
Infective endocarditis(IE) a brief insight- by Rxvichu!!!
65
Presented by, Vishnu.R.Nair, 5 th year Pharm.D, National College of Pharmacy(NCP).
-
Upload
rxvichu -
Category
Health & Medicine
-
view
103 -
download
2
Transcript of Infective endocarditis(IE) a brief insight- by Rxvichu!!!
Presented by,
Vishnu.R.Nair,
5th year Pharm.D,
National College of Pharmacy(NCP).

WELCOME TO A DETAILED VERSION OF INFECTIVE ENDOCARDITIS!! HAPPY
READING!!

1. DEFINITIONS
2. EPIDEMIOLOGICAL STATISTICS
3. ETIOLOGY
4. PATHOPHYSIOLOGY
5. CLINICAL PRESENTATION
6. DIAGNOSTIC PARAMETERS(SUMMARIZED)
7. MANAGEMENT OF IE
8. BIBLIOGRAPHY/REFERENCE.

Acute bacterial endocarditis caused by Staphylococcus aureus with perforation
of the aortic valve and aortic valve vegetations. Courtesy of Janet Jones, MD,
Laboratory Service, Wichita Veterans Administration Medical Center.

Acute bacterial endocarditis caused by Staphylococcus aureus with aortic
valve ring abscess extending into myocardium. Courtesy of Janet Jones, MD,
Laboratory Service, Wichita Veterans Administration Medical Center.
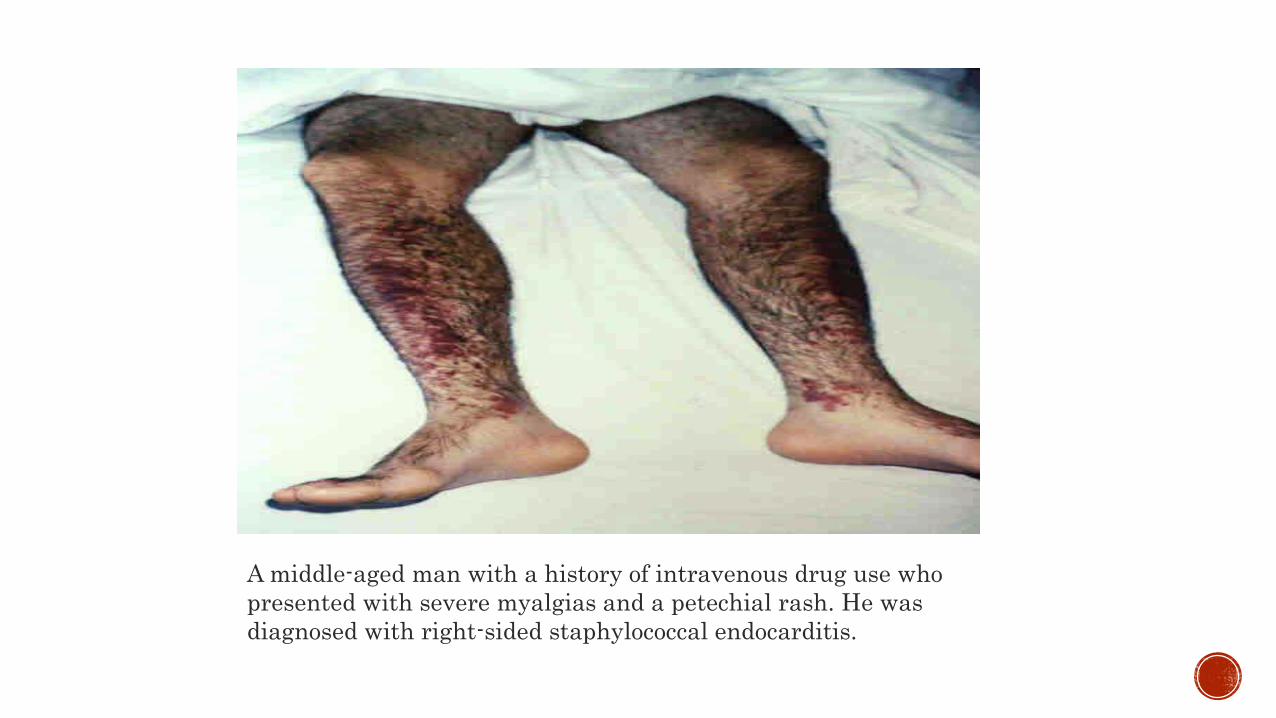
A middle-aged man with a history of intravenous drug use who
presented with severe myalgias and a petechial rash. He was
diagnosed with right-sided staphylococcal endocarditis.

