Infertility Management in Advanced Age Prof Cihat Ünlü Bakırköy Acıbadem Hospital.
49
Infertility Management in Advanced Age Prof Cihat Ünlü Bakırköy Acıbadem Hospital
-
Upload
sharleen-stone -
Category
Documents
-
view
225 -
download
5
Transcript of Infertility Management in Advanced Age Prof Cihat Ünlü Bakırköy Acıbadem Hospital.
Infertility Management in Advanced Age
Prof Cihat Ünlü
Bakırköy Acıbadem Hospital

Age Related Predictive Factors in Infertility
• Loss of Ovarian Reserve• Oocyte Senescence • Increased sperm DNA Damage• Duration of Infertility• Increase in Other Gynecological
İnfertility Factors– Tuboperitoneal Factors and PIDs– Uterine Fibroids, etc.
Tatone C, Gynecol Endocrinol. 2008Vagnini L et al. Reprod Biomed Online. 2007
Female Partner AgeMale Partner Age

Fecundability and Age of Female Partner
Human Reprod 2004

The Influence of Female Partner Age
Previous Pregnancy with ARTNo Previous Pregnancy Previous Pregnancy without ART
Fertil Steril 2003
Loss of Ovarian Reserve
• Change of Menstruel Cycles• Endocrine and biochemical profile change
D3• FSH• E2• Inhibin
• Decreased Success Rates Due to... • Decreased oocytes nb• Decreased fertilization rates• Decreased ET rates • Decreased cumulative PRs• Increased Abortion• Increased Aneuploidy
Clin Exp Obstet Gynecol. 2004, Minerva Ginecol. 2003
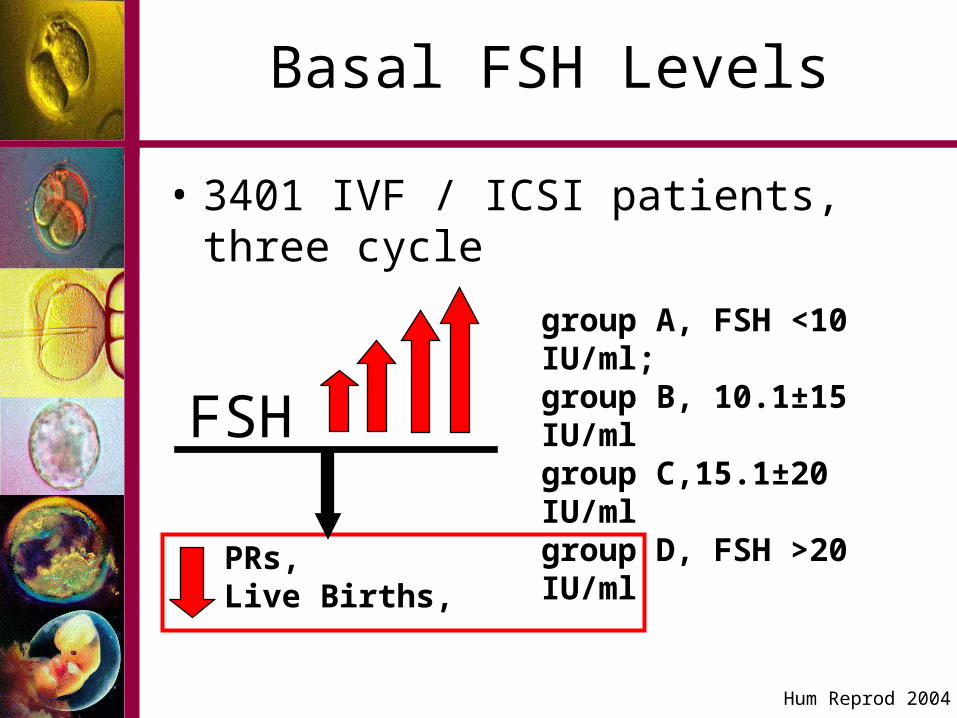
Basal FSH Levels
• 3401 IVF / ICSI patients, three cycle
FSH
Hum Reprod 2004
group A, FSH <10 IU/ml; group B, 10.1±15 IU/ml group C,15.1±20 IU/ml group D, FSH >20 IU/ml
PRs, Live Births,

