Indonesia Country Report - mhlw.go.jp · PDF fileIndonesia Country Report Dr. Rachmi Untoro...
17
1 The 6 th ASEAN & Japan High Level Officials on Caring Societies: Healthy Next Generation: Strengthening Joint Collaboration Between Health and Social Welfare 8-11 September 2009 Tokyo, Japan Indonesia Country Report Dr. Rachmi Untoro Dr. Sri Hermiyanti Drs. Chazali Husni Situmorang Mr. Abas Basuni
Transcript of Indonesia Country Report - mhlw.go.jp · PDF fileIndonesia Country Report Dr. Rachmi Untoro...

1
The 6th ASEAN & Japan High Level Officials on Caring Societies:
Healthy Next Generation:
Strengthening Joint Collaboration Between Health
and Social Welfare
8-11 September 2009
Tokyo, Japan
Indonesia Country Report
Dr. Rachmi Untoro
Dr. Sri Hermiyanti
Drs. Chazali Husni Situmorang Mr. Abas Basuni

2
INDONESIA COUNTRY REPORT
I. Introduction
The government of Indonesia has showed in many instances their special attention on women newborn and child health. There are several inter sector
collaboration lead by the MOH, working on different scopes on maternal and child
health in the country. The improvement of health services in general and for maternal and child care in particular is best achieved also through tight collaboration between
health care and social welfare services. This collaboration will strive towards achieving
the MDG 4 and 5 for reducing maternal, and child mortality and morbidity.
To reduce maternal and child mortality, ensuring continuum of care for MNCH is important which spans from pregnancy, childbirth, postpartum, newborn and child
care; as well as continuum care at individual, family, community, primary care and first
referral levels. Through continuum of care approaches will beneficial for children to become a healthier next generation. These approaches are also an investment to high
quality human resources, support economics development and an important role in
poverty reduction
II. Current Situation
General Information
Indonesia is an archipelago country that stretched from Sabang at the top of Sumatra Island to Merauke at the bottom of Papua across the equator for more than
5,000 kilometers from east to west and more than 2,000 kilometers from north to
south, or from 6‟ north to 11‟ south latitude, and from 95‟ to 141‟ east longitude. It lies on a crossroads between two oceans, the Pacific and the Indian, and bridges two
continents, Asia and Australia.
It is an appropriate description of the archipelago as there are estimated to be a total of 17,504 islands, of which only about 6,000 are inhabited. There are five main
islands and about 30 smaller islands. The five main islands are: Sumatra (446,687
square kilometer); Java/Madura (129,306 square kilometer); Kalimantan, which
comprises two thirds of the island of Borneo (507,412 square kilometer); Sulawesi (193,847 square kilometer); and Papua (424,501 square kilometer), which is part of
the world's second largest island, New Guinea.

3
Inter census Population Survey (SUPAS) 2005 reveals total population were 218,868,791 with population density 117.6 people per sq km. The highest
population density province was DKI Jakarta (11,968.8 people per sq km)
meanwhile provinces in Kalimantan, Maluku and Papua had lowest density (5.9
people per sq km). Population distribution was unequal as 58.70% of total population lived in Java
Island (the area with only 6.95% of Indonesia), 21.03% in Sumatra, 7.21% in
Sulawesi, 5.53% in Kalimantan, 5.40% in Nusa Tenggara and Bali, and 2.13% in Maluku and Papua. In average, number of people lived in rural 56.88% and 43.12%
in urban area. Male populations were 107,274,528 and female populations were
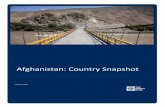
106,100,759. The composition of population by age was 29.04% (0-14 years old), 63% (15-64 years old) and 4.65% (≥ 65 years old).
Picture 1: Population pyramid of Indonesia
Source: Intercensal Population Survey (SUPAS) 2005
1. GNI per capita
To measure the welfare of the country, it is used Gross National Income (GNI). According to World Bank Development Indicator 2008, the GNI of Indonesia is
US$ 1,420 in per capita per year in 2006 and US$ 1,650 in 2007, stated Indonesia
as lower middle income country at rank 141 out of 178 country)
2. Poverty rate
According to National Socio-economic Survey, poor population is people having
average monthly cost per capita is below poverty line (PL), which consists of Food
Poverty Line (FPL) and Non Food Poverty Line (NFPL). FPL is classified based on
population cost for primary need, both food and non food. Number of poor population
in Indonesia was decreased from was 38.7 million (19,1%) in 2000 to 35.10 million
(15.97%) by February 2005; and in 2008 has reduced to 34,96 million (15,42%), as a
result of a range of poverty reduction programmes undertaken by the government.
(BPS - Statistic Indonesia, 2005)