This is a magnified portion of a parasternal long axis view from a
transthoracic echocardiogram. There is a small curvilinear vegetation on the
mitral valve as indicated. The patient presented with a headache and fever,
and CT scan of the brain revealed an occipital hemorrhage. The patient had a
history of intravenous drug use and multiple blood cultures grew
Staphylococcus aureus.

A young adult with a history of intravenous drug use,
endocarditis involving the tricuspid valve with
Staphylococcus aureus, and multiple septic pulmonary
emboli. Pulmonary lesions on chest radiograph are most
prominent in the right upper lobe with both solid and
cavitary appearance.

Mitral valve: endocarditis with valve destruction and vegetation. Note the
posterior leaflet of the mitral valve, with an irregular vegetation on the atrial
surface, resulting in valve destruction at the commissure between the
anterior leaflet and the posterior leaflet.
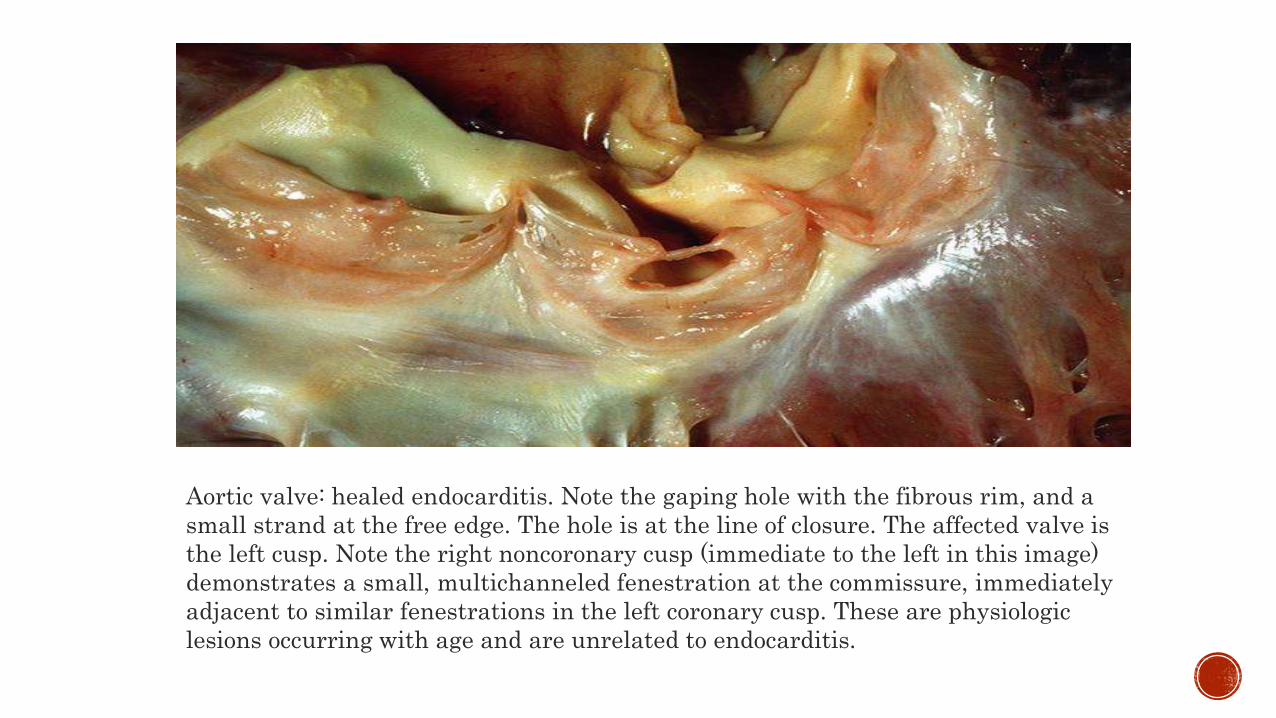
Aortic valve: healed endocarditis. Note the gaping hole with the fibrous rim, and a
small strand at the free edge. The hole is at the line of closure. The affected valve is
the left cusp. Note the right noncoronary cusp (immediate to the left in this image)
demonstrates a small, multichanneled fenestration at the commissure, immediately
adjacent to similar fenestrations in the left coronary cusp. These are physiologic
lesions occurring with age and are unrelated to endocarditis.

