INDEX OF CANCER PREPAREDNESS...5 Index of Cancer Preparedness Methodology report The conomist...
21
INDEX OF CANCER PREPAREDNESS Methodology report Founding supporters
Transcript of INDEX OF CANCER PREPAREDNESS...5 Index of Cancer Preparedness Methodology report The conomist...

INDEX OF CANCER PREPAREDNESS
Methodology report
Founding supporters

2Index of Cancer Preparedness
Methodology report
© The Economist Intelligence Unit Limited 2019
Contents2 Methodology overview
3 Index framework
4 Background indicators
5 Methodology development
5 Literature review
5 Preliminary indicators selection
5 Country selection
6 Construction of the scores
6 Weightings and index consistency
7 Quantitative and qualitative indicators
8 Limitations
9 Indicator framework detail
16 Main data sources
17 Research team
18 References

3Index of Cancer PreparednessMethodology report
© The Economist Intelligence Unit Limited 2019
Methodology overview
The Index of Cancer Preparedness (ICP) measures how ready healthcare systems are for the challenge of cancer across 28 countries. It seeks to answer the question: how well prepared are countries to achieve major reductions in premature deaths from cancer, increase cancer survival rates, and improve quality of life for cancer patients and survivors? This document describes the methods used to build the index.
The index explores the issue of cancer preparedness through three broad domains: 1) policy and planning, 2) care delivery and 3) health systems and governance. The first domain on policy and planning focuses on levers that are mostly in the hands of policymakers. The second domain looks at the delivery of cancer-specific activities within health systems themselves, while the final domain acknowledges that cancer cannot be defeated by cancer-focused activities alone. The three domains are broken down into 13 sub-domains and 45 indicators. Scores are weighted and normalised, so that the final score for each country ranges from 0 to 100, with 100 being the highest possible score, representing complete alignment with best practice.
The design of the index was driven by the creation of a theoretical framework: the curation of a collection of indicators that measure elements of cancer preparedness that are inherently desirable. We therefore hope that the index can offer value beyond simply the final composite score, and be used to drive discussion based around action at the domain, sub-domain and indicator level. In addition to the index we have also collected data for 21 background indicators to support correlation analysis. These indicators provide context but are not computed in the index scores; they include indicators of healthcare spend, health outcomes and risk factors.
The index was built following a literature review and expert panel meeting. It covers a total of 28 countries from across five geographic regions: Africa/Middle East, Latin America, North America, Asia-Pacific and Europe; and three World Bank income groups: lower-middle, upper-middle and high income. The index findings are discussed in detail in a complementary white paper by The Economist Intelligence Unit, entitled Cancer preparedness around the world: National readiness for a global epidemic. The index results, the white paper and supporting content can be found at http://worldcancerinitiative.economist.com/.

4Index of Cancer Preparedness
Methodology report
© The Economist Intelligence Unit Limited 2019
Index framework
The Economist Intelligence Unit, working with an expert panel, developed a framework to score countries based on the following research question:
• How well prepared are countries to achieve major reductions in premature deaths from cancer, increase cancer survival rates, and improve quality of life for cancer patients and survivors?
The development of the index was driven by the creation of a theoretical framework—informed by a literature review, then discussed and critiqued by a group of experts—that consisted of elements of cancer preparedness that are inherently desirable, such as having cancer registries, running screening programmes and ensuring essential drug access. Through consultation with experts and internal audits we explored potential indicators on the basis of their relevance, availability and cross-country comparability. For areas that lacked appropriate indicators we designed, in consultation with topic
experts, survey questions to capture and score the desired phenomena.
The resulting ICP combines 13 sub-domains, broken down into 45 indicators (29 quantitative and 16 qualitative indicators). The sub-domains are themselves clustered into three domains:
Policy and planning: the first domain focuses on levers that are mostly in the hands of policymakers. It examines whether countries are taking the necessary steps to effectively understand and manage their cancer burden; and, are they taking action to reduce cancer incidence through reducing risky behaviours?
Care delivery: the second domain looks at the delivery of cancer-specific activities within health systems themselves, starting with immunisation and screening campaigns and working through to the delivery of care for cancer patients and survivors. The accessibility of drugs and technologies are included here, along with questions on the
Source: ICP.
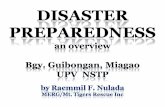
The three domains and 13 sub-domains of the ICP
Cancer preparedness
Policy and planning Care delivery Health system & governance
National cancer control plan Immunisation Political will
Population basedcancer registry Screening detection Infrastructure
Cancer research Service availability andworkforce
Intersectoral actionand governance
Tobacco control Clinical guidelines
Lifestyle and diet Patient-centred care

5Index of Cancer PreparednessMethodology report
© The Economist Intelligence Unit Limited 2019
comprehensiveness of clinical guidelines and the use of patient-centred care.
Health system and governance: the final domain acknowledges that cancer cannot be defeated by cancer-focussed activities alone. It looks at factors such as political will and intersectoral action, and the provision of basic healthcare and a health-enabling environment.
Figure 1 shows how the domains and sub-domains are organised.
Background indicators
Additionally, data for a set of 21 background indicators were collected to allow correlation analysis. They provide context but are not computed into the index scores. These indicators include measures of healthcare spending, health outcomes and risk factors. These measures were identified by The Economist Intelligence Unit and the expert panel as key variables that may be associated with differing levels of performance in cancer preparedness.