2
> 38 age
< 38 age
group A, FSH <10 IU/ml; group B, 10.1±15 IU/ml group C,15.1±20 IU/ml
PRs, Live Births, > 38 age
½
Basal FSH and Age
Pregnancy Loss
Hum Reprod 2004

Prediction of Ovarian Response in ART
Sensitivity SpecifityPrognostic Significance
OD (Range, %95 CI)
Age % 73.58 % 55.56 % 72.171.21
(1.05-1.39)
Age+
Basal FSH% 82.80 % 77.27 % 81.74
1.28 (Age; 1.09-1.51,
FSH; 1.42, 1.19-1.70)
Hum Reprod 2000

•Basal FSH, < 12 mIU/ml•Basal E2, < 75 pg/ml•Basal İnhibin > 45 pg/ml•Decrease of Ovarian Volume•Clomiphene Citrate Challenge Test,•GAST •Antral folllicle nb
Prediction of Oocyte Quality Solely by Age
Success in Prediction of
Inducible Oocyte nb
Prediction of Ovarian Reserve
Clin Exp Obstet Gynecol. 2004, Minerva Ginecol. 2003

Duration of Infertility
Fertıl Sterıl 2003
Duration of Infertility as age related factor
Decreased Success !> 3 years

Paternal and Maternal Age
Fertil Steril 2003
Paternal age ≥40 accepted as a key risk factor

The influence of age on sperm DNA damage
508 men in an unselected group of couples attending infertility investigation and treatment. •DNA fragmentation by (TUNEL) assay;( at least 200 spermatozoa) [DNA fragmentation index (DFI)]. Group I: < or =35 years, Group II: 36-39 years,
Group III: > or =40 years. DFI was significantly lower in Group I than in Group II (P = 0.034) or III (P = 0.022). The regression analysis demonstrated a significant increase in sperm DFI with age (P = 0.02).
TUNEL assay clearly demonstrates an increase in TUNEL assay clearly demonstrates an increase in sperm DNA damage with age. sperm DNA damage with age.
Vagnini L et al. Reprod Biomed Online. 2007

DF -DF +
DNA hasarlarının (DF) akridin orange ile gösterilmesi
0
10
20
30
40
50
60
A CEmbriyo kalitesi
<%56 DF+
p<0.05
Ünlü C, Aydos K. 2006

DNA hasarı Normal morfoloji
<%56 %60
>%56 %21
0
10
20
30
40
50
60
70
80
<%56 >%56
DNA hasarlı spermatozoa
% Fertilizasyon
Ünlü C, Aydos K. 2006

Practical Management of
Infertility in Advanced Age

Aims of Management in Infertility
1. Detection of Infertility Factors
2. Consideration of the Advantages / Disadvantages of the treatment choices
3. The Counseling of Infertile Couple
4. Planning the Treatment
5. Performing Treatment choices with optimum time intervals

Ethical and Medical Problems in Advanced Aged Couples
1. What are the age limits for couples (Female and Male Limits)?
2. Do insurance policies resisting for special age limits in treatment of infertility against the human reproduction rights?
3. Do couples have rights in selecting the treatment method in advanced age?
4. No luxury for time loss according to wrong treatment option.
5. Decreased Ovarian Response6. Decreased ART success and increased drop outs.7. Increased treatment anxiety (Doctor and Patient)8. Should the optimum treatment numbers regaring the
methods be different in advanced age?