Aortic valve: bicuspid, with infectious endocarditis. In this excised valve, note the bulky
vegetations on the ventricular surfaces, with distortion of the valve surfaces.

Mitral valve: postrheumatic, with infectious endocarditis. A defect is seen in the
scarred valve, with focal surface hemorrhage. The patient also underwent aortic valve
replacement, as there was contiguous infection.

IE, surface of valve leaflet, with fibrin. A chronic infiltrate is seen, under the denuded
thrombosed surface, with primarily macrophages, and focal macrophage giant cells.

ENDOCARDITIS: “Inflammation of endocardium(membrane, lining the chambers of the heart, and covering cusps of heart valves)”
INFECTIVE ENDOCARDITIS: “Infection of heart valves by microbes”.

Annual incidence worldwide : 2-15 cases/1,00,000 people per year
Male to female ratio : 2:1
Less common in children
Conditions, associated with high IE incidence include:
- Long term HD(Hemodialysis)
- Diabetes mellitus
- Poor dental hygiene.

Depends on types involved:
1. Native Valve Endocarditis(NVE)
2. Prosthetic Valve Endocarditis(PVE)
3. IVDA(Intravenous drug abuse) Infective Endocarditis
4. Nosocomial IE

1. NATIVE VALVE ENDOCARDITIS(NVE):- Caused by:
a. Rheumatic valvular disease
b. CHF
c. Mitral valve prolapse
d. Marfan Syndrome(Genetic disorder of connective tissue)
- Organisms involved include:
a. S.viridans
b. S. bovis
c. Staphylococcus
d. Enterococci.

2. PROSTHETIC VALVE ENDOCARDITIS(PVE):- Organisms involved include:
a. S.aureus
b. S.epidermidis
c. Corynebacterium
d. Fungi(Aspergillus, C.albicans)
3. IVDA INFECTIVE ENDOCARDITIS:- Organisms involved include:
a. MRSA
b. P. aeruginosa
c. Streptococci
d. Enterococci.

4. NOSOCOMIAL IE:- Occurs due to:
a. Catheters
b. Pacemakers
c. Defibrillators
d. HD shunts.
- Organisms involved include:
a. S.aureus
b. Enterococci
c. Streptococci.

Damaged valves & endocardium causes IE
Damaged part of heart valve forms local blood clot(non-bacterial thrombotic IE) Platelet & fibrin deposits(as part of blood clotting process) allows bacteria to form vegetations
Body has no direct methods to combat valvular vegetations(since valves DO NOT HAVE A DEDICATED BLOOD SUPPLY)
Combination of damaged heart valves + bacterial growth + lack of strong immune response causes IE.

A. SIGNS:
- Fever
- Heart murmur
- Presence/ absence of embolic phenomenon, splenomegaly / skin manifestations.
B. SYMPTOMS:
- Fever
- Chills
- Weakness
- Weight loss
- Malaise
- Night sweats.

Include:
a. Artificial heart valves
b. Congenital heart defects
c. History of endocarditis
d. Damaged heart valves
e. IVDA History.

A. ARTIFICIAL HEART VALVES:
- Germs more likely to get attached to get attached to an artificial(prosthetic) heart valve, than to a normal one
B. CONGENITAL HEART DEFECTS:
- Children, born with heart defects have high risk of getting this disease
C. HISTORY OF ENDOCARDITIS:
- Endocarditis episode damages heart tissue & valves increases risk for future IE
D. DAMAGED HEART VALVES :
- Rheumatic fever/ infections damages/ scars 1/more of heart valves increases risk of future infections
E. IVDA HISTORY:
- Needles used to inject drugs maybe contaminated with bacteriae IE risk.

Include:
a. Stroke & organ damage
b. Infections in other parts of body
c. Heart failure

A. STROKE & ORGAN DAMAGE:
- In IE bacterial vegetations form in heart at infection site
- Breaking loose of these clumps of vegetations travelling of the same to brain, abdominal organs, kidneys / extremities leads to stroke/ damage to other organs/ tissues.
B. INFECTIONS IN OTHER PARTS OF BODY:
- Endocarditis leads to development of pockets of pus(abscesses) in brain, kidneys, spleen/liver
- Abscess can develop in heart muscle itself leads to abnormal heartbeats.
C. HEART FAILURE:
- IE, if left untreated endocarditis can damage heart valves causes permanent destruction of heart’s inner lining causes heart to work harder to pump blood can lead to HF.