6Index of Cancer Preparedness
Methodology report
© The Economist Intelligence Unit Limited 2019
Methodology development
Literature review
The initial step in the development of the methodology was a literature review carried out by experienced health specialists at The Economist Intelligence Unit. The search took in health policy documents, academic literature, and other health system studies. Its goal was to identify existing frameworks, indicators and data sources on the topic of cancer preparedness.1-10 The literature review used a range of search approaches including a focused bibliographic database search (in MEDLINE, PubMed and Embase), iterative grey literature searches, and supplemental search techniques such as citation and author searches, scanning of reference lists and related-articles searching.
Preliminary indicators selection
An initial set of domains and indicators were then selected, guided by the concept of “tracer indicators”, which involves the selection of a subset of indicators that are representative of a group of services. Such an approach has been used in multiple publications identified in the literature review and recently by the World Health Organisation (WHO) in developing a universal health coverage index published in 2016.
We then convened a panel of international healthcare cancer policy experts to discuss and validate the preliminary approach in a one-day session in London. During this session, the most relevant indicators of cancer preparedness were determined for each of the index domains.
Further to expert recommendations, we performed additional rounds of verifications to establish the best possible metrics, such
as data audits, literature searches and data analysis.
We would like to thank the panel participants:
• Tit Albreht: co-ordinator, Joint Action Innovative Partnership for Action Against Cancer (iPAAC), National Institute of Public Health of Slovenia
• Carlos Castro: medical director, Liga Colombiana Contra el Cáncer
• Sonali Johnson: head of advocacy, Union for International Cancer Control (UICC)
• Sandro Martins: co-ordinator, Specialized Healthcare, Ministry of Health, Brazil
• Karima Saleh: senior economist (health), health, nutrition and population, World Bank
• Josep Tabernero: president, European Society for Medical Oncology (ESMO)
• Šarūnas Narbutas: president, Lithuanian Cancer Patient Coalition and Youth Cancer Europe
Country selection
The index covers 28 countries from across five broad regions of the world: Africa/Middle East, Latin America, North America, Asia-Pacific and Europe (Table 1). Within each region, we tended to select countries with the largest populations, along with examples of smaller countries that represent interesting or unusual approaches to cancer preparedness. We wanted to not only capture the diversity in policy adoption and implementation in high-income countries, but also include comparisons from where the burden of cancer is growing fastest: in upper- and lower-middle income countries. We hope to extend the

7Index of Cancer PreparednessMethodology report
© The Economist Intelligence Unit Limited 2019
Weightings and index consistency
Weightings are intended to reflect the importance attached to each dimension of the index. While we acknowledge that wider issues around health systems and governance (domain 3) are important, we decided—through discussion with the expert panel—that the first two domains were relatively more impactful, and indeed consisted of more indicators. We therefore attached 40% weights to domain 1 (policy and planning) and 2 (care delivery), and a 20% weight to domain 3 (health systems and governance). Within each of the three domains, the sub-domains and indicators were considered of equal importance and so given equal weight. However, there is functionality in the workbook that allows the user to apply different weights and recalculate index results.
We checked the consistency of the index by running correlations between sub-domains. None were found to be significantly overlapping or co-linear. We did not run a formal principal component analysis or sensitivity analysis because conceptually the index was designed as a combination of desired policy inputs, and so has value beyond simply giving a final composite score; the framework is not statistically determined, but rather based on elements of cancer preparedness that are inherently desirable. Moreover, given the relatively limited number
research to more countries in future iterations of the index.
Construction of the scores
The ICP is a composite index, and overall scores for each country are produced through normalising, weighting and combining scores of the three domains and their indicators. In turn, sub-domain scores are calculated as the weighted sum of individual indicator scores.
All scores are presented in a normalised scale of 1 to 100 (where 100 is the best possible score), displaying the relative performance of each country. Normalisation is based on the formula:
x = (x - Min(x)) / (Max(x) - Min(x))
Min(x) and Max(x) are, respectively, the lowest and highest values possible for any given indicator. For quantitative indicators with pre-existing data sets—for example the number of clinical oncologists in a country—Max(x) is simply the highest score in the data set. For qualitative data sets, where we set the scoring range (see section on qualitative indicators on the next page), Max(x) is the highest possible score, whether or not any country actually met that score. We used the min-max technique as it is widely accepted, frequently used and also an easily understandable method of normalisation.
Table 1: The full list of 28 countries, organised by world-bank income levels
• High income • Australia; Canada; France; Germany; Italy; Japan; Netherlands; Saudi Arabia; South Korea; Spain; Sweden; UK; US
• Upper middle income • Argentina; Brazil; Chile; China; Colombia; Mexico; Romania; Russia; South Africa; Thailand; Turkey
• Lower middle income • Egypt; India; Indonesia; Kenya

