Inflammation and cancer: a failure of resolution?
4
Inflammation and cancer: a failure of resolution? Toby Lawrence Faculty of Medicine, Imperial College, 1 Aspenlea Road, London W6 8LH, UK There are clear links between chronic inflammation and cancer; strong epidemiological and genetic evidence indicates that inflammation can drive tumour progre- ssion, and more-recent evidence indicates that the dis- ruption of endogenous anti-inflammatory mechanisms in mice can lead to tumour development. The resolution of inflammation is an active coordinated process that requires the production of anti-inflammatory mediators, the termination of proinflammatory signalling pathways and the appropriate clearance or migration of inflamma- tory cells. Disruption of any of these processes can lead to chronic persistent inflammation and tumour growth. Although the mediators and mechanisms that drive inflammation have become increasingly well character- ized, the endogenous mechanisms that limit the inflam- matory response, and particularly their role in cancer, are unclear. There are clear opportunities for drug discovery and the development of new therapeutic approaches that target tumour-associated inflammation and the mechan- isms of chronic inflammation. Inflammation and cancer Inflammation is a salutary response that is normally self-limiting; chronic inflammation can result from the per- sistence of an inflammatory stimulus or the dysregulation of endogenous anti-inflammatory mechanisms [1]. The role of inflammation in the development and progression of cancer is an area of intense scientific interest (for review, see Refs [2–4]); this area is usually considered from the perspective that persistent inflammation in the context of chronic infec- tion or tissue injury might promote cell transformation through DNA damage or that tumour cells produce proin- flammatory factors that drive chronic inflammation and tumour growth [4–6]. The various mechanisms by which inflammation and proinflammatory mediators promote can- cer have been reviewed extensively and are not the subject of this article [6–10]. Here, I present an alternative perspective – that the disruption of endogenous mechanisms that drive the resolution of inflammation could result in chronic inflammation and tumour promotion. The inflammatory response The host response to insult or injury is acute inflammation, classically defined by an initial recruitment of polymorpho- nuclear granulocytes followed by monocytes, which differ- entiate locally into macrophages. This response is often initiated by the activation of resident macrophages through pattern-recognition receptors. This triggers the sequential release of proinflammatory mediators such as eicosanoids, cytokines, chemokines and proteases, which drive leukocyte recruitment and activation [1]. There is enormous capacity for synergy and redundancy within this response but several key mediators have been identified, the inhibition of which can have a profound anti-inflammatory effect. One such mediator seems to be tumour necrosis factor (TNF)-a, which has been established as an important therapeutic target in a range of chronic inflammatory diseases [11] and provides the most conclusive evidence of a link between inflammation and cancer [7,12,13]. Resolution of inflammation Despite its self-amplifying nature, the inflammatory response is self-limiting in normal circumstances. The mediators and signalling mechanisms that initiate and promote the inflammatory response are well characterized but relatively little is known about the factors that mediate resolution and, thereby, prevent chronic inflammation. Recent research has established that the resolution of inflammation is a coordinated process that is dependent on the expression of specific mediators [1,14] (Figure 1); several endogenous anti-inflammatory mediators have been identified, including the cytokines interleukin (IL)- 10 and transforming growth factor (TGF)-b, in addition to lipid mediators such as lipoxins and prostaglandins [1]. Gene disruption studies and pharmacological inhibition have outlined a role for these mediators in the negative regulation of inflammation [1,14]. The resolution of inflam- mation also requires the apoptosis of leukocytes and phagocytic clearance by local macrophages. This process of phagocytic clearance is intimately linked to the down- regulation of macrophage activation and promotes the release of other anti-inflammatory mediators such as TGF-b [15]. Although there is evidence that macrophages can also undergo apoptosis locally during the resolution of inflammation [16], another major clearance mechanism for macrophages is migration through the draining lym- phatics [17], which provides the means for macrophages and other antigen-presenting cells (APCs) to prime T and B cells in local lymph nodes, thereby generating a protective immune response. The resolution of inflammation and cancer The mediators and mechanisms that limit inflammation and innate immunity and that drive the resolution of inflammation have recently been reviewed [1,4,14]. Here, Opinion TRENDS in Pharmacological Sciences Vol.28 No.4 Corresponding author: Lawrence, T. ([email protected]). Available online 28 February 2007. www.sciencedirect.com 0165-6147/$ – see front matter ß 2007 Elsevier Ltd. All rights reserved. doi:10.1016/j.tips.2007.02.003
-
Upload
toby-lawrence -
Category
Documents
-
view
213 -
download
1
Transcript of Inflammation and cancer: a failure of resolution?