Include:
a. Hematological tests
b. Transesophageal echocardiogram
c. ECG
d. Chest X-ray
e. CT-Scan/ MRI

A. HEMATOLOGICAL TESTS:- Blood culture helps to identify bacteria in bloodstream
- Blood tests helps physician to identify certain conditions(anemia), that can be a sign of endocarditis
B. TRANSESOPHAGEAL ECHOCARDIOGRAM:- Echocardiogram uses sound waves produces images of heart at work
helps physician to have a closer look at heart valves
- Often used to check signs of infection
- In this test an ultrasound device passed through mouth, & into esophagus.
C. ECG:- May be applicable, if physician feels that endocarditis may be causing an
irregular heartbeat
- In ECG Sensors (electrodes), that can detect heart’s electrical activity attached to chest(& limbs, optional) measures timing & duration of each electrical phase in heartbeat.

D. CHEST X-RAY:
- X-ray images helps doctor to see condition of lungs & heart
- X-ray images helps physician to see, if endocarditis has caused heart enlargement/ if infection has spread to lungs
E. CT-SCAN/MRI:
- Mainly used to check if infection has spread to brain, chest/ other parts of body.

Includes:
A. Guidelines summary
B. Goals of therapy
C. Medication summary
D. Pharmacological therapy
E. Non-pharmacotherapy
F. Prevention of IE

The AMERICAN HEART ASSOCIATION(AHA) issued guidelines for IE treatment in adults in 2015.
The salient features of the guidelines are summarized in the following sub-headings:
a. Definition
b. Blood culture principles
c. Echocardiography
d. Surgical intervention
e. Antimicrobial therapy
f. Anticoagulation principles
g. CNS imaging principles.

A. DEFINITION:
- IE is defined, based on MODIFIED DUKE CRITERIA
- Includes pathologic & clinical criteriae
- Diagnosis is differentiated as DEFINITE, POSSIBLE or REJECTED IE
B. BLOOD CULTURE PRINCIPLES:
- Blood cultures should be collected, at least THREE TIMES from different venipuncture sites
- The 1st & 2nd collections should be taken AT LEAST 1 HOUR APART.
C. ECHOCARDIOGRAPHY:
- Transthoracic echocardiography(TTE) should be performed as quickly as possible, in all cases of suspected IE
- If TTE images are negative, in spite of persistent suspicion for IE Transesophageal echocardiography(TEE) should be performed.

D. SURGICAL INTERVENTION:
- Indications for surgical intervention include:
a. Persistent vegetation, following systemic embolization
b. 1/ more embolic events, during 1st 14 days of antimicrobial therapy
c. Growing vegetation, in spite of appropriate antimicrobial therapy
d. Acute mitral/ aortic regurgitation, with signs of heart failure
e. Heart failure, that does not respond to medical therapy
f. New heart block
g. Large abscess/extension of abscess, despite appropriate antimicrobial therapy.

E. ANTIMICROBIAL THERAPY:
- Indications include:
a. Native valve IE, caused by Viridans group Streptococci(VGS)
b. VGS/ S. bovis infection of prosthetic material
c. Staphylococcal infection
d. Staphylococcal infection of prosthetic material
e. Enterococcal infection
f. Infection with HAECK micro-organisms**
g. Fungal infection
** HAECK microbes refer to :
1. Haemophilus aphrophilus 4. Eikenella corrodens
2. Actinobacillus actinomycetemcomitans 5. Kingella kingae
3. Cardiobacterium hominis

F. ANTICOAGULATION PRINCIPLES:
- It is reasonable to discontinue all forms of anticoagulation, for 2 weeks, in patients, with :
1. A mechanical valve
2. Patients with IE, in whom a CNS embolic event has occurred
- Established antiplatelet therapy may be continued in patients with IE, who are cleared of all bleeding complications.
G. CNS IMAGING:
- CNS imaging should be performed to evaluate for CNS bleeding/ intracranial mycotic aneurysm, in the following conditions of IE patients:
a. Neurological deficits
b. Severe localized headache
c. Meningeal signs.
1. To relieve signs and symptoms of disease
2. Reduce morbidity & mortality associated with the condition
3. Prevent progression into complications
4. To eradicate the causative organism, with minimal drug exposure
5. To provide rational antimicrobial therapy
6. To prevent IE in high-risk patients, with appropriate prophylactic antimicrobials
7. To improve HRQoL.

