Incidental Subcortical Lesions Identified on...
9
1090 Incidental Subcortical Lesions Identified on Magnetic Resonance Imaging in the Elderly. II. Postmortem Pathological Correlations ISSAM A. AWAD, M.D.,* PETER C. JOHNSON, M.D.,t ROBERT F. SPETZLER, M.D.,* AND JOHN A. HODAK, M.D.t SUMMARY The pathological correlates of subcortical lesions noted on magnetic resonance imaging (MRI) in the elderly are not known. Postmortem in vitro proton MRI was performed on the brains of seven consecutive elderly patients dying of nonneurologic causes. Scans were done in the fresh and fixed states with the specimen immersed in saline and formaldehyde respectively. A 1.5 Tesla superconductive system was used with a multiple spin-echo protocol generating T 2 weighted images. Subcortical MRI lesions were localized in three dimensions and identified at brain cutting. In addition, pathological correlations were obtained from an eighth patient who underwent MRI eleven days before death. Histological examinations were performed in a blinded fashion, including control areas from the same brains. Subcortical MRI lesions were found to be associated with arteriosclerosis, dilated perivascular spaces, and vascular ectasia (p < 0.05). These histological changes were characteristic of "e~tat crible"" which, like subcortical MRI lesions, is associated with age and hypertension. Shrinkage (or atrophy) of the brain parenchyma around ectatic blood vessels would result in an extensive network of tunnels filled with extracellular water. The proton MRI signal from such areas of the brain would be increased. Gliosis and small areas of infarction occasionally coexisted with "£tat crible'," but these were not present in all areas with MRI lesions and could not be distinguished by MRI signal alone. In conclusion, clinical and pathological correlations lend support to the uniform hypothesis that MRI provides a nonspecific index of brain parenchyma! alterations caused by aging and chronic cerebro vascular disease. Stroke Vol 17, No 6, 1986 PATCHY FOCI of increased signal intensity are fre- quently identified on magnetic resonance imaging (MRI) in the elderly. '• 2 - 4 - 5 - 12 - 14 - l5 While some of these foci correspond to known or suspected pathologic pro- cesses, most are unexpected or incidental. 1 - 2415 In an accompanying report, incidental subcortical MRI lesions in the elderly were shown to be associated with age, hypertension, and a prior history of brain ischemia. 2 Occult lacunar infarctions commonly afflict the el- derly. 6 - 10 - 17 - l8 While these appear as foci of increased signal intensity on MRI, 1 - 13 it is unlikely that extensive subcortical white and gray matter infarction can occur without severe symptomatology. A chronic alteration in brain parenchyma, other than frank infarction, is therefore most likely to be responsible for the multiple, patchy, and sometimes confluent incidental lesions noted on MRI. The literature is limited regarding the pathological correlates of these lesions. Pathological correlations of incidental premortem radiological findings are difficult to perform. The pathological process often progresses to more ad- vanced and symptomatic stages before death. Further- more, it may be complicated by terminal events prior to postmortem examination. To circumvent these diffi- culties, postmortem MRI was performed in vitro on the From the Divisions of Neurological Surgery,* Neuropathology.t and Neuroradiology.t Barrow Neurological Institute, Phoenix, Arizona. Dr. Awad was the recipient of the Crile Traveling Fellowship from the Cleveland Clinic Foundation, and served as a Neurovascular Fellow at the Barrow Neurological Institute from July 1985 to June 1986. He is currently on the staff of the Division of Neurosurgery, Stanford Univer- sity School of Medicine, Stanford, California. Address correspondence to: Robert F. Spetzler, M.D., Barrow Neu- rological Institute, 350 West Thomas Road, Phoenix, Arizona. Received April 16, 1986, revision #1 accepted July 2, 1986. brains of seven consecutive elderly patients dying of nonneurologic causes and autopsied at this institution. An additional elderly patient had an MRI study eleven days before dying of acute renal failure. Incidental MRI lesions were identified in these eight cases and were localized precisely at brain cutting. Gross and histologic correlations were performed, including a blinded analysis of control areas from the same brains (areas not harboring MRI lesions). Patients and Methods The patients represented consecutive cases over 60 years of age, who died of nonneurologic causes, and who underwent postmortem examination at the Bar- row Neurological Institute. Cases with known demyel- inating disease, known structural brain pathology, or previous brain surgery were excluded. The MRI was performed eleven days premortem on case 7, and could not be repeated after death for techni- cal reasons. The case was included in this report be- cause of the severity of MRI findings, and the short interval between the scanning and death. In all other cases, the MRI was done postmortem on the fixed brain just prior to pathological examination. In addi- tion, MRI was also performed in the fresh state (prior to fixation) in cases 5 and 6. Technique of Postmortem MRI The brain was harvested at autopsy and was sus- pended from the falx cerebri in a cylindrical Tupper- ware™ container small enough to fit within the head holder compartment of the MRI system. Isotonic sa- line chilled to 4° C immersed the freshly harvested brain. Ventricular air acquired during brain removal was evacuated through the foramina of Luscka and by guest on July 2, 2018 http://stroke.ahajournals.org/ Downloaded from
Transcript of Incidental Subcortical Lesions Identified on...

