
Incorporating OMM to Enhance Your Clinical Practice...
21
Incorporating OMM to Enhance Your Clinical Practice: Diagnostic and Treatment approach to the extremities To Shan Li, D.O. Assistant Professor 3/1/14
Transcript of Incorporating OMM to Enhance Your Clinical Practice...

Incorporating OMM to Enhance Your Clinical Practice:
Diagnostic and Treatment approach to the extremities
To Shan Li, D.O. Assistant Professor
3/1/14

Lower Extremity
• Hip • Thigh • Knee • Leg • Ankle • Foot

General Considerations
Trauma
• Strain • Sprain • Fracture • Dislocation • Repetitive use • “itis”
Non-Trauma • Infection • Malignancy • Inflammatory • Visceral • Skin • Neurologic
– Referred – Neuropathy
• Vascular

Where’s the osteopathic component?
• It exists in all of the above – Joint mechanics, Posture (Structural) – Autonomic (Neurologic)
• Upper Ext: T5 to T7 • Lower Ext: T10 to L2-3
– Diaphragms (Circulatory/Lymphatic) – Ergonomics, Functional (Behavioral) – Disease states (Metabolic)

What are the essentials of an osteopathic approach?
• Localize the complaint • Know the anatomy
– landmarks – functional anatomy
• Diagnose the underlying cause – Musculoskeletal
• Spasm or myofascial strain – Tender point, Trigger point – Interosseous membrane
– Neurologic • Sympathetics • Chapman point • Nerve impingement
What are the essentials of an osteopathic approach?
• Diagnose the underlying cause – Circulatory/Lymphatic
• Vascular supply and drainage
– Metabolic • Improve state of tissue • Decrease work of the body

Clinical Tips
• Think broadly • Be flexible • Diagnose SD and understand its relevance
– Palpate structures – Assess motions

Hip
• Flexion • Extension • Internal rotation • External rotation • Adduction • Abduction
• 2-3 x body weight with walking
Psoas
• Connects to the hip • Thomas test to check for psoas tightness (can
restrict hip extension)

Hip & Thigh- Some considerations • Inguinal ligament
– Can treat with direct MFR using fingertips into inguinal ligament
• Greater trochanter – Can check for tender point
• Quadriceps • Iliotibial band
– Check for tension and Chapman points

Hamstrings
• Evaluate as part of straight leg raise • Compare left and right

Q-angle of the knee
• Increased Q-angle introduces mechanical strain into the knee
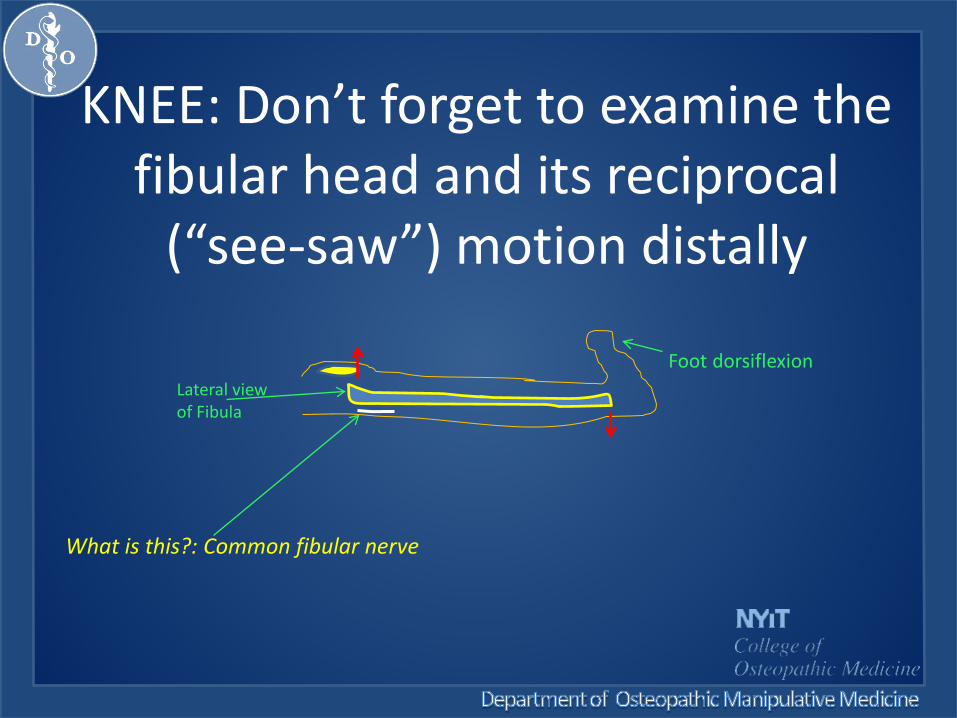
KNEE: Don’t forget to examine the fibular head and its reciprocal
(“see-saw”) motion distally
Foot dorsiflexion Lateral view of Fibula
What is this?: Common fibular nerve

The fibular nerve is behing the fibula head
• Common Fibular (peroneal) nerve – Directly posterior to
fibular head – A posterior fibular head
or fracture may cause foot drop

Tibiofibular Joint
• The fibular head glides anteriorly with pronation (dorsiflexion, eversion and external rotation) of the foot • The fibular head glides posteriorly with supination (plantarflexion, inversion and internal rotation) of the foot

Knee motion • Primary motion is flexion and extension, so
check for restrictions in these motions – Unable to flex knee normally = knee flexion
restriction, or alternatively, knee extension dysfunction (extended knee is also acceptable terminology)
– Unable to extend knee normally = knee extension restriction, or alternatively, knee flexion dysfunction (flexed knee is also acceptable)
• Can test for medial and lateral glide of the patella

Ligaments of the Knee
• Anterior Cruciate ligament • Posterior Cruciate ligament • Medial Collateral ligament • Lateral Collateral ligament • Patella ligament (aka Patella tendon)

Tibia
• Compare the anterior tibial tubercle and how it relates to the center of the patella
• Common tibial dysfunctions are – Internal tibial torsion (tibial tubercle is more
medial relative to patella) – External tibial torsion (tibial tubercle is more
lateral relative to patella)

Ankle • Inversion sprains are common • Check for ankle motion
– Dorsiflexion (if restricted = ankle dorsiflexion restriction or ankle plantarflexion dysfunction)
– Plantarflexion (if restricted = ankle plantarflexion restriction or ankle dorsiflexion dysfunction)
– Inversion (if restricted = ankle inversion restriction or ankle eversion dysfunction)
– Eversion (if restricted = ankle eversion restriction or ankle inversion dysfunction)

Deciding to treat
• Name the somatic dysfunction? • What is its role?
– Primary vs. Secondary
• What model do you have in mind? – What is the intended purpose of treatment
• Direct vs. Indirect • Reassess

Techniques/Regions to consider • Spine (esp. thoracic, lumbar) • Thoracic inlet • Pectoral traction • Ribs & Diaphragm • Pelvis & Sacrum • Limb muscles and joints (hip, knee, ankle,
foot) – ME, MFR, Articulatory, CS
• Interosseous membrane • Pedal Pump


















