‘The Holy Grail’ -mediators of inflammation. Lecture 3 Rod Flower, WHRI, London.
description
Inflammation: Mediators to Management
Inflammation and the Spine: Mediators to Modulators
J. Scott Bainbridge, M.D.
Denver Back Pain Specialists, LLC
www.DenverBackPainSpecialists.com
Overview
Nociceptive vs Neuropathic Pain
Vs Inflammatory Pain
Lines blurred
Stimuli and Mediators of Inflammation
Inflammation soup
Multi-level Processing of Pain
Neuro-plasticity
Multi-level modulation of inflammatory response
Treatment Strategies and Options
Objectives
Elucidate evidence for role of inflammation in pain of spinal origin.
Describe chemical pathways, mediators, and pharmacological treatments of inflammation.
List side effects of commonly used anti-inflammatory drugs.
Introduce basis for use of exercise, CAM, mindfulness, nutritional, and other treatments for inflammatory pain.
Disclosure
Principal investor in Nutrakinetics, LLC.
Nutraceutical company with interest in anti-inflammatory products
Spouse, Professor Jacquelyn Bainbridge, Pharm.D., involved in team building and distribution of Mona Vie nutritional products
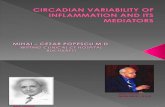
Scholz and Woolf; 2002
Plasticity
Peripheral sensitization
Altered sensory neuron excitability
Wind-up
Central sensitization
Synaptic reorganization
Long term potentiation
Disinhibition
Glial activation
Kwon; 2004
Hall; 2004
Hall and Springer; 2004
Scholz and Woolf; 2002
Kwon et al; 2004
Clinical uses of glucocorticoids
Acute whiplash: + one trial IV
Acute spinal cord inj: + high dose methylprednisolone
IM or PO: negative (spine pain)
Spinal: mixed
Intraoperative (HNP/radic): +
Glucocorticoid Action
Decrease Inflammation
decrease prostaglandin, leukotriene synthesis
decrease PMN migration
Direct Membrane Stabilization
Modulation of Periph Nociceptor Neurons
Mod of Spinal Cord Dorsal Horn Cells
Slight Anesthetic Effect
Pharmacologic Properties of Commonly Used Corticosteroids
Relative Potency
Click to edit Master text styles
Second level
Third level
Fourth level
Fifth level
Corticosteroid Side Effects
Fever
Myalgia
Malaise
Fluid and electrolyte imbalance
Hypertension
Hyperglycemia
Myopathy
Ulcers
Immunosuppression
Behavioral changes
Allergic reaction
Pituitary-adrenal suppression
Abrupt withdrawal after prolonged use: acute adrenal insufficiency
Corticosteroid Side Effects
Cardiovascular System
Prolonged Use: hypertension due to Na+ uptake
Direct effects due to steroid receptors on heart and smooth muscle
cardiac output and vascular tone
Corticosteroid Side Effects
Musculoskeletal
Avascular necrosis
Bone mineral density loss
Muscle weakness and wasting
Case report of steroid myopathy after one epidural injection
(Boonen S et al. Br J Rheumatol 1995;34:385-6)
Corticosteroid Side Effects
Central Nervous System
Euphoria
Behavioral changes; psychosis
EEG abnormalities
Excitability of nervous tissue
Corticosteroid Side Effects
Gastrointestinal System
Gastric acid secretion
Risk ulcer especially if on NSAIDs
Fat absorption
Endocrine System
ACTH, TSH, FSH, Testosterone
Adrenal Suppression
Intra-articular glucocorticoid injection
Serum cortisol suppressed at 1 week independent of dose 40mg triamcinolone
Duration of local and systemic effect increase with decreased solubility
(Armstrong RD et al. Ann Rheum Dis 1981;40:571-4)
Adrenal Suppression
Epidural steroid injection (ESI)
Suppresses adrenal function 3 weeks
25 mg Hydrocortisone/80 or 160 mg Methylprednisolone
(Benzon HT. Pain 1986;24:277-95)
Adrenal Suppression
ESI
Study of 2 individuals, single dose 160mg methylprednisolone, steroid naive
Complete cortisol suppression 6 days
Incomplete at least 4 weeks
Therefore, epidural dosing similar systemic availability to low daily oral glucocorticoid
(Dubois EF et al. Clin Rheumatol 2003;22:12-7)
Osteocalcin Depression with Oral Prednisone
Wilson AM et al. Chest 1998;114:1022-7.