8Index of Cancer Preparedness
Methodology report
© The Economist Intelligence Unit Limited 2019
of countries included in the first wave of the study, and with the vision to expand the coverage in the future, a purely statistically determined framework would be sensitive to addition of any new countries.
Some indicators have all countries scoring the same, positive value—for example all countries legislate for warnings on cigarette packages—and therefore do not discriminate between countries. We decided to keep these indicators, as they reflect key policy decisions and, while the index is designed for global use, this first tranche of countries are all high- and middle-income countries. We hope to be able to add low-income countries in future iterations, in which these indicators will become more instructive. Rankings and scores were checked in an iterative process by Economist Intelligence Unit specialists, which allowed us to identify data anomalies that could then be corrected.
Quantitative and qualitative indicators
The 29 quantitative indicators in the index draw on numeric raw data from key global healthcare organisations including the WHO and the World Bank.8, 11-20 The few missing data points were imputed by calculating regional averages. A total of 16 qualitative indicators were designed by The Economist Intelligence Unit for this study; they analyse topics for which no cross-country data were previously available.21-23 These are based on standardised assessments of country performance using detailed scoring guidelines, and are displayed as scores in a numeric scale (usually 0 to 3, where 3 is best):
• Four indicators measure the existence and quality of national cancer control plans. The first of the four indicators measure the presence or absence of a specific, up-to-date cancer control plan, or if it is just covered in a wider NCD plan. The second
indicator assesses the comprehensiveness of the plan. The third asks whether the plan incorporates a specific implementation framework—including funding—while the fourth looks at whether a monitoring and evaluation framework for the plan is in place.
• Three indicators measure the existence and quality of population-based cancer registries. The first looks at the existence of regional or national population registries. The second assesses the scope and coverage of cancer registries, incorporating matters such as whether the registry collects not only incidence data but also tumour site, stage, treatment and outcomes data. The third indicator asks whether the cancer registry is interoperable with other health information systems, such as electronic health records.
• One indicator assesses whether there is a national cancer research policy or programme.
• Three indicators look at service availability and workforce. The first one estimates the density of clinical oncologists in a country. The second looks at the availability of a selection of cancer medicines on the WHO Essential Cancer Drug List. The drugs we checked for were: cisplatin; fluorouracil; docetaxel; imatinib; rituximab; trastuzumab. The third indicator assessed the degree of reimbursement for cancer medicines—some systems restrict reimbursement (for example by introducing co-payments).
• One indicator looked at clinical guidelines. It assessed whether up to date national evidence-based guidelines exist for four priority cancers: breast, lung, prostate and colorectal.
• Three indicators looked at patient-centred care. The first assessed whether national policies or recommendations exist for

9Index of Cancer PreparednessMethodology report
© The Economist Intelligence Unit Limited 2019
(particularly for low-income countries) medicines reach only main urban centres, while access in rural areas is lacking.
2. Conversely, many qualitative indicators based on the examination of national policies and plans should be interpreted as an aspiration from the government; they should not necessarily be interpreted as a measure of effectiveness or quality of implementation of programmes or objectives.
3. Research for this study was carried out in the second half of 2018; it considered the best evidence at that time on matters pertaining to cancer preparedness. This is a landscape that is undergoing continuous change, and so the situation in some countries may have since moved on.
4. For quantitative indicators, the index relies on the latest available data. Databases from different organisations are updated with differing frequencies. Therefore, there may be some lags in the situation depicted by certain indicators as regards the situation on the ground.
5. The study offers a simplified view of the complex landscape of cancer preparedness based on indicators deemed the most representative across selected topics. Selection was informed by an examination of the literature and consultations with experts but is necessarily limited in scope. Consequently, some areas of cancer preparedness may not have been addressed.
co-ordinated and integrated cancer care with multidisciplinary teams. The second looks for the existence of national clinical guidelines for long-term follow-up, rehabilitation and return to work. The third indicator asks about the existence and role of patient support organisations; not only whether they exist, but do they also play a role in cancer policy development and decision-making.
• One indicator measures the degree of intersectoral action for health and health equity. It asks whether national policies for health and well-being exist that address at least two priority determinants of health and involve at least two sectors. It was not necessary that the policies target cancer specifically.
Limitations
Any research programme has limitations. We describe here five potential limitations of the ICP:
1. Qualitative indicators developed by The Economist Intelligence Unit on availability of medicines on the WHO Essential Cancer Drug List were based on an assessment in one big public hospital in the capital of the country. This was intended to produce a realistic assessment of a certain level of availability of medicines “on the shelf”, instead of what was indicated in national policies and regulations. The limitation of this approach is that the results of these indicators may not reflect the situation across the country. In the research process, it was noted that in many cases