Antibiotics are the mainstay of treatment for IE
Goals to maximize treatment success include:
a. Early diagnosis
b. Accurate micro-organism identification
c. Reliable susceptibility testing
d. Prolonged IV administration of bactericidal antimicrobial agents
e. Proper monitoring of potentially toxic antimicrobial agents
f. Aggressive surgical management of correctable mechanical complications.
• Empiric antimicrobial therapy must be comprehensive, and should cover all likely pathogens in the context of the clinical setting.

Includes:
1. MANAGEMENT OF STREPTOCOCCAL ENDOCARDITIS
2. MANAGEMENT OF STAPHYLOCOCCAL ENDOCARDITIS
3. MANAGEMENT OF ENTEROCOCCAL ENDOCARDITIS
4. DRUG DOSING FOR TREATMENT OF IE
5. TREATMENT OF NVE, CAUSED BY S.VIRIDANS, S.BOVIS & STAPHYLOCOCCI(DRUGS OF CHOICE)
6. TREATMENT OF PVE, CAUSED BY S.VIRIDANS, S.BOVIS & STAPHYLOCOCCI(DRUGS OF CHOICE)
7. TREATMENT OF NVE & PVE, CAUSED BY ENTEROCOCCI(DRUGS OF CHOICE)
8. ISSUES, WITH DRUGS USED IN IE.
Streptococci(especially S.viridans) constitutes the most common cause of IE
Most viridans streptococci highly sensitive to Penicillin G
For uncomplicated Native Valve IE usually the following therapy is recommended:
a. High-dose PENICILLIN G/CEFTRIAXONE (for 4 weeks)
b. (PENICILLIN G/ CEFTRIAXONE) + GENTAMICIN (for 2 weeks)
• 2-week treatment regimens are applicable for the following patients:
a. Absence of cardiovascular risk factors(like HF, aortic insufficiency, etc)
b. No evidence of VTE
c. Isolate is PENICILLIN-SENSITIVE
d. Presence of Native Valve infection
e. Clinical response is evident within 7 days.

2-week treatment regimen is NOT RECOMMENDED FOR THE FOLLOWING PATIENTS:
a. Patients >65 yrs of age
b. Patients, with impairment of 8th cranial nerve function
c. Renal dysfunction(CrCl < 20 ml/min)
d. Patients, with known cardiac/ extracardiac abscess
e. Infection with ABIOTROPHIA, GRANULICATELLA/ GEMALLA SPECIES
• VANCOMYCIN is recommended in patients, who can’t tolerate PENICILLIN/ CEFTRIAXONE
• Avoid co-administration of GENTAMICIN when VANCOMYCIN is given
• 6-week treatment regimen may be considered for the following patients:
a. Prosthetic valve endocarditis
b. Prosthetic material, caused by S.viridans and S.bovis.

Mainly caused by S. epidermidis
S. aureus induced IE has become common, owing to the following reasons:
a. Increased i.v drug abuse
b. Frequent use of peripheral and central venous catheters
c. Valve replacement surgery
• For LEFT-SIDED IE, caused by MRSA Focus on 6 week-course of NAFCILLIN/OXACILLIN + A short course of GENTAMICIN
• For patients with documented hypersensitivity to PENICILLINS Give 1st
generation cephalosporins, unless there is no history of immediate-type hypersensitivity reactions

VANCOMYCIN is the drug of choice for patients, with :
a. MRSA infection
b. Known hypersensitivity to PENICILLIN
• VANCOMYCIN is not much effective in MSSA, since the drug kills S.aureusslowly
• Patients, who are penicillin-allergic, and fail to respond to vancomycin therapyDAPTOMYCIN is recommended (at a dose of 6 mg/kg/day)
• DAPTOMYCIN was approved by US-FDA in 2006, for the treatment of RIGHT-SIDED NVE.

