Increasing the Affordability of Health Care Revised 7/2007
56
Increasing the Affordability of Health Care Revised 7/2007 1
description
Increasing the Affordability of Health Care Revised 7/2007. 1. Total National Health Expenditures, 1980 – 2005 (1). Spending on health care is on the rise. Source: Centers for Medicare & Medicaid Services, Office of the Actuary. Data released January 8, 2007. - PowerPoint PPT Presentation
Transcript of Increasing the Affordability of Health Care Revised 7/2007

Increasing the Affordabilityof Health Care
Revised 7/2007
1

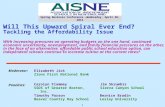
Total National Health Expenditures, 1980 – 2005(1)
Inflation Adjusted(2)
$200
$400
$600
$800
$1,000
$1,200
$1,400
$1,600
$1,800
$2,000
$2,200
80 81 82 83 84 85 86 87 88 89 90 91 92 93 94 95 96 97 98 99 00 01 02 03 04 05
Bill
ions
Source: Centers for Medicare & Medicaid Services, Office of the Actuary. Data released January 8, 2007.(1) CMS completed a benchmark revision in 2006, introducing changes in methods, definitions and source data that are
applied to the entire time series (back to 1960). For more information on this revision, see http://www.cms.hhs.gov/NationalHealthExpendData/downloads/benchmark.pdf.
(2) Expressed in 1980 dollars; adjusted using the overall Consumer Price Index for Urban Consumers.
Spending on health care is on the rise.
2

National Expenditures for Health Services and Supplies(1) by Category, 1980 and 2005(2)
Hospital Care, 32.9%Hospital Care, 43.2%
Physician Services, 22.6%
Physician Services, 20.1%Other Professional(4), 7.7%
Other Professional(4), 7.2% Home Health Care, 2.5%Home Health Care, 1.0% Prescription Drugs, 10.8%Prescription Drugs, 5.1%
Other Medical Durables and Non-durables, 3.1%Other Medical Durables and Non-durables, 5.8%
Nursing Home Care, 6.5%Nursing Home Care, 8.1%
Other(3), 13.8%Other(3), 9.4%
1980 2005
Source: Centers for Medicare & Medicaid Services, Office of the Actuary. Data released January 8, 2007.(1) Excludes medical research and medical facilities construction.(2) CMS completed a benchmark revision in 2006, introducing changes in methods, definitions and source data that are
applied to the entire time series (back to 1960). For more information on this revision, see http://www.cms.hhs.gov/NationalHealthExpendData/downloads/benchmark.pdf.
(3) “Other” includes net cost of insurance and administration, government public health activities, and other personal health care.
(4) “Other professional” includes dental and other non-physician professional services.
$234.0B $1,860.9B
However, hospitals are a shrinking share of the growing spending pie.
3

The U.S. is the only country where health care accounts for more than 13 percent of the GDP, spending 16.5% in 2006.
4

21%27%
31%
19%
10%
17%
20%
15%
13%
19%
Total Less than $35,000 $35,000– $49,999 $50,000– $74,999 $75,000 or more
Very Serious Somewhat Serious
38%
47%50%
34%
23%
Percent of Adults Facing Serious Problems Paying for Insurance in the Past Two Years, by Income Level, 2006
Fifty percent of adults with incomes less than $50,000 have experienced problems paying for insurance in the past two years…
Note: Percent values on the top of each bar reflect the sum of the values within each bar.Source: The Commonwealth Fund (2006) Public Views on Shaping the Future of the U.S. Health Care System 5

Percent of Firms Offering Health Benefits, 2002 and 2006
66%
58%
70%
95%98%
61%
48%
73%
87%92%
98%
86%
All Firms 3-9 10-24 25-49 50-199 200 or More
Number of Workers at Firm
2002 2006
Source: “Employer Health Benefits 2006 Annual Survey,” (#7527), The Henry J. Kaiser Family Foundation and Health Research and Educational Trust, September 2006
…and may small businesses do not even offer coverage.
6

