
Information Pack for General Surgery Residency … GS Residency Info...Prepared by Tan Kok Yang 1...
32
Prepared by Tan Kok Yang 1 Information Pack for General Surgery Residency Programme as Participating Site NHG-AHPL Residency Programme May 2011
Transcript of Information Pack for General Surgery Residency … GS Residency Info...Prepared by Tan Kok Yang 1...

Prepared by Tan Kok Yang 1
Information Pack for General Surgery Residency
Programme as Participating Site
NHG-AHPL Residency
Programme
May 2011

Prepared by Tan Kok Yang 2
Introduction
During the exciting times of moving into Singapore’s newest restructured hospital, we invite
you to take the challenge in being one of the team in delivering a seamless patient
experience. As the General Surgery Department looks towards expanding into KTPH,
bounderies will be redefined and new frontiers will be explored.
As part of the NHG Residency programme for General Surgery, we aim to continue our good
tradition of teaching both basic knowledge and clinical skills by exploring new approaches
and optimizing the commitment of senior staff. These will be through structured teaching
and academic activities in line with the philosophies of the NHG Residency Programme.
Our department will be able to provide a wide mix of general surgical cases which is bound
to enhance the experience of our residents. Current areas of development and expansion
include Hepatobiliary Surgery, Colorectal Surgery, Upper Gastrointestinal Surgery and
Bariatric Surgery, Advanced Laparoscopic Surgery, Breast and Endocrine Surgery and
Advanced Endoscopy. Some of these specialties are pioneering new techniques of surgery
substantiated by research findings from the department. Residents will be given
opportunities to experience all the various facets of and learn the skills of General Surgery
with a hands-on approach that is supervised.
Our department also takes pride in its research output with frequent publications in
International peer-reviewed journals. Our presenters have also been recipients of awards
for their presentations at Scientific Meetings. There are a number of ongoing prospective
randomized trials and international collaborations that are being undertaken by the
department. Residents will be given the unique opportunity to immerse in this research
culture and be given opportunities to perform and publish clinical research findings.
We look forward very much to your contribution.

Prepared by Tan Kok Yang 3
General Surgery Faculty
Site Programme Director: Tan Kok Yang
Core Faculty: Kenneth Mak (HOD)
Tan Tzu Jen
Emile Woo
Cheah Yee Lee
Faculty: Anton Cheng
Poon Pak Leng
Jude Lee
Reyaz Singaporewalla
Subash Kumar
Radikha Lakshmi
(Ganesh Ramalingam)

Prepared by Tan Kok Yang 4
The Department of Surgery at Khoo Teck Puat Hospital comprises a Division of General
Surgery as well as a Division of Urology. These two clinical divisions provide a broad range of
clinical services, supported by visiting specialists to provide selected surgical subspecialty
services within KTPH.
Scope of Services
The General Surgery (GS) Division provides all-hours care for patients within the following
general surgical subspecialty domains, including:
Upper Gastrointestinal Surgery
Colorectal Surgery
Hepatobiliary and Pancreatic Surgery
Breast Surgery
Endocrine Surgery
Bariatric Surgery
Trauma Surgery
Vascular Surgery
Minimally Invasive Surgery
Endoscopy (both basic and advanced)
The GS Division also partners other clinical departments in the hospital to provide multi-
disciplinary care in the following clinical areas:
Geriatric Surgical Service
o With the Departments of Geriatric Medicine, Anaesthesia, Cardiology,
Dietetics and Nutritional Service, Rehabilitative Services and Nursing.
Head and Neck Surgery
o With the Departments of ENT and Dental Surgery
Trauma Service
o With the Departments of Anaesthesia and Orthopaedics
Bariatric Surgery

Prepared by Tan Kok Yang 5
o With the Health for Life Centre, Departments of Medicine, Anaesthesia,
Dietetics and Nutritional Service and Rehabilitative Services
Surgical Critical Care
o With the Department of Anaesthesia
The GS Division provides emergency surgical support for visiting consultants from KKWCH,
who in turn run an ambulatory antenatal clinic as well as outpatient gynaecology clinic in
KTPH. This includes support for peri-mortem caesarian sections in trauma patients.
The Urology Division provides both ambulatory and in-patient care for both elective and
acute urological clinical problems. Ambulatory urology includes a one-stop assessment
service in the outpatient clinics, with facilities for ultrasound scanning, cystoscopy and
Uroflow studies available. Outpatient management of urological stones is available through
ESWL facilities within the Urology clinic. In-patient services include the management of both
elective and acute urological problems, including the surgery for urological malignancies and
for urological trauma.
Visiting Specialists provide coverage in the following clinical areas:
Vascular Surgery
o Through service agreement with NUHS Department of Cardiothoracic and
Vascular Surgery, as well as by Dr Sanjay Nalachandran (private practice)
Plastic Surgery
o Through service agreement with SGH Department of Plastic Surgery
Neurosurgery
o Through service agreement with NUHS Division of Neurosurgery, Department
of Surgery
Emergency Cardiothoracic Surgical Support
o Through service agreement with National Heart Centre and NUHS
Department of Cardiothoracic and Vascular Surgery