1090 Incidental Subcortical Lesions Identified on MagneticResonance Imaging in the Elderly.
II. Postmortem Pathological CorrelationsISSAM A. A W A D , M.D. ,* PETER C. JOHNSON, M.D. , t ROBERT F. SPETZLER, M.D. ,*
AND JOHN A. HODAK, M . D . t
SUMMARY The pathological correlates of subcortical lesions noted on magnetic resonance imaging(MRI) in the elderly are not known. Postmortem in vitro proton MRI was performed on the brains of sevenconsecutive elderly patients dying of nonneurologic causes. Scans were done in the fresh and fixed stateswith the specimen immersed in saline and formaldehyde respectively. A 1.5 Tesla superconductive systemwas used with a multiple spin-echo protocol generating T2 weighted images. Subcortical MRI lesions werelocalized in three dimensions and identified at brain cutting. In addition, pathological correlations wereobtained from an eighth patient who underwent MRI eleven days before death. Histological examinationswere performed in a blinded fashion, including control areas from the same brains. Subcortical MRI lesionswere found to be associated with arteriosclerosis, dilated perivascular spaces, and vascular ectasia (p <0.05). These histological changes were characteristic of "e~tat crible"" which, like subcortical MRI lesions, isassociated with age and hypertension. Shrinkage (or atrophy) of the brain parenchyma around ectatic bloodvessels would result in an extensive network of tunnels filled with extracellular water. The proton MRIsignal from such areas of the brain would be increased. Gliosis and small areas of infarction occasionallycoexisted with "£tat crible'," but these were not present in all areas with MRI lesions and could not bedistinguished by MRI signal alone. In conclusion, clinical and pathological correlations lend support to theuniform hypothesis that MRI provides a nonspecific index of brain parenchyma! alterations caused by agingand chronic cerebro vascular disease.
Stroke Vol 17, No 6, 1986
PATCHY FOCI of increased signal intensity are fre-quently identified on magnetic resonance imaging(MRI) in the elderly. '•2- 4-5-12-14-l5 While some of thesefoci correspond to known or suspected pathologic pro-cesses, most are unexpected or incidental.1-2415 Inan accompanying report, incidental subcortical MRIlesions in the elderly were shown to be associatedwith age, hypertension, and a prior history of brainischemia.2
Occult lacunar infarctions commonly afflict the el-derly.6- 10-17-l8 While these appear as foci of increasedsignal intensity on MRI,1-13 it is unlikely that extensivesubcortical white and gray matter infarction can occurwithout severe symptomatology. A chronic alterationin brain parenchyma, other than frank infarction, istherefore most likely to be responsible for the multiple,patchy, and sometimes confluent incidental lesionsnoted on MRI. The literature is limited regarding thepathological correlates of these lesions.
Pathological correlations of incidental premortemradiological findings are difficult to perform. Thepathological process often progresses to more ad-vanced and symptomatic stages before death. Further-more, it may be complicated by terminal events priorto postmortem examination. To circumvent these diffi-culties, postmortem MRI was performed in vitro on the
From the Divisions of Neurological Surgery,* Neuropathology.t andNeuroradiology.t Barrow Neurological Institute, Phoenix, Arizona.