These factors contribute to a growing number of uninsured.
Number and Percent Uninsured, 1985 – 2005
0
5
10
15
20
25
30
35
40
45
50
85 86 87 88 89 90 91 92 93 94 95 96 97 98 99 00 01 02 03 04 05
Num
ber
of U
nins
ured
(M
illio
ns)
0%
2%
4%
6%
8%
10%
12%
14%
16%
18%
Per
cent
of
Tot
al P
opul
atio
n
Number Percent
Source: US Census Bureau, Income, Poverty, and Health Insurance Coverage in the United States: 2005. Data released August 2006. Table 8. People With or Without Health Insurance Coverage by Selected Characteristics: 2004 and 2005.Link: http://pubdb3.census.gov/macro/032006/health/h01_001.htm.(1) 2004 and 2005 figures reflect revised estimates released by the Census Bureau on March 23, 2007.
7

Increased spending is linked to several factors.
1. Increased demand for care– Demographics– Health status– Technology: health care can do more things for
more people
2. Rising costs to provide care– Labor shortage– Technology– Regulatory burden– For private sector, government underfunding
8

Drivers of DemandDemographics
9

The aging of the population is driving up demand for health care.
Source: US Census Bureau
US Population Trends and Projections by Age,1980 - 2050
0
50,000
100,000
150,000
200,000
250,000
300,000
350,000
400,000
450,000
1980 1990 2000 2010 2020 2030 2040 2050
Tho
usan
ds
20 - 64
65 - 84
0 - 19
85 and over
10

With the aging of the Baby Boomer population, hospital admissions of Boomers will more than double…
23.025.5 24.0 23.0
8.78.9
16.522.9
0
5
10
15
20
25
30
35
40
45
50
2004 2010* 2020* 2030*
YEAR
Ho
spit
al A
dm
issi
on
s
(Mill
ion
s)
Non-Boomer Adults Boomers
* Projected.1 Non-Boomer adults indicates non-Boomers over the age of 15.Source: “When I’m 64”, American Hospital Association, May 2007. FCG projections based on National Center for Health Statistics, National Hospital Discharge Survey 2004, May 2006
11
Number of hospital admissions

…leading to a majority of hospital patients being over 65.
Hospital Admissions(2004 Estimate)
Under 6562%
Over 6538%
* Projected. Source: “When I’m 64”, American Hospital Association, May 2007. FCG projections based on National Center for Health Statistics, 2004 National Hospital Discharge Survey, May 2006
Hospital Admissions*(2030 Projection)
Over 6556%
Under 6544%
Total Hospital Admissions in 200435 Million Total Hospital Admissions in 2030*
49 Million
12

Physician office visits for adults will number more than one billion by 2020.
427 477591
769
295302
415
547
0
200
400
600
800
1,000
1,200
1,400
2004 2010* 2020* 2030*
YEAR
Off
ice
Vis
its
(Mil
lio
ns)
Non-Boomer Adults Boomers
* Projected.1 Non-Boomer adults indicates non-Boomers over the age of 15.Source: “When I’m 64”, American Hospital Association, May 2007. FCG projections based on National Center for Health Statistics, National Ambulatory Care Survey 2004, June 2006
13
Number of Physician Office Visits

INSERT YOUR DATA HERE
• INSERT ANY AGING OR DEMOGRAPHIC CHANGES YOU ARE EXPECTING IN YOUR COMMUNITY
14

Drivers of DemandHealth Status
15

We have a rising number of people with chronic conditions.
0
20
40
60
80
100
120
140
160
180
1995 2000 2005 2010 2015 2020 2025 2030
42%
43%
44%
45%
46%
47%
48%
49%
50%
Population Percent of Population
Number and Percent of Americans with Chronic Medical Conditions,*1995 – 2030
Mill
ions
of
Pe
ople
Source: Adapted from Partnership for Solutions, Johns Hopkins University, Chronic Conditions: Making the Case for Ongoing Care, December 2002
Per
cen
t of
Tot
al
Pop
ula
tion
*Values for 2005 to 2030 are projections.
16

Lifestyle factors are contributing to the rising levels of chronic illness.
Prevalence of Diabetes(1) and Obesity(2), U.S. Population, 1990-2005
Diabetes
Obesity
0%
5%
10%
15%
20%
25%
90 91 92 93 94 95 96 97 98 99 00 01 02 03 04 05
Per
cent
age
of P
opul
atio
n
Source: Centers for Disease Control and Prevention. (1) Diabetes is age-adjusted prevalence from the National Diabetes Surveillance System.
http://www.cdc.gov/diabetes/statistics/prev/national/index.htm(2) Obesity is median % of individuals 18 years or older reporting body mass index greater than 30 kg/m2 in states,
DC, and the U.S. territories reporting data to the Behavioral Risk Factor Surveillance System. http://apps.nccd.cdc.gov/brfss/Trends/trendchart.asp?qkey=10010&state=US
17

