Alternative Nutrition Darwin Deen, Jr. MD, MS. What is Alternative Nutrition?
Upload
henry-mosleyCategory
view
212download
0
Initial Treatment of Hypertension
Darwin Deen, MD, MS
Family Medicine Clerkship

Objectives
• Review the JNC VII diagnostic criteria for hypertension
• Consider the impact of lifestyle changes on blood pressure
• Review the available pharmacologic agents available for the initial treatment
• Review reasons for selecting specific agents

Fast Facts about HT
• Hypertensive population: 42 x 106
• Controlled hypeertensives: 27%• Those unaware of Dx: 13 x 106
• Aware but untreated: 7 x 106
• Of those treated: 58% uncontrolled• 73% of HT have BP 140-160/<90

Initial Drug Therapy
BP Classification
SBP* (mm Hg)
DBP* (mm Hg)
Lifestyle Modificatio
n
Without Compelling Indications
With Compelling Indications
Normal <120 and <80 Encourage
No antihypertensive drug indicated.
Drug(s) for compelling indications.
Prehypertension
120–139or 80–
89Yes
Stage 1 hypertension
140–159or 90–
99Yes
Thiazide-type diuretic for most. May consider ACEI, ARB, BB, CCB, or combination.
Drug(s) for compelling indications.
Other antihypertensive drugs (diuretic, ACEI, ARB, BB, CCB) as needed.
Stage 2 hypertension
160 or 100 Yes
Two-drug combination for most (usuallythiazide-type diuretic
and ACEI or ARB or BB or CCB).
JNC 7: Classification and Management of Blood Pressure for Adults
JNC 7. May 2003. NIH publication 03-5233.

Diagnostic Workup
• Assess risk factors and comorbidities
• Reveal identifiable causes of HT
• Assess presence of target organ damage
• Thorough history and physical
• Labs: UA, glucose, Hct, lipids, K+ Cr, Ca
• Optional: Urinary alb/Cr ratio
• EKG

CVD Risk Factors
• HT
• OB
• HL
• DM
• Cigarette Smoking
• Inactivity
• Microalbuminuria
• Age– >55 in men– >65 in women
• FH of premature CVD

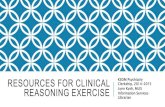
JNC 7: Treatment Algorithm for Hypertension
SBP=systolic blood pressure; DBP=diastolic blood pressure; ACEI=angiotensin- converting enzyme inhibitor; ARB=angiotensin receptor blocker; BB=-blocker; CCB=calcium channel blocker
JNC 7. May 2003. NIH publication 03-5233.
Optimize dosages or add additional drugs until goal blood pressure is achieved.Consider consultation with hypertension specialist.
Not at goal blood pressure
Without compelling indications
Stage 1 hypertension(SBP 140–159 or DBP 90–99 mm Hg)Thiazide-type diuretic for most.May consider ACEI, ARB, BB, CCB, or combination.
Stage 2 hypertension(SBP 160 or DBP 100 mm Hg)Two-drug combination for most (usually thiazide-type diuretic and ACEI or ARB or BB or CCB).
Lifestyle modifications
Not at goal blood pressure (<140/90 mm Hg)(<130/80 mm Hg for those with diabetes or chronic kidney disease)
Initial drug choices
With compelling indications
Drugs for compelling indicationsOther antihypertensive drugs (diuretic, ACEI, ARB, BB, CCB) as needed.
®
© 2003 Thomson Professional Postgraduate Services®
www.lipidhealth.org

Compelling Indications
• Heart Failure
• Post- MI• High CVD risk• DM
• CRF– Cr > 1.5 in men– Cr > 1.3 in women
• S/P CVA
• Thiaz/loop, BB, ACE, ARB, Aldo ant
• BB, ACE, Aldo ant• Thiaz, BB, ACE, CCB
• Thiaz, BB, ACE, ARB, CCB
• ACE, ARB (push to 35% increase in Cr. For Cr 2-3 try loop diuretic.
• Thiaz, ACE

Lifestyle Modifications to Manage HTN
Modification Recommendations Approximate Systolic
Blood Pressure Reduction
Weight Reduction Maintain normal body weight (BMI 18.5-24.9)
5-20 mm Hg for each 10 kg weight loss
Adapt DASH eating plan Consume diets rich in fruits, vegetables, low fat dairy and low saturated fat
8-14 mm Hg
Dietary sodium reduction Reduce sodium to no more than 2.4 g/day sodium or 6 g/day NaCl
2-8 mm Hg
Increase physical activity Engage in regular aerobic activity such as walking (30 min/day on most days)
4-9 mm Hg
Moderate alcohol consumption Limit alcohol to no more than 2 drinks/d for men and 1 drinks/day for women.
2-4 mm Hg
Source: The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure JNCVII. JAMA. 2003;289:2560-2572.

