Initial Set Up Guide Final
22
Dynavision D2™ Visuomotor Training System Initial Set-Up Guide
-
Upload
jennifer-fortuna -
Category
Documents
-
view
30 -
download
0
Transcript of Initial Set Up Guide Final

Dynavision D2™ Visuomotor Training System
Initial Set-Up Guide
2
Table of Contents Introduction ................................................................................................................................... 3 Initial Set-Up .................................................................................................................................. 4 Programmable Options ................................................................................................................ 10 Modes .......................................................................................................................................... 11 Lights ............................................................................................................................................ 15 Report Management .................................................................................................................... 18 Tips for Individualized Treatment ................................................................................................ 20 References ................................................................................................................................... 21

3
Introduction
The Dynavision D2™ has been recognized as the premier visual-motor reaction training system for over 25 years. Originally developed for sports vision training of athletes, the Dynavision D2™ has proven effective for use in visual, cognitive and physical rehabilitation; driver retraining; concussion baseline testing; and concussion management (Anderson et al., 2011; Klavora, Heslegrave, & Young, 2000; Wells et al., 2014; Klavora, & Leung, 1996; Clark et al., 2014). Programmable options standard with Dynavision D2™ software enable the clinician to facilitate individualized treatment and training programs for clients of different ages, abilities, and conditions. Performance data is quantitative and objective ensuring accuracy for initial evaluation and progress monitoring.
Clinical Applications Programmable options standard with D2™ software enable facilitate individualized treatment programs for clients of different ages, abilities, and conditions. The D2™ is currently utilized by a variety of medical professions:
Physical Therapy
Occupational Therapy
Speech Therapy
Physiotherapy
Optometry
Neurology Environmental Modifications
Adapt for the patient’s strengths/needs
Consider environmental modifications
Remove visual/auditory distractions
Dim lights to increase contrast
Trial “add-on’s” Evidence of Effectiveness Evidence-based practice (EBP) informs decision making by incorporating research evidence, clinical reasoning, and the client’s best interests through all stages of service delivery. Numerous peer-reviewed research articles have been published supporting efficacy of the Dynavision D2™ in rehabilitation, sports vision training, driver retraining, and concussion management. Visit www.dynavisioninternational.com to access these articles free of charge.

4
Initial Set-Up
Log In
Step 1: Click the Dynavision Software icon on the desktop.
Step 2: Type the word Admin in the box labeled System Password. Click OK.
5
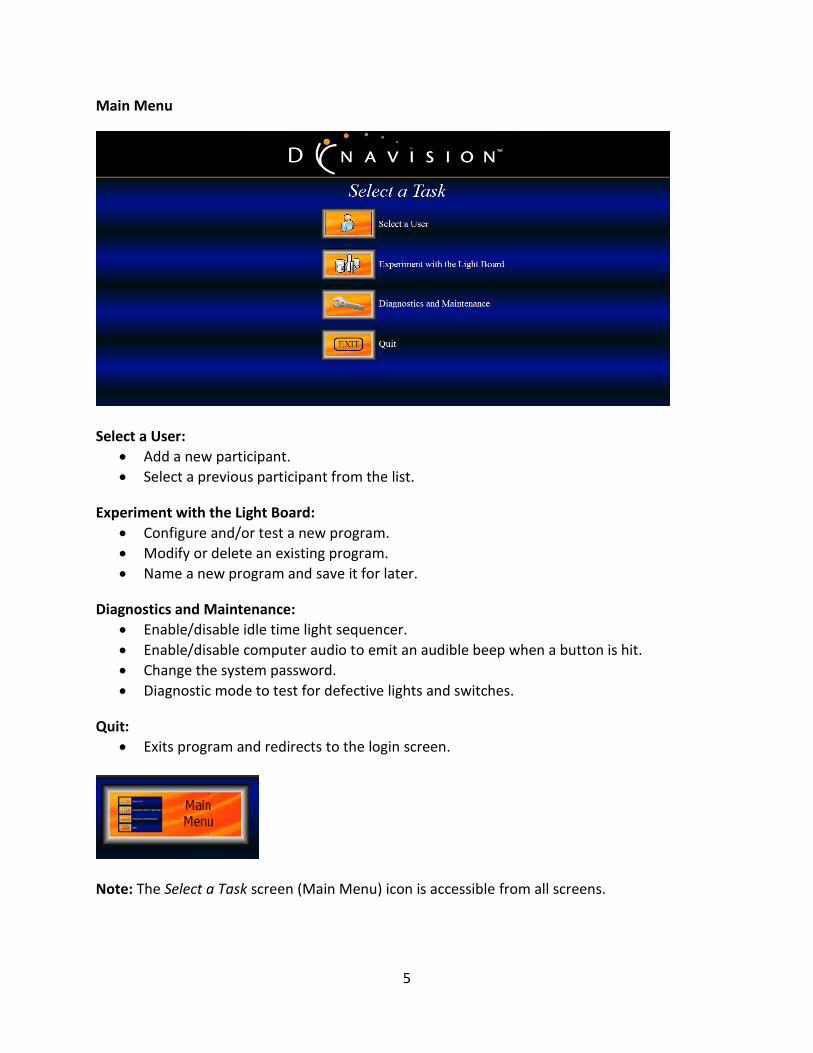
Main Menu
Select a User:
Add a new participant.
Select a previous participant from the list.
Experiment with the Light Board:
Configure and/or test a new program.
Modify or delete an existing program.
Name a new program and save it for later.
Diagnostics and Maintenance:
Enable/disable idle time light sequencer.
Enable/disable computer audio to emit an audible beep when a button is hit.
Change the system password.
Diagnostic mode to test for defective lights and switches.
Quit:
Exits program and redirects to the login screen.
Note: The Select a Task screen (Main Menu) icon is accessible from all screens.