By 2030, 37 million Boomers will be managing more than one chronic disease.
18

On average, the cost of health care for an individual with more than 5 chronic conditions is nearly 15 times that of an individual with no chronic conditions.
19

INSERT YOUR DATA HERE
• INSERT DATA ON CHRONIC CONDITIONS SPECIFIC TO YOUR COMMUNITY.
• In addition to your own internal data that can be gleaned from the medical records, visit www.cdc.gov for state level data on chronic disease from the BRFSS survey.
20

Drivers of DemandTechnology:
Health care can do more things for more people
21

Technology Medicare Costs
Drug-eluting coronary stents $2 – 4 B
ICD for sudden death prophylaxis $1 – 3 B
PET for Alzheimer’s disease $1 B
Verteporfin for macular degeneration $750 M
Left-ventricular assist devices $1 – 7 B
Source: Adapted from Neumann PJ, Medicare National Coverage Decisions: How is CMS Doing? Presented at National Health Policy Conference, February 2005
Projected Annual Costs of Recent Technology Related Medicare Coverage Expansions
Each year we can do more things for more people, but innovations are costly.
22

People demand innovations in care because they save lives.
0
50
100
150
200
250
300
350
400
1980 1990 2000
Mortality from Heart Attacks in Relation to Advances in Care
1980s
Blood ThinnersBeta Blockers
CABG
Metal stents
ThrombolyticsImplantable defibrillators
Drug-eluting stents
1990s 2000s
StatinsACE inhibitors
Dea
th
Rat
e p
er 1
00,0
00
Source: www.cdc.gov/nchs; The Value of Investment in Health Care 23

Rising Costs of Providing CareLabor Shortage
24

Percent of Hospital Costs(1) by Type of Expense, 3Q06
Source: AHA analysis of Centers for Medicare and Medicaid Services data, using base year 2002 weights.(1) Does not include capital.(2) Includes postage and telephone expenses.
(2)
Wages and Benefits, 59.6%
Other Services, 19.6%
Prescription Drugs, 6.2%
Other Products(e.g., Food,
Medical Instruments),
14.6%
Health care is very labor intensive, but…
25

Vacancy Rates for Selected Hospital Personnel, December 2006
…hospitals also face workforce shortages in key care-giving professions…
8.1% 8.1% 8.0%
6.6%5.9% 5.9%
11.4%
Therapists (ST, OT, PT)
RegisteredNurses
Pharmacists NursingAssistants
LPNs LaboratoryTechnicians
ImagingTechnicians
Source: 2007 AHA Survey of Hospital LeadersNote: 116,000 vacancies is a national estimate created by extrapolating the vacancy rate to all 5,000 community hospitals in 2005. ST: Speech Therapist, OT: Occupational Therapist, PT: Physical Therapist.
116,000 RN Vacancies*
26

National Supply and Demand Projections for FTE RNs,2000 – 2020
Source: National Center For Health Workforce Analysis, Bureau of Health Professions, Health Resources and Services Administration, 2004. Link: http://bhpr.hrsa.gov/healthworkforce/reports/rnpopulation/preliminaryfindings.htm.
RN FTE Supply
RN FTE Demand
1,500
1,700
1,900
2,100
2,300
2,500
2,700
2,900
2000 2005 2010 2015 2020
FT
Es
(Th
ou
san
ds)
Shortage of over 1,000,000 nurses in 2020
A continuing and growing workforce shortage is a key driver of the increased costs of RNs…
27

…as well as physicians.
12.7 15.919.7
23.8
1315
243.4
7.1
12.1
4.3
6.3
9.2
4.4
5.6
7.4
190.22.7
9.9
0
10
20
30
40
50
60
70
80
90
2005 2010* 2015* 2020*
Nu
mb
er
of
Ph
ys
icia
ns
(Th
ou
sa
nd
s)
Orthopedic Surgery
Cardiology
Other Medical Specialties
Gerontology
General Surgery
* Projected.Sources: Physician Supply and Demand: Projections to 2020, HRSA, October 2006“Research Shows Rapid Decline in Geriatric Medicine Students,” Press Release, University of Cincinnati, April 4, 2007“Aging Boomers Face a Doctor Shortage,” CBS News, March 4 2003
28
Physician Shortage for Select Specialties