10Index of Cancer Preparedness
Methodology report
© The Economist Intelligence Unit Limited 2019
Table 2: Indicator framework detail, showing domain, sub-domain and indicators. The scoring system is described and the indicator definition. Type of indicator is qualitative, quantitative or categorical
Domain Sub-domain/Indicator Scoring system Definition Type
1) Policy and planning
1.1) National cancer control plan
1.1.1) Existence of national cancer control plan
There is no plan = 0Partially, only a component of an non-communicable diseases (NCDs) plan = 1Yes, there is a dedicated national cancer control plan = 2
Indicates whether or not the country has a national policy, strategy or action plan for cancer and whether the plan is part of a broader NCDs plan, or a health system plan
Qualitative
1.1.2) Comprehensiveness of cancer control plan
Plan does not specify any of the below = 0Plan addresses only one of the below = 1Plan addresses two or three of the below = 2Plan addresses all of the below = 3
Options:a) Includes specific targets and sub-domainsb) Coverage of continuum of cancer care services: prevention, early detection and diagnosis, treatmentc) Supportive and palliative care d) Patient-centred care
The scope and quality of the national cancer control plan. A country without a plan scores zero
Qualitative
1.1.3) Implementation framework for cancer control plan
Plan does not specify any of the below = 0Plan addresses only one of the below = 1Plan addresses two of the below = 2Plan addresses all of the below = 3
a) Leadership for plan implementationb) Timeline (start and end dates) c) Financial resources for plan activities
The implementation framework of the national cancer control plan. A country without a plan scores zero
Qualitative
1.1.4) Monitoring and evaluation of cancer control plan
Not addressed in the plan and there are no published evaluation reports = 0Plan addresses only one of the below = 1Plan addresses two of the below = 2
a) Cancer control governance (as per national plan)b) There is a framework for monitoring and evaluation of the cancer control plan
The governance and monitoring framework of the national cancer control plan. A country without a plan scores zero
Qualitative
Indicator framework detail

11Index of Cancer PreparednessMethodology report
© The Economist Intelligence Unit Limited 2019
Table 2: Indicator framework detail, showing domain, sub-domain and indicators. The scoring system is described and the indicator definition. Type of indicator is qualitative, quantitative or categorical
Domain Sub-domain/Indicator Scoring system Definition Type
1.2) Population-based cancer registry (PBCR)
1.2.1) Existence of PBCR There is no PBCR = 0Existence of PBCR (regional or national) = 1Existence of regional high-quality PBCR = 2 Existence of national high-quality PBCR = 3
The existence and quality of a national or regional PBCR
Qualitative
1.2.2) PBCR scope and coverage No registry exists = 0Registry addresses only one of the below = 1Registry addresses two or three of the below = 2Registry addresses four or more of the below = 3
Registry collects: a) incidence datab) patient demographics data c) tumour (cancer) characteristics data d) stage of disease data e) treatment and outcomes data f) Last year of data (updated with last three years)
The scope and coverage of the national or regional PBCR
Qualitative
1.2.3) PBCR linkage with other health information systems
PBCR is not linked to other health information systems = 0Linkage/interoperability with other health information systems = 1
The degree to which the PBCR is linked to other health information systems (eg, electronic health records)
Categorical
1.3) Cancer research
1.3.1) Field epidemiology training programmes
No availability of field epidemiology training programmes = 0Availability of field epidemiology training programmes = 1
Availability of field epidemiology training programmes
Categorical
1.3.2) National cancer research policy or programme
Country does not have a national cancer research policy or programme = 0Existence of national cancer research policy or programme = 1
Indicates whether or not the country has a national cancer research policy or programme
Categorical
1.4) Tobacco control
1.4.1) Operational policy, strategy or action plan to reduce the burden of tobacco use
Absence of operational policy, strategy or action plan to reduce the burden of tobacco use = 0Presence of operational policy, strategy or action plan to reduce the burden of tobacco use = 1
Indicates whether or not the country has an operational policy, strategy or action plan for tobacco use
Categorical