4
3. Condition of Education
Population capability of reading and writing is reflected in literacy rate, which is
percentage of population aged 10 years and over who are able to read and write
Latin and other letters. Nationally, percentage of population capable to read Latin
letter in 2005 was 69.35%. Percentage of population capable to read other letters
was 1.03%, Latin and other letters was 21.53% and illiterate was 8.09%. Therefore,
percentage of literate population, consists of being able to read Latin letter, other
letters and Latin and other letters, was 91.91%.
4. Access to Drinking Water (Access to safe water)
Drinking water source using by household is classified into protected and
unprotected water source. In 2005, percentage of household having protected water source was 82.67%, consisted of protected well (35.63%), plumbing water
(17.99%), pump (13.73%), protected spring (8.52%), packaged water (4.06%) and
rainwater (2.70%). Meanwhile, percentage of household having unprotected water
source was 17.37%, consisted of unprotected well (9.75%), unprotected spring (3.96%), river (3.21%) and others (0.45%). (Source: Welfare Statistic, BPS-
Statistics Indonesia 2005)
Vital Statistics
1. Crude Death Rate
The Intercensal Population Survey 1995 estimation showed that the CDR in
1995 was 7.7 per 1,000 population, decreasing to 7.6 per 1,000 population in 1996
and did not show any changes until 1998. In 1999, the CDR decreased to 7.5 per
1,000 populations and to 7.4 per 1,000 populations in 2000. According to IDHS 2002,
national CDR was 8 per 1.000 populations in 2000. It shows that tendency of CDR
during the period of 1995–2000 was relatively stable with a few decreases. CDR in
hospital 3.8% in 2002 (88.441 number of death from 2.346.136 number of cases),

5
and 3.3% in 2005 (85.567 number of death from 2.561.106 number of cases).
(Source : MOH RI – 2005)
2. Crude Birth Rate and Total Fertility Rate
The National Total Fertility Rate (TFR) showed a stagnant in 2002 stood at 2.6
(IDHS 2002-2003) and 2.6 in 2007 (IDHS 2007) which urban (2.3) is lower than
rural (2.8). The National Crude Birth Rate (CBR) showed 2.09 per 1000 population (IDHS 2007) which urban (2.02 per 1000 population) is lower than rural (2.15 per
1000 population).
3. Infant Mortality Rate
Over the years, the IMR has improved as a result of a number of health
programs that have been implemented. In 1992 IMR was 68 deaths per 1,000 live births that declined to 57 deaths per 1,000 live births in 1994. The rate dropped
again to 46 deaths per 1,000 live births in 1997, and between 2002 and 2003 the
figure further declined to 35 deaths per 1,000 live births (IDHS, 2002-2003) and continues to decline to 34 deaths per 1,000 live births (IDHS 2007).
4. Under 5 Mortality Rate
In 1992 the U5MR stood at 97 deaths per 1,000 live births, but by 1994 this
figure had declined to 81 deaths per 1,000 live births. Between 2002 and 2003 the
figure dropped further to 46 and by 2007 had declined to 44 deaths per 1,000 live births (IDHS 2007). There are three main causes of infant mortality that remain a
serious challenge. They are acute respiratory infection (pneumonia), perinatal
complications and diarrhea.
A combination of these three accounts for a 75 percent share of infant deaths.
The main causes of death among children under five are almost identical: respiratory disease (pneumonia), diarrhea, neurological diseases (including meningitis and
encephalitis) and typhoid. Protecting and providing healthcare services to the poor
and vulnerable groups in rural and remote areas, as well as in pockets of poverty in
urban areas will be essential in reducing CMR. In addition to this, cooperation between the central and regional governments as well as cross-sectoral cooperation
to improve the maternal and child health is also urgently needed. The latest data
reported that U5MR in 2007 (IDHS 2007) was 44 per 1000 live births.
5. Maternal Mortality Ratio
Maternal mortality ratio is useful to describe the level of awareness on healthy living behavior, nutrition status and maternal health, environment health condition,
health service level particularly for pregnant women, delivery and parturition health
service. Maternal mortality ratio can be seen from 390 to 307 per 100,000 live-birth in 1998-2003. (Source: 2002-2003 IDHS). According to IDHS 2007, had showed
decreasing MMR to 228 per 100,000 live-birth.