Prepared by Tan Kok Yang 6
o This provides emergency surgical support for the interventional cardiology
service as well as for acute thoracic trauma care, in patients too unstable for
transfer to a hospital with tertiary level cardiothoracic surgery services.
Medical and Radiation Oncology
o Through service agreement with National Cancer Centre
o This provides for medical oncology clinics to be run in KTPH, dedicated clinics
for GI malignancies (Dr Simon Ong, Thursdays), Breast and Gynaecological
malignancies (Dr Lynette Ngo, Fridays), Head & Neck, Lung and Urological
malignancies (Dr Ang Mei Kim, Tuesdays) on a weekly basis. The medical
oncologists will also attend to in-patient consultations.
o Ambulatory Chemotherapy services will be provided in KTPH from September
2010. The hospital has plans to set up an in-house radiation therapy service,
with one linear accelerator to be operational in Q1, 2011 and a second linear
accelerator in 2012.
Visiting Consultants have admitting privileges to care for patients at KTPH. The surgical
teams within the Department ‘adopt’ the relevant VC into their teams so that junior staff
members within the affected team have the designated responsibility to look after the
patients on behalf of the specific VC.

Prepared by Tan Kok Yang 7
Department Staff Profile
Specialty/
Subspecialty
Remarks
Senior Consultants Clin Assoc Prof Kenneth Mak General Surgery, HPB
Surgery, Liver Transplantation, Trauma
Department Head, Educational Supervisor Core Faculty for NHG-AHPL Residency Programme
Dr Anton Cheng Kui Sing General Surgery, Laparoscopic Surgery, Bariatric Surgery
Dr Lim Tow Poh Urology
Consultants Dr Tan Kok Yang General Surgery, Colorectal
Surgery Associate Programme Director and Core Faculty for NHG-AHPL Residency Programme. Dept Research Coordinator
Dr Poon Pak Leng General Surgery, Colorectal Surgery
Coordinator for Medical Undergraduate Teaching
Dr Tan Tzu-Jen General Surgery, HPB Surgery, Bariatric Surgery, Laparoscopic Surgery
Core Faculty for NHG-AHPL Residency Programme
Dr Subash Kumar Breast Surgery
Dr Jude Lee E L General Surgery, Laparoscopic Surgery, Upper GI Surgery
Core Faculty for NHG-AHPL Residency Programme
Dr Emile Woo General Surgery Core Faculty for NHG-AHPL Residency Programme
Dr Amit Mukherjee Urology
Dr Colin Teo Chang Peng Urology

Prepared by Tan Kok Yang 8
Specialty/
Subspecialty
Remarks
Dr Ong Chin Hu Urology 2 years as AC
Dr Reyaz Moiz Singaporewalla
General Surgery, Endocrine Surgery, Head + Neck Surgery
1 year as AC Junior Staff Supervisor
Dr Radhika Lakshmanan General Surgery, Breast Surgery
1 year as AC
Dr Ganesh Ramalingam General Surgery, Trauma Surgery
0.5 years as AC Junior Staff Supervisor
Dr Cheah Yee Lee General Surgery Core Faculty for NHG-AHPL Residency Programme
The Department is recruiting several additional specialists, who are scheduled to join KTPH within
the next 6 months. This includes
Dr Julian Wong MBChB (Aberdeen), FRCS (General surgery)
Vascular Surgery Dr Wong will be 0.5 FTE in KTPH and 0.5 FTE in NUHS

Prepared by Tan Kok Yang 9
Visiting Specialists Prof Raj Nambiar Gen Surgery Ad hoc VC, participates in
teaching activities
Prof Low Cheng Hock Gen Surgery Ad hoc VC. Participates in teaching activities
A/Prof Chou Ning Neurosurgery Sessional visiting specialists. Provide 24/7 Neurosurgery cover in KTPH.
Dr Yeo Tseng Tsai
Dr David Choy
A/Prof Peter Robless Vascular Surgery Ad-hoc VC
Dr Chia Kok Hoong Ad-hoc VC
Dr Sanjay Nalachandran Sessional VC
Michael George Caleb Cardiothoracic Surgery Ad-hoc VC
Dr Francis Seow Choen Colorectal Surgery Ad-hoc VC
Dr Wong Soong Kuan Ad-hoc VC
Dr Eric Gan HPB, Advanced Endoscopy Sessional VC. Provides additional support for ERCP
Dr Ang Tiing Leong Gastroenterology, Advanced Endoscopy
Ad-hoc VC. Provides additional support for ERCP, EUS, stenting
Dr Christopher Khor Advanced Endoscopy Ad-hoc VC