Failures of Patient Education
• 50% of patients discontinue their anti-hypertensive within 1 year of initiating treatment.
• DASH diet for hypertension: – limit sodium– Increase fruits and vegetables (8-10/d)– Increase low fat dairy (3-4/d)
• Focus on diet history for HT patients

Key Diet History Questions for Patients with HTN
• Do you use a salt shaker?
• Do you taste your food before you add salt?
• How often do you eat salty foods, such as chips, pretzels, salted nuts, canned and smoked foods?
• Do you read labels for sodium content?
• How many servings of fruits and vegetables do you eat everyday?
• How often do you eat or drink dairy products? What kind?
• How often do you eat out? What kinds of restaurants?
• Do you like to drink alcohol? How much?
• How often do you exercise, including walking?

TIPS on drugs for HT
• CCB OK for ISH
• For DM: ACE or ARB with or without diuretic then add BB or CCB
• When ACE causes cough, substitute ARB
• Don’t use short acting CCB (increases deaths due to arrhythmias).
• Alpha blockers (e.g. clonidine) only as second line (more side effects).

• Most patients should start with a diuretic as they enhance the effectiveness of other agents.
• Most patients will require more than one agent.
• Add a baby aspirin to improve cardiovascular outcomes.

Special Populations
• Minorities
• Women
• Aged
• Blacks have greater prevalence, severity, and impact and poorer response to monotherapy. ACE induced angioedema is more common
• BCPs elevate BP, Aldomet, BB, and vasodilators OK in pregnancy
• Higher prevalence, ISH more common, more frequent complications from ACE, CCB

Thiazides
• Chlorothiazide (Diuril)
• Chlorthalidone
• Hydrochlorthiazide(Microzide, Hydrodiuril)
• Polythiazide (Renese)
• Indapamide (Lozol)
• Metolazone (Mykrox, Zaroxolyn)

Benefits of Thiazide Diuretics
• Evidence-based support for end points that matter (prevention of CV and all-cause mortality).
• Reduce calcium excretion potential benefit for osteoporosis prevention.

Loop Diuretics
• Bumetanide (Bumex)
• Furosemide (Lasix)
• Torsemide (Demadex)
Potassium-sparing Diuretics
•Amiloride (Midamor)•Triamterene (Dyrenium)

Aldosterone Receptor Blockers
• Eplerone (Inspra)
• Spironolactone (Aldactone)
Combined alpha- and beta- blockers•Carvediol (Coreg)•Labetalol (Normodyne, Trandate)

Beta-blockers
• Atenolol (Tenormin)
• Betaxolol (Kerlone)
• Bisoprolol (Zebeta)
• Metoprolol (Lopressor, Toprol XL)
• Nadolol (Corguard)
• Propranolol (Inderal and XL)
• Timolol (Blocadren)

Beta-blockers with intrinsic sympathomimetic activity
• Acebutolol (Sectral)
• Penbutolol (Levatol)
• Pindolol (generic)

ACE inhibitors
• Benzapril (Lotensin)• Captopril (Capoten)• Enalpril (Vasotec)• Fosinopril (Monopril)• Lisinopril (Prinivil, Zestril)• Moexipril (Univasc)• Perindopril (Aceon)• Quinapril (Accupril)• Ramipril (Altace)• Trandolapril (Mavik)

Angiotensin II antagonists
• Candesartan (Atacand)
• Eprosartan (Tevetan)
• Irbesartan (Avapro)
• Losartan (Cozaar)
• Olmesartan (Benicar)
• Telmisartan (Micardis)
• Valsartan (Diovan)

Calcium channel blockers
• Dihyropyridines– Amlodipine (Norvasc)– Felodipine (Plendil)– Isradipine (Dynacirc
CR)– Nicardipine (Cardene
SR)– Nifedipine (Adalat
CC,
Procardia XL)
– Nisoldipine (Sular)
• non-Dihyropyridines• Diltiazem (Cardizem
CD, Dilacor XR,
Tiazac, Cardizem LA)
• Verapamil (CalanSR,
Isoptin SR)

Alpha1 blockers
• Doxazosin (Cardura)
• Prazosin (Minipress)
• Terazosin(Hytrin)
Direct Vasodilators
Hydralazine (Apresoline)
Minoxidil (Loniten)

Centrally acting drugs
• Clonidine (Catapres)
• Methyldopa (Aldomet)
• Reserpine (generic)
• Guanfacine (generic)

Treatment Algorithm
Lifestyle Modification
Not at goal BP
Initial Drug Choices
W/O Compelling Indications
Stage 1 Stage 2
With Compelling Indications
Drug for Indication
Thiaz, ACE, ARB, BB, CCB 2 Drug Combo Not at Goal BP
Adjust Dose or add additional agents