TREATMENT OF STAPHYLOCOCCUS ENDOCARDITIS IN I.V DRUG ABUSERS:- Frequently caused by S.aureus(60-70%)
- Treatment for MSSA includes 4-week therapy of a PENICILLINASE-RESISTANT PENICILLIN
- Alternative: 2-week course of NAFCILLIN/OXACILLIN + an AMINOGLYCOSIDE.
TREATMENT OF STAPHYLOCOCCAL PVE:- Since there is high risk of morbidity & mortality associated with this condition,
and refractoriness to therapy antimicrobial combinations are recommended.
- For MRSA & Coagulase-negative staphylococci VANCOMYCIN + RIFAMPIN(for 6 weeks)
- AMINOGLYCOSIDE may be added for first 2 weeks , if the organism is susceptible
- For MSSA Focus on PENICILLINASE-RESISTANT PENICILLIN, instead of VANCOMYCIN
- If causative organism is other than that of staphylococci focus on other treatment regimens, for a period of 6 weeks.

Enterococci constitute 5-18% of IE cases
Such infections are significant, due to the following reasons:
a. No single antibiotic is bactericidal
b. Enterococci are usually resistant to all cephalosporins, and, to some extent, aminoglycosides
c. Demands combination of cell-wall active agent (PENICILLIN/VANCOMYCIN) + AMINOGLYCOSIDE, for killing of organism
d. Increased rates of resistance to all available drugs.
• Enterococcal endocarditis requires 4-6 weeks of HIGH-DOSE PENICILLIN G/ AMPICILLIN + GENTAMICIN, for cure
• 6-week course is recommended for patients, with:
a. Symptoms, lasting longer than 3 months
b. PVE
If the patient is resistant to AMINOGLYCOSIDES/ Enterococci is beta-lactamase producing(Enterococcus faecium) use VANCOMYCIN/ AMPICILLIN-SULBACTAM + GENTAMICIN.

DRUG ADULT DOSE PEDIATRIC DOSE
AMPICILLIN-
SULBACTAM
2 g, i.v, every 4 hours 50 mg/kg every 4 hrs/ 75
mg/kg every 6 hrs
AQ. CRYSTALLINE
PENICILLIN G SODIUM 3 million units, i.v, every
4/6 hrs
50,000 units/kg, i.v, every
6 hrs
CEFAZOLIN 2 g, i.v, every 8 hours 33 mg/kg, i.v, every 8 hrs
CEFEPIME 2 g, i.v, every 8 hours 50 mg/kg, i.v, every 8 hrs
CEFTRIAXONE 2 g, i.v/i.m , every 24 hours 100 mg/kg, i.v/i.m, every 24
hours
CIPROFLOXACIN 400 mg, i.v, every 12
hours/ 500 mg PO, every
12 hours
Avoid use, if possible,
below 18 yrs of age
DOXYCYCLINE 100 mg, i.v/PO, every 12 hrs 1-2 mg/kg i.v/PO,every 12 hrs

DAPTOMYCIN 6 mg/kg, i.v, every 24 hours Not applicable for pediatrics
GENTAMICIN SULFATE 1 mg/kg, i.v/i.m, every 8 hours 1 mg/kg, i.v/i.m, every 8 hours
IMIPENEM-CILASTATIN 500 mg , i.v, every 6 hours 15-25 mg/kg, i.v, every 6 hours
LINEZOLID 600 mg, i.v/PO, every 12 hours 10 mg/kg, i.v, every 8 hours
NAFCILLIN/OXACILLIN 2 g, i.v, every 4 hours 50 mg/kg, i.v, every 6 hours
QUINUPRISTIN-DALFOPRISTIN 7.5 mg/kg, i.v, every 8 hours 7.5 mg/kg, i.v, every 8 hours
RIFAMPIN 300 mg, i.v/PO, every 8 hours 5-7 mg/kg, i.v/PO, every 8 hours
STREPTOMYCIN 15 mg/kg, i.v/i.m, every 12 hours Not applicable for pediatrics
VANCOMYCIN 15-20 mg/kg, i.v, every 8/12 hours 15 mg/kg, i.v, every 6 hours.