6
6. Life Expectancy at birth
As we have known, the increase of life expectancy indirectly shows the increase
of life quality and community health. Based on the per province population
projection result done by BPS-Statistics Indonesia, 2003, the life expectancy rate in
Indonesia has gone through an increase from year to year and in 2003, the life expectancy rate in Indonesia has become 66.18. The highest life expectancy rate is
in Special Region of Yogyakarta (72.17), followed by Special Region of the Capital
City of Jakarta (72.12) and the shortest is West Nusa Tenggara (63.51).Trend of life expectancy at birth in 2008 is 70,6 ( man 68,6 and women 72,6)
Cause of Death
1. Causes of Maternal death
The main cause of maternal mortality in Indonesia classified as a preventable death, these are bleeding 30%, eclampsia 25%, infection 12%, puerperial
complication 8%, abortion complication 5%, prolong labour 5% (IHHS 2001).
Prevention of maternal death conducted through promotion and prevention program such as behavior change interventions, women and family empowerment,
community mobilization and monitoring of local MNCH status. MOH had included
these pre-event interventions in the MNCH program menu and budget allocation. Reduction of maternal mortality legislated in the MNCH regulations and through the
best practices or evidence-based interventions as listed in the MPS activities and
MNCH menus.
2. Causes of Infant deaths
The Indonesia Household Health Survey (IHHS/SKRT) 2001 explored the causes of infant mortality are perinatal complications (36%), acute respiratory infection
(pneumonia) (28%), diarrhea (9%), neonatal tetanus (3%), digestive disorder (4%)
and neurological disorder (3%). A combination of top three accounts for a 75 percent share of infant deaths. 57% infant death occurred less 1 month this is related to
poor maternal & neonatal status, sub standard access & quality health services and
care seeking behavior.
3. Causes of under 5 deaths
The main causes of death among children under five are almost identical: respiratory disease (pneumonia) 23%, diarrhea 13%, neurological diseases 12%
(including meningitis and encephalitis) and typhoid 11%. According to IDHS 2002-
2003 the prevalence pneumonia at under five children 7,2% and the prevalence of
diarrhea around 13%. The IHHS 2002 also shows that 70% mortality caused by malaria occurred at fewer than five children. From routine report the coverage of
household with pregnant woman or children under five years old which using treated
bed net only 50% compare the target 65%.
Nutritional Status
Nutritional status of community can be measured through some indicators, i.e.
low birth weight (LBW), nutrition status of under-fives, nutrition status of eligible

7
women with chronic energy deficiency and iodine deficiency disorders that are going
to be explained in details below:
1. Low Birth Weight (LBW)
The national LBW has not yet been available. However, the proportion of LBW can be known based on the estimation of the Indonesian Demographic and Health
Survey. The following table shows the proportion of LBW in 1992-1997 is 7.7%
(urban 6.6%, rural 8.4%) and 2002-2003 is 7.6%. Low birth weight (below 2,500 grams) is one of the main factors that influence
the perinatal and neonates mortality rate. Low birth weight (LBW) can be categorized
into 2, i.e. LBW due to premature (less than 37 weeks pregnancy) and intrauterine growth retardation (IUGR) due to LBW at term birth. In developing countries, there
are many cases of LBW with IUGR because of severe malnutrition of mother, anemia,
malaria, and sexually transmitted diseases prior to conception or during pregnancy.
2. Under-fives Nutritional Status
Under-fives nutritional status is one of the indicators that describe the status of community welfare. One of the methods to evaluate under-fives nutritional status is
the anthropometric using the body-weight index by age (W/A) method. The
categories being used are over nutrition (z-score > +2 SD); normal nutrition (z-score –2 SD up to +2 SD); lack nutrition (z-score < -2 SD up to –3 SD); severe
nutrition (z-score < -3SD).
Report of the National Socio-Economic Survey carried out in the previous years, a description was obtained on the development of under-fives nutrition status normal
nutrition 72.09% (2000) to 68.48% (2005), over nutrition 3.25% (2000) to 3.48%
(2005), lack nutrition 17.13% (2000) to 19.24% (2005), and severe nutrition 7.53% (2000) to 8.8% (2005).
3. Nutritional Status of Eligible Women with Chronic Energy Deficiency (CED)
One of the methods to know the nutritional status of eligible women aged
between 15-49 years old is by measuring circumference of upper arm. This measurement can be used as a method to identify how much risk of a woman to
deliver LBW infants. Indicator of the chronic energy deficiency uses the standard of
upper arm circumference <23.5 cm. The Survey of the BPS-Statistics Indonesia during 2000 – 2005 obtained a description on the risk of CED that was measured
based on upper arm circumference by age group better are 15-19 years old 38.04%
to 33.08%, 20-24 years old 26.59% to 21.67%, 25-29 years old 19.01% to 14.55%,
30-34 years old 15.11% to 10.45%, 35-39 years old 14.04% to 9.05%, 40-44 years old 13.16% to 9.37%, and 45-49 years old 13.16% to 10.25%.
The percentage of eligible women with adequate/normal nutrition during 2001-2005 was increased from 78.47% in 2001 to 89.5% in 2005. The percentage of
eligible women with adequate/normal nutrition in urban areas (80.61% to 92.0%)
was higher than in rural areas (76.54% to 88.47%).