Bone Mineral Density and ESI
Does ESI cause bone loss?
Cross-sectional study of relationship between cumulative ESI dose and BMD
Inconclusive dose relationship
Osteoporosis/osteopenia higher than general population
Could be that all doses caused decreased BMD
(Dubois EF et al. Clin Rheumatol 2003;22:12-7)
Bone Mineral Density and ESI
Prospective study 204 patients, 123 follow-up at one year
No change in BMD after standard doses spinal steroids
All spinal injections included
DXA at forearm
Calcium/Vit D ?
(Manchikanti L. Pain Physician 2000 Oct;3(4):357-66)
Bone Mineral Density and ESI
If ESI = 10-20mg PO x 4 weeks, THEN:
ACR 2001 update for oral steroids
Ca++/Vit D all starting low/moderate dose
Bisphosphonates 5mg/day for > 3 mo
Bisphosphonates 5mg/d long term with osteoporosis or osteoporotic fracture
Local Anesthetics
Hematologic effects
Epidural inhibit platelets, fibrinolysis, and leukocyte function
Granulocyte migration /metabolic activation at surgical sites
(Naguib M et al. Drug Safety 1998 Apr; 18(4)221-50)
Local Anesthetics
Tissue Effects
Cytotoxic to chondrocytes
Bupivicaine 0.5%, 15-30 min in vitro
Intact cartilage provided partial protection
(Chu CR et al. Arthroscopy 2006; 22:693-9)
Inhibit Fibroblasts
Myotoxic
(Hogan Q. Regional Anesthesia 1996;21:43-50)
Local Anesthetics
Neural Toxicity
Intrathecal lidocaine more neurotoxic than epidural
Dose-dependent toxicity found in rats
Doses studied much higher than those used in humans
(Kirihara Y et al. Anesthesiology 2003;99:961-8)
Local Anesthetics
Overall safety
Large scale surveys attest to overall safety of spinal anesthetics
(Hodgson P et al. Anesth Analg 1999;88:797-809)
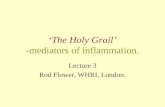
Tumor Necrosis Factor (TNF-)
TNFa is a principal mediator of acute inflammatory responses
Macrophages: primary source
Mediator of inflammation, tissue destruction, and organ injury
Lipopolysaccharide is a strong inducer of TNF- release from macrophages
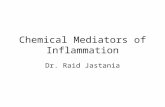
Homotrimer structure (3 protein chains)
Membrane-bound and soluble forms of TNF-
33
Point of Slide: Background on general immune functions of TNFa (if required, otherwise move to backup slides)
TNF-alpha (or simply TNF) is the principal mediator of the acute inflammatory response. [Abbas p247] It is produced by macrophages and lymphocytes, but its primary source is macrophages. TNF-alpha functions with interleukin-1 to mediate inflammation. [Abbas p253] Tumor necrosis factor has a broad spectrum of biologic activity. [Bazzoni 1996 p1717] It is a mediator of inflammation, tissue destruction, and organ injury. [Harris 2005 p940]
All members of the TNF family, including TNF-alpha, are believed to consist of 3 polypeptide (protein) chains (shown in different colors on this illustration). [Bazzoni 1996 p1717] This structure of 3 protein chains is called a homotrimer.
Tumor necrosis factor exists in both membrane-bound and soluble (circulating) forms. [Janeway, online book] The membrane-bound form is cleaved by a molecule called TACE, and is freed from the cell membrane.
