiency• Surgical Staff Empowerment
ACUTE
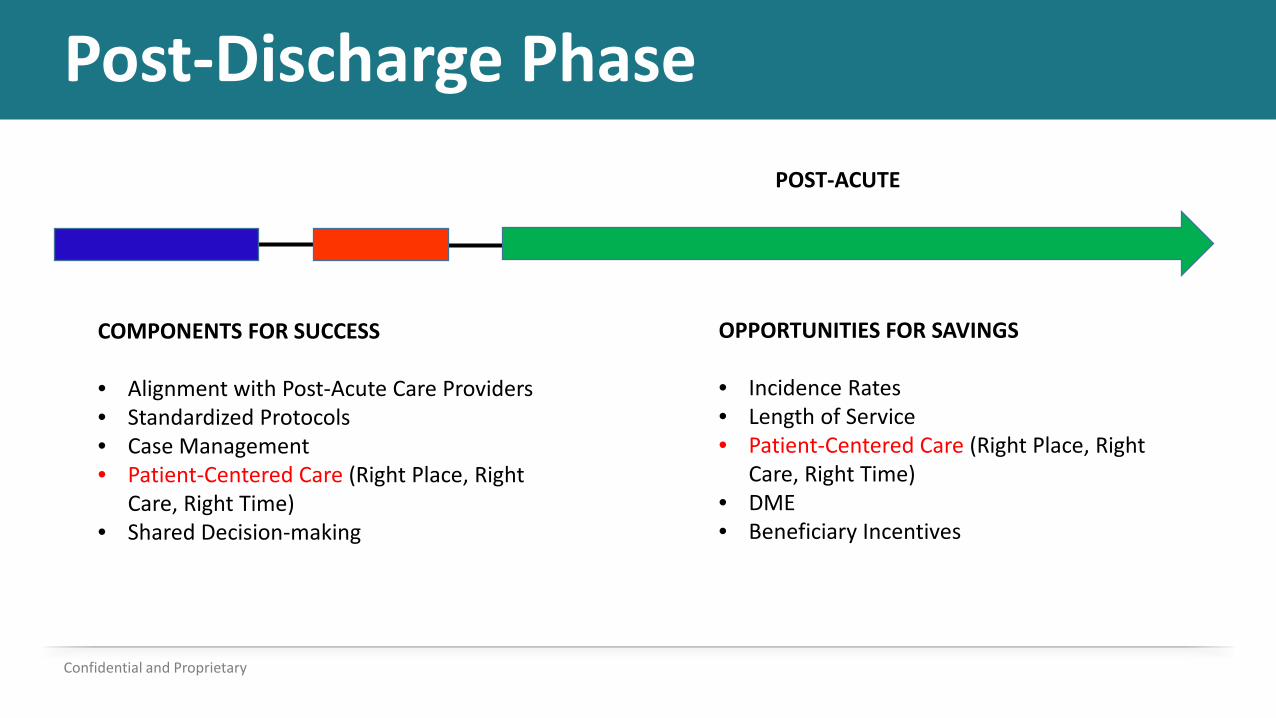
Post-Discharge Phase
Confidential and Proprietary
POST-ACUTE
COMPONENTS FOR SUCCESS
• Alignment with Post-Acute Care Providers• Standardized Protocols• Case Management• Patient-Centered Care (Right Place, Right
Care, Right Time)• Shared Decision-making
OPPORTUNITIES FOR SAVINGS
• Incidence Rates• Length of Service• Patient-Centered Care (Right Place, Right
Care, Right Time)• DME• Beneficiary Incentives
What is Patient-Centered Care?
Does this accurately depict patient-centered care?
