Inflammation and repair rince
70
Inflammation PRESENTED BY DR.RINCE MOHAMMED J.R 1 O.M.F.S,G.D.C KOTTAYAM
-
Upload
rince-mohammed -
Category
Health & Medicine
-
view
130 -
download
0
Transcript of Inflammation and repair rince

Inflammation PRESENTED BY DR.RINCE MOHAMMEDJ.R 1 O.M.F.S,G.D.C KOTTAYAM

Contents
Introduction Definition Cardinal Signs Types of inflammation Acute inflammation – Pathogenesis Chemical mediators of acute inflammation Systemic & laboratory manifestations Exudate Vs Transudate Out comes of Acute Inflammation
Chronic inflammation Chronic inflammatory cells Chronic inflammation types Summary and conclusion References

Introduction
Inflammation is the reaction of living tissue to injury or infection. It is a protective vascular connective tissue reaction or response
intended to remove injurious stimuli as well as the necrotic cells. Repair-causes the replacement of damaged tissues by
regeneration of parenchyma cells or by filling of any residual defect by fibrous scar tissues. (Healing)
jayalakshmi jayakumar
inflammation repair closly related.inflmn-response phase repair healing phase...

Definition
A local response to cellular injury that is marked by capillary dilatation, leukocytic infiltration, redness, heat, and pain and that serves as a mechanism initiating the elimination of noxious agents and of damaged tissues.
(Websters medical dictionary)

Sometimes harmful – hypersensitivity reactions,immune diseses.
Repair also can cause scarring ,fibrosis that may lead to obstruction of movement.
Anti inflammatory drugs - enhance favourable effects of inflammation and controls its harmful sequelae.
The nomenclature used to describe inflammation in different tissues employs the tissue name and the suffix “- itis ” e.g pancreatitis meningitis pericarditis arthritis
jayalakshmi jayakumar
allergy to drugs insect bite,toxins.immune diseases like rhumatoid artritis,

Cardinal Signs (Celsus)
Rubor- redness due to increased blood flow and vasodilation Calor- or heat due to increase blood flow to the periphery Tumor- swelling from inflammatory edema Dolor-pain from swelling and presence of inflammatory
mediators Functio laesa-loss of function due to main and structural
necrosis (Virchow 1793)

:
Types of inflammation
Acute inflammation – immediate and early response to an injurious agent,short duration usually less than 48 hrs PMN as inflammatory cells
Chronic inflammation – longer duration,occurs either after the causative agent of acute inflammation persist for a long time or the stimulus induces chronic inflammation from the beginning Lymhocytes,plasma cells,macrophages –inflammatory cells

Acute inflammation

Stimuli for acute inflammation
Infections (bacterial, viral, fungal, parasitic) and microbial toxins. Tissue necrosis from any cause, including ischemia (as in a
myocardial infarct),trauma, and physical and chemical injury Foreign bodies Dirt, sutures etc Immune reactions (hypersensitivity reactions) are reactions in
which the normally protective immune system damages the individual's own tissues.
jayalakshmi jayakumar
physical injury-thermal injury, as in burns or frostbite; irradiation; exposure to some environmental chemicals). Several molecules released from necrotic cells are known to elicit inflammation

Acute inflammation - Pathogenesis
3 major components:
1. Alteration of vascular flow and caliber (vasodilation leads to
increased blood flow)
2. Increased Vascular Permeability (Vascular Leakage)
3. Emigration of leukocytes from microcirculation (leukocyte activation
leads to elimination of offending agent)
jayalakshmi jayakumar
jayalakshmi jayakumar
1 and 2 vascular changes 3 cellular change

VASCULAR CHANGES
Major role in acute inflammation

Leukocyte Emigration AdhesionTransmigrationChemotaxisPhagocytosis
Termination
Stasis
↑ Vascular permeability
Vasodilation

1.Changes in Vascular Flow and Caliber
Transient constriction of arterioles – immediate vascular response after an injury.
Vasodilation Arterioles are involved, and leads to increased blood flow, which is
the cause of heat and redness at the site of inflammation. Induced by the action of mediators like histamine and nitric oxide,
on vascular smooth muscle.
jayalakshmi jayakumar
events

Increased permeability of the microvasculature leads to exudation of protein rich fluid into the extravascular space causing swelling (tumor).
Stasis of the blood flow -Loss of fluid from the vessels leads to Concentration of red cells resulting in decreased velocity and stasis of the blood flow
Leukocytic margination-Neutrophils, accumulate along the vascular endothelium.At the same time endothelial cells are also activated by mediators produced at sites of injury, and express increased levels of adhesion molecules.