Prepared by Tan Kok Yang 10
Registrars and Advanced Specialty Trainees
List Names Specialty/
Subspecialty
Remarks
Registrars
Dr Eugene Yang Weiren Neurosurgery NUH AST for Neurosurgery
Dr Roy Koh Neurosurgery NUH AST for Neurosurgery; on HMDP
Dr Eugene Lim Kee Wee General Surgery Completed AST exit examinations in August 2010
Dr Surendra Kumar
Mantoo
General Surgery AST (4th year)
Dr Ngiam Kee Yuan General Surgery AST (3rd year)
Dr Sim Hsien Lin General Surgery AST (3rd year); Currently in TTSH Surgery
Dr Anil D Rao General Surgery Probationary AST
Dr Shum Cheuk Fan Urology Service Registrar
Dr Germaine Xu Guiqin General Surgery AST; Currently TTSH
Dr Desmond Ooi Guo
Shen
General Surgery AST; Currently NUH
Dr Aaron Poh Guo Han General Surgery Service Registrar
Dr Tan Chun Hai General Surgery Service Registrar
Dr Daniel Lee Jin Keat General Surgery Service Registrar
Dr Arunesh Majumder General Surgery Service Registrar

Prepared by Tan Kok Yang 11
Junior Staff
Total number of MOs (out of complement of 10)
10
Total number of HOs 5
Number of Transitional Year trainees 1
Number of residents 5 From May 2011
Prepared by Tan Kok Yang 12
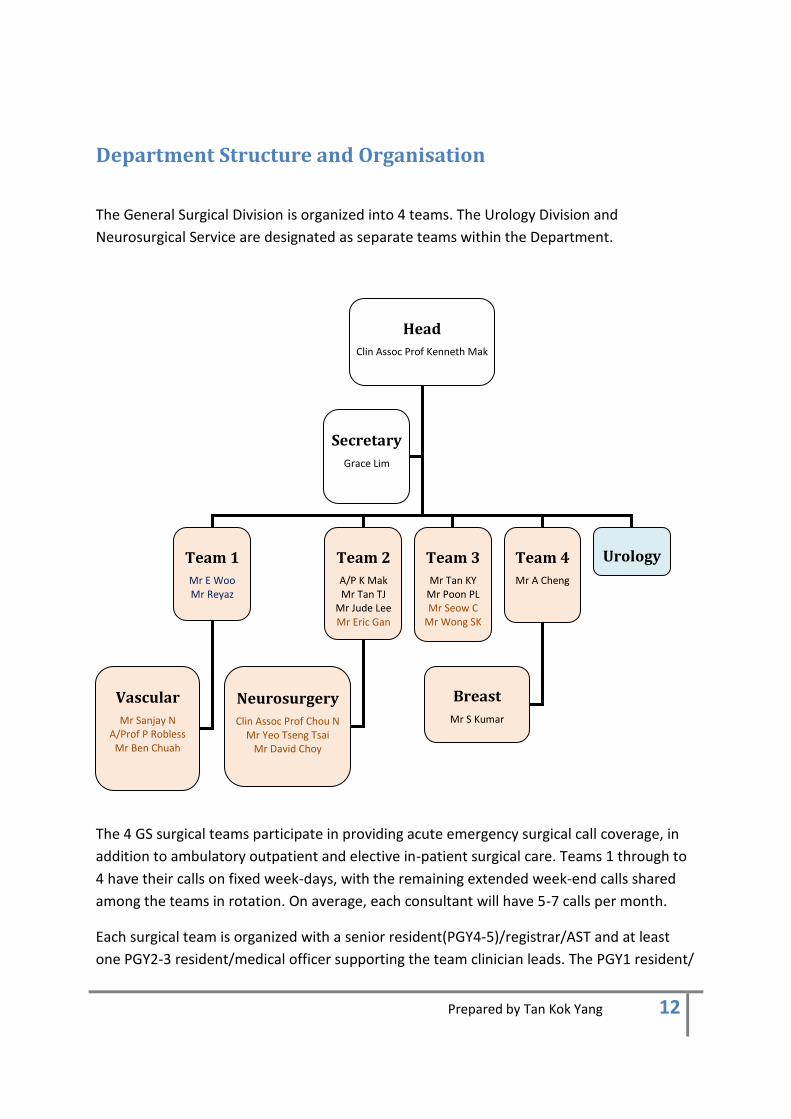
Department Structure and Organisation
The General Surgical Division is organized into 4 teams. The Urology Division and
Neurosurgical Service are designated as separate teams within the Department.
The 4 GS surgical teams participate in providing acute emergency surgical call coverage, in
addition to ambulatory outpatient and elective in-patient surgical care. Teams 1 through to
4 have their calls on fixed week-days, with the remaining extended week-end calls shared
among the teams in rotation. On average, each consultant will have 5-7 calls per month.
Each surgical team is organized with a senior resident(PGY4-5)/registrar/AST and at least
one PGY2-3 resident/medical officer supporting the team clinician leads. The PGY1 resident/
Head
Clin Assoc Prof Kenneth Mak
Team 1
Mr E Woo Mr Reyaz
Team 2
A/P K Mak Mr Tan TJ
Mr Jude Lee Mr Eric Gan
Team 3
Mr Tan KY Mr Poon PL Mr Seow C
Mr Wong SK
Secretary
Grace Lim
Team 4
Mr A Cheng
Urology
Neurosurgery
Clin Assoc Prof Chou N Mr Yeo Tseng Tsai
Mr David Choy
Vascular
Mr Sanjay N A/Prof P Robless
Mr Ben Chuah
Breast
Mr S Kumar
Prepared by Tan Kok Yang 13
house officers are distributed among the teams to maximize their learning opportunities.
The vascular service is supported by a GS registrar, and the neurosurgical team is supported
by a GS medical officer.
Acute Care Call System
Current Department on-call teams to comprise one senior resident(PGY4-5)/registrars, two
PGY2-3 resident/medical officer and one PGY1 resident/house officer. The senior members
of the call team reviews acute cases as far as possible at the A&E Department, clerking the
cases at the point of first review, so as to minimize the burden in the wards, after transfer
from the A&E.
All on-call staff have access to rest rooms during their calls. In addition, the hospital has a
staff lounge which the staff can utilize for rest during the day, even when they are not on
call. Duty hours will be guided according to ACGMEi requirements and will be tracked.
ICU – HD coverage
The ICU strategic development masterplan for KTPH envisages a phased expansion of the
SICU – High Dependency Unit bed capacity beyond its current 8 SICU + 4 HD beds. The
Department of Anaesthesia will continue to run the Surgical ICU in a closed concept. Surgical
High Dependency will be under the charge of Department of Surgery. There will be rotation
of residents into Surgical ICU and HD with formal training provided jointly by the
Departments of Anaesthesia and Surgery.