Inflammation and cancer: a failure ofresolution?Toby Lawrence
Faculty of Medicine, Imperial College, 1 Aspenlea Road, London W6 8LH, UK
Opinion TRENDS in Pharmacological Sciences Vol.28 No.4
There are clear links between chronic inflammation andcancer; strong epidemiological and genetic evidenceindicates that inflammation can drive tumour progre-ssion, and more-recent evidence indicates that the dis-ruption of endogenous anti-inflammatory mechanisms inmice can lead to tumour development. The resolution ofinflammation is an active coordinated process thatrequires the production of anti-inflammatory mediators,the termination of proinflammatory signalling pathwaysand the appropriate clearance or migration of inflamma-tory cells. Disruption of any of these processes can lead tochronic persistent inflammation and tumour growth.Although the mediators and mechanisms that driveinflammation have become increasingly well character-ized, the endogenous mechanisms that limit the inflam-matory response, and particularly their role in cancer, areunclear. There are clear opportunities for drug discoveryand the development of new therapeutic approaches thattarget tumour-associated inflammation and the mechan-isms of chronic inflammation.
Inflammation and cancerInflammation is a salutary response that is normallyself-limiting; chronic inflammation can result from the per-sistence of an inflammatory stimulus or the dysregulation ofendogenous anti-inflammatory mechanisms [1]. The role ofinflammation in the development and progression of canceris an area of intense scientific interest (for review, see Refs[2–4]); this area is usually considered from the perspectivethat persistent inflammation in the context of chronic infec-tion or tissue injury might promote cell transformationthrough DNA damage or that tumour cells produce proin-flammatory factors that drive chronic inflammation andtumour growth [4–6]. The various mechanisms by whichinflammationandproinflammatorymediators promote can-cerhavebeen reviewedextensivelyandarenot the subject ofthisarticle [6–10].Here, I presentanalternativeperspective– that the disruption of endogenous mechanisms that drivethe resolution of inflammation could result in chronicinflammation and tumour promotion.
The inflammatory responseThe host response to insult or injury is acute inflammation,classically defined by an initial recruitment of polymorpho-nuclear granulocytes followed by monocytes, which differ-entiate locally into macrophages. This response is often
Corresponding author: Lawrence, T. ([email protected]).Available online 28 February 2007.
www.sciencedirect.com 0165-6147/$ – see front matter � 2007 Elsevier Ltd. All rights reserve
initiated by the activation of residentmacrophages throughpattern-recognition receptors. This triggers the sequentialrelease of proinflammatory mediators such as eicosanoids,cytokines, chemokines andproteases, which drive leukocyterecruitment and activation [1]. There is enormous capacityfor synergy and redundancy within this response butseveral key mediators have been identified, the inhibitionof which can have a profound anti-inflammatory effect. Onesuch mediator seems to be tumour necrosis factor (TNF)-a,which has been established as an important therapeutictarget in a range of chronic inflammatory diseases [11] andprovides the most conclusive evidence of a link betweeninflammation and cancer [7,12,13].
Resolution of inflammationDespite its self-amplifying nature, the inflammatoryresponse is self-limiting in normal circumstances. Themediators and signalling mechanisms that initiate andpromote the inflammatory response are well characterizedbut relatively little is known about the factors thatmediateresolution and, thereby, prevent chronic inflammation.Recent research has established that the resolution ofinflammation is a coordinated process that is dependenton the expression of specific mediators [1,14] (Figure 1);several endogenous anti-inflammatory mediators havebeen identified, including the cytokines interleukin (IL)-10 and transforming growth factor (TGF)-b, in addition tolipid mediators such as lipoxins and prostaglandins [1].Gene disruption studies and pharmacological inhibitionhave outlined a role for these mediators in the negativeregulation of inflammation [1,14]. The resolution of inflam-mation also requires the apoptosis of leukocytes andphagocytic clearance by local macrophages. This processof phagocytic clearance is intimately linked to the down-regulation of macrophage activation and promotes therelease of other anti-inflammatory mediators such asTGF-b [15]. Although there is evidence that macrophagescan also undergo apoptosis locally during the resolution ofinflammation [16], anothermajor clearancemechanism formacrophages is migration through the draining lym-phatics [17], which provides the means for macrophagesand other antigen-presenting cells (APCs) to prime T andBcells in local lymph nodes, thereby generating a protectiveimmune response.