Rising Costs of Providing CareTechnology, Regulatory Burden and
Government Underfunding
29

Hospitals face significant increases in the costs of caring for patients…
9.3%
8.7%
9.0%
9.3%
10.3%
8.8%
Rural Hospitals
Urban Hospitals
All Hospitals
MedicalSupplies/Devices
Pharmaceuticalproducts
Percent Change in Hospital Expenses for Pharmaceuticals and Medical Supplies/Devices, 2004 to 2005
Source: AHA 2006 Survey of Hospital Leaders30

…driven in part by new technology that increases costs for providing the same service.
$500
$5,000
$2,300
Cardiac BalloonCatheter
Stent Coated Stent
Stents: The Rising Costs of Technological Development
Source: University HealthSystem Consortium31

WHO REGULATES HOSPITALS
IRS EPA FTC FCC
FBI
HHS/HRSA HHS/NIOSH JCAHO NRC DOL
SEC
OPO’s
FAA
DEA
Regional Home Health Intermediaries
DME Regional Contractors
Treasury
DOJ
OSHA
DOT
FDA
Regional Offices Intermediaries Carriers PRO’s
PRRB
Medicare Integrity Program Contractors
Congress
Federal Circuit Courts Supreme Court
Departmental Appeals
OIG
State
Survey & Certification
Courts
Attorneys General
Medicaid
Health Boards
Medical Boards
Local Governments
Licensure
Hospitals
CMS
Regulatory burden contributes to rising costs for hospitals and the system as a whole.
32

-15.5
-1.9
-2.6-2.1
-2.3
-5.0
-9.8
-15
-8.1
-3.4-2.4-1.4
4.32.3
-7.1
-1.6 -1.4
-$24-$22
-$20-$18
-$16-$14
-$12-$10
-$8-$6
-$4-$2
$0$2
$4$6
Hospital Payment Shortfall Relative to Costs Medicare and Medicaid, 1997 – 2005, (in billions of dollars)
1997 1998 1999 2000 2001 2002 2003
Medicare
MedicaidTotal 2005 Medicaid and Medicare Shortfall of $25.4 Billion
Source: AHA Annual Survey
Bill
ion
s o
f D
olla
rs
For the private sector, government underfunding adds to costs…
2004 2005
33

…as do rising levels of uncompensated care, contributing to…
$18.5
$20.7$21.6 $21.5 $22.3
$24.9$26.9
$28.8
$19.0
1997 1998 1999 2000 2001 2002 2003 2004 2005
Aggregate Hospital Uncompensated Care Costs,1997-2005(in billions)
Source: AHA Annual Survey34

6.7%
4.0%
-1.7%
5.3%
3.7%
-2.0%
1997
2005
Source: AHA Annual Survey
Total, Operating and Patient Care Margins,1997 (pre-BBA) vs. 2005
Total Margin Operating Margin
Patient Care Margin
…decreasing hospital margins…
35

Operating Margins of the Top Insurers, 2003 – 2005
Source: Hoovers. Data from January 2007. Link: www.hoovers.com.(1) 2004 operating margin data for WellPoint include both pre- and post-merger data for the merger with Anthem in November 2004
8% 8%
10%9%
10%
9%
11%
13%
11%
9%
12%11%
0%
2%
4%
6%
8%
10%
12%
14%
Aetna WellPoint UnitedHealth Group Cigna
Op
era
tin
g M
arg
in
2003 2004 2005 (1)
…while margins of top insurers are in the double digits.
36

“More can and should be done to make care more affordable.
With costs of caring on the rise and demand increasing in an ever changing environment we
must seize opportunities to make care more affordable.”
37

A New Lens is Needed…
38

The increase in spending on health care is a frequent topic of debate, but the value of this investment is seldom part of the discussion.
CBO Issues Warning on Rising Health Care Costs
Senate Republicans in Albany Eye Big Medicaid Cuts
Medicare Revamp Fails to Cure Angst Over Costs
39

Research indicates significant health gains have accompanied increased spending.
Since 1980, per capita expenses up $2,254, but:• Overall death rate down 16%• Life expectancy from birth up by 3.2 years• Disability rates down 25% for people over 65• 56% fewer days spent in the hospital
Health gains of $2.40 to $3.00 per dollar invested
40

Advances in health care have lead to fewer deaths and less disability.
206206millionmillionmoremore
days indays inhospitalhospital
2.32.3millionmillionmoremore
disableddisabledpersonspersons
470,000470,000moremore
deathsdeaths
41
Where we would be in 2000 without advances since 1980?