8
4. Child abuse and child labor.
The data of child abuse and neglect in Indonesia are 182,400 (Ministry of
Social Affairs,2006), reflected in violence of physical, emotional, sexual, exploitation
and trafficking as well as neglected.
From 2004 to 2006 showed increasing number of physical violence 140-247
cases; emotionally psychological violence 40-450 cases; sexual violence 235-426
cases; neglected 101-131 cases. The number of trafficking cases in 2007 isn123ncases; total numbers from 2003 up to 2007 is 492 cases. The number of
child labor is 74. (Formal labor: 20 and informal labor : 54).
Child abuse, neglected and child labor could cause child development problems
( physical, mental, emotional and social development problems). This condition in
the long run will cause the low quality of human resources.
Pregnancy and Delivery
1. Average age at first marriage
The median of the first marriage age was 19,5% women 20 – 49 years (IDHS
2002-2003). There were 11.2% at 15 years old, 36.0% at 18 years old, and 54.1% at 20 years old.
2. Skilled birth attendant and Place of delivery
The maternal care indicators related to care during pregnancy have not changed
much since the 2002-03 IDHS to 2007 IDHS. However, improvement is observed in
delivery characteristics. The proportion of births delivered by a health professional increased from 66 percent to 73 percent, and the proportion of births delivered in a
health facility increased from 40 percent to 46 percent.
Health Facilities
1. Health Center
During 2000–2005, number of health center (including health center with bed) was continuously increased, from 7,237 units in 2000 to 7,669 units in 2005. In
that period, health center ratio to 100,000 populations was between 3.46–3.56
per 100,000 populations. It means that every 4 health centers covered 100,000 people.
Meanwhile, according to concept of health center working area, where one
health center averagely covers targeted 30,000 people, number of health center per 30,000 people in 2005 was averagely 1.07 units. It was not changed
comparing to 1.04 units per 30,000 people in 2004.
In the same period, number of sub health center also tended to increase from
21,267 units in 2000 to 22,171 units in 2005. Ratio of sub health center to 100,000 populations in 2000 and 2005 ranged between 10.13-10.53. It means
that every 10-11 sub health centers cover 100,000 people.
Based on number of health center and sub health center in 2000–2005, ratio of sub health center to health center was averagely 3:1. It means that every health

9
center was supported by 3 sub health centers in providing health service to
community. Increasing quality of health service in health center, some health centers had
been improved into health centers with beds. The number of health centers with
beds in 2000-2005 was increase from 1,785 units to 2,077 units (Source: MOH
RI 2005).
2. Hospital
In 2000 – 2005, number of hospitals (general and specific) in Indonesia were
increasing, from 1,145 units in 2000 to 1,178 in 2001 (2.88%) and 1,215 in
2002 (3.14%), then to 1,234 in 2003 (1.56%), 1,246 in 2004 (0.97%) and 1,268 in 2005 (1.77%). By ownership, in that period, number of government
hospital was only a half from total hospitals in Indonesia. The number of
general hospital from 910 units in 2000 (government 520 units, private 390
units) to 995 units in 2005 (government 559 units, private 436 units). The number of specific hospital from 235 units in 2000 (government 75 units, private
160 units) to 273 units in 2005 (government 83 units, private 190 units).
3. Community-based Health Facilities
In order to increase coverage of community health service, kinds of effort are implemented by utilizing existed potencies and resources in community. The
community-based health programs include integrated health post (Posyandu),
village maternal hut (Polindes), family herbs (Toga), village drug post (POD), etc.
Posyandu is one of famous community-based health programs. It conducts at least 5 priority programs, i.e. maternal and child health, family planning,
nutritional development, immunization and diarrhoeal controlling. Posyandu ratio
to village was 5.01, which means that averagely there were 5 Posyandu in every village.
Polindes is a community-based health program in order to assist midwifery
services by providing delivery unit, maternal and child health service and family planning. Meanwhile, there were 9,010 village drug posts, and its ratio to village
was 0.14. (Source : DG of Community Health, 2005). In 2006, there are new
programs of Poskesdes (village health post), Poskestren (health post in Islamic
boarding school) and Mushola Sehat (healthy Islamic prayer place). Those are 12,942 (Poskesdes), 200 (Poskestren) and 229 (Mushola Sehat). (Source :
Health Ministerial Report, 13 March 2007).
III. Program Intervention
Political commitment
Since 2005, effective policies and strong commitment created to improve maternal and neonatal and child health. Any efforts was made in assuring adoption of a
policy will guarantee its implementation. Even the Indonesian government was still
struggling with national financial problem, MOH consistently addressing bridging mechanism of low household financial capabilities with getting access to basic services.
Policies and Programs