2.Increased Vascular Permeability 15
Hallmark of acute inflammation as it causes escape of protein rich exudate leading to edema.
loss of protein from plasma reduces intravascular osmotic pressure, and increases that of interstitium.
So marked outflow of fluid Edema
jayalakshmi jayakumar
jayalakshmi jayakumar
pathogenesis-3 components.1 vasodilation (Alteration of vascular flow and caliber) 2 Vascular Leakage)3 Emigration of leukocytes

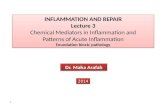
Mechanism of vascular leakage
Contraction of endothelial cells
Resulting in gaps in endothelium. most common mechanism. Elicited by histamine, bradykinin, leukotrienes,and substance P. It is called the immediate transient response because it occurs
rapidly and is short-lived.

Endothelial retraction Structural reorganization of cytoskeleton of endothelial cells Reversibile retraction of intercellular junctions Delayed and prolongedDirect endothelial injury Resulting in endothelial cell necrosis.Eg:Burns,bacterial infections Immediate and sustained reaction.

Leukocyte-dependent endothelial cell injury Marginating leukocytes may damage the endothelium through
activation and release of toxic oxygen radicals and proteolytic enzymes making the vessel leaky.
Transcytosis occurs across cellular channels.

jayalakshmi jayakumar
Shows the difference between normal and inflamed tissues....vasodilation

CELLULAR EVENTS

Leukocyte EmigrationAdhesionTransmigrationChemotaxisPhagocytosis
Termination
Stasis
↑ Vascular permeability
Vasodialtion

3.Emigration of leukocytes
critical function of inflammation is to deliver leukocytes to the site of injury and to activate the leukocytes to eliminate the offending agents.
Leukocytes leave the vasculature routinely through the following sequence of events:
1. Margination, rolling, and adhesion to endothelium
2. Diapedesis (trans-migration across the endothelium)
3. Migration toward a chemotactic stimuli from the source of tissue injury.

Margination and Rolling
With increased vascular permeability, fluid leaves the vessel causing leukocytes to settle-out of the central flow column and “marginate” along the endothelial surface
Endothelial cells and leukocytes have complementary surface adhesion molecules which briefly stick and release causing the leukocyte to roll along the endothelium until it adhire firmly.
Rolling and adhesion are mediated by selectins, integrins, Immunoglobulin superfamily adhesion molecules.
jayalakshmi jayakumar
jayalakshmi jayakumar
There are three types of selectins: one expressed on leukocytes (L-selectin), one on endothelium (E-selectin), and one in platelets and on endothelium (P-selectin).The expression of selectins and their ligands is regulated by cytokines produced in response to infection and injury.

Transmigration (diapedesis)
After adhesion leukocytes insert their pseudopods into endothelial cell junction and squeeze through this layer into the extarvascular space..
It cross basement membrane by damaging it locally with Collagenases

Chemotaxis.
Once they have exited the capillary, the leukocytes move through the tissue guided by secreted cytokines, bacterial and cellular debris, and complement fragments (C3a, C5a),leukotrienes (LTB4).
Most chemotactic agents signal via G-protein-coupled receptors resulting in intracellular Ca2+ release and activation of small GTPases. This leads to actin/myosin polymerization and filopodia formation directed to the chemical agent.
jayalakshmi jayakumar
The process by which leukocytes migrate in response to a chemical signal is called chemotaxis.


Phagocytosis and Degranulation
During the next and final stage of the cellular response, the neutrophils and macrophages engulf and degrade the bacteria and cellular debris in a process called phagocytosis.It involves
Recognition Engulfment Killing (degradation/digestion)

Recognition and Binding The phagocytic cells are recognized by chemotactic factors released
by bacterial products.It is made easier by opsonisation-coating with natural opsonins like C3b, IgG,lectins.
Engulfment After a particle is bound to phagocyte receptors,pseudopods flow
around it, and form a vesicle (phagosome) that encloses the particle.It fuses with lysosome-phagolysosome.

jayalakshmi jayakumar
mpo myeloperoxidase

Killing (degradation/digestion) Triggers an oxidative burst which forms Reactive oxygen species.it
causes Increased oxygen consumption Glycogenolysis Increased glucose oxidation Formation of superoxide ion Killng by halogenation, or lipid/protein peroxidation