The secreted molecules then aggregate into the trimolecular complex of TNF, which can bind to and activate receptors. [Papadakis 2000 p1148] Both membrane-bound and soluble forms of TNF bind to TNF receptors on cell surfaces. [Harris 2005 p380]
NSAIDs
Good evidence for efficacy in acute or episodic back pain
NSAID Cardiovascular Toxicity
Nonselective NSAIDs as a class associated with increased risk of acute MI
Relative risk 1.19, 95% CI 1.08-1.31
This meta-analysis limited by heterogeneity
NSAID Gastrointestinal Toxicity
1.3-1.6% annual risk of hospitalization or death due to NSAID-associated gastropathy
1 in 3 RA patients over course of disease
Long-term NSAID users:
10% Nonspecific dyspepsia
1-10% Serious GI bleeding or ulceration
< 1% Kidney toxicity and others
NSAIDs Renal Toxicity
Aspirin doses as low as 75 mg/day may still have adverse renal effects
Study of elderly patients given aspirin 75 mg/day for 1 week, 150 mg/day for 1 week, 325 mg/day for 1 week, then no aspirin for 1 week
All aspirin doses reduced creatinine clearance and uric acid secretion, especially in patients with low albumin levels or taking diuretics
Risk of NSAID toxicity increased with diminished renal function or decreased effective intravascular volume due to diuretic therapy, cirrhosis, or congestive heart failure
NSAIDs and Pregnancy
NSAIDs may be associated with increased risk for miscarriage
Association of NSAIDs with miscarriage based on prescription use of NSAIDs in 63 (1.5%) of 4,268 women who had a miscarriage and 318 (1.5%) of 21,750 women who had a live birth which shows no significant difference but there were significant differences in subgroups when accounting for use of NSAIDs in the preceding 1-9 weeks
In utero exposure to analgesics may be associated with increased risk of developing schizophrenia
Large cohort study found > 4 times increased risk of schizophrenia in persons with analgesic exposure during second trimester
Use of NSAIDs during third trimester may cause premature closure of ductus arteriosus and persistant pulmonary hypertension; uncommon if drug discontinued 6-8 weeks before delivery
Use of NSAIDs during third trimester may cause premature closure of ductus arteriosus and persistant pulmonary hypertension; uncommon if drug discontinued 6-8 weeks before delivery
Other NSAID ADRs
CNS changes (dizziness, aseptic meningitis)
Hepatotoxicity (especially with diclofenac)
Severe rashes (e.g., Steven Johnsons Syndrome)
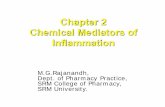
Nutrients/Supplements
Anti-oxidants
Anti-inflammatory (COX inhibition or other mechanisms)
Recommendations for patients
Diet high in antioxidants (multicolored food choices)
Diet high in good fats (polyunsaturated, omega-3)
Supplement vitamin D3, Omega-3, possibly concentrates of antioxidants
Avoid trans-fats, excessive alcohol or simple sugars/starches (pro-inflammatory)
Bibliography
Alper, A. B., Jr., H. Tomlin, et al. (2006). "Effects of the selective cyclooxygenase-2 inhibitor analgesic celecoxib on renal carbonic anhydrase enzyme activity: a randomized, controlled trial." Am J Ther 13(3): 229-235.
Autio, R. A., J. Karppinen, et al. (2006). "The effect of infliximab, a monoclonal antibody against TNF-alpha, on disc herniation resorption: a randomized controlled study." Spine (Phila Pa 1976) 31(23): 2641-2645.
Ballantyne, J., S. Fishman, et al. (2010). Bonica's management of pain. Philadelphia, PA, Lippincott, Williams & Wilkins.
Bombardier, C., L. Laine, et al. (2000). "Comparison of upper gastrointestinal toxicity of rofecoxib and naproxen in patients with rheumatoid arthritis. VIGOR Study Group." N Engl J Med 343(21): 1520-1528, 1522 p following 1528.
Boswell, M. V., R. V. Shah, et al. (2005). "Interventional techniques in the management of chronic spinal pain: evidence-based practice guidelines." Pain Physician 8(1): 1-47.