12Index of Cancer Preparedness
Methodology report
© The Economist Intelligence Unit Limited 2019
Table 2: Indicator framework detail, showing domain, sub-domain and indicators. The scoring system is described and the indicator definition. Type of indicator is qualitative, quantitative or categorical
Domain Sub-domain/Indicator Scoring system Definition Type
1.4.2) Compliance with smoke-free legislation
Low compliance = 0Moderate compliance = 1High compliance = 2
Compliance with regulations on smoke free-environments (national legislation)
Qualitative
1.4.3) Warning labels No = 0 Yes = 1
A nationwide law mandating health warning labels for tobacco packages has been adopted in the country
Categorical
1.4.4) Bans on advertising, promotion and sponsorship
Complete absence of ban, or ban that does not cover national television (TV), radio and print media = 0Ban on national TV, radio and print media as well as on some but not all other forms of direct and/or indirect advertising = 1Ban on all forms of direct and indirect advertising = 2
Legislation to determine whether all or any forms of tobacco advertising, promotion and sponsorship are banned
Qualitative
1.4.5) Affordability of cigarettes, trend change 2008 to 2016
Cigarettes more affordable since 2008, or no trend change = 0Cigarettes less affordable since 2008 = 1
Indicates whether cigarettes have become less or more affordable for the period in 2008-16—based on per-head GDP needed to buy 2,000 cigarettes of the most sold brand in the country. Measures country's effort to raise tobacco taxes
Qualitative
1.5) Lifestyle and diet
1.5.1) Operational policy, strategy or action plan to reduce unhealthy diet related to NCDs
Absence of an operational policy, strategy or action plan to reduce unhealthy diet = 0Presence of an operational policy, strategy or action plan to reduce unhealthy diet = 1
Indicates whether or not the country has an operational policy, strategy or action plan to reduce unhealthy diets related to NCDs
Categorical
1.5.2) Operational policy, strategy or action plan to reduce physical inactivity and/or promote physical activity
Absence of operational policy, strategy or action plan to reduce physical inactivity and/or promote physical activity = 0Presence of operational policy, strategy or action plan to reduce physical inactivity and/or promote physical activity = 1
Indicates whether or not the country has an operational policy, strategy or action plan to reduce physical inactivity and/or promote physical activity
Categorical
1.5.3) Operational policy, strategy or action plan to reduce the harmful use of alcohol
Absence of operational policy, strategy or action plan to reduce the harmful use of alcohol = 0Presence of operational policy, strategy or action plan to reduce the harmful use of alcohol = 1
Indicates whether or not the country has an operational policy, strategy or action plan to reduce the harmful use of alcohol
Categorical

13Index of Cancer PreparednessMethodology report
© The Economist Intelligence Unit Limited 2019
Table 2: Indicator framework detail, showing domain, sub-domain and indicators. The scoring system is described and the indicator definition. Type of indicator is qualitative, quantitative or categorical
Domain Sub-domain/Indicator Scoring system Definition Type
2) Care delivery
2.1) Immunisation
2.1.1) National Human papilloma virus (HPV) vaccination programme
Absence of national HPV vaccination programme = 0Presence of national HPV vaccination programme = 1
Indicates the presence or absence of a national HPV vaccination programme
Categorical
2.1.2) Hepatitis B vaccination coverage, infants
% The percentage of one-year olds who have received three doses of hepatitis B vaccine in a given year. (90% coverage set as a threshold based on WHO target for elimination of hepatitis B by 2030.*
Quantitative
2.2) Screening and early detection
2.2.1) National screening programme for cervical cancer
Absence of national screening programme for cervical cancer = 0Presence of national screening programme for cervical cancer = 1
Indicates whether or not the country has a national screening programme for cervical cancer
Categorical
2.2.2) National screening programme for breast cancer
Absence of national breast cancer screening programme = 0Presence of national breast cancer screening programme = 1
Indicates whether or not the country has a national breast cancer screening programme
Categorical
2.2.3) Availability of mammography or clinical breast exam (CBE)
No availability of mammography or CBE = 0Availability of CBE = 1Availability of mammography = 2
Availability of mammography or CBE for early detection of breast cancer at the public primary healthcare level
Qualitative
2.2.4) Availability of faecal occult blood test or faecal immunological test
No availability of faecal occult blood test or faecal immunological test = 0Availability of faecal occult blood test or faecal immunological test = 1
Availability of faecal occult blood test or faecal immunological test at the public primary health care level
Categorical
2.2.5) Availability of bowel cancer screening by exam or colonoscopy
No availability of bowel cancer screening by exam or colonoscopy = 0Availability of bowel cancer screening by exam or colonoscopy = 1
Availability of bowel cancer screening by exam or colonoscopy at the public primary health care level
Categorical
2.3) Service availability and workforce
2.3.1) Availability of radiotherapy in the public health system
No availability of radiotherapy in the public health system = 0Availability of radiotherapy in the public health system = 1
Indicates whether or not the country has radiotherapy generally available in the public health system.
Categorical
2.3.2) Radiation oncologists density N/A Number of radiation oncologists in the country (per 1,000 population)
Quantitative
* WHO. Global Hepatitis Report, 2017. Geneva: World Health Organization, 2017)