6
Add a User
Step 1: Click Select a User.
Step 2: Click Add User.

7
Add a User Cont’d
Step 3: Enter new user information (name, age, diagnosis, etc.). Click Save.
Step 4: Click Use Light Board. Note: Assigning participants an ID number and private password ensures HIPAA compliance.

8
Select a Program
Step 1: Select a program from the list.
Step 2: Click Run Program.
Note: The T-Scope will count down from 5 to 0 to start the run.

9
Add a Program
Step 1: Click Select a User from the main menu. Step 2: Select a client from the list. Step 3: Click Use Light Board.
Step 4: Click Add Program.
Note: Six standard programs are indicated with *

10
Programmable Options
Adjustable light board with 64 LED buttons
Five concentric rings
Four quadrants
Modes (A,B,C, Reaction Time Test)
Green Lights (percentage/area)
Tachistoscope (T-Scope)
Run time
Light speed
Note: Customize new programs by activating or deactivating programmable options. Programmable options will vary according to the Mode selected.
Adjustable Light Board
Raise or lower the height of D2™ with the push of a button. A rocker switch is located on the lower left corner of the light board. Height may be adjusted between 5 ½ feet and 8 feet tall.

11
Modes Proactive (Mode A):
Reactive (Mode B):
Mode C: Scan (Mode C):
Note: Gradually moving the client closer to the light board will increase visual demands. Reaction Time Test (Mode D):
Note: Mode D will establish the client’s visual motor baseline and monitor progress over time.
A single red light will illuminate. The client must press and hold the red light with one hand. A second red light will appear at a random location. The client must release the first light to deactivate the second light as quickly as possible. A total of six tests are used; three for the right hand and three for the left hand.
The client is positioned 6 feet from the D2™. A light will move along the outer edge of the light board and the client must visually track it. The light will change direction every 15 seconds. This cycle continues until the run is over.
A light will illuminate and the client must strike it to deactivate it. When one light is deactivated, another will appear at a random location. This cycle continues until the run is over.
A light will illuminate for a preset length of time and the client must strike it to deactivate it before time is up and it moves to a random location. This cycle continues until the run is over.

12
Run Time
1. Click Change to edit Run Time.
2. Click on desired length of time for the run. Tachistoscope (T-Scope)
1. Click Change to edit T-Scope options.