Infertility Treatment Choicesin Advanced Age
• Ovulation Induction
• Sperm Insemination Techniques
– IUI
– ICI
– FSP
• IVF / ICSI
• Advanced Treatment Options

Treatment Choices in OIin Advanced Age
• Short GnRH analog protocols
• Flare-up Protocols• Mikrodose GnRH
protocols• GnRH antagonist
protocols• Minimal stimülation
protocols• GnRH Analog
Cessations
• Addition of Cortisol• Addition of CC• Addition of
Aromatase inh.• Addition of low dose
aspirine• Addition of Growth
hormone• Natural cycle

Efficacy of IUI in Advanced Age
IUI with OI has virtually no place in their treatment.Dovey S Fertil Steril 2008
Age Cycle Patient PRs ITT
< 35 2351 983 11.5 10.1
35-37 947 422 9.2 8.2
38-40 614 265 7.3 6.5
41-42 166 81 4.3 3.6
> 42 120 55 1 0.8
4,199 cycles performed in 1,738 infertility patients

IVF/ ICSI and Advanced Age
Cumulative PRs Rate of Abortion• IVF-ET
> 38 16% 21% < 38 28% 13%
• ICSI> 38 9% 26%
< 38 27% 14%
Poor-responders
Clin Exp Obstet Gynecol. 2004, Reprod Biomed Online. 2003
PRs≤ 34 yaş 19.5%≥ 35- < 39 7.2% ≥ 40 yaş 1.5%
Normo-responders

Indications of IVF
• Tubal Infertility
• Tuboperitoneal Factor
• Endometriosis
• Unexplained Infertility
• Male Factor
• Immunological Infertility
• Recurrent IUI Failure
• Preimplantation Genetic Diagnose(PGD)

Tubal Infertility
Mild
ModerateDistal Tubal Obst
Proximal Tubal Obst.
Age > 35
Poor Ovarian Reserve
Infertilite duration > 3 years
Additional Factor
Insurance ??
Hydrosalpinx +
ReconstructiveSurgery
ReconstructiveSurgery
IVF / ET 4-6 cyclesOI + IUI
Curr Opin Obstet Gynecol, 2004
6-12 monthsObservation
4-6 cyclesOI + IUI
6-12 monthsObservation
IVF / ET cost effective 4 cycles PR % 70

Unexplained Infertility???
Randolph 2000, Godon & Sperof 2002, Guzick et al 1998
0
5
10
15
20
25
PRs
/ cyc
le
•Fecundity rate % 1.3 !•Spontaneus Pregnancy ?????
Spontaneus Pregnancy
(Timed İntercourse)3 years 30-60% 5 years 50-80%
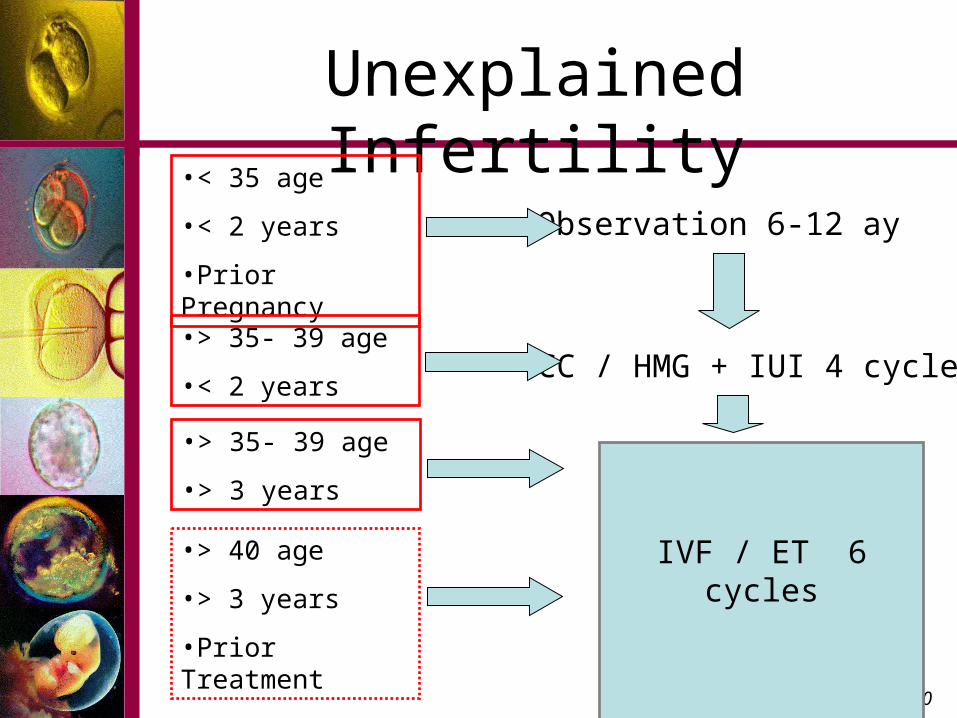
Unexplained Infertility
•< 35 age
•< 2 years
•Prior Pregnancy
Observation 6-12 ay
•> 35- 39 age
•< 2 years
Guzick 1998, Soules, 2000
CC / HMG + IUI 4 cycles
IVF / ET 6 cycles•> 40 age
•> 3 years
•Prior Treatment
•> 35- 39 age
•> 3 years