FOR S.VIRIDANS & S.BOVIS, THAT ARE HIGHLY SUSCEPTIBLE TO PENICILLIN:
a. Aq. Crystalline Penicillin G sodium(4 weeks)
b. Ceftriaxone (4 weeks)
c. Aq. Crystalline Penicillin G sodium + Gentamicin (2 weeks)
d. Ceftriaxone+ Gentamicin (2 weeks)
e. Vancomycin (4 weeks)
FOR OXACILLIN-RESISTANT STAPHYLOCOCCI:
- Vancomycin(6 weeks)
- Daptomycin(6 weeks)

FOR S.VIRIDANS & S.BOVIS, THAT ARE RESISTANT TO PENICILLIN:
a. Aq. Crystalline Penicillin G sodium(4 weeks)+Gentamicin (2 weeks)
b. Ceftriaxone (4 weeks)+ Gentamicin(2 weeks)
c. Vancomycin(4 weeks).
FOR OXACILLIN-SUSCEPTIBLE STAPHYLOCOCCI:
a. Nafcillin/oxacillin (6 weeks)+Gentamicin sulfate, for 3-5 days(optional)
b. Cefazolin(6 weeks)+ Gentamicin sulfate, for 3-5 days(optional)
c. Vancomycin(6 weeks).

FOR S.VIRIDANS & S.BOVIS, THAT ARE HIGHLY SUSCEPTIBLE TO PENICILLIN:
a. Aq. Crystalline penicillin G Sodium (6 weeks)+/- Gentamicin(2 weeks)
b. Ceftriaxone (6 weeks) +/-Gentamicin(2 weeks)
c. Vancomycin(2 weeks)
FOR S.VIRIDANS/ S.BOVIS, THAT ARE RELATIVELY/FULLY RESISTANT:
a. Aq. Crystalline penicillin G sodium+ Gentamicin(6 weeks)
b. Ceftriaxone +Gentamicin(6 weeks)
c. Vancomycin (6 weeks)

FOR OXACILLIN-SUSCEPTIBLE STAPHYLOCOCCI:
a. Nafcillin/oxacillin + Rifampin(6 weeks, or more, as necessary)+Gentamicin(2 weeks)
b. Vancomycin+Rifampin(6 weeks or more, as necessary)+ Gentamicin(2 weeks)
FOR OXACILLIN-RESISTANT STAPHYLOCOCCI:
a. Vancomycin + Rifampin (6 weeks or more, as necessary) + Gentamicin(2 weeks).

FOR AMPICILLIN, PENICILLIN & VANCOMYCIN SUSCEPTIBLE ENTEROCOCCI:
- Ampicillin+ Gentamicin(4-6 weeks)
- Aq. Crystalline Penicillin G sodium + Gentamicin(4-6 weeks)
- Vancomycin + Gentamicin(6 weeks)
FOR GENTAMICIN-RESISTANT STRAINS:
- If the organism is susceptible to Streptomycin use the same, in place of Gentamicin(with other drugs, as mentioned above)
FOR PENICILLIN- RESISTANT STRAINS:
- Ampicillin-sulbactam + Gentamicin (6 weeks)
- Vancomycin + Gentamicin(6 weeks)

FOR ENTEROCOCCUS FAECIUM STRAINS,THAT ARE RESISTANT TO PENICILLIN, AMINOGLYCOSIDES & VANCOMYCIN:
- Linezolid(8 weeks, or more)
- Quinupristin-Dalfopristin(8 weeks/more)
FOR ENTEROCOCCUS FAECALIS STRAINS, THAT ARE RESISTANT TO PENICILLIN, AMINOGLYCOSIDES & VANCOMYCIN:
- Imipenem-cilastatin + Ampicillin(8 weeks, or more)
- Ceftriaxone+ Ampicillin(8 weeks/ more).

1. DAPTOMYCIN:
- ADRs :
a. Myopathy
b. Rhabdomyolysis
- Monitoring parameters:
a. CPK (weekly)
b. Monitor for signs & symptoms of muscle pain
c. In patients, with renal dysfunction
d. Patients, receiving concomitant HMG-CoA reductase inhibitors(Statins)

2. GENTAMICIN:
- ADRs:
a. Nephrotoxicity
b. Ototoxicity
c. Neuromuscular blockade
- Monitoring parameters:
a. Serum concentrations of Gentamicin
- Special notes:
a. Avoid concomitant use of other nephrotoxic agents, like DIURETICS, NSAIDS, RADIOCONTRAST MEDIA, VANCOMYCIN,etc
b. Avoid rapid i.v administration.

3. LINEZOLID:
- ADRs:
a. Thrombocytopenia
b. Optic neuropathy
c. Peripheral neuropathy
- Monitoring parameters:
a. Platelet counts(weekly)
b. Visual changes
- Special notes:
a. Avoid concomitant use of MYELOSUPPRESSIVE AGENTS.