13
Basic T-Scope Options
1. Use the Flash menu to select the number of digits. 2. Select the amount of time (0.10-1.00 seconds) digits are displayed. 3. Click Advanced to choose additional options. Advanced T-Scope Options:
What Kind? Select the type of content shown on the T-Scope.
Select from Numbers, Letters, Words, Scrolling Text, Math, or Icons.
Select between 1-10 characters in length.
Select the length of Numbers, Letters or Words.
Select the speed and source of Scrolling Text.

14
Advanced T-Scope Options Cont’d From Where? Select the source of content shown on the T-Scope.
Select from All Numbers or custom lists saved in the T-Scope Library
Select the source of Scrolling Text, Math, and Icons.
Time between Flashes: Select the length of time between content flashing on the T-Scope.
Select Exactly or At Least
Select between 1 Second and 8 Seconds
In What Order? Select the order in which content is presented on the T-Scope.
Select from Random or Sequential
Flash For: Select the length of time digits are flashed on the T-Scope.
Select between 0.10 Seconds and 1.0 Seconds
Text Size: Select the size of characters that will appear on the T-Scope.
Select from Large, Medium, or Small
Specify Sequence: Specify the order in which content will appear on the T-Scope.
Add, delete, or rearrange the sequence of characters.
Edit Library: Edit custom content saved in the T-Scope Library.
Organized by type: Numbers, Letters, Words, Scrolling Text, Math, or Icons.

15
Lights Light Speed
1. Click Change to edit the speed of lights.
Select between 0.25 Seconds and 5.0 Seconds.
Increase or decrease speed by 0.01 second increments.
Light speed is programmable for Reactive (Mode B) and Scan (Mode C).
Green Lights: Select the percentage of green lights to flash on the light board.
Select a percentage between None and 100%, or 8 Fixed lights.
Green light percentage is programmable for Reactive (Mode B) and Scan (Mode C).

16
Green Light Area: Select the area where green lights will flash on the light board.
Select Partial or Full
Green area is programmable for Reactive (Mode B) and Scan (Mode C). Quadrants: Select the quadrants where lights will flash on the light board.
Activate or deactivate the Upper Left, Upper Right, Lower Left, or Lower Right quadrants.
Quadrants are programmable for Proactive (Mode A and Reactive (Mode B).
17
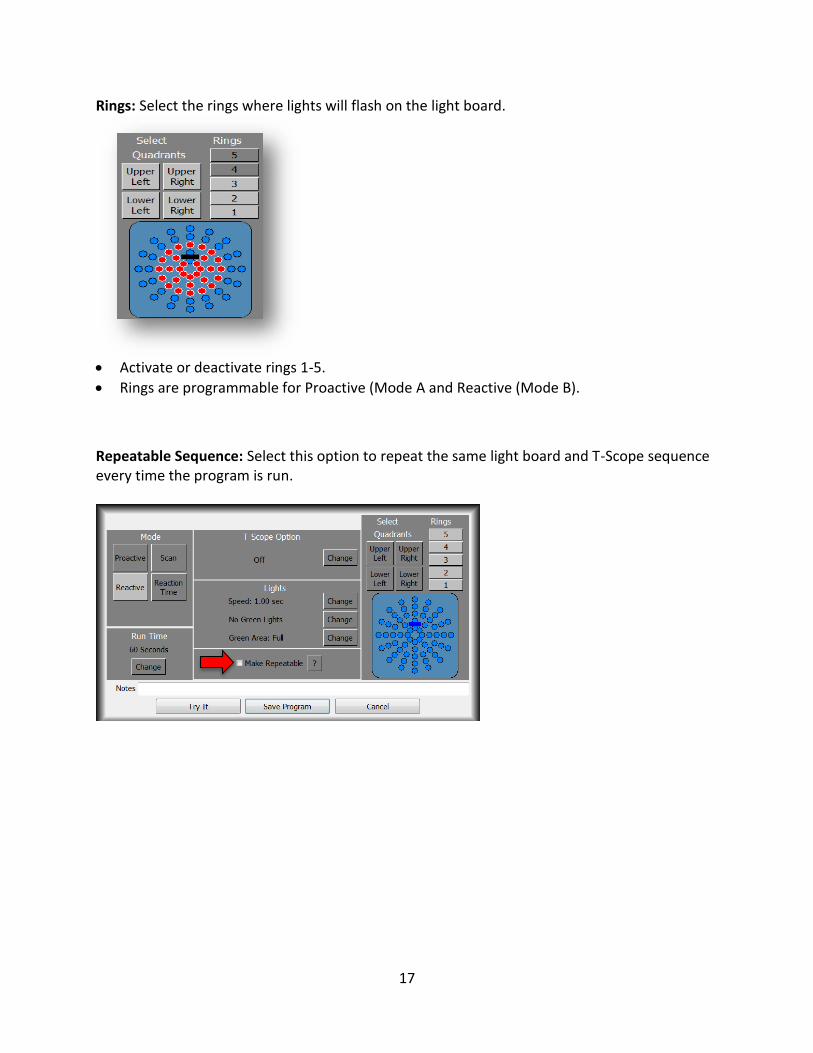
Rings: Select the rings where lights will flash on the light board.
Activate or deactivate rings 1-5.
Rings are programmable for Proactive (Mode A and Reactive (Mode B).
Repeatable Sequence: Select this option to repeat the same light board and T-Scope sequence every time the program is run.