Dr. Awad was the recipient of the Crile Traveling Fellowship fromthe Cleveland Clinic Foundation, and served as a Neurovascular Fellowat the Barrow Neurological Institute from July 1985 to June 1986. He iscurrently on the staff of the Division of Neurosurgery, Stanford Univer-sity School of Medicine, Stanford, California.
Address correspondence to: Robert F. Spetzler, M.D., Barrow Neu-rological Institute, 350 West Thomas Road, Phoenix, Arizona.
Received April 16, 1986, revision #1 accepted July 2, 1986.
brains of seven consecutive elderly patients dying ofnonneurologic causes and autopsied at this institution.An additional elderly patient had an MRI study elevendays before dying of acute renal failure. IncidentalMRI lesions were identified in these eight cases andwere localized precisely at brain cutting. Gross andhistologic correlations were performed, including ablinded analysis of control areas from the same brains(areas not harboring MRI lesions).
Patients and MethodsThe patients represented consecutive cases over 60
years of age, who died of nonneurologic causes, andwho underwent postmortem examination at the Bar-row Neurological Institute. Cases with known demyel-inating disease, known structural brain pathology, orprevious brain surgery were excluded.
The MRI was performed eleven days premortem oncase 7, and could not be repeated after death for techni-cal reasons. The case was included in this report be-cause of the severity of MRI findings, and the shortinterval between the scanning and death. In all othercases, the MRI was done postmortem on the fixedbrain just prior to pathological examination. In addi-tion, MRI was also performed in the fresh state (priorto fixation) in cases 5 and 6.
Technique of Postmortem MRIThe brain was harvested at autopsy and was sus-
pended from the falx cerebri in a cylindrical Tupper-ware™ container small enough to fit within the headholder compartment of the MRI system. Isotonic sa-line chilled to 4° C immersed the freshly harvestedbrain. Ventricular air acquired during brain removalwas evacuated through the foramina of Luscka and
by guest on July 2, 2018http://stroke.ahajournals.org/
Dow
nloaded from
MRI IN THE ELDERLY: II. PATHOLOGICAL CORRELATIONSMwarf et al 1091
Magendie by tilting of the specimen. This suspensionand immersion technique was necessary to preventdistortion or deformation of the brain. The containerwas oriented in the head holder allowing the falx cere-bri to align precisely with the sagittal scanning plane.
Imaging was performed using a 1.5 Tesla supercon-ductive unit manufactured by General Electric Corpo-ration. Scanning was done in the axial, sagittal, andcoronal planes with sections 5 mm thick and a scan-ning time of approximately 45 minutes. A multipleSpin-echo protocol was used, identical to that used forroutine clinical studies. Parenchymal foci of increasedsignal intensity were identified on the T2 weightedscans, and were localized in at least two planes.
Immediately after completing the MRI scans in thefresh state, the saline solution was replaced by a phos-phate buffered saline solution containing 10% formal-dehyde and 1% methyl alcohol. The suspended brainwas fixed by immersion for 10 to 14 days.
On the day preceding brain cutting, the MRI scanwas performed on every specimen while still immersedin the formaldehyde solution. Identical scanning pro-tocols were used, identifying and localizing the MRIlesions in the fixed brain. A software localizing gridand cursors allowed the determination of precise co-ordinates for each MRI lesion and the optimal braincutting plane for each specimen.
Brain Cutting and Pathologic ExaminationThe fixed brain was cut in the appropriate plane
using the MRI images (in three dimensions) as guidingmaps. These images provided a wealth of topographic
and internal anatomic detail sufficient to guide an ex-perienced neuropathologist (PCJ) through the cuttingof the specimen. The section of interest could be veri-fied by the precise localization of anatomical structuresseen on the corresponding MRI slice, e.g. one couldeasily verify the size and shape of the ventricular sys-tem, the precise pattern of gyri and sulci, and the sizeand shape of deep structures including the fornix,thalamus, and basal ganglia, etc. Since all MRI lesionswere localized in two or more imaging planes andusually on more than one slice, they were Unlikely tobe "missed" with this anatomically guided sectioningtechnique.