The resolution of inflammation and cancerThe mediators and mechanisms that limit inflammationand innate immunity and that drive the resolution ofinflammation have recently been reviewed [1,4,14]. Here,
d. doi:10.1016/j.tips.2007.02.003

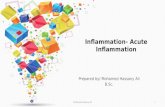
Figure 1. The processes involved in the resolution of inflammation. The resolution
of inflammation is a coordinated process involving: (1) the release of endogenous
anti-inflammatory mediators; (2) the inhibition of proinflammatory signalling
pathways; (3) apoptosis and phagocytic clearance of inflammatory cells, which is
also linked to the inhibition of proinflammatory signalling and the release of anti-
inflammatory mediators; (4) the migration of macrophages and APCs to the
draining lymphatics (this is an important requirement for macrophage clearance
and for promoting adaptive immune responses); and, in the event of infection,
the inflammatory response results in (5) the generation of immunological memory
by priming adaptive immunity.
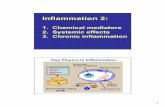
Figure 2. The proinflammatory molecules expressed by inflammatory cells that
can drive tumour progression. The innate immune system can be triggered by
chronic infection or by commensal organisms in the context of tissue injury when
pathogen-associated molecular patterns (PAMPs) activate inflammatory cells,
particularly macrophages; this drives the production of growth factors and
cytokines that can promote tumour growth. Tissue injury and infection can also
lead to the release of endogenous ‘danger signals’ such as the chromatin-
associated protein high-mobility group box (HMGB)1, which triggers macrophage
activation. Abbreviation: MMP, matrix metalloprotease.
Opinion TRENDS in Pharmacological Sciences Vol.28 No.4 163
I discuss how these mechanisms might be involved incancer. It is accepted that tumours are not composed simplyof transformed cells and that as much as 80% of the tumourmass can comprise stromal cells and inflammatory cells thatharbour no genetic lesions [18]. The contribution of theseaccessory cells to tumour development and promotion, theextrinsic pathway, is an extremely active area of research.Adoptive transfer and genetic experiments have shown thatboth stromal cells and bone-marrow-derived leukocytes arerequired for the establishment andmaintenance of tumoursin mice [19–22]. There is convincing evidence that inflam-mation and activation of the innate immune system have arole in the progression of cancer [4] (Figure 2). In particular,tumour-associated macrophages (TAMs) are thought tohave an important role in tumour progression and metas-tasis [3,23,24]. In fact, it has been suggested that TAMinfiltration of tumours is indicative of poor clinical prognosisin certain types of cancer.
Although there is strong evidence that the chronicactivation of innate immunity and inflammation can drivetumour initiation and growth, only a few studies haveaddressed how the deregulation of endogenous anti-inflam-matorymechanismsmight influence cancer.However, somerecent studies suggest that defects in endogenous anti-inflammatory mechanisms that promote the resolution ofinflammation could be an important factor in the pro-gression of cancer, and these are highlighted next.
Endogenous anti-inflammatory mediatorsTGF-b
TGF-b has a well-established tumour suppressor role inepithelial cells, which is frequently inactivated in humancancers [25]. However, TGF-b is also a potent anti-inflam-matory cytokine and is required to dampen both T-cell and
www.sciencedirect.com
macrophage activation. A recent study using tissue-specificinactivation of Smad4 expression, a protein required forTGF-b signalling, shows how TGF-b might act specificallyon T cells to suppress tumour development [26]. Inacti-vation of the Smad4 gene in the T-cell lineage, but not theepithelium, caused the spontaneous development ofgastrointestinal tumours in mice, which indicates thatthe TGF-b-mediated suppression of T-cell-derived cyto-kines inhibits tumour growth in an extrinsic manner.Similar observations were made in a mouse model of coloncancer [27]; T-cell dependence of tumour growth was estab-lished in Rag1�/� mice lacking lymphocytes. The expres-sion of a dominant–negative TGF-b receptor in T cellsto inhibit TGF-b signalling increased tumour growth;however, the transgenic expression of TGF-b in T cellssignificantly delayed the development of tumours. It isunclear why, in the context of these tumour models, T-cellactivation drives tumour growth but studies with Rag1�/�
mice have shown that both T and B cells can promotetumourigenesis [22,28,29]. The lack of appropriate acces-sory signals frommacrophages and other APCs such as IL-12 in the tumour microenvironment might prevent thegeneration of T cells that produce antitumour cytokinessuch as interferon (IFN)-g, instead favouring T cells thatproduce tumour-promoting cytokines.