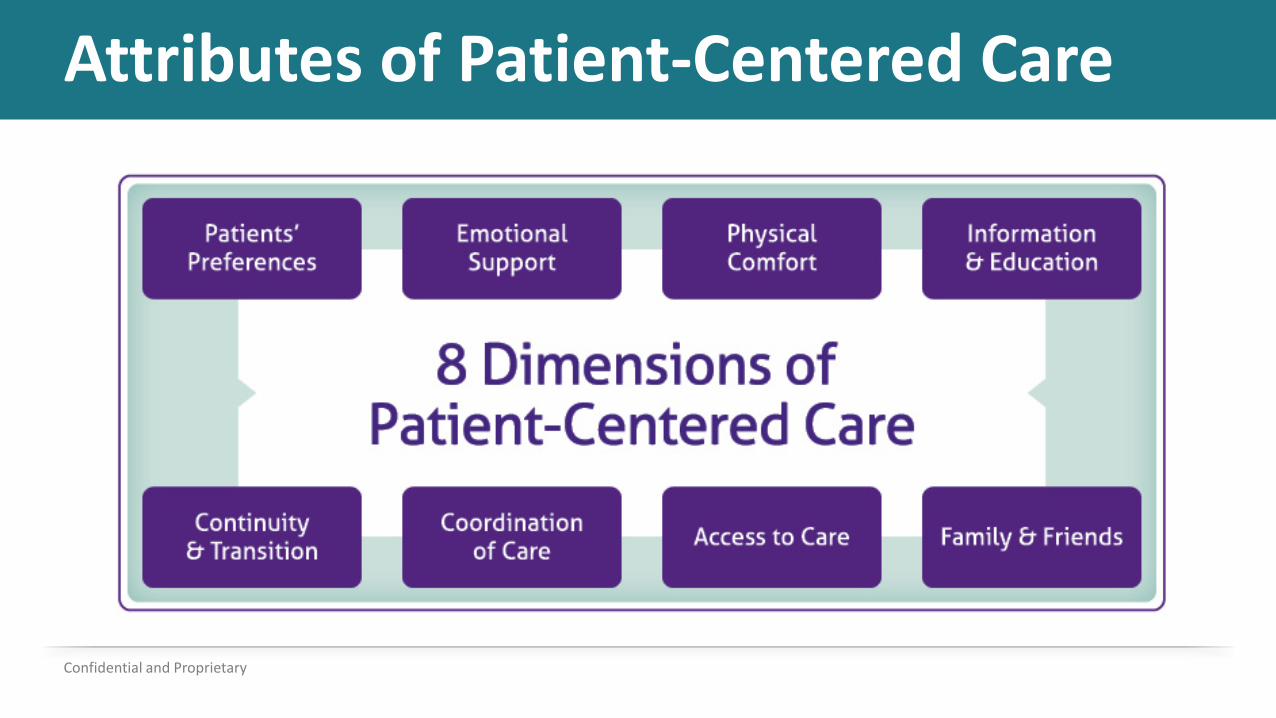
Attributes of Patient-Centered Care
Confidential and Proprietary
Bundled Payment Considerations•What infrastructure is needed to support a bundled payment model?
• Who determines program priorities?• What data is needed to build and manage a bundle?• What are the data sources??• What data analysis is needed?• What are your care redesign goals and methods?
Consider implications for all bundle types (Medicare, MA, Commercial, Medicaid, Self-insured employers)
BP Considerations – cont.
•How will you determine quality metrics and evaluate outcomes?
• How will you establish a benchmark and determine a target?• Where are opportunities to control cost?
• Acute• Post-acute
• What is your risk tolerance?• How will you assess or track performance quality?
Consider implications for all bundle types (Medicare, MA, Commercial, Medicaid, Self-insured employers)
BP Considerations – cont.
• How will you implement a care model design process to track patient progression, care management, financial influence/status, and care team effectiveness?
• How do you track provider performance?• How do you track care navigation performance?• What do you do when providers are not meeting quality
performance targets or fail to be engaged?• What are common pain points in BP programs?
• What strategies can overcome these pain points?