Prepared by Tan Kok Yang 14
Educational Activities
Residents participate in educational activities at hospital level and department level. All
educational activities are designated protected time for training.
Hospital Level
Monthly clinical forum
Monthly clinic-pathologoical conference
Fortnightly Radiology Department tutorials
Department Level
Mon Tue Wed Thur Fri Sat
Am AST /PGY
4-5
teaching
0730-
0830
Grand Wd
Round
0730-0830
PGY 1-3
teaching
0730-0830
M&M
0730-0900
Journal
Club
0700-0830
Combined
programmes
with TTSH
AST
masterclasses
Pm Clinical
teaching
1630 -
1730
Breast
Tumour
board
Fortnightly
GI Tumour
board
1630 –
1800
Fortnightly
Radiology
conference
1630-1730
Monthly
To be
scheduled
by APD
Teaching
clinics
Subspecialty
teaching
Research
meeting

Prepared by Tan Kok Yang 15
I) Monday Clinical Teaching by Core Faculty
Goal: To increase the knowledge involving common surgical topics, including diagnosis,
treatment and managements of surgical diseases.
Venue: To be confirmed with GS Department secretary
Time: Monday, 1630-1730
This will combine topic discussions with clinical teaching. Residents are required to present
1 intereresting case under their service each. Residents are required to read around that
particular topic prior to the teaching and present key points of learning.
Requirements:
1) Residents must attend at least 75% of clinical teachings.
II) Surgical Grand Rounds
Goal: To increase knowledge in the area of diagnosis and treatment of surgical diseases
with special emphasis on critical care issues. Surgical management will be scrutinized and
discussed.
Venue: SICU for all
Time: Tuesday, 0730-0830
The Surgical Grand Rounds consist of bedside teaching session and discussion on the cases
in the SICU. Clinical management, diagnosis, surgical and critical care management of these

Prepared by Tan Kok Yang 16
patients will be discussed. The sessions are usually conducted by the HOD or Senior
Consultants of the department. Visiting consultants are usually present for further input.
Residents are expected to present these cases for discussion. Senior residents are expected
to be able to discuss their clinical decisions and management for the patients. All residents
are expected to discuss the cases for presentation with the consultant in charge prior to
presentation. Residents should read up on relevant topics
Requirements:
1) Residents must attend at least 75% of the Grand Rounds.
2) Active participation in the discussions is expected and will be tracked by APD.
III) Journal Club
Goal: This forum serves 2 purposes:
1. Updates of relevant surgical topics in various disciplines
2. Critical appraisal of journal articles and discussions on evidence levels
Venue: Boardroom
Time: Friday, 0730-0830
Trainees and residents will take turns to present at the journal clubs. The topic or paper for
presentation should be determined with the consultant in charge (teams will take turns) at
least 1 week prior to presentation and the topic or paper disseminated to the department
for prereading
Requirements:

Prepared by Tan Kok Yang 17
1) Residents must attend at least 75% of the Journal Club.
2) For topic review, presenter should present a summary of a few key papers on the
topic.
3) For critical appraisal of a paper, the presenter is expected to do a well thought-out
summary, present key data and systematically criticize the methodology.
IV) Morbidity & Mortality Conference (M & M)
Goal: To provide residents and faculty an opportunity to review and improve their
approach to treatment and management of surgical patients through thoughtful and
systematic analysis of any complications, deaths and complex cases which occurred or were
operated on in the preceding week. To increase the residents’ knowledge and awareness of
system and evidence based practice in enhancing total patient care. Residents will have an
opportunity to learn from the management issues fo other residents and faculty members.
M & M is held weekly on Thursday to review current complications, deaths and interesting
or complex cases operated on the preceeding week. Listed operations for the following
week will also be discussed with emphasis on identification of correct indications for surgery
and preoperative work-up. This is a forum for open, non-heirachical discussion of
mortalities, surgical complications and management of complications with an honest review
of what could have been done better or whether changes need to be implemented.
Venue: Boardroom
Time: Thursday, 0730-0900
Objectives:
1) Residents will present surgical complications and/or deaths and systematically
discuss their decision making and management of care to identify possible
options which may have resulted in a more positive outcome. (Please follow the
format of the department M&M reporting)

Prepared by Tan Kok Yang 18
2) Resident analyze decision making and apply knowledge, experience and feedback
to future practice experience.
3) The Senior Resident are tasked to manage M&M reporting will need to fill up the
reporting form and ensure that the information on the M&M reporting slides is
accurate for auditing and archiving by the hospital.
V) Teaching Lectures
Goals: To discuss and teach common core topics of managing medical and surgical
emergencies for interns and junior residents.
Core acute topics in medicine and surgery will be front loaded in the first few weeks of a
new residency year to facilitate understanding and increasing competency of junior
residents in handling common medical emergencies. (Organised by primary institution)
All surgical core topics will be covered in coordination with TTSH through these lectures.
Lectures should be interactive.
Venue: To be confirmed
Time: Wednesday, 0730-0830
V) General Surgery Tumour Board
Goals: For residents to understand and be involved in the multidisciplinary management of
cancer patients. Also become familiar with some of the complexities of certain cancer
patients.

Prepared by Tan Kok Yang 19
This is a forum for multidisciplinary discussion of cancer patients including discussions on
surgical and histological findings that may impact on the further management of cancer
patients with neoadjuvant and adjuvant treatments.
Residents:
1) Residents should present cancer patients that they have been involved with.
Discussion points on the patients should be confirmed with the consultant-
in-charge.
2) Tumour board findings and recommendations should be clearly documented
by the resident in the case-sheets and follow-up ensured.
Venue: Boardroom
Time: Thursday, 1630-1800 fortnightly
VI) Radiology Conference
Goals: For residents to learn reading of diagnostic imaging findings through clinical
correlation with surgical and pathological findings.
This is a forum is conducted by radiologists with discussions on key findings of images.
Indications are discussed. Correlation with clinical and surgical findings are performed for a
learning experience for all levels.
1) Residents must attend 75% of radiology conferences
2) Residents are expected to present the clinical aspects of the cases
Venue: To be confirmed
Time: Friday, 1630-1730 monthly

Prepared by Tan Kok Yang 20
VII) Research Meeting
Goals: Residents are expected to be involved in clinical research in the department and the
meeting is a time for discussions on the methodology and progress.
Time: Fortnightly with supervisor faculty
VIII) Teaching Clinics and Subspecialty Teaching
Goals: These are for clinical teaching in the outpatient setting and also for more specialized
teaching of subspecialties.
Courses and Workshops
The following are courses that the residents are expected to participate in while rotating to
KTPH General Surgery.
Hospital level
Combined perioperative services orientation workshop
Annual hospital-wide research forum
Research / Manuscript writing workshop
Prepared by Tan Kok Yang 21
Department Level
American College of Surgeons Fundamentals of Laparoscopic Surgery
Bowel anastomosis workshop
Basic ultrasound workshop
Fine-needle aspiration cytology course

Prepared by Tan Kok Yang 22
Educational Contents and Goals of GS Rotation to KTPH in R1
Goals and Objectives
Patient Care
Patient care responsibilities will be graduated according to resident proficiency and PGY
status.
The resident should demonstrate the ability to:
1. Evaluate common surgical conditions through a comprehensive history, physical
examination, and appropriate diagnostic studies and particularly identify ill patients.
2. Be familiar with fluid, electrolyte and nutritional requirements of surgical patients;
become competent with ward procedures including intravenous assess, central
venous line, chest tube insertion.
3. Understand the operative steps for commonly performed lower complexity
procedures
1. Appendicectomy for simple and complicated appendicitis including laparoscopic
approach
2. Inguinal hernia repair
3. Proper excision of lumps and bumps including lymph node biopsy
4. Incision drainage of abscesses
5. Principles of opening and closing the abdomen
4. Manage trauma patients including application of ATLS principles and basic surgical
management.
5. Be familiar with common general surgical conditions including hepatobiliary sepsis,
gastrointestinal bleeding and pancreatitis.
Medical knowledge
The resident should develop a modest understanding of
1. Physiology of surgical illness and stress
2. Basic pathology of surgical disease in a general surgery department
3. Resuscitation of surgical patient (sepsis, hemorrhagic shock)