18
Report Management
Run Results by Quadrant:
Total score and average reaction time
Divided by quadrant and color
Separates red/green light scores and average reaction times
Run Results by Text Report:
Total Score and average reaction time
Displays fastest/slowest reaction time
Generates statistics on quadrants, rings, hits, and average reaction time
Time/Score Breakdown:
Total score and average reaction time
Provides hits/lights by interval
Displays location of hits on light board
19
Clinical Observations
Left/right symmetry of the upper extremities
Unsteady seated or standing balance
Alternating hands instead of using hand that is closest to the illuminated button
Intention tremors
Pauses before striking or calling/adding numbers
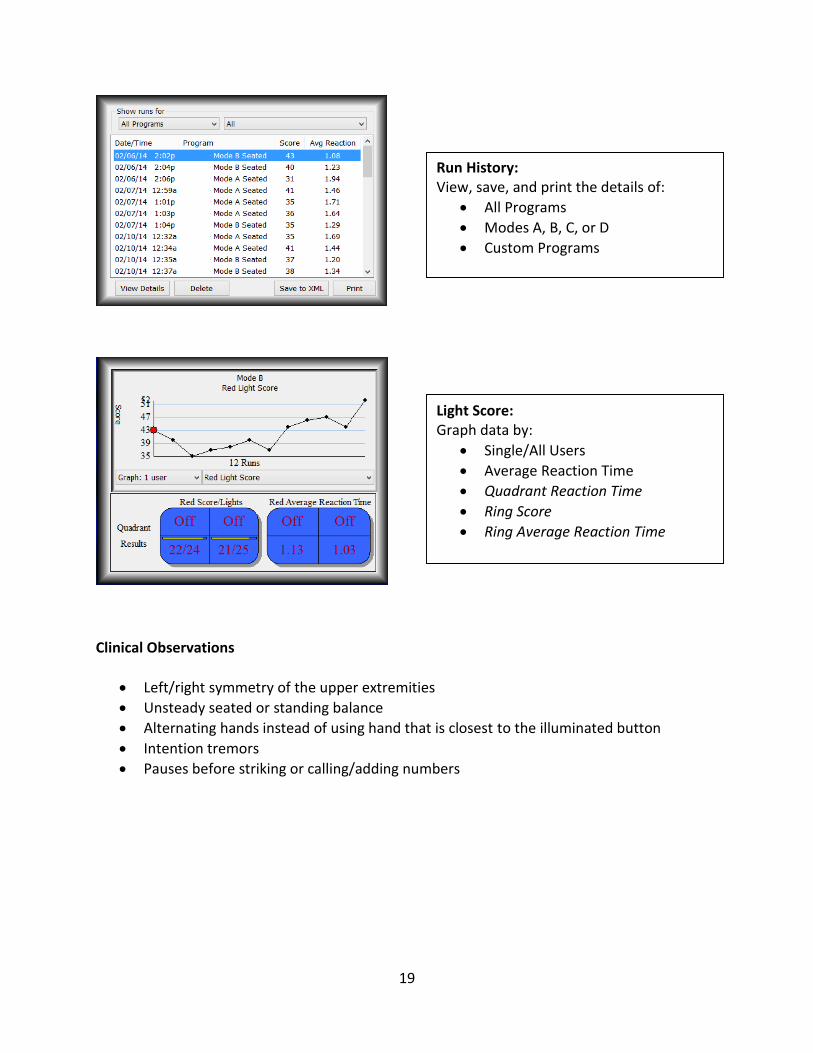
Run History: View, save, and print the details of:
All Programs
Modes A, B, C, or D
Custom Programs
Light Score: Graph data by:
Single/All Users
Average Reaction Time
Quadrant Reaction Time
Ring Score
Ring Average Reaction Time