10
As stated in National Development Program (Propenas), reducing maternal mortality, infant mortality and child mortality has become the main priority of health
development. In order to achieve the purpose, the focus of health development policies
will mainly on the improvement of quantity, network, and quality of health centers and
hospital and the improvement of quality and quantity of health personnel. The policy is expected to make the quality health facilities and services closer and accessible to the
people. The coverage and the quality of reproductive health services including family
planning services shall be improved.
In order to improve community health status, particularly maternal, neonatal and child
health, Ministry of Health had adopted the Making Pregnancy Safer (MPS) strategy that in-line to the Ministry of Health Grand Strategies as follows:
1. Improve access to and coverage of quality of maternal, neonatal and under 5
child care at the basic and comprehensive setting 2. Enhance and build effective partnerships, to advocate for and maximize available
resources and strengthen coordination of plans and activities in MPS.
3. Encourage woman, family and community empowerment, to ensure appropriate practices, provision and utilization of maternal, neonatal, and under 5 health
services.
4. Increasing Health Surveillance, Monitoring and MNCH Information System, and Health Financing
Referring to „Healthy Indonesia 2010”, Making Pregnancy Safer campaign had been launched and implemented since 2001. It focuses on an integrated and systematic
planning approach in clinical intervention with the emphasis on partnership.
The campaign is done by improving access and coverage of medical services for mothers and new-born babies, infants, and under 5 children, developing effective
partnership through inter-program and inter-sector cooperation, encouraging women
and family empowerment, and encouraging people involvement. Indonesian government consistently relied on MPS strategy in accomplishing MDG 2015 which is
similar in goal with difference in time of achievement toward Medium-term Health
Development Plan 2009 and Healthy Indonesia 2010.
Equity in MNCH access and services
In order to improve poor people‟s access to health services, the policy is to develop a system of health insurance. The method has been tried since the economy
crisis in 1998, through Social Safety Net Program, which offered free services to poor
people. The National Medium-term Development Plan (2004-2009) stated the program will be continued and improved by implementing a system of health insurance with
premiums being paid by the government. All poor people can get free medical services
at health centers and their network and at third-class hospitals, including services for pregnant women, and delivery, be it normal or difficult delivery. To make people easily
access the service, recruitment and deployment of medical staff at hospitals and health
centers (especially doctors and midwives) will be done.
It has been developed a various methods of pre-effort of health financing, such as
Health Fund, Health Insurance (Askes), Worker Insurance (Astek/Jamsostek), Managed