14Index of Cancer Preparedness
Methodology report
© The Economist Intelligence Unit Limited 2019
Table 2: Indicator framework detail, showing domain, sub-domain and indicators. The scoring system is described and the indicator definition. Type of indicator is qualitative, quantitative or categorical
Domain Sub-domain/Indicator Scoring system Definition Type
2.3.3) Capacity of radiotherapy machines to meet patient need
N/A Actual number of radiotherapy machines available/number of radiotherapy machines required. Number of radiotherapy units, including Linear Accelerators and Cobalt-60 from the public and private sectors
Quantitative
2.3.4) Clinical oncologists density N/A Number of clinical oncologists in the country (per 1,000 population). The data are collated from various sources including government sources, published research, professional associations and experts. The clinical specialty of clinical oncology/medical oncology may vary across countries
Qualitative
2.3.5) Availability of medicines on WHO Essential Cancer Drug List
An interview with public hospital pharmacist in the capital confirms that these medicines are in stock = 1 or are not in stock = 0 (for each of the below)
a) Cisplatin (+1)b) Fluorouracil (+1)c) Docetaxel (+1)d) Imatinib (+1)e) Rituximab (+1)f) Trastuzumab (+1)
General availability of medicines on WHO Essential Cancer Drug List in the public health system
Qualitative
2.3.6) Coverage for cancer medicines
Cancer medicines are not reimbursed (patients pay full price) = 0Cancer medicines are partially reimbursed (patients are required to cover a proportion of the costs) = 1Cancer medicines are fully reimbursed (100%) = 2
Degree of reimbursement for cancer medicines in the country
Qualitative
2.3.7) Oral morphine availability Absence of oral morphine = 0General availability of oral morphine = 1
Indicates whether or not the country has oral morphine generally available in the public health system
Categorical
2.3.8) Palliative care in the public health system
No availability of community or home-based palliative care in the public health system = 0Availability of community or home-based palliative care in the public health system = 1
General availability of palliative care in the public health system
Categorical

15Index of Cancer PreparednessMethodology report
© The Economist Intelligence Unit Limited 2019
Table 2: Indicator framework detail, showing domain, sub-domain and indicators. The scoring system is described and the indicator definition. Type of indicator is qualitative, quantitative or categorical
Domain Sub-domain/Indicator Scoring system Definition Type
2.4) Clinical guidelines
2.4.1) National guidelines for NCDs management through a primary care approach
Absence of evidence-based national guidelines for the management of major NCDs through a primary care approach = 0Presence of evidence-based national guideline for the management of major NCDs through a primary care approach = 1
Existence of evidence-based national guidelines/protocols/standards for the management of the four main NCDs—cardiovascular disease, diabetes, cancer and chronic respiratory diseases
Categorical
2.4.2) National evidence-based guidelines for cancer care
No evidence-based guidelines exist in the country for the four priority cancers below = 0Guidelines exist for only one of the below = 1Guidelines exist for two to three of the below = 2Guidelines exist for all of the below = 3
a) Breast cancerb) Lung cancerc) Prostate cancerd) Colorectal cancer
Existence of up to date (<five years) national evidence-based guidelines for priority cancers
Qualitative
2.5) Patient-centred care
2.5.1) Co-ordinated and integrated cancer care with multidisciplinary teams
There are no national policies for coordinated and integrated care = 0Existence of national policies for co-ordinated and integrated cancer care with multidisciplinary teams = 1
National policies or recommendations for co-ordinated and integrated cancer care with multidisciplinary teams
Qualitative
2.5.2) Cancer survivorship and rehabilitation
There are no national clinical guidelines for long-term follow up and rehabilitation = 0Existence of one of the below = 1Existence of two of the below = 2
a) Existence of clinical guidelines for long-term follow up and preventive care for cancer survivors b) Existence of national policies or programmes for rehabilitation and return to work
Existence of national clinical guidelines for long-term follow up and rehabilitation
Qualitative
2.5.3) Patient organisations There are no patient organisations = 0Only one of the below = 1Two of the below = 2
a) Existence of at least one national cancer patient support organisation b) Patients'/Patient organisations' involvement in cancer policy development and decision-making
Existence and role of patient organisations Qualitative