Influence of Age in Endometriosis

Stage of Endometriosis

Management in Endometriosis
Mild / Moderate (Stage I / II) Moderate / Severe (Stage III / IV)
Age < 38Duration of Infertility < 8 yearsNormal Ovarian Reserve Diagnose > 5 years
6 Months Expectant (% 50)
4-6 cycles OI + IUI
Age >38Duration of
Infertility > 8 yearsAdditional Factor
Poor Ovarian Reserve
Diagnose > 5 years
IVF / ET IVF / ETIVF / ET
Impossible Tubo-ovarianRestoration
Normal tubo-ovarian
restoration
Suboptimal resection
Fertil Steril 2002
Am J Obstet Gynecol 2003

Male Infertility
TMS > 5 x mil TMS 1.5 - 5 x mil TMS < 1.5 x mil
Male Age < 40 ?Female Age < 35Infertility duration < 2 yearsNo Additional Factor
İUİ 3-4 x
Normal Morphology
> 14
5-14 < 4
Male Age > 40 ? Female Age > 35Infertility duration > 3 yearsAdditional Factor
IVF4-6 x ICSI 4-6 xOehninger, Ombelet Reprod Bio Med 2003

Male Infertility
TESE PESAMESA
Ejaculatuar canal obs.Vas deferens obs.
Intratesticular obst.Epididymal obst.
CongenitalAquired
MIBPPC, Fertil Steril 2002
TURED
Microsurgery
Additional Factor+ Epididymal obst.Female Age > 35Duration of Infertility > 15 yearsDifficulties in surgery
Inflamation

Further Treatment Options
• Preimplantation Genetic Diagnose• Assisted Embryo Hatching• Enriched Culture Media• Co-Culture Methods (ECC, etc)• Blastocyst Transfer• Cytoplasmic Transfer• Nuclear Transfer• Oocyte Donation• Oocyte Sharing• Sperm Donation

Preimplantation Genetic Diagnose
• Maternal Age (> 35)• Recurrent IVF Failure (>3)• Recurrent Pregnancy Loss• Unexplained Infertility • Severe Male Infertility• Y Chromosome Deletions• Translocation Carriers• Abnormal Embryo Morphology

Advanced Age and PGD ?
Maternal Age Trizomi 21 Trizomi 18 Trizomi 13
15 - 19 1:1250 1:17000 1:33000
20 - 24 1:1400 1:14000 1:25000
25 - 29 1:1100 1:11000 1:20000
30 - 34 1:700 1:7100 1:14000
35 - 39 1:200 1:2400 1:4800
40 - 44 1:60 1:700 1:1600
•Mendelien Disease Screening
•Increase implantation rates %15.6 % 26.6
•Increase pregnancy rates
•Decrease abortion rates % 14 % 4.3
J Ass Reprod Genet 1998Human Reprod 1999

Preimplantation Genetic Diagnose
Aneuploidy• Chromosomal abnormality• Chromosomal 13, 14, 15,
16, 17, 18, 21, 22, X and Y • Down sendrom • Turner sendrom • Kleinfelter sendrom
Structural Abnormality• Translocation• Invertion• Deletion• Duplication
Y Chromosome deletionsUniparental Disomi (UDP)
• Genomic Imprinting
Mono Genetic Disease
• X linked • Frajil — X • Duchenne/Becker
muscular distrophy• Hemofili • Otosomal dominant• Myotonic distrophy• Huntington disease• Charcot-Marie-Tooth • Otosomal Resessive• Cystic Fibrosis • Talasemi • Spinal muscular atrophy
Oocyte Donations
35.• Premature ovarian failure, • Gonadal disgenesis (Turner send., etc), • Bilateral Ooforectomy, • Iatrogenic Ovarian Failure (Chemotherapy or
Radiotherapy) • IVF failures with risk of genetic disorders
Indıcations:
RCOG Guideline, 2001