11
Care (JPKM), other health insurances and Health Care for Poor People (Jamkesmas).
According to National Socio-economic Survey, total number of poor population in Indonesia in February 2005 were 35.10 million (15.97%) and estimated to be 39.05
million (17.75%) in March 2006. The coverage for the poor and low income group will
increase to 75 million in 2008.
The government also specially allocate operational budget to provide access for the
community who lived in geographically and situational-based is considered as remote area. As mentioned before, archipelago country with many cluster islands usually
confronted with transportation problems that lead to limitation of access. In order to
maintain health service coverage, MOH provide mobile service unit, remote area team
or health taskforce, remote area health program and operational budget.
Focus on effective interventions
Since 2006, MOH had developed and packaged effective interventions and budgeting. De-concentration fund from central government allowed only for MNCH
program implementation as long as appropriate to the national effective care menus.
The evidence-based interventions whose have been proven to reduce mortality from the major causes of maternal deaths, neonatal deaths, infant deaths and under 5
deaths, are selected and implemented through inter-program and sector partnership
at high levels of population coverage in the whole country. The cost of providing these interventions to the vulnerable group who need them is affordable. The focus on
coverage should be linear to the existing health system characteristics or the quality
with which each intervention is delivered. These are critically important in the effort to
achieve the MDG target.
Focus interventions to accelerate Reducing of Maternal, Neonatal and Child Mortality
are: Birth Preparedness and Complication Readiness (P4K) labeled by commitment
sticker
Using MCH- Handbook Midwife-TBA Parnerships
Public-Private Partnerships
Increase Access and Quality of MNCH Services and assure timely and adequate
Emergency Obstetrics and Neonatal Care in every level of health delivery system (BEONC, CEONC).
Quality Family Planning Services and prevention of Unmet Needs
Establish drugs and commodities for emergency care, including availability of blood supply unit in every district hospital
Integrated Management of Childhood Illnessis
Management of Low BirthWeigth ad Asphyxia
Increase the capacity and quantity of strategic health resources Early Child Stimulation, Detection and Child Growth and Development
Management on MNCH Programme: DTPS for MNCH, AMP, LAM, MNCH
Information system, Facilitative supervision, Monitoring & Evaluation
Indicator as a proxy for mortality reduction efforts

12
As mentioned in the 2007 MOH Report, the coverage showed policies and
delivery strategies are being successful in reaching the target audiences. Besides, the numbers of health provider who provide effective care are also considered as good
indicators on monitoring mortality reduction.
Coverage indicators:
• Coverage of ANC ( first visit and fourth visit)
• Coverage of Deliveries assisted by Health Personnel • Coverage of Obstetrics and Neonatal Complications addressed
• Coverage of Postnatal Visits and Neonatal Visit
• Coverage of Infants Visit, Coverage of under 5 services
• Number of Community Midwives provided Basic Delivery Care • Number of Health Center provided Basic Emergency Obstetrics & Neonatal Care
(BEONC)
• Number of Hospitals provided Comprehensive Emergency Obstetrics & Neonatal Care (CEONC)
• Number of Maternal Death covered by Health Information System
• Contraceptive Prevalence Rate (CPR)
• Coverage of Health Center serve IMCI • Coverage of Health Center serve Early Child Stimulation and detection, Growth
and Development
• Coverage of Health Centre provide Child violence services
Strengtehening MNCH program
A. Community and family support for mothers and children
1. Birth Preparedness and Complication Readiness (BPCR/P4K)
BPCR/P4K using Sticker is one breakthrough to accelerate decreasing of maternal mortality which is the Sticker put it in each pregnant mother house.
BPCR/P4K is also as one component of Alert Village /Desa Siaga Program.
Through the BPCR/P4K every pregnant mother can monitor intensively by her husband, her family, community and midwife as well, early detection and
prompt treatment when complication arise, safe and secure delivery assisted
by skilled health provider and avoid maternal death. Through P4K with sticker also encourage and empower husband, family and community to be alert of
pregnant mother through preparation and provision of saving, transportation,
blood donors when pregnant mother needed. To improve knowledge of
pregnant mothers for making birth plan, MCH Handbook is given to them during the first visit with health provider.
2. Mother Friendly Movement
Ministry of Women Empowermaent and Ministry of Health initiates Mother
Friendly Movement/ Gerakan Sayang Ibu (GSI) which are a movement among
government and community to improve women quality of life especially to increase acceleration of MMR and IMR. GSI has programs for providing Birth
Preparedness, ensuring good nutrition for pregnant mother and save deliveries.
3. Conditional Cash Transfer (CCT) / Program Keluarga Harapan