IL-10
Another important anti-inflammatory cytokine is IL-10.The targeted deletion of the Il10 gene in mice causes spon-taneous inflammatory bowel disease (IBD) and promotesthe development of colorectal cancer [30,31]. Inflammation

164 Opinion TRENDS in Pharmacological Sciences Vol.28 No.4
in this model is driven by the overproduction ofproinflammatory cytokines by intestinal macrophages.Interestingly, tumour development was found to be depen-dent on colonization of the gastrointestinal track withHeli-cobacter hepaticus [32] – a close relative of Helicobacterpylori, which is a major risk factor for gastric cancer inhumans. IL-10 is not thought to have a role in malignanttransformation, and the development of colon carcinomas inIl10�/� mice strongly indicates that the anti-inflammatoryactivity of IL-10 inhibits tumour development in a similarway to TGF-b. Cell-specific targeting of IL-10 and the sig-nalling components of this pathway might provide moreinsight into the specific role of this cytokine in cancer.
TAMs: Dr Jekyll or Mr Hyde?TAMs are thought to have an important role in tumourprogression and metastasis [24,33]. This presents a para-dox because ‘classically activated’ macrophages have directtumouricidal activity and, as APCs, promote antitumourimmune responses. Macrophages are an extremely hetero-geneous cell lineage [34], depending on the anatomicallocation and physiological or pathophysiological contextin which they are studied. In inflammation, monocytesare recruited from the circulation and differentiate intomacrophages at the site of tissue injury or infection; thesemacrophages acquire a distinct phenotype that is dictatedby the nature of the tissue microenvironment and thestimulus. Recent research indicates that TAMs have aspecific phenotype that is distinct from that of residenttissue macrophages and macrophages in inflammatorylesions [23,24,35]. TAMs downregulate antigen-presentingfunctions, and antimicrobial and tumouricidal activity (e.g.reduced expression of MHC class II, IL-12 and induciblenitric oxide synthase, respectively) while increasing theproduction of mediators that promote angiogenesis andtumour growth, such as vascular endothelial growth factor(VEGF) and the cyclooxygenase (COX)-2-derived prosta-glandin E2 (PGE2). It is unclear what drives this TAMphenotype, although the tumour microenvironment andhypoxia are thought to have a major role [23,24,36].
During the resolution of inflammation, specific signalsdownregulate macrophage activation and promote theclearance of activated macrophages, either by apoptosis[16] or by migration through the lymphatic drainage [17].Understanding the signals and mechanisms that drivethese processesmight offer new insights intowhat sustainsTAM recruitment and activation. The phagocytosis ofapoptotic leukocytes through specific receptors is thoughtto provide an important anti-inflammatory signal formacrophages [15,37]; indeed, a recent study has shownthat cyclin-dependent kinase (CDK) inhibitors can specifi-cally promote leukocyte apoptosis and drive the resolutionof inflammation in vivo [38]. The manipulation of theseanti-inflammatory pathways in macrophages could pro-vide a novel approach to treating cancers for which macro-phage recruitment and activation are indicative of poorprognosis.