Prepared by Tan Kok Yang 23
4. Typical clinical presentation, basic evaluation and management of common general
surgical conditions
Appendicitis
Abdominal hernias
Cholecystitis
Hepato-biliary sepsis
Pancreatitis
Intestinal obstruction
Gastrointestinal perforation
Gastrointestinal cancers
Gastric outlet obstruction
Gastrointestinal bleeding
Practice Based Learning and Improvement
The resident should demonstrate the ability to
1. Critically evaluate published literature regarding the diseases managed on general
surgery service, and formulate evidenced-based therapeutic plan.
2. Summarise the relevant major cases and present them at the M&M meeting in a
constructive and educational manner
3. Prepare in advance for teaching rounds and conferences with an emphasis on
punctual and regular attendance.
4. Teach junior doctors and medical students posted to the department.
5. Residents should participate in workshop and conferences organised by the
department.
Interpersonal and Communications Skill
The resident should demonstrate the ability to
1. Work effectively with peers and nursing colleagues in managing patients.
• Communicate abbreviated yet thorough patient discussions with senior staff

Prepared by Tan Kok Yang 24
• Counsel patients and their families, including discussions of complex general surgical
procedures and disorders.
• Update relevant involved medical and allied health personnel via phone or written
communication with regard to patient care.
Professionalism
The resident should
1. Demonstrate responsible commitment to patients; be ready to provide bedside and
operative care to patients irrespective of time of day.
2. Demonstrate sensitivity to age, gender, and culture of patients and their families and
other health care professionals.
3. Carry out administrative responsibilities (medical reports, discharge procedures) in a
time-sensitive manner
Systems Based Practice.
The resident should
1. Demonstrate the ability to efficiently organize the care of the surgical patient in a
cost-effective and evidenced-based manner.
2. Appropriately recruit other specialists and health care professionals to optimize the
care of the surgical patient
3. Adhere to hospital policies and procedures and other regulatory guidelines
Support for Training and Service
The programme is supported financially by the Ministry of Health (MOH) Singapore and
Alexandra Health Pte Ltd with financial commitment for hiring backfill for faculty to optimize
service and teaching.
Manpower backfills are as follows:

Prepared by Tan Kok Yang 25
Protected Time for Education
– 0.5 FTE for Designated Institutional Officer
– 0.2 to 0.3 FTE for Associate DIO (ADIO)
– 0.5 FTE for Program Directors (PD)
– 0.3 FTE for Associate Program Directors (APD)
– 0.2 for Core Clinical Faculty Members (CCFM)
Education/Teaching Time includes:
a) Protected Education/Teaching Time (PET)
• Defined as teaching activities without any service rendered. E.g. lectures, journal club,
conferences.
b) Service Education/Teaching Time (SET)
• Teaching while providing service
• Includes ward rounds, clinics in which there is a resident with you and active learning is
taking place
• For CCFM= 15hrs per week PET+SET
• For Faculty Members= at least 0.1FTE, any combination of PET and SET
KTPH members of the NHG-AHPL GMEC, headed by ADIO Dr Tavintharan Subramaniam have
regular meetings to evaluate resources, training and have oversight on all residency
rotations in KTPH. Admin support will be from Institutional Coordinator, Sabrina Kay.
Faculty development funds are available for educational courses for the teaching faculty.
IT facilities and resources are provided with broadband access. Medline journal indexing as
well as electronic journal subscriptions are provided by KTPH. The hospital also has a
Learning Centre with a library being set up.

Prepared by Tan Kok Yang 26
KTPH has a computerized clinical data management system that will allow all residents to
assess radiographic, laboratory data, discharge summaries from any computer in the
hospital using a secured password assess.
Information and resources for education will be available on the education website of KTPH.
At department level, the department has a library with a wide selection of textbooks and
reference materials. The department also has a collection of AV material, including training
course videos and videos on various surgical procedures.
The department also has specific surgical skills training facilites including an Experimental
Surgery Lab, Minimally Invasive Surgery trainers and facilities to conduct the FLS course.
All residents will have ongoing assess to TTSH simulation centre facilites.
Resident Orientation Hospital-wide orientation package for new staff will be provided. This will include the
perioperative services orientation, information on call rooms, safety and security, rest areas
and education and resources areas.
Residents will be briefed by the APD on the goals, learning objectives, team assignments and
expected duties at the start of each rotation. Roster of clinical activities will be provided to
the residents including their daily clinical duties and call duties. Education programme will
also be distributed.
The NHG Residency Handbook and General Surgery Program Handbook will be provided if
not already.