Consider implications for all bundle types (Medicare, MA, Commercial, Medicaid, Self-insured employers)
Path to Success
Confidential and Proprietary
• Motivation• Innovation• Teamwork• Collaborative Networks• Standardization• Training• Patient-Centered Care Redesign• Wellness• Patient Satisfaction

Care Management Team
Confidential and Proprietary
• Patient/Family/Caregiver• Primary Physician• Physician Specialist (PCP, Cardiologist, Hospitalist)• Nurse Practitioner-Physician Assistants• Project Lead• Case Manager/Care Coordinator • Social Worker

Partnerships
Confidential and Proprietary
• Physician alignment• Post-acute preferred providers• Consultants
• Data analytics• Care navigation solutions• Strategic consultants
• Care redesign methodologies and implementation• Gainshare and risk share arrangements• PAC development/management
• ED physicians and staff
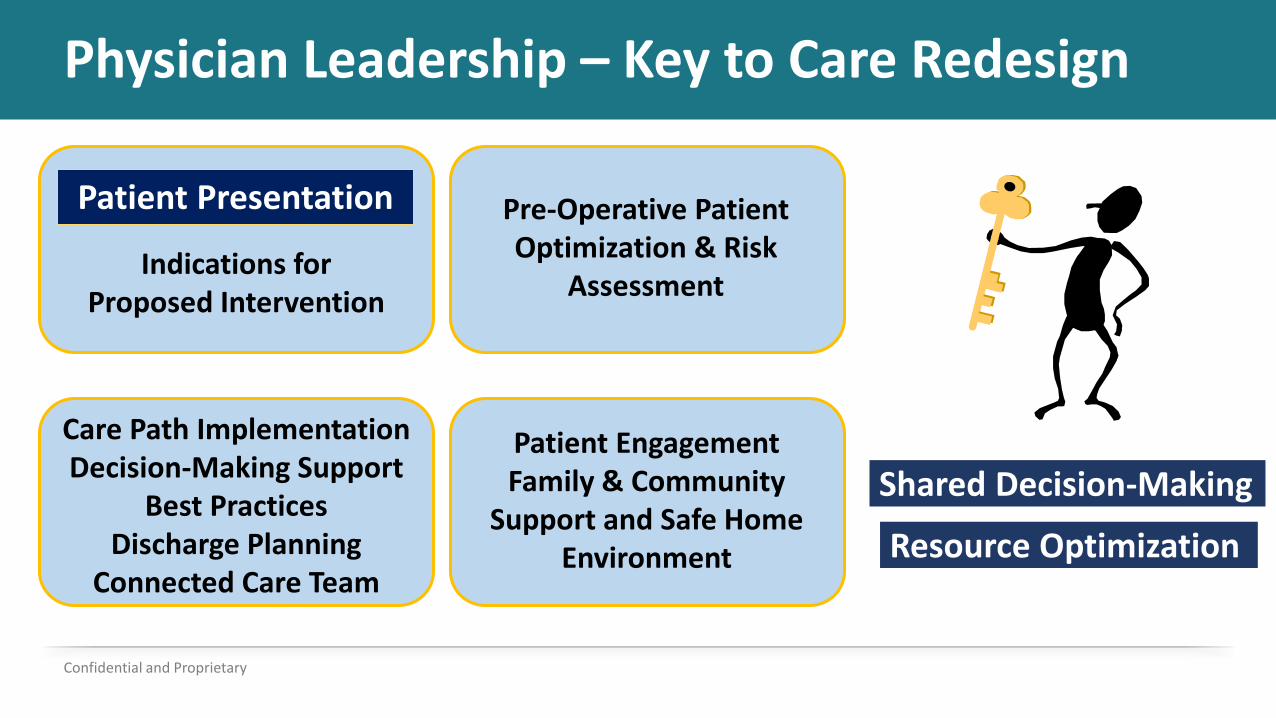
Physician Leadership – Key to Care Redesign
Confidential and Proprietary
Indications for Proposed Intervention
Patient Presentation Pre-Operative Patient Optimization & Risk
Assessment
Patient EngagementFamily & Community
Support and Safe Home Environment
Care Path ImplementationDecision-Making Support
Best PracticesDischarge Planning
Connected Care Team
Shared Decision-Making
Resource Optimization
Physician Engagement and Alignment
• Supportive or Neutral• Champion or Leader• Medical Director and Peer
Network• Physician Scorecards• Linking financial incentive to