Chemical mediators
Cell derived or plasma derived Have “triggering” stimuli Usually have specific targets Can cause a “cascade” Are short lived

Cell Derived
• Histamine• Serotonin• Eicosanoids• Nitric oxide• Platelet activating factor (paf)• Cytokines• Lysosome constituents• Free radicals• Neuropeptides
Plasma Protein Derived
• Complement System• Coagulation & Kinin System• Fibrinolytic system

Histamine Vasoactive “amine” Mast Cells, basophils Vasodilatation, Increase vascular permeability,
Endothelial activation Produced in response to physical injury,immune
reactions, neuropeptides, C3a & C5a, Cytokines

Serotonin
(5HT, 5-Hydroxy-Tryptamine) Platelets and EnteroChromaffin Cells Also vasodilatation, Increase vascular
permeability Released during platelet aggregation

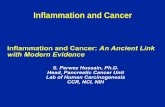
Eicosanoids (arachidonic acid derivatives)
jayalakshmi jayakumar
When cells are activated by stimuli, such as microbial products and various mediators of inflammation, membrane AA is rapidly converted by the actions of enzymes to produce prostaglandins and leukotrienes.Arachidonic Acid (AA) Metabolites: Prostaglandins, Leukotrienes, and Lipoxins
jayalakshmi jayakumar
block leukotriene receptors (e.g. Montelukast) are useful in the treatment of asthma.

Cyclooxygenase pathway PGD2,PGE2,PGF2α
Causes Vasodilation,capillary permeability, and the pain and fever that accompany inflammation.
PGI2(prostacyclin) Produced by prostacyclin synthase in endothelial cell,Vasodilation,
Inhibits Platelet aggregation TxA2
Produced by Thromboxane synthase in platelets,Vasoconstriction & stimulates platelets aggregation
jayalakshmi jayakumar
jayalakshmi jayakumar
nonsteroidal anti-inflammatory drugs (NSAIDs), such as indomethacin. They inhibit both COX-1 and COX-2 and thus inhibit prostaglandin synthesis;

Lipoxygenase PathwayLTB4
Produced by neutrophils & some macrophagesChemotactic agent for neutrophils
LTC4,LTD4 & LTE4 Produced by mast cellsVasoconstriction,bronchospasm
Lipoxins -Endogenous antagonists of Leukotrienes,Vasodilatation Inhibit chemotaxis,

Platelet-Activating Factor (PAF) Produced by WBCs & endothelial cells Activate platelets, induces platelet aggregation, Causes
Vasoconstriction, Bronchoconstriction It contributes to extravascularization of plasma proteins and so, to
edema.

Nitric oxide
Potent vasodilator Produced from the action of nitric oxide synthetase from arginine

Cytokines/chemokines Cytokines are proteins produced mainly by LYMPHOCYTES and
MACROPHAGES. Includes interferon, interleukin, TNF etc. Interferon -Activation of macrophages CHEMOKINES are small proteins which are attractants for PMN.


Plasma protein derived mediators
Complement System Coagulation & Kinin System Fibrinolytic system

Complement System Consists of Plasma proteins Upon activation different complement proteins(C3b) coat/opsonize
microbes for phagocytosis & destruction C3a & C5a cause mast cells to release histamine which inturn
causes Vasodilation thus increasing vascular permeability C5a activates lipoxygenase pathway causing release of more
inflammatory mediators C5a also helps in leukocyte activation, adhesion & chemotaxis

Coagulation SystemHageman factor/Factor12a
A protein synthesized by liver Activated factor12 further activates Kinin System,Clotting
System,Fibrinolytic System,Complement System

Kinin System Ultimately leads to formation of bradykinin Bradykinin causes arteriolar dilation, increases vascular
permeability & broncho constriction,also pain.