20
5 Tips for Individualized Treatment 1. Identify Current Level of Function Investigate the client’s current level of function prior to programming the D2™. Some factors to consider include visual and cognitive deficits, posture, activity endurance, standing and/or seated balance, and upper extremity range of motion. Clinical observation, parent/caregiver interviews and teacher questionnaires are excellent sources for information. 2. Provide a “Just Right” Challenge Challenge the client slightly above his or her current level of function. Consider what the client is currently able to do, but also what you are asking the client to do. Begin treatment at the level where the client is experiencing difficulty, and then increase demands as new skills develop. Grade the number of illuminated rings, light speed, color of lights, length of run, and complexity of content flashing on the T-Scope to accomplish this. 3. Improve Access to Programming Improve access to the D2™ by addressing personal and environmental barriers. Personal factors to consider include height, muscle weakness/spasticity, hemiplegia, and attention span. Environmental factors such as fluorescent lighting and excessive visual distractions. For a client with limited upper extremity range of motion, lower the light board and provide a sturdy surface to sit or stand on. For clients who are easily distracted, dim the lights to increase visibility. Oftentimes simple changes such as these greatly improve performance on the D2™. 4. Prompt for Success Use simple and consistent visual and verbal cues reinforce learning. Model what you want the client to do prior to starting the run. Demonstrate different strategies to deactivate lights, including using the palm, fingers, or back of the hand. Matching red and green gloves to red and green lights will ease understanding and make crossing midline easier. Allow clients with motor planning deficits to hold a small object in the hand that is not being tested. Create a visual marker such as an X made with tape to indicate where you want the client to stand. Simple cues yield the best results, especially when working with client’s with cognitive or attention deficits. 5. Individualize Treatment Develop individualized plans for every client. Program separate runs for each position the client participates from. Consider the client who uses both a wheelchair and crutches for mobility. Deactivate the upper two quadrants of the light board when the client participates from a seated position; activate all four quadrants when the client participates from a standing position. When using the T-Scope, select content that matches the client’s current level of cognition. Incorporate therapy goals for seated or standing balance, upper extremity range of motion, and reach when possible.

21
References
Akinwuntan, A.E., Devos, H., Verheyden, G., Baten, G., Kiekens, C., Feys, H., & De Weerdt, W. (2010). Retraining moderately impaired stroke survivors in driving-related visual attention skills. Topics in Stroke Rehabilitation, 17(5), 328-336. Anderson, L., Cross, A., Wynthein, D., Schmidt, L., & Grutz, K. (2011). Effects of Dynavision training as a preparatory intervention post cerebrovascular accident: a case report. (2011). Occupational Therapy in Health Care, 25(4), 270-282. Bigsby, K., Mangine, R.E., Clark, J.F., Rauch, J.T., Bixenmann, B., Susaret, A.W., Hasselfeld, K.A., & Colosimo, A.J. (2014). Effects of postural control manipulation on visuomotor training performance: comparative data in healthy athletes. International Journal of Sports Physical Therapy, 9(4), 436-446. Clark, J.F., Ellis., J.K., Bench, J., Khoury, J., & Graman, P. (2012). High performance vision training improves batting statistics for University of Cincinnati baseball players. PLo5 ONE, 7(1). Clark, J.F., Graman, P., Ellis, J.K., Mangine, R.E., Rauch, J.T., Bixenmann, B., Hasselfeld, K.A., Divine, J.G., Colosimo, A.J., & Myer, G.D. (2014). An Exploratory study of the potential side effects of vision training on concussion incidence in football. In press. Crotty, M., & George, S. (2009). Retraining visual processing skills to improve driving ability after stroke. Archives of Physical Medicine and Rehabilitation, 90, 2096-2102. Fragala, M.S., Beyer, K.S., Jajtner, A.R., Townsend, J.R., Pruna, G.J., Boone, C.H., Bohner, J.D., Fukuda, D.H., Stout, J.R., & Hoffman, J.R. (2014). Journal of Strength and Conditioning Research, 28(8), 2079-2087. Hoffman, J.R., Williams, D.R., Emerson, N.S., Hoffman, M.W., Wells, A.J., McVeigh, D.M., McCormack, W.P., Mangine, G.T., Gonzalez, A.M., & Fragala, M.S. (2012). L-alanyl-L-glutamine ingestion maintains performance during a competitive basketball game. Journal of the International Society of Sports Medicine, 9(4), 2-8. Hunt, L.A., & Arbesman, M. (2008). Evidence-based and occupational perspective of effective interventions for older clients that remediate or support improved driving performance. American Journal of Occupational Therapy, 62, 136-148. Kauffman, D.C., Clark, J.F., & Smith, J.C. (2014). The influence of sports goggles on visual target detection in female intercollegiate athletes. Journal of Sports Sciences, 13, 1-7. Klavora, P., Gaskovski, P., & Forsyth, R.D. (2000). Test-retest reliability of three Dynavision tasks, Perceptual and Motor Skills, 80, 607-610.