quality outcome
Physician Engagement
Confidential and Proprietary
Phase One
Physician Engagement and Alignment
• Education and “buy in” from staff
• Quality committee• Case studies• Build trust with support team• Maximizing service
opportunities
Physician Engagement
Confidential and Proprietary
Phase Two
Physician Communication Strategy• Meet them where there are at• Tailor approach to physician, group and/or organization• Positive messages and reinforcing success and strengths• Problems and weak areas are “opportunities”• Consistent message supported by data and best practices• Leverage benchmarking to create competition• Apply multi-angled approach by standardizing message from convener,
administration, case manager, support staff and other physicians/providers
Confidential and Proprietary
Care Redesign Philosophy• Pre-operative/pre-admission• Acute period• Post-discharge• Outpatient Care
• Patient-centered• Evidence-based (best practices)• Biopsychosocial care model• Physician-led care team
Confidential and Proprietary
Care Redesign• Team approach• Initiating provider engagement
• Quality• Incentives (2-sided)
• Care pathways / Care plans• Collaboration• Pre-admission risk assessments / calculators
Confidential and Proprietary
Care Management Attributes• Care redesign• Risk stratification tool with defined transition of care pathways and
predictive outcome measures• Individualized care pathways supported by evidence-based medicine• Care Coordination throughout the continuum of care• Work within the clinically integrated networks • Community resource development • Beneficiary waiver utilization • Management of chronic and comorbid conditions • Ongoing case studies and reviews
Confidential and Proprietary
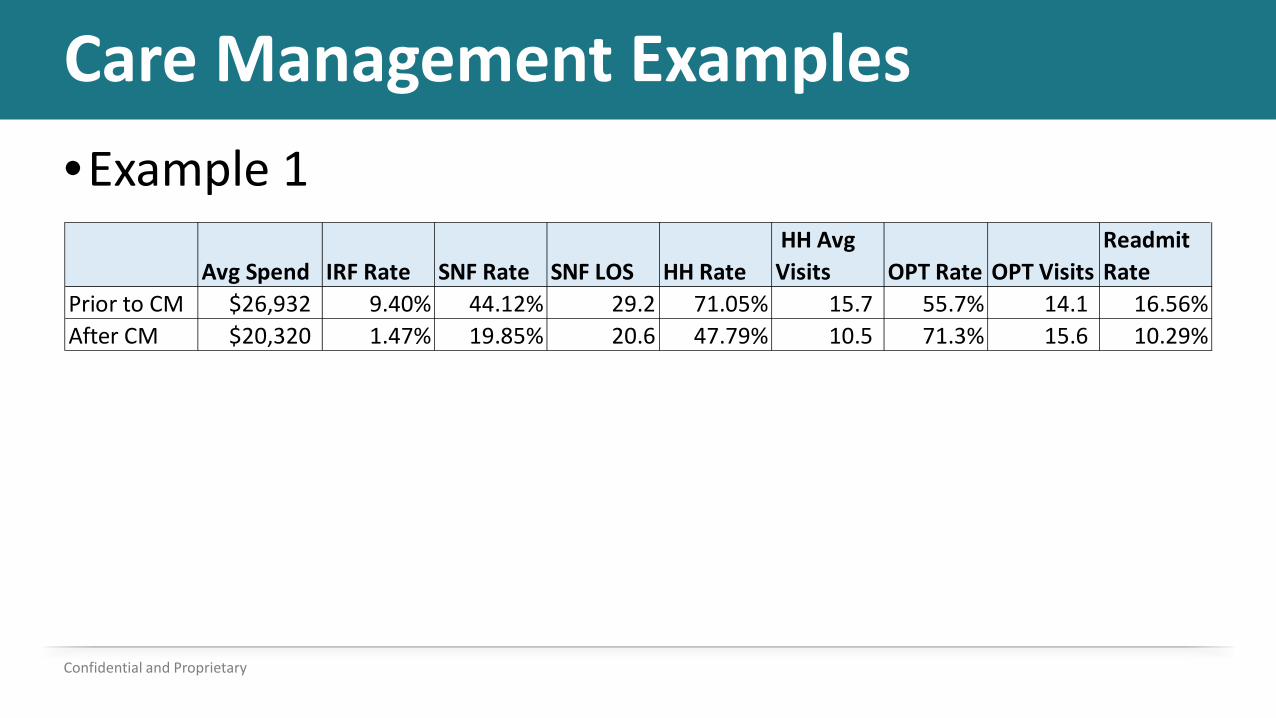
Care Management Examples•Example 1
Confidential and Proprietary
Avg Spend IRF Rate SNF Rate SNF LOS HH Rate HH Avg Visits OPT Rate OPT Visits
Readmit Rate
Prior to CM $26,932 9.40% 44.12% 29.2 71.05% 15.7 55.7% 14.1 16.56%After CM $20,320 1.47% 19.85% 20.6 47.79% 10.5 71.3% 15.6 10.29%
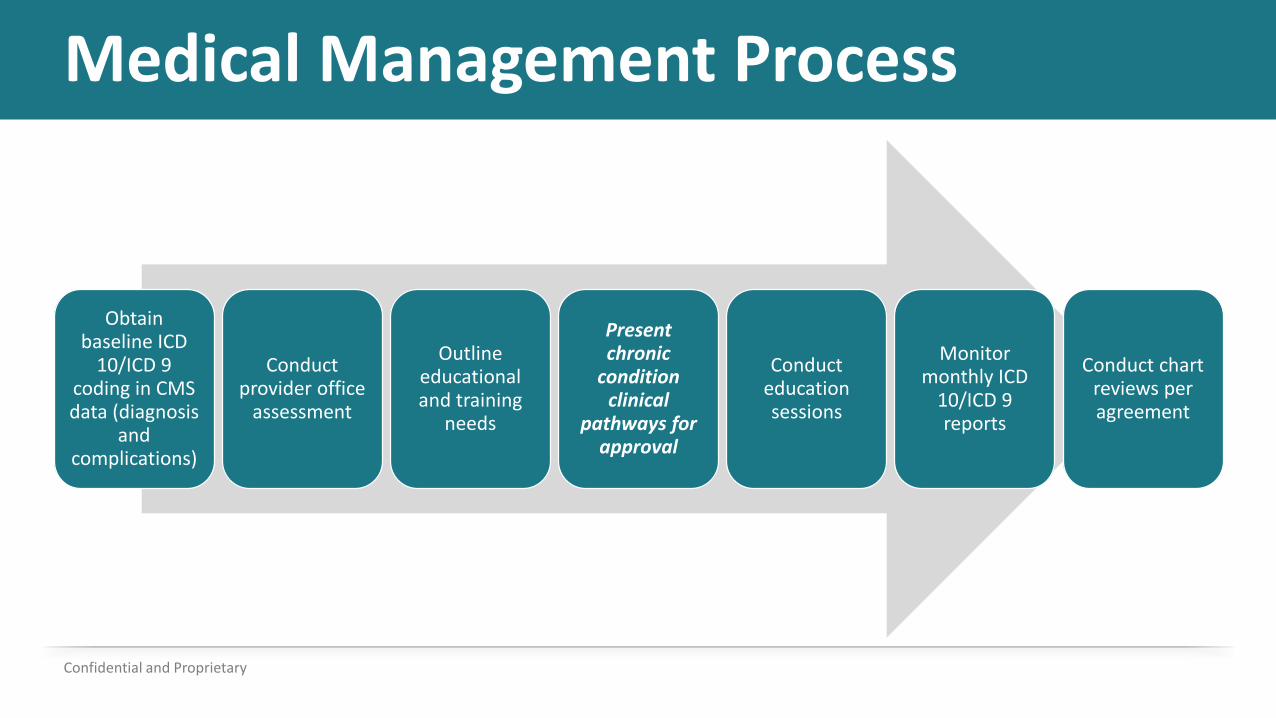
Medical Management Process
Confidential and Proprietary
Obtain baseline ICD
10/ICD 9 coding in CMS data (diagnosis
and complications)
Conduct provider office
assessment
Outline educational and training
needs
Present chronic
condition clinical
pathways for approval
Conduct education sessions
Monitor monthly ICD
10/ICD 9 reports
Conduct chart reviews per agreement
Comprehensive Medical Management• CHF• COPD• Depression• Diabetes• Hypertension• Obesity• Osteoporosis• Prediabetes• History of MI• Vascular disease• MRSA
• Substance abuse• Smoking cessation• Trauma informed care• Motivational interviewing• Social isolation• Other behavioral and mental
health• Social support• Physical environment• Private/public partnerships
Confidential and Proprietary
Medical Management Example