Prepared by Tan Kok Yang 27
Other Learners
As stated previously, due to the department’s commitment to medical student, BST and AST
training, there will be a number of other learners. This has previously been factored in
during the projection for GS re.sidency numbers for the department. Adequacy of clinical
material will be deconflicted by the KTPH APD ensuring adequate faculty to resident ratio
and educational benefits.
Common educational training and resources are shared among residents and other learners.
There will be constant review to ensure adequate places for workshops for all residents.
Medical students will provide residents opportunity to engage in teaching, supervision and
leadership.
Complaints and Grievances Residents will be briefed on the possible communication channels for them to raise
complaints and concerns in a confidential manner with steps taken to minimize fear of
retaliation.
Prepared by Tan Kok Yang 28
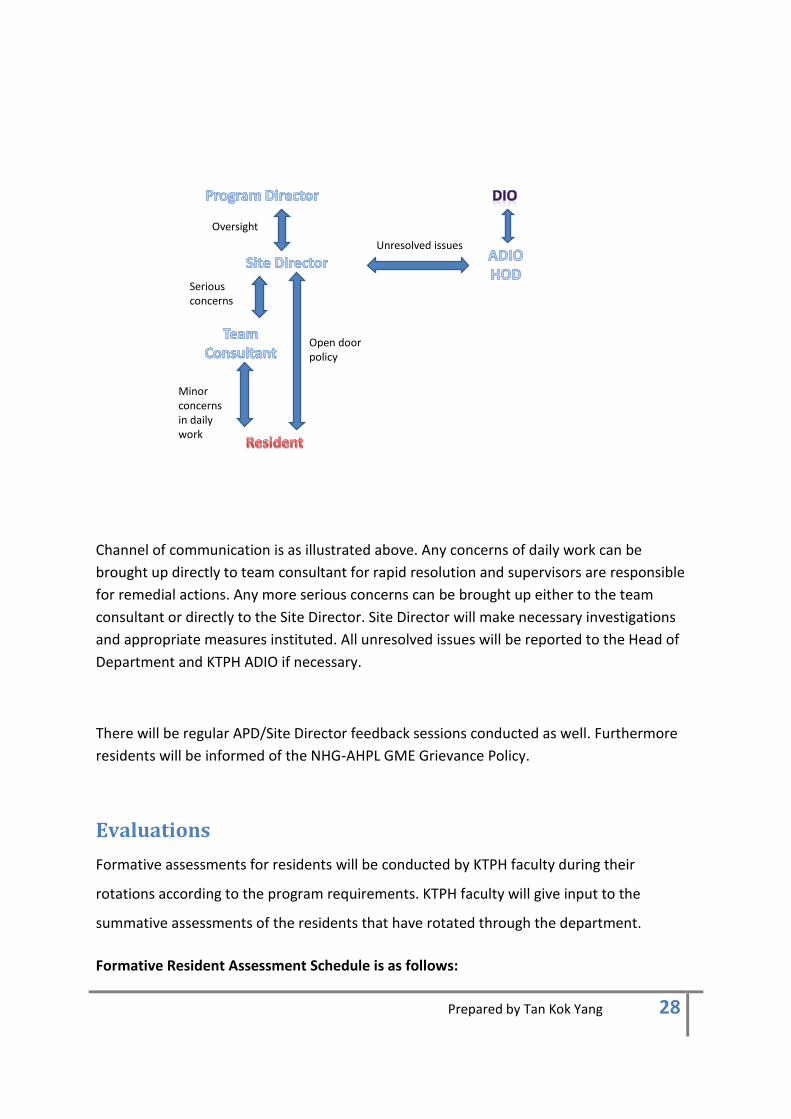
Oversight
Open doorpolicy
Minor concerns in daily work
Serious concerns
Unresolved issues
Channel of communication is as illustrated above. Any concerns of daily work can be
brought up directly to team consultant for rapid resolution and supervisors are responsible
for remedial actions. Any more serious concerns can be brought up either to the team
consultant or directly to the Site Director. Site Director will make necessary investigations
and appropriate measures instituted. All unresolved issues will be reported to the Head of
Department and KTPH ADIO if necessary.
There will be regular APD/Site Director feedback sessions conducted as well. Furthermore
residents will be informed of the NHG-AHPL GME Grievance Policy.
Evaluations
Formative assessments for residents will be conducted by KTPH faculty during their
rotations according to the program requirements. KTPH faculty will give input to the
summative assessments of the residents that have rotated through the department.
Formative Resident Assessment Schedule is as follows:
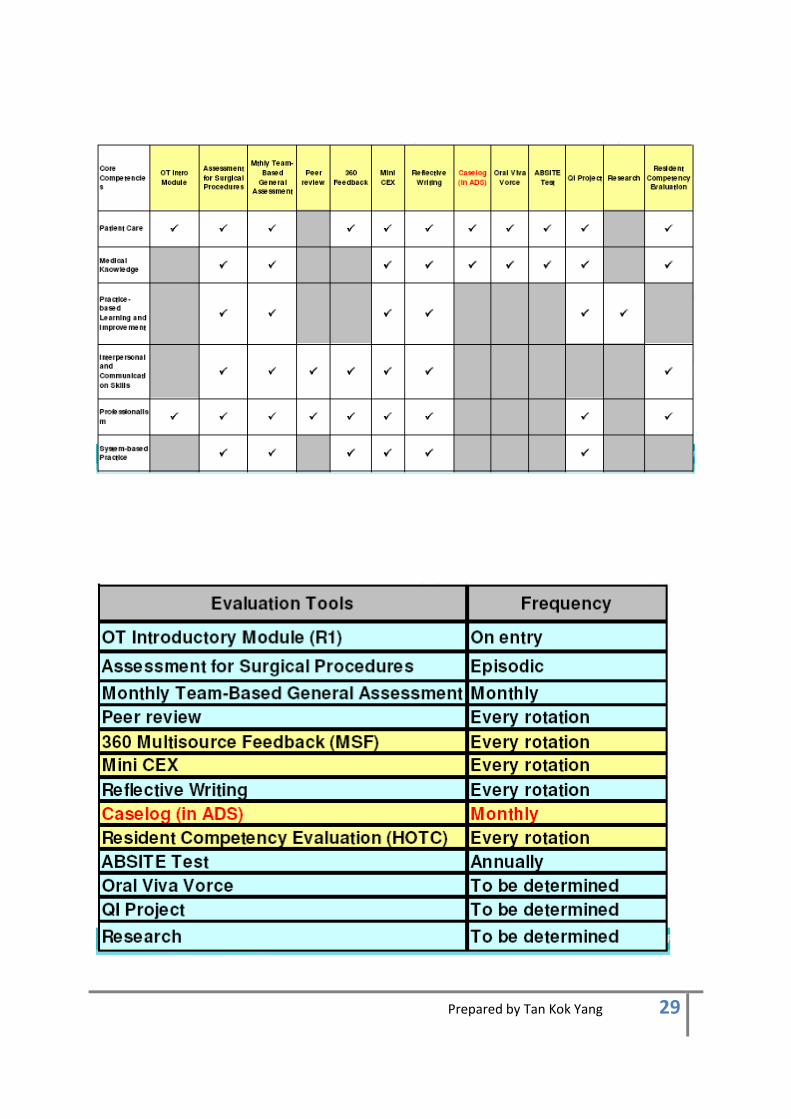
Prepared by Tan Kok Yang 29