Concluding remarksThere is strong epidemiological and genetic evidence ofa link among activation of the innate immune system,
www.sciencedirect.com
inflammation and cancer [4]. Much of this evidence is basedon the promotion of cell survival and proliferation by proin-flammatory cytokines. There is further evidence thatspecific cytokines and chemokines promote the invasionand metastasis of tumours. Experiments using animalmodels have clearly established an extrinsic role for cellsof the immune system in tumour promotion. There is enor-mous scope for pharmacological manipulation of theimmune system that could benefit cancer therapy. Thereis already strong evidence that chronic administration ofnonsteroidal anti-inflammatory drugs such as aspirin andselective COX-2 inhibitors can reduce the incidence of can-cer. New biological therapies that target proinflammatorymediators such as TNF-a and IL-6 are currently beingtested in cancer patients, and the outcome of these trialswill be of great interest. The rationale behind the use ofthese inhibitors is to block the tumour-promoting action ofinflammation; however, the chronic inhibition of innateimmunity could have serious implications for cancerpatients, some of whom might be particularly susceptibleto opportunistic infection. Perhaps amore effective strategywould be to target the tumour-specific mediators andmech-anisms that prevent the resolution of inflammation, whichmight leave the innate immune system intact. Recent evi-dence indicates that the anti-inflammatory cytokines IL-10and TGF-b could have an extrinsic tumour suppressoraction [26,27], suggesting that perturbations in thenegativeregulation of immune cells could drive tumour growth. Itwould be of interest to study the role of other endogenousanti-inflammatory mediators in tumour progression. Theproduction of these mediators has an important role inlimiting the inflammatory response but there are severalprocesses required for the resolution of inflammation(Figure 1). It would also be interesting to study the molecu-larmechanisms that limit theactivationofproinflammatorysignalling pathways in the context of inflammation-associ-ated cancer. Furthermore, there could be scope for targetingTAMs; a better understanding of the specific TAM pheno-type could provide opportunities for selectively blockingtumour-promoting activity and, possibly, enhancing theintrinsic antitumour potential of macrophages.
Understanding why and how chronic inflammation ismaintained will provide new insights into chronic inflam-matory disease and will be crucial for understanding therole of inflammation in cancer. This will offer new targetsfor therapeutic intervention that could complement cur-rent strategies to target the intrinsic pathways of trans-formed tumour cells.
References1 Lawrence, T. et al. (2002) Anti-inflammatory lipid mediators and
insights into the resolution of inflammation. Nat. Rev. Immunol. 2,787–795
2 Balkwill, F. and Coussens, L.M. (2004) Cancer: an inflammatory link.Nature 431, 405–406
3 Balkwill, F. et al. (2005) Smoldering and polarized inflammation in theinitiation and promotion of malignant disease. Cancer Cell 7, 211–217
4 Karin, M. et al. (2006) Innate immunity gone awry: linking microbialinfections to chronic inflammation and cancer. Cell 124, 823–835
5 Weitzman, S.A. and Gordon, L.I. (1990) Inflammation and cancer: roleof phagocyte-generated oxidants in carcinogenesis. Blood 76, 655–663
6 Shacter, E. and Weitzman, S.A. (2002) Chronic inflammation andcancer. Oncology 16, 217–226, 229

Opinion TRENDS in Pharmacological Sciences Vol.28 No.4 165
7 Karin, M. and Greten, F.R. (2005) NF-kB: linking inflammation andimmunity to cancer development and progression. Nat. Rev. Immunol.5, 749–759
8 Karin, M. (2005) Inflammation and cancer: the long reach of Ras. Nat.Med. 11, 20–21
9 Mazhar, D. et al. (2005) COX and cancer. QJM 98, 711–71810 Wang, D. and Dubois, R.N. (2006) Prostaglandins and cancer. Gut 55,
115–12211 Feldmann, M. andMaini, R.N. (2003) Lasker Clinical Medical Research
Award. TNFdefined asa therapeutic target for rheumatoidarthritis andother autoimmune diseases. Nat. Med. 9, 1245–1250
12 Arnott, C.H. et al. (2004) Expression of both TNF-a receptor subtypes isessential for optimal skin tumour development. Oncogene 23, 1902–1910
13 Moore, R.J. et al. (1999) Mice deficient in tumor necrosis factor-a areresistant to skin carcinogenesis. Nat. Med. 5, 828–831