Death rates for key diseases have declined dramatically.
345.2
249.6
186.9
20.7
96.2
65.360.8
18.1 25.225.431.832.3
1980 1990 2000
Death Rates for Key Conditions Studied1980-2000
Source: Health, United States 2002
Heart Attack
Type 2Diabetes
Stroke
BreastCancer
42

America’s health care system is at a crossroads, and hospitals are part of the solution.
43

Key opportunities exist to increase affordability.
• Focus on wellness– Go beyond the medical model of care to look at wellness
and prevention
• Better manage chronic disease– Anticipate the wave of the Boomers and the growing
incidence of chronic disease
• Improve care delivery– More demand for services requires new approaches to
care delivery
• Increase transparency of quality performance• Better understand and reduce duplication of services• Speed adoption of IT
44

Focus on Wellness
Promote preventive services
Reward personal participation
Reward healthy behaviors
45

More employers are investing in wellness.
• Individuals with healthy lifestyles typically are:• More productive• File fewer medical claims• Have lower medical costs
• Research shows a $3 to $1 return on investment
• Prevention/detection demonstrates success in
cancer and heart disease
46

Research has shown that a focus on wellness is cost effective.
-30%-28%
-27%
-35%
-25%
-15%
-5%
Health Costs AbsenteeismWorkers' Comp./DisabilityManagement Claims Costs
Ave
rag
e C
han
ge
Average Percent Change in Employers’ Costs Resulting from Workplace Health Promotion and Wellness Programs
Source: Chapman, L. (2003). Meta-evaluation of Worksite Health Promotion Economic Return Studies. Art of Health Promotion Newsletter, 6(6).
47

Employers also believe financial incentives could work.
78%
79%
80%
81%
82%
83%
84%
85%
2005 2007
“Money is not enough so employers must build something into the plan such as tools and health coaches.” – Midwest Business Group on Health.
Source: PricewaterhouseCoopers Management Barometer Survey
Do you believe that providing financial incentives to employees for participating in healthy lifestyle programs will reduce your company’s health care costs?
48

Focus on wellness
• INSERT INFORMATION ON THE WELLNESS PROGRAMS YOU ARE INVOLVED IN…
For additional examples or ideas, visit www.aha.org/communityconnections
49

Better manage chronic disease
• INSERT INFORMATION ON YOUR EFFORTS TO MANAGE CHRONIC DISEASE IN YOUR COMMUNITY – Its helpful to include data that show results.
(i.e. lower admissions of asthma or improved lab results of those participating in a program)
50

Improve care delivery
• INSERT INFORMATION ON YOUR EFFORTS TO IMPROVE CARE DELIVERY– Its helpful to include data that show results.
(i.e. wait times in the ED, faster discharge times, quicker bed turn over)
– Demonstrated improved patient satisfaction levels (i.e. survey results)
51

Increase transparency of quality performance
• INSERT INFORMATION ON YOUR HQA QUALITY SCORES or OTHER BENCHMARK DATA YOU USE TO ASSESS YOUR QUALITY PERFORMANCE
52

Better understand and reduce duplication
Following care guidelines and protocols, clinicians could help reduce readmission rates to hospitals and lessen complications.
INSERT INFORMATION ON WAYS YOUR ORGANIZATION IS ADDRESSING THIS GOAL
53

Speed adoption of IT
Today’s health care system is choked with paper. Health care will be more affordable if we spend more time at the bedside and less on paperwork.
INSERT INFORMATION ON WAYS YOUR ORGANIZATION IS ADDRESSING THIS GOAL
54

Broadening of the digital backbone in healthcare
• “Widespread adoption of electronic medical records and other health information technology is estimated
to save $162 billion a year by improving care management, reducing preventable medical errors,
lowering death rates from chronic diseases, and reducing the number of employee sick days.”
Payer benefitsDrops in administrative costsMore accurate forecasting
Provider benefitsReduced duplicate testingReduced adverse drug reactions
Source: Pricwaterhouse Coopers, June 2007 55

Keeping health care affordable will involve every segment of the health care system – insurers, hospitals, business, physicians, nurses, employers and individuals.
We can and must
do this together!
56