Prepared by Tan Kok Yang 30
Assessments will be triggered by the Program Coordinator who maintains a program
calendar with the timeline for the assessments and evaluations clearly marked out. The site
director will oversee if there are any delays in the returning of evaluation and take
necessary action.
KTPH faculty are members of the Clinical Competency Committee which will use information
from resident evaluations and other sources including exam scores, patient feedback,
attendance records, publications to perform semiannual resident evaluations.
Faculty Evaluation Schedule:
Site director will have oversight of the feedback on his faculty. Program Evaluation
Committee will take into considerations feedback on faculty in discussing action plans.
Feedback to faculty will be provided yearly.
Program Evaluation
This will be performed as a whole together with TTSH.

Prepared by Tan Kok Yang 31
Supervision
The Site Director/APD together with the HOD are the educational supervisors of the
department. The site director will meet with all residents at the start of the rotation and
also on a regular basis.
The team consultant is responsible for the care of all the patients under his/her team.
He/She will delegate graded responsibilities according to the competency of the residents.
Given the supervision is conducted within the team structure, the trainees will receive close
supervision during ward rounds, clinics and during the team’s weekly operating lists and
endoscopy lists.
Duty Hours and Fatigue
Duty Hours will be according to ACGMEi requirements which are available on the NHG-AHPL
Residency Handbook. The roster planner will take into account these requirements.
Averaged over 4 weeks, residents duty hours will not exceed 80 per week, night duties have
a 24+6 rule with 24 hours of duty followed by 6 hours of no further new cases. All residents
will get 1 full day of rest per week. After night duty, residents will get 10 hours off at least.
All duty hours will be reported by the resident to the Institutional Coordinator who will fed
back to the Site Director weekly. Remedial actions will be performed to ensure compliance
to the 320 hours per 4 weeks requirement.
In addition, all faculty will be informed to look out for signs of fatigue and stress in the
residents under their charge.
All residents will be informed of the symptoms and signs of fatigue and sleep deprivation.
Research and Scholarly Activities
The site director, Tan Kok Yang, is also the department research coordinator. He has the
responsibility of assigning research projects to all trainees in the department.
Scholarly Activities for the Department will have the following principles:
Core faculty should be PI/Co-I of at least 1 project

Prepared by Tan Kok Yang 32
Faculty encouraged to be Co-I of at least 1 project
Research grants for the department
Involvement of ALL GS residents in at least 1 research project from R2 year
Research project will be assigned with option to change topic
Residents should have ownership of the project and will have 1 research mentor
Project to be completed in 1 year with communication with resident even after
leaving the department
Research presentations at least in local forums, KTPH Research Forum


