16Index of Cancer Preparedness
Methodology report
© The Economist Intelligence Unit Limited 2019
Table 2: Indicator framework detail, showing domain, sub-domain and indicators. The scoring system is described and the indicator definition. Type of indicator is qualitative, quantitative or categorical
Domain Sub-domain/Indicator Scoring system Definition Type
3) Health system and governance
3.1) Political will
3.1.1) General government expenditure on health: percentage of total government expenditure, 10-year growth
N/A Composite score based on ten-year average of—and average annual growth rate in—government expenditure on health as a share of government expenditure
Quantitative
3.1.2) Change in out-of-pocket expenditure over ten years
N/A Change in out-of-pocket expenditure as a percentage of current health expenditure over ten years
Quantitative
3.1.3) Universal health coverage of essential health services
N/A Coverage of essential health services (defined as the average coverage of essential services based on tracer interventions that include reproductive, maternal, newborn and child health, infectious diseases, NCDs, and service capacity and access, among the general and the most disadvantaged population)
Quantitative
3.1.4) Health technology assessment (HTA)
No HTA system = 0Existence of HTA organisation independent from payers and providers = 1Legislative requirement for HTA results to be considered in decision-making = 2
Existence of HTA system Qualitative
3.2) Infrastructure
3.2.1) Surgeons density N/A Number of licensed qualified surgeons actively working (per 1,000 population)
Quantitative
3.2.2) Skilled health professionals density
N/A The total number of physicians, nursing and midwifery personnel per 10,000 population
Quantitative
3.3) Intersectoral action and governance
3.3.1) Intersectoral action for health and health equity
There are no intersectoral policies for health = 0Existence of national policies for health that address at least two priority determinants of health = 1
Existence of national policies for health and well being that address at least two priority determinants of health (and involve at least two sectors) in target populations
Qualitative
3.3.2) Control of corruption N/A Control of corruption—capturing perceptions of the extent to which public power is exercised for private gain, including both petty and grand forms of corruption, as well as "capture" of the state by elites and private interests
Quantitative

17Index of Cancer PreparednessMethodology report
© The Economist Intelligence Unit Limited 2019
• Economist Intelligence Unit secondary research
• Interviews
• WHO
• IARC, Global Cancer Observatory
• Cancer Atlas
• World Bank
• IHME, Global Health Data Exchange (GHDx)
• CONCORD
Main data sources

18Index of Cancer Preparedness
Methodology report
© The Economist Intelligence Unit Limited 2019
• Alan Lovell, senior associate, EIU Healthcare
• Anelia Boshnakova, senior policy analyst, EIU Healthcare
• Camilo Guerrero, consultant, EIU Public Policy, Economics and Politics
• Chrissy Bishop, senior analyst, EIU Healthcare
• Darshni Nagaria, analyst, EIU Healthcare
• Shreya Patel, analyst, EIU Healthcare
• Zain Taha, analyst, EIU Healthcare
Research team