22
Klavora P, Gaskovski, P, Forsyth R.D. (1994). Test-retest reliability of the Dynavision apparatus. Perceptual and Motor Skills, 79: 448-450 Klavora, P., Gaskovski, P., Heslegrave, R.J., Quinn, R.P. & Young, M. (1995). Rehabilitation of visual skills using the Dynavision: a single case experimental design. Canadian Journal of Occupational Therapy, 62, 37-43. Klavora, P., Gaskovski, P., Martin, K., Forsyth, R.D., Heslegrave, R.J., Young, M., & Quinn, R.P. (1995). The effects of Dynavision Rehabilitation on behind-the-wheel driving ability and selected psychomotor abilities of persons after stroke. American Journal of Occupational Therapy, 49(6), 534-542. Klavora, P., Heslegrave, R.J., & Young, M. (2000). Driving skills in elderly persons with stroke: comparison of two new assessment options. Archives of Physical Medicine and Rehabilitation, 81, 701-705. Klavora, P., & Esposito. J. (2002). Sex differences in performance on three novel continuous response tasks. Perceptual and Motor Skills, 95, 49-56. Klavora, P., & Warren, M. (1998). Rehabilitation of visuomotor skills in poststroke patients using the Dynavision apparatus. Perceptual and Motor Skills, 86, 23-30. Schwab, S. & Memmert, D. (2012). The impact of a sports vision training program in youth field hockey players. Journal of Sports Science and Medicine, 11, 624-631. Strong, J.G., Jutai, J.W., Russell-Minda, E., & Evans, Mal. (2008). Driving and low vision: validity of assessments for predicting performance of drivers. Journal of Visual Impairment & Blindness, 102(6), 340-351. Unsworth, C.A., Lovell, R.K., Terrington, N.S., & Thomas., S.A. (2005). Review of tests contributing to the occupational therapy off-road driver assessment. Australian Occupational Therapy Journal, 52, 57-74. Vesia, M., Esposito, J., Prime, S.L., Klavora, P. (2008). Correlations of selected psychomotor and visuomotor tests with initial Dynavision performance. Perceptual and Motor Skills, 107, 14-20. Warren, M. (2008). Application of the Dynavision 2000 to rehabilitation of soldiers with traumatic brain injury. *A written statement prepared on behalf of Performance Enterprises for the House Committee on Veteran’s Affairs Hearing on Traumatic Brain Injury Related Issues. Wells, A.J., Hoffman, J.R., Beyer, K.S., Jajtner, A.R., Gonzalez, A.M., Townsend, J.R., Mangine, G.R., Robinson, E.H., McCormack, W.P., Fragala, M.S., & Stout, J.R. (2014). Reliability of the Dynavision D2 for assessing reaction time performance. Journal of Sports Science and Medicine, 13, 145-150.