Infantil infected chronic subdural hematoma
15
Infantil infected chronic subdural hematoma Case presentation Helene Hurth, MS6 Innsbruck Medical University
description
Infantil infected chronic subdural hematoma. Case presentation Helene Hurth, MS6 Innsbruck Medical University. M.M. H&P: 5 m.o . male: fever , irritability for 3 days , intermittent emesis poor hygiene , macrocephaly no h/o trauma , no LOC - PowerPoint PPT Presentation
Transcript of Infantil infected chronic subdural hematoma

Infantil infected chronic subdural hematoma
Case presentationHelene Hurth, MS6
Innsbruck Medical University

M.M.• H&P: 5 m.o. male: fever, irritability for 3 days, intermittent emesis
poor hygiene, macrocephalyno h/o trauma, no LOC
alert, moves all extremities, PERRL, EOMI, bulging fontanelle,
Temp: 40,6°C (105,1°F), BP 82/67mmHg, HR 180, RR 34, SpO2 99% no ecchymosis/lacerations/abrations/deformities/crepitus
• Lab: CRP 40,3 mg/dl, WBC 14,8• PMH:term born, methamphetamine pos at birth
PICU at 1 month for RSV, apnea spells• SH: father retains full custody
open CWS case – mother: substance abuse3y/o healthy sibling

M.M.

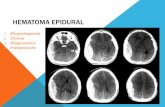
Preoperative MRIBilateral chronicsubdural hematoma
Le: 25 mmRi: 15 mm
Enhancement of membranes
3mm rightward midline shift

M.M.
• Subdural tab via AF after admission: 4+ GNR in gram stain – E.coli
• Burr hole drainage w/ bilateral drains the next morning
• Abx: Ceftriaxone, Meropenem

Postoperative MRI
Le: 12 mmRi: 7-8 mm
Resolution ofmidline shift
Septations

OP
• Craniotomy w/ resection of membranes on day 5 after borr hole drainage due to remaining fever and up trending inflammatory markers

Childhood extraaxial CNS infections• Age peaks: >11y (50%) & <1y (>20%)
• Duration of symptoms based on underlying cause
• Fever, headache, altered consciousness, focal deficits, full AF, poor feeding, seizures
S. Gupta, J Neurosurg Pediatrics 2011

Childhood extraaxial CNS infections• Postsinusitis: (frontal) SDE, epidural abscess, Pott‘s puffy tumor; +-
cerebritis
• Postmeningitis: diffuse hemispheric/infratentorial SDE
• Postoperative: epiduralabscess, SDE, osteomyelitis at OP-site
• Otogenic -> mastoiditis: SDE, epidural abscess
S. Gupta, J Neurosurg Pediatrics 2011

Childhood extraaxial CNS infections• Treatment: Initial wide craniotomy + abx• Complications: recurrent seizures, venous sinus/
cortical vein thrombosis• Outcome: preoperative presentation
Etiologyearly, aggressive surgical treatment
S. Gupta, J Neurosurg Pediatrics 2011

Infected CSDH
• Rare • Strept spp, Staph aureus, H. influenzae, E. coli,
Salmonella spp • Hematogenous • Satisfactory outcome • Antibiotic treatment• Drainage vs craniotomy

Surgical treatment: CSDH• Pre-OP T2*-MRI, randomly BH or SC• Burr holes: equivalent, lower mortality/morbidity/hospital stay• Small craniotomy w/ resection of outer and intrahematomal
membranes: superior if intrahematomal membranes present
M. Tanikawa, Acta Neurochirurgica 2001
N=20 N=29

Surgical treatment: CSDH• Outcome, reoperation, hospital stay• Hematoma recurrance: thick membranes
-> residualhematoma-> rebleeding
MRI (T2*) imagingto predict need for craniotomy
M. Tanikawa, Acta Neurochirurgica 2001

Case Tanikawa et al.

Summary
• Neurosurgery often required in extraaxial CNS infections
• Early diagnosis!• Consider infected CSDH with signs of bacteremia