13
Ministry of Social Affair initiates Conditional Cash Transfer / Program Keluarga
Harapan which are a movement among government and community to improve women quality of life particularly for poor pregnant or lactating
mother and childrenbetween 0-15 years old to get the quality health services
through cash supported to very poor household.
The reason underlying CCT is basically to improve the quality of human
resources of children as healthy next generation through compulsory basic
education, health and social welfare services in line with the MDG‟s target.
CCT program is crucial program since it is not merely social assistance but also
to educate the poor people in spending money for basic and specific purpose in relation with health and social welfare and education needs. In fact, CCT
has relative advantages compared with another poverty reduction schemes.
First, it has direct impact on real income with cash transfer. The poor is
expected to use the money for meeting their basic needs. It is also a form of income redistribution through more public spending allocated for welfare of
the poor. CCT is directed for reducing future poverty and inequality. It is a
kind of human investment for healthy next generation in the future trough better education, and health and welfare. Through the program the poor
people are socialized with the value of education, health and welfare for the
interest of their children. It changes paradigm in poverty reduction program from immediate benefit to the future and potential benefit.
Another advantage of CCT is to lessen the possibility of child labor as the time
of children mostly used for education. The relative importance of CCT is to
accelerate MDG‟s achievement including reduce poverty, promote gender issues, reduce child mortality rate, reduce maternal rate, and promote
education for all. Nevertheless, CCT program is not implemented exclusively
from another poverty reduction programs. Poverty is a complicated problem which requires more comprehensive approach. Therefore, as a kind of social
assistance, CCT should be followed by empowerment programs for the poor
under the heading of National Program for Community Empowerment in Indonesia.
Thus, CCT program affirms our belief that children is an important asset of our
society for the future in order to create healthy next generation, and we are
committed to tackling poverty through strengthening and promoting human resource development especially the children through the provision of
education, health and welfare. Indonesia has commitment to continue to
protect the right of children.
4. Family and Women Empowerment Models
Through women organization or women groups conduct the program to improve women empowerment, to improve women knowledge and skilled, to
support increasing income generating, giving the same opportunity in the
community forums.

14
The main activities of Community based Programs in supporting mother and child
health that stated above are:
- inform danger sign of mother, neonatal and under 5 children
- encourage using of MCH Handbook
- empowering health cadres - provide blood donors
- provide transportation if needed to refer mother
- provide saving for emergency situation
in line with this program, some districts and villages are produce regulations which
support maternal and neonatal health e.g.: regulation on midwife and TBA partnership, regulation on prohibit TBA in delivering baby (moving the role of TBA) and regulation
on village fund for activities that support Alert Village.
Another program in community which have strong contribute for improving mothers and children health is Integrated Services Post (Posyandu), which is a post
that provide growth and development monitoring and immunization for under five
years old, diarrhea prevention, ante natal care for pregnant mother, family planning, health promotion and food supplement distribution. Posyandu conduct in a some place
in sub village every month, coordinated by health cadres and visited by village midwife
to give immunization and ante natal care. Pregnant mother, baby and under five years old children who went to Posyandu should bring Buku KIA/ MCH Handbook that consist
of their medical and nutritional record and important information about health and
nutrition. Until 2007 there are about 55 % pregnant mothers and under 5 years old
children in Indonesia have Buku KIA that develop supported by JICA since 1997.
B. The roles of health and welfare professionals in related fields
To improve maternal and neonatal health in Indonesia, government and all
community element work together, hand in hand for best result. Health professionals
will responsible to: maintain quality of health services include training and quality assurance. Indonesian Obstetrics and Gynecologist Association (POGI), Indonesian
Pediatric Association (IDAI), Indonesian Midwife Association (IBI), Indonesia Nurse
Association (PPNI) and supported by Ministry of Health establish National Clinical
Training Network for Reproductive Health (JNKP-KR) that responsible to clinical training for doctor and midwife clinical training. JNPK has 3 levels, which are: Tertiary Clinical
Training Centre in Central Level, Secondary Clinical Training Centre in Province Level,
Primary Clinical Training Centre in District Level; each level have responsibilities to train Normal Delivery Care (APN), BEONC, CEONC and Contraceptive Technical Update.
POGI and IBI are also working together with Ministry of Health for distributing health
provider in districts for ObGyn and in villages for midwife.
To maintain good quality in maternal and neonatal health services, DHO with
POGI and IBI conduct Audit Maternal and Perinatal (AMP) every 3 month to review
mortality and morbidity cases in pregnant, delivery and perinatal period in district area. The result of AMP will be recommended to DHO, POGI, IDAI, IBI and local government
to improve health services include providing better health equipment, better
procedures and giving punishment for “naughty” health provider that not allow the procedures.