4. QUINUPRISTIN-DALFOPRISTIN:
- ADRs:
a. Phlebitis
b. Myalgias
c. Arthralgias
d. Hyperbilirubinemia
- Monitoring parameters:
a. Signs & symptoms of joint/ muscle pain
- Special notes:
a. Avoid venous irritation(phlebitis), by increasing the infusion volume from 250 to 500/750 ml
b. Alternative administration, via a central line.

5. RIFAMPIN:
- ADRs:
a. Hepatotoxicity
- Monitoring parameters:
a. LFTs(at baseline, and then every 2-4 weeks, during therapy)
- Special notes:
a. Avoid concomitant medications, that cause hepatotoxicity
b. Rifampin may cause RED/ ORANGE DISCOLORATION of bodily secretions(sweat, tears, urine, etc).

6. VANCOMYCIN:
- ADRs:
a. Nephrotoxicity
b. “RED MAN SYNDROME”
- Monitoring parameters:
a. Serum drug concentration of Vancomycin
- Special notes:
a. Red Man Syndrome if occurs can be managed, by prolonging the infusion time from 1-2 hours
b. Also consider administration of an ANTIHISTAMINE, prior to loading/ maintenance doses of drug.

Surgery is the main adjunct, that is followed in certain patients with IE
Indications for surgery include:
a. HF
b. Persistent bacteremia
c. Persistent vegetation
d. Increase in vegetation size
e. Recurrent emboli, in spite of prolonged antibiotic therapy
f. Valve dysfunction
g. Presence of large abscesses
h. IE, caused by resistant organisms.

- Surgery is mainly performed to:
a. Remove infected tissues
b. Restore hemodynamic function
- Surgeries involved, include:
a. Valvectomy
b. Valve replacement surgery.

Antimicrobial prophylaxis is used to prevent IE in patients, with high risk of the same
Choice of antimicrobial agent selection depends upon:
a. Types of patients, who are at risk
b. Procedures, that cause bacteremia
c. Organisms, likely to cause IE
d. Pharmacokinetics, cost , spectrum & ease of administration of available agents
- Major objective of antimicrobial prophylaxis in IE is to DIMINISH THE LIKELIHOOD OF IE IN HIGH-RISK INDIVIDUALS, WHO ARE UNDERGOING PROCEDURES, THAT CAUSE TRANSIENT BACTEREMIA.
- Endocarditis prophylaxis is recommended for ALL DENTAL PROCEDURES, that involve manipulation of gingival tissue of PERIAPICAL REGION of teeth, or PERFORATION of ORAL MUCOSA.

ANTIBIOTIC REGIMENS FOR IE PROPHYLAXIS WITH A DENTAL PROCEDURE:
ANTIMICROBIAL OPTIONS ADULT DOSES PEDIATRIC DOSES(in mg/kg)
ORAL AMOXICILLIN 2 g 50
IM/ IV AMPICILLIN 2 g 50
IM/ IV CEFAZOLIN/ CEFTRIAXONE 1 g 50
ORAL CEPHALEXIN 2 g 50
ORAL CLINDAMYCIN 600 mg 20
ORAL AZITHROMYCIN/CLARITHROMYCIN 500 mg 15
IV/ IM CLINDAMYCIN 600 mg 20.

1. Veverka.A, Crouch.A.Michael. “INFECTIVE ENDOCARDITIS”, Pharmacotherapy:A Pathophysiological Approach by Joseph.T.Dipiro et al. 7th
edition, McGraw Hill Publishers, pp:1821-1839.
2. Epaulard O, et al. Infective endocarditis-related stroke:diagnostic delay and prognostic factors. Scand J Infect Dis. 2009. 41(8):558-62.[Medline]
3. Durack DT, et al. New criteria for diagnosis of infective endocarditis:utilizationof specific echocardiographic findings. Duke Endocarditis Service. Am J Med.1994 Mar.96(3):200-9. [Medline]
4. Brusch JL. Infective endocarditis and its mimics in the critical care unit. Cunha BA, ed. Infectious Diseases in Critical Care.2nd ed. New York,NY: Informa Healthcare; 2007.261-2
5. Karchmer AW. Infective Endocarditis. Braunwald’s Heart Disease: A Textbook of Cardiovascular Medicine. 7th ed. WB Saunders Co;2005. 1633-1658.
DO SHARE YOUR REVIEWS OR QUERIES REGARDING
THIS!!!

THANK YOU!!!!!