Fibrinolytic System Ultimately leads to formation of plasmin Plasmin
converts C3 to C3a Converts factor-12 to factor-12a Breaks down fibrin to fibrin degradation products which
further increases the vascular permeability

Morphological patterns of acute inflammation
Serous (watery) Fibrinous (hemorrhagic, rich in FIBRIN) Suppurative -Produce pus & purulent exudates- neutrophil, necrotic
cells & edema fluid Ulcerative

Systemic manifestations Fever lymphadenitis Myalgia Malaise shock
Laboratory manifestations Leukocytosis Increased ESR Elevated serum acute
phase proteins (C-reactive protein, fibrinogen, etc)
Hypercoagulability
51Acute inflammation

Exudate
Its presence implies an increase in the normal permeability of small blood vessels in an area of injury and, therefore, an inflammatory reaction.
A filtrate of blood plasma. High protein concentration Contains cellular debris & High
specific gravity.
Transudate
It is an ultrafiltrate of plasma, resulting from osmotic or hydrostatic imbalance across the vessel wall without an increase in vascular permeability.
A fluid with low protein content Little or no cellular material &
Low specific gravity.
52


OUT COMES OF INFLAMMATION


Acute Inflammation
Resolution
Chronic Inflammation
Abscess
SinusFistula
Fibrosis/Scar
Ulcer
Injury
FungusVirus
CancersT.B. etc.

CHRONIC INFLAMMATION

Chronic inflammation is the inflammation with prolonged duration usually from weeks to months and sometimes to years in which active inflammation, tissue injury and healing process proceed simultaneously.

Causes
Persisting infection or prolonged exposure to irritants Repeated acute inflamations (otitis, rhinitis) Primary chronic inflammation - low virulence, sterile inflammations
(silicosis),viral infections Autoimmune reactions (rheumatoid arthritis, glomerulonephritis,
multiple sclerosis)

Features:
Infiltration of mono-nuclear cells like lymphocytes, macrophages and plasma cells.
The dominant cellular player in chronic inflammation is the tissue macrophage
Destruction of tissue by inflammatory cells. Proliferation of new vessels leading to repair (angiogenesis &
fibrosis).

Chronic inflammatory cells
1) MACROPHAGES: Formed from monocytes. Activated by cytokines,endotoxins,Extra cellular matrix proteins and
cause tissue destruction, Neovascularisation, fibrosis. In liver _ Kupffer cells Spleen and lymph nodes _ Sinus histocytes Nervous system _ Microglial cells Lungs _ Alveolar macrophages

2) LYMPHOCYTES: Both T- & B-lymphocytes are involved. Activated macrophages release TNF & IL1 and activate lymphocytes
which then produce different antibodies that cause destruction of antigens at the inflammatory site.
3) EOSINOPHILS: Found in parasitic infections and IgE mediated allergic reactions.

4) MAST CELLS: Mast cells are tissue cells which are like basophils in shape. They are present in bone marrow and around blood vessels and do
not enter the blood. They release histamines and amino acid metabolites. They cause
initial vascular changes in acute inflammation and also cause anaphylactic reactions.

Types of chronic inflammation
1) Agranulomatous: Granuloma is not formed, Inflammation is characterized by all features of chronic inflammation.Examples:• Chronic viral infections e.g., Hepatitis• Chronic autoimmune diseases e.g., Rheumatoid arthritis and Ulcerative
colitis• Chronic chemical intoxication e.g., Chronic alcoholic liver disease• Allergic reactions e.g., Bronchial asthma

2) Granulomatous inflammation Characterized by aggregates of activated macrophages that assume
a squamous cell like epitheloid appearance. GRANULOMA is defined as aggregates of macrophages formed due
persistant response of T-lymphocytes to particular antigens. This has a granular cheesy appearance called as caseous necrosis.

Bacterial:Tuberculosis,Leprosy,Syphilis,gumma etcParasitic:Schistosomiasis Fungal:Histoplasma capsulatum,Blastomycosis.
Inorganic metals / Dust:SilicosisForeign bodies:Suture, Vascular graft.Unknown:Sarcodiosis..

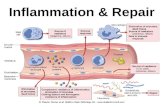
Leukocyte Emigration AdhesionTransmigrationChemotaxis
Phagocytosis
Injurious agent
↑ Vascular permeability
Endothelial contractionRetraction
TranscytosisDirect endothelial injury
Vasodilation
Summary
jayalakshmi jayakumar
jayalakshmi jayakumar
when an injurious agent enters body it triggers inflammatory response.

conclusion
Inflammation is fundamentally a protective response, designed to eliminate the cause of injury (e.g., microbes, toxins) and the consequences of such injury (e.g., necrotic cells and tissues).
Inappropriately triggered or poorly controlled inflammation is the cause of tissue injury in many disorders.

REFERENCES
Robbins and Cotran Pathologic Basis of Disease eighth edition Essential pathology for dental students-Harsh Mohan 3rd
edition

THANK YOU