• GI Hemorrhage• 40% of Ortho group’s readmissions identified as avoidable• Protocol change• Virtual elimination of avoidable readmissions to less than 5%
Confidential and Proprietary
Network Development• Post-acute care network
• Preferred and non-preferred network• Protocols/pathways for IRF, SNF, HHA and OPT• Reports and scorecards• Ongoing management and engagement
• Community resources• Beneficiary incentive waivers• Current network and resources (internal and external)• Geographic needs
Confidential and Proprietary
Network Development Strategy• Identify preferred provider network based on past performance
and quality ratings• Facilitate onsite meetings and education with episode initiators
and PAC providers• Establish consensus care protocols and reporting metrics based on
our standardized pathways• Identify opportunities for specialized program development• Develop collaborative relationships• PAC protocols reviewed and updated quarterly• PACs reviewed continuously and held accountable for protocol
adherence
Confidential and Proprietary
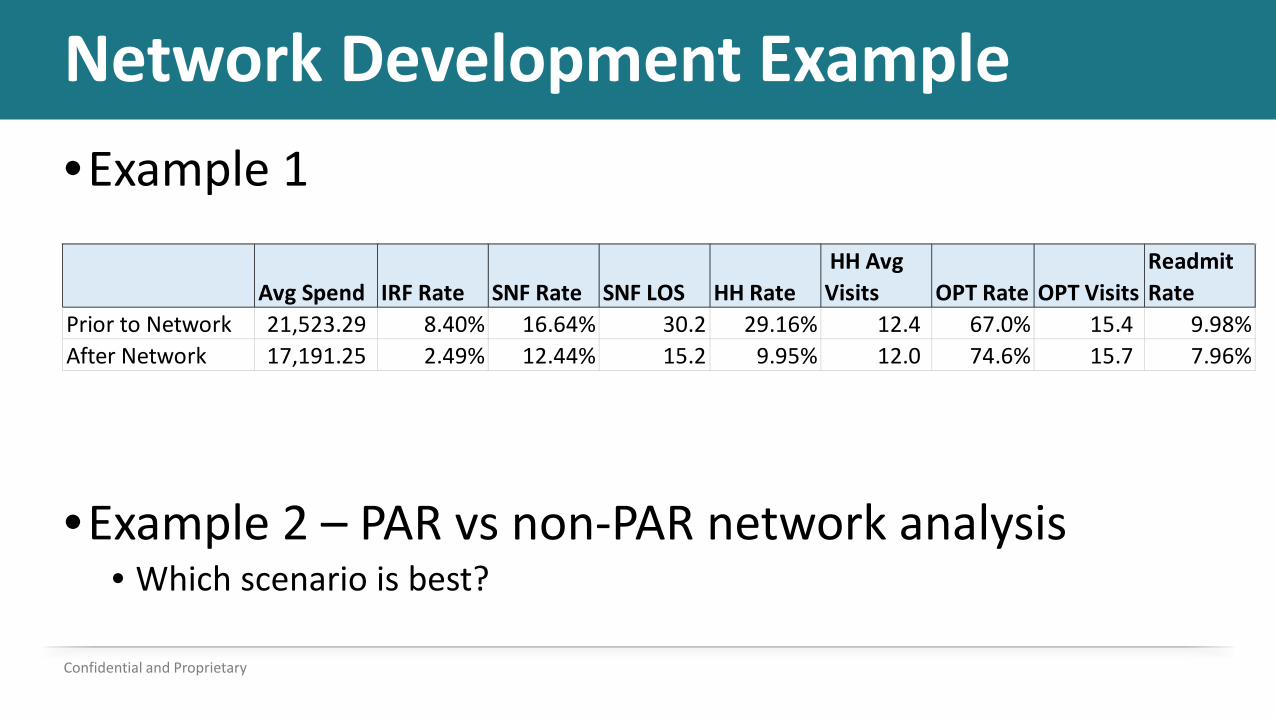
Network Development Example•Example 1
•Example 2 – PAR vs non-PAR network analysis• Which scenario is best?
Confidential and Proprietary
Avg Spend IRF Rate SNF Rate SNF LOS HH Rate HH Avg Visits OPT Rate OPT Visits
Readmit Rate
Prior to Network 21,523.29 8.40% 16.64% 30.2 29.16% 12.4 67.0% 15.4 9.98%After Network 17,191.25 2.49% 12.44% 15.2 9.95% 12.0 74.6% 15.7 7.96%