19Index of Cancer PreparednessMethodology report
© The Economist Intelligence Unit Limited 2019
1. WHO. Cancer prevention and control in the context of an integrated approach. Geneva: WHO, 2017. Available from: http://apps.who.int/medicinedocs/documents/s23233en/s23233en.pdf.
2. UICC. World cancer declaration: progress report 2016. Geneva: UICC, 2016. Available from: https://www.uicc.org/sites/main/files/atoms/files/UICC_WorldCancerDeclaration_Progress_Report_2016_Book.pdf.
3. Fitzmaurice C, Akinyemiju TF, Al Lami FH, et al. Global, Regional, and National Cancer Incidence, Mortality, Years of Life Lost, Years Lived With Disability, and Disability-Adjusted Life-Years for 29 Cancer Groups, 1990 to 2016: A Systematic Analysis for the Global Burden of Disease Study. JAMA Oncol. 2018.
4. IARC. World Cancer Report 2014 [Internet]. Lyon: IARC; [cited August 20th 2018]. Available from: http://publications.iarc.fr/Non-Series-Publications/World-Cancer-Reports/World-Cancer-Report-2014.
5. Albreht T, Kiasuwa R, Van den Bulcke M. European Guide on Quality Improvement in Comprehensive Cancer Control. Ljubljana: National Institute of Public Health, 2017. Available from: https://cancercontrol.eu/archived/uploads/images/Guide/pdf/CanCon_Guide_FINAL_Web.pdf.
6. Albreht T, Borras J, Conroy F, et al. European Guide for Quality National Cancer Control Programmes. Ljubljana: European Partnership for Action Against Cancer (EPAAC), 2014. Available from: http://www.epaac.eu/images/WP_10/European_Guide_for_Quality_National_Cancer_Control_Programmes_EPAAC.pdf.
7. WHO. Global Action Plan for the Prevention and Control of NCDs 2013-2020. Geneva: WHO, 2013. Available from: http://apps.who.int/iris/bitstream/handle/10665/94384/9789241506236_eng.pdf;jsessionid=0591F57D5D2CB9F9A1D7D37D106BCAED?sequence=1.
8. American Cancer Society, IARC, UICC. The cancer atlas [Internet]. Atlanta (GA): American Cancer Society; [cited January 25th 2019]. Available from: http://canceratlas.cancer.org/.
9. WHO, IAEA. National cancer control programmes core capacity self-assessment tool: NCCP core self-assessment tool, 2011. Geneva: WHO. Available from: http://apps.who.int/iris/bitstream/handle/10665/44729/9789241502382_eng.pdf;jsessionid=85AF031EFB240295C5691F556FD475A5?sequence=1.
10. WHO. NCD Global Monitoring Framework: Indicator Definitions and Specifications. Geneva: WHO, 2014. Available from: http://www.who.int/nmh/ncd-tools/indicators/GMF_Indicator_Definitions_FinalNOV2014.pdf?ua=1.
11. WHO. Global Health Observatory data repository [Internet]. Geneva: WHO; [cited January 25th 2018]. Available from: http://apps.who.int/gho/data/node.home.
12. WHO. Global Health Expenditure Database [Internet]. Geneva: WHO; [cited January 25th 2018]. Available from: http://apps.who.int/nha/database.
13. WHO. WHO report on the global tobacco epidemic 2017 [Internet]. Geneva: WHO; [cited January 25th 2018]. Available from: https://www.who.int/tobacco/global_report/2017/en/.
14. WHO. Cancer country profiles 2014 [Internet]. Geneva: WHO; [cited January 25th 2018]. Available from: https://www.who.int/cancer/country-profiles/en/.
15. WHO. Health Technology Assessment Country profile [Internet]. Geneva: WHO; [cited January 25th 2018]. Available from: https://www.who.int/health-technology-assessment/country-profile/en/.
References

20Index of Cancer Preparedness
Methodology report
© The Economist Intelligence Unit Limited 2019
16. World Bank Group. The Worldwide Governance Indicators [Internet]. Washington, DC: World Bank Group; [cited January 25th 2019]. Available from: http://info.worldbank.org/governance/wgi/#home.
17. IARC. Global Cancer Observatory: Cancer Today [Internet]. Lyon: IARC; [cited January 25th 2019]. Available from: https://gco.iarc.fr/today/data-sources-methods.
18. Institute for Health Metrics and Evaluation. Global Health Data Exchange [Internet]. Seattle, WA: Institute for Health Metrics and Evaluation (IHME); [cited January 25th 2019]. Available from: http://ghdx.healthdata.org/.
19. Allemani C, Matsuda T, Di Carlo V, et al. Global surveillance of trends in cancer survival 2000–14 (CONCORD-3): analysis of individual records for 37 513 025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries. The Lancet. 2018;391(10125):1023-75.
20. Rosenblatt E, Izewska J, Anacak Y, et al. Radiotherapy capacity in European countries: an analysis of the Directory of Radiotherapy Centres (DIRAC) database. Lancet Oncol. 2013;14(2):e79-86.
21. UICC. Cancer registries: Why, what and how? Geneva: UICC. Available from: https://www.uicc.org/sites/main/files/atoms/files/UICC%20Cancer%20Registries-%20why%20what%20how.pdf.
22. Mathew A. Global Survey of Clinical Oncology Workforce. J Glob Oncol. 2018(4):1-12.
23. Romero Y, Trapani D, Johnson S, et al. National cancer control plans: a global analysis. Lancet Oncol. 2018;19(10):e546-e55.

LONDON20 Cabot SquareLondon, E14 4QWUnited KingdomTel: (44.20) 7576 8000Fax: (44.20) 7576 8500Email: [email protected]
NEW YORK750 Third Avenue5th FloorNew York, NY 10017United StatesTel: (1.212) 554 0600Fax: (1.212) 586 1181/2 Email: [email protected]
HONG KONG1301 Cityplaza Four12 Taikoo Wan RoadTaikoo ShingHong KongTel: (852) 2585 3888Fax: (852) 2802 7638 Email: [email protected]
GENEVARue de l’Athénée 321206 GenevaSwitzerlandTel: (41) 22 566 2470Fax: (41) 22 346 93 47Email: [email protected]
DUBAIOffice 1301aAurora TowerDubai Media CityDubaiTel: (971) 4 433 4202Fax: (971) 4 438 0224Email: [email protected]
SINGAPORE8 Cross Street#23-01 Manulife TowerSingapore 048424Tel: (65) 6534 5177Fax: (65) 6534 5077 Email: [email protected]