Chou, R., J. D. Loeser, et al. (2009). "Interventional therapies, surgery, and interdisciplinary rehabilitation for low back pain: an evidence-based clinical practice guideline from the American Pain Society." Spine (Phila Pa 1976) 34(10): 1066-1077.
Chou, R., A. Qaseem, et al. (2007). "Diagnosis and treatment of low back pain: a joint clinical practice guideline from the American College of Physicians and the American Pain Society." Ann Intern Med 147(7): 478-491.
Cohen, S. P., N. Bogduk, et al. (2009). "Randomized, double-blind, placebo-controlled, dose-response, and preclinical safety study of transforaminal epidural etanercept for the treatment of sciatica." Anesthesiology 110(5): 1116-1126.
Doidge, N. (2007). The brain that changes itself : stories of personal triumph from the frontiers of brain science. New York, Viking.
Dubois, E. F., M. F. Wagemans, et al. (2003). "Lack of relationships between cumulative methylprednisolone dose and bone mineral density in healthy men and postmenopausal women with chronic low back pain." Clin Rheumatol 22(1): 12-17.
Hall, E. D. and J. E. Springer (2004). "Neuroprotection and acute spinal cord injury: a reappraisal." NeuroRx 1(1): 80-100.
Bibliography
Hurwitz, E. L., E. J. Carragee, et al. (2008). "Treatment of neck pain: noninvasive interventions: results of the Bone and Joint Decade 2000-2010 Task Force on Neck Pain and Its Associated Disorders." Spine (Phila Pa 1976) 33(4 Suppl): S123-152.
Jensen, G. S., X. Wu, et al. (2008). "In vitro and in vivo antioxidant and anti-inflammatory capacities of an antioxidant-rich fruit and berry juice blend. Results of a pilot and randomized, double-blinded, placebo-controlled, crossover study." J Agric Food Chem 56(18): 8326-8333.
Kay, J., J. W. Findling, et al. (1994). "Epidural triamcinolone suppresses the pituitary-adrenal axis in human subjects." Anesth Analg 79(3): 501-505.
Korhonen, T., J. Karppinen, et al. (2006). "The treatment of disc-herniation-induced sciatica with infliximab: one-year follow-up results of FIRST II, a randomized controlled trial." Spine (Phila Pa 1976) 31(24): 2759-2766.
Kwon, B. K., W. Tetzlaff, et al. (2004). "Pathophysiology and pharmacologic treatment of acute spinal cord injury." Spine J 4(4): 451-464.
LeDoux, J. E. (2002). Synaptic self : how our brains become who we are. New York, Viking.
Lefkowith, J. B., G. S. Geis, et al. (2000). "Safety of celecoxib vs other nonsteroidal anti-inflammatory drugs." JAMA 284(24): 3123-3124.
Manchikanti, L. (2002). "Role of neuraxial steroids in interventional pain management." Pain Physician 5(2): 182-199.
Manchikanti, L., V. Pampati, et al. (2000). "The effect of neuraxial steroids on weight and bone mass density: a prospective evaluation." Pain Physician 3(4): 357-366.
Pappagallo, M. (2005). The neurological basis of pain. New York, McGraw-Hill, Medical Pub. Division.
Scholz, J. and C. J. Woolf (2002). "Can we conquer pain?" Nat Neurosci 5 Suppl: 1062-1067.
Scuderi, G. J., J. M. Cuellar, et al. (2009). "Epidural interferon gamma-immunoreactivity: a biomarker for lumbar nerve root irritation." Spine (Phila Pa 1976) 34(21): 2311-2317.
Silverstein, F. E., G. Faich, et al. (2000). "Gastrointestinal toxicity with celecoxib vs nonsteroidal anti-inflammatory drugs for osteoarthritis and rheumatoid arthritis: the CLASS study: A randomized controlled trial. Celecoxib Long-term Arthritis Safety Study." JAMA 284(10): 1247-1255.
Whelton, A., J. L. Lefkowith, et al. (2006). "Cardiorenal effects of celecoxib as compared with the nonsteroidal anti-inflammatory drugs diclofenac and ibuprofen." Kidney Int 70(8): 1495-1502.