Photographs of the gross sections were obtained fordocumentation of the macroscopic findings. Slices (15mm X 15 mm X 2 mm) were excised from areasharboring MRI lesions. Similar slices were excisedfrom control areas in the same brain (areas not harbor-ing MRI lesions). The control slices were preferablysampled from contralateral or homologous zones, un-less those areas also harbored MRI lesions. The sliceswere embedded in paraffin and were given a randomcode. Contiguous sections of each slice were stainedwith hematoxylin and eosin (H&E) for routine histo-logical examination, with Luxol's fast blue (LFB) formyelin, and with glial fibrillary acidic protein (GFAP)stain for astrocytes and their processes.
The coded sections were examined by a single neu-ropathologist (PCJ) in a blinded fashion. The histo-logical findings from each slice were recorded on astandardized sheet. The following specific changeswere graded as none, mild, or severe: parenchyma]
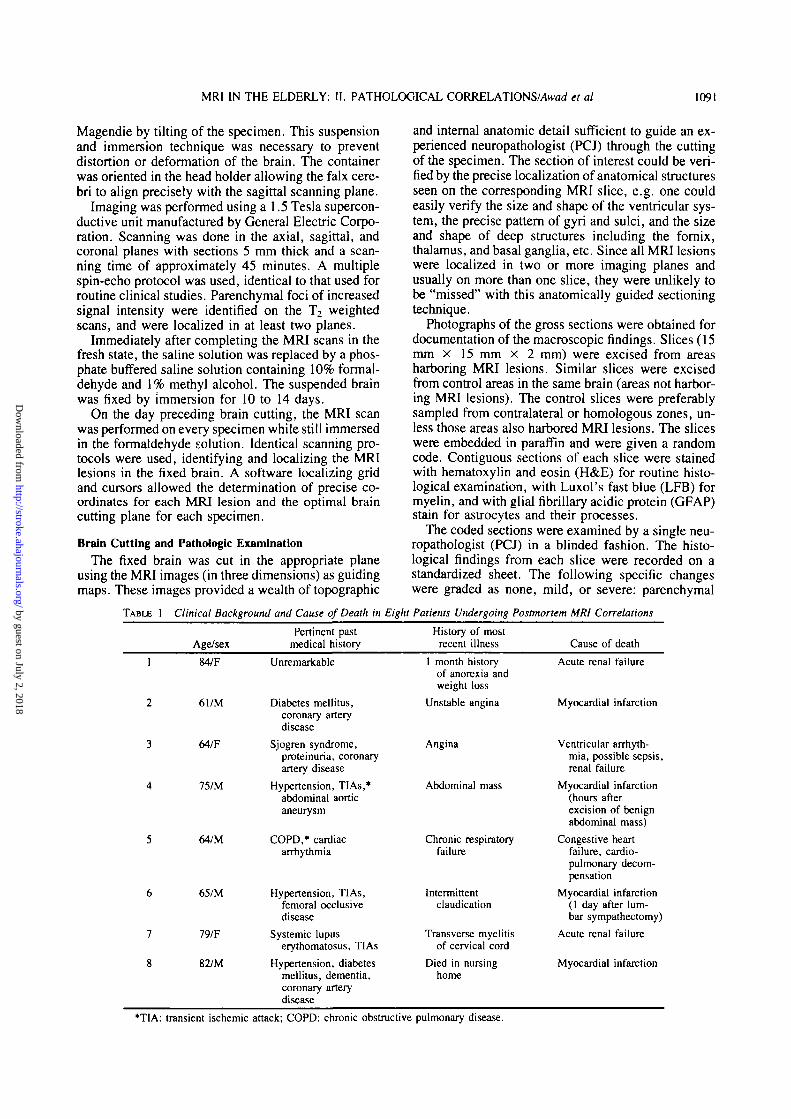
TABLE 1 Clinical Background and Cause of Death in Eight Patients Undergoing Postmortem MRI Correlations
Age/sexPertinent past
medical historyHistory of most
recent illness Cause of death
84/F
61/M
64/F
75/M
64/M
65/M
79/F
82/M
Unremarkable
Diabetes mellitus,coronary arterydisease
Sjogren syndrome