14 Gilroy, D.W. et al. (2004) Inflammatory resolution: new opportunitiesfor drug discovery. Nat. Rev. Drug Discov. 3, 401–416
15 Savill, J. et al. (2003) Cell biology. Eat me or die. Science 302, 1516–1517
16 Gilroy, D.W. et al. (2003) Inducible cyclooxygenase-derived 15-deoxyD12-14PGJ2 brings about acute inflammatory resolution in ratpleurisy by inducing neutrophil and macrophage apoptosis. FASEB J.17, 2269–2271
17 Bellingan, G.J. et al. (2002) Adhesionmolecule-dependent mechanismsregulate the rate of macrophage clearance during the resolution ofperitoneal inflammation. J. Exp. Med. 196, 1515–1521
18 Leek, R.D. et al. (1996) Association of macrophage infiltration withangiogenesis and prognosis in invasive breast carcinoma. Cancer Res.56, 4625–4629
19 Orimo, A. et al. (2005) Stromal fibroblasts present in invasive humanbreast carcinomas promote tumor growth and angiogenesis throughelevated SDF-1/CXCL12 secretion. Cell 121, 335–348
20 Lin, E.Y. et al. (2001) Colony-stimulating factor 1 promotes progressionof mammary tumors to malignancy. J. Exp. Med. 193, 727–740
21 Coussens, L.M. et al. (2000) MMP-9 supplied by bone marrow-derived cells contributes to skin carcinogenesis. Cell 103, 481–490
AGORA initiative provides frdeveloping
The Health Internetwork Access to Research Initia
community scheme with the UN Foo
As part of this enterprise, Elsevier has given hun
Research in Agriculture (AGORA). More than 100 i
which aims to provide developing countries with f
help increase crop yields and encou
According to the Africa University in Zimbabwe,
and staff. ‘‘It has brought a wealth of information
information made available goes a long way in
activities within the University. Given the econom
have come at a
For more information, visit
www.sciencedirect.com
22 de Visser, K.E. et al. (2005)De novo carcinogenesis promoted by chronicinflammation is B lymphocyte dependent. Cancer Cell 7, 411–423
23 Mantovani, A. et al. (2002) Macrophage polarization: tumor-associatedmacrophages as a paradigm for polarizedM2mononuclear phagocytes.Trends Immunol. 23, 549–555
24 Pollard, J.W. (2004) Tumour-educated macrophages promote tumourprogression and metastasis. Nat. Rev. Cancer 4, 71–78
25 de Caestecker, M.P. et al. (2000) Role of transforming growth factor-bsignaling in cancer. J. Natl. Cancer Inst. 92, 1388–1402
26 Kim, B.G. et al. (2006) Smad4 signalling in T cells is required forsuppression of gastrointestinal cancer. Nature 441, 1015–1019
27 Becker, C. et al. (2004) TGF-b suppresses tumor progression in coloncancer by inhibition of IL-6 trans-signaling. Immunity 21, 491–501
28 Coussens, L.M. and Werb, Z. (2001) Inflammatory cells and cancer:think different! J. Exp. Med. 193, F23–F26
29 Daniel, D. et al. (2003) Immune enhancement of skin carcinogenesis byCD4+ T cells. J. Exp. Med. 197, 1017–1028
30 Kuhn, R. et al. (1993) Interleukin-10-deficient mice develop chronicenterocolitis. Cell 75, 263–274
31 Berg, D.J. et al. (1996) Enterocolitis and colon cancer in interleukin-10-deficient mice are associated with aberrant cytokine production andCD4+ Th1-like responses. J. Clin. Invest. 98, 1010–1020
32 Erdman, S.E. et al. (2003) CD4+CD25+ regulatory lymphocytes requireinterleukin 10 to interrupt colon carcinogenesis in mice. Cancer Res.63, 6042–6050
33 Condeelis, J. and Pollard, J.W. (2006) Macrophages: obligate partnersfor tumor cell migration, invasion, and metastasis. Cell 124, 263–266
34 Taylor, P.R. and Gordon, S. (2003) Monocyte heterogeneity and innateimmunity. Immunity 19, 2–4
35 Hagemann, T. et al. (2006) Ovarian cancer cells polarize macrophagestoward a tumor-associated phenotype. J. Immunol. 176, 5023–5032
36 Harris, A.L. (2002) Hypoxia – a key regulatory factor in tumour growth.Nat. Rev. Cancer 2, 38–47
37 Savill, J. et al. (1990) Vitronectin receptor-mediated phagocytosis ofcells undergoing apoptosis. Nature 343, 170–173
38 Rossi, A.G. et al. (2006) Cyclin-dependent kinase inhibitors enhancethe resolution of inflammation by promoting inflammatory cellapoptosis. Nat. Med. 12, 1056–1064
ee agriculture journals tocountries
tive (HINARI) of the WHO has launched a new
d and Agriculture Organization.
dreds of journals to Access to Global Online
nstitutions are now registered for the scheme,
ree access to vital research that will ultimately
rage agricultural self-sufficiency.
AGORA has been welcomed by both students
to our fingertips’’, says Vimbai Hungwe. ‘‘The
helping the learning, teaching and research
ic hardships we are going through, it couldn’t
better time.’’
www.aginternetwork.org