Oocyte Donation Success
Human Reprod 1999

Oocyte Donation Success
Recipient Age and Clinical PRs, Live Births
Fertil Steril 2001
Oocyte Donation and Embryo Quality

Oocyte Donation Success
Endometrial Thickness and Clinical PRs, Live Births
Fertil Steril 2001
Endometrial Pattern and Clinical PRs, Live Births

Co-culture
One factor that may contribute to the poor success rates in ART is the current in-vitro culture conditions !!!!
Only 20-50% of preembryos to the blastocyst stage.
Aim is to transfer
Activation of Maternally derivedgenetic information
Co-culture with somatic cellsGrowth factor media
Co-culture
• Co-culture cell lines used in human IVF express a number of growth factors.
• Growth rates and morphology have been significantly improved for preembryos maintained in co-culture systems.
• Preembryo development on somatic cell lines may enhance implantation and pregnancy rates in human IVF.
• It appears that the autocrine and paracrine interactions between the preembryo and its culture environment takes place.
Wiemer KE et al. Hum Reprod 1993,Barmat LI et al. Fertil Steril 1997,Magli MC et al. Int J Fertil 1995,Morgan K et al. Hum Reprod 1995,

Mechanism of the Effects of Co-culture
• Detoxify the culture medium.
• Produce embryotrophic factors. • GM-CSF, • IL-1,• LIF.
Jacobs AL, Endocrinology 1993,De Los Santos MJ et al. Biol Reprod 1996,Spandorfer SD et al. Am J Reprod Immunol 1998,Spandorfer SD, ASRM Annual Meeting, 1999, Spandorfer SD, et al. Am J Reprod Immunol 2000,

Coculture Results
Jayot S et al. Fertil Steril 1995.Nieto FS et al. J Assist Reprod Genet 1996,Barmat et al. J Ass Reprod Genet, 1999Barmat et al. Fertil Steril 1998,Spandorfer et al. J Ass Reprod Genet, 2002
•Improvement in preembryo grade, •Increase in the average number of blastomeres, •Decrease in the average percentage of fragments per preembryo •Improvement in implantation and pregnancy rates

Co-culture
• Bovine reproductive tract cells, • African green monkey kidney cells (Vero),• Human oviduct cells, • Human granulosa cells lines,• Human Tubal Epithelial cell lines,• Human Endometrial cell lines.Human Endometrial cell lines.
Menezo Y. et al Biol Reprod 1990,Bongso A et al. Fertil Steril 1992,Wiemer KE et al. Hum Reprod 1993,Sakkas D et al. Fertil Steril 1994,Quinn P et al. J Assist Reprod Genet 1996,Barmat et al. J Ass Reprod Genet, 1999Barmat et al. Fertil Steril 1998,Spandorfer et al. J Ass Reprod Genet, 2002

Somatic Cell CocultureSomatic Cell Coculture
• Xenologous• Heterologous• Autologous
Risk of disease transmission to the exposed preembryos !
Autologous human endometrial cells coculture
Jayot S et al. Fertil Steril 1995 Nieto FS et al. J Assist Reprod Genet 1996,

Endometrial Cell Coculture Results

Time of Endometrial Biopsy (<5 versus >5 days from LH surge)

Endometrial Cell Coculture
Endometrial Cell Coculture
Autologous endometrial coculture in patients with
IVF failure: outcome of the first 1,030 cases. • Significant improvement in embryo quality with
ECC. • Patients with a poor prognosis secondary to prior
IVF failures can have a good outcome when utilizing AECC
• Improved implantation and pregnancy rates with AECC.
J Reprod Med. 2004

Thank You