15
Partnership with NGO had been made and maintain to cover various problem in
Indonesia especially about demand creation on MNCH program, vary NGO are participated from local NGO and international donors such as WHO, UNFPA, UNICEF,
Safe the Children, US AID, AusAID, etc. They are working together, hand in hand with
central and local government to identify local specific problem and try to solve it with
their own resources in the field. Family Welfare Education (PKK) is one of local NGO that is supported by Ministry of Internal Affair and active in each district in Indonesia,
simultaneously work to empower women in maternal, neonatal and child health.
International donor work on their project areas which are decided by National Developing and Planning Board (Bappenas) and have specific scope of work depends
on their specialties and local problem.
C. Administrative systems and framework promoting “the continuum of care”
According to our commitment to reach goal MDG 4 and 5, we use principle of
“continuum of care” for maternal, neonatal and child health programs. As mention in Countdown to 2015, the continuum of care for MNCH includes integrated health service
delivery throughout the lifecycle, from adolescence, pre pregnancy to pregnancy,
childbirth, the postnatal period and childhood. The care is provided by families and
communities, through outpatient and out reach services, and through clinics and other health facilities.
60
92
6661.8
39.5
56.8
75.172
61
93.3
7376.9
34.6
76.8
35.532.4
0
10
20
30
40
50
60
70
80
90
100
FP ANC SBA Post natal
care
Early
Breastfeeding
URI care ORT in
Diarrhea
Vit A Immunization
IDHS 2002-2003 & prelimenary report IDHS 2007
prepregnancy birth postnatal pregnancy childhood

16
Table activities in continuum of care in Indonesia
GROUP ACTIVITIES PROVIDED BY
Contraceptive Prevalence - FP information - Contraception providing
- Training for
contraceptive technological update
for health provider
- Quality assurance
- DHO, PHO, MOH, Family Planning Coordinating
Board
- Communities - NGO
Antenatal visit - Tracking and register pregnant mother,MCH-
HB
- Integrated Health Post (Posyandu)
- Information of
Pregnancy, delivery
and post delivery Danger Sign (BPCR)
- Communities - Community Midwife
- Village Health Post/
Maternity Huts, Health Center
Skilled attendant at
delivery
- Partnership
Community Midwife
and TBA - Birth Preparedness
and Complication
Readiness - Distribution midwife to
village
- Normal Delivery Training
- EmONC Training
- Communities
- DHO, PHO
- Community Midwife - Village Health Post/
Maternity Huts
- Health Center - HC-BEONC
- Hospital CEONC
Postnatal visit within 2
days
- Integrated Health Post
(Posyandu)
- Communities
- Community Midwife
Early and exclusive
breastfeeding
- Rooming-in for mother
and neonatal
Case management of
pneumonia
- Integrated
Management Childhood Illness
(IMCI)
- DHO, PHO, Health
Center
Oral Rehidration therapy
for Diarhea
- ORT Providing
- IMCI - Posyandu
- Health Promotion
through MCH handbook
- DHO, PHO, Health
Center - Communities
Vitamin A distribution - Posyandu
- Vitamin A national
campaign every February and August
- DHO, PHO, Health
Center
- Communities
Immunization - Vaccine Providing
- Immunization
Sweeping
- DHO, PHO, Village
Midwife

17
Result of every group of activities in continuum of care has improved every year as shown in country report based on IDHS, IHHS and routine report from HC, DHO and
PHO every year, but we realize that we should make focused intervention that show
below to accelerate decreasing MMR and MMR.
Indonesia is one of various countries ratified and committed to achieve the MDG and
some aspect to be considered on the way to the ultimate goal, such as:
Diagram of Health Delivery and Referral System
MPS Workshop, HOGSI - Malang, 3 April 2003434348
CENTRAL
PROVINCE
HOSPITAL
Village
Sub-District
DISTRICT
• BPCR
• SBA-TBA Partnership
• FP
• ANC/BDC/AMSTL/IBF
• Postnatal Care
• LAM MNCH-FP
• BEONC
• FP
• ANC
• BDC/AMSTL/IBF
• Postnatal Care
• Integrated Essential RH
• LAM MNCH-FP
• CEONC
• FP
• ANC/BDC/AMSTL/IBF
• Intensive Care
• Postnatal Care
• Planning
• Facilitating
• DTPS MPS
• AMP
• Facilitative Supervision
• Monev
• LAM MNCH-FP Analysis
• Planning
• Facilitating
• Monev
• Planning
• Empowering
•Advocating
• Monev
HOSPITAL
Health Center
Health Post
Maternity Hut
Integrated Services
Community• BPCR
• Health Seeking Behavior
BEONC
FP
ANC
BDC/AMTSL/IBF
Postnatal care
MCH-HB
Integrated Essential
RH
LAM MNCH-FP
IMCI
Mgt Asphyxia
Mgt Sev Malnut
CEONC
FP
ANC/BDC/AMSTL/BF
Intensive Care
Postnatal Care
Mgt Sev Malnut
BPCR, MCH-HB
Health Seeking Behavior
BPCR, MCH-HB
SB-TBA Partnership
FP
ANC/BDC/AMSTL/BF
Postnatal Care
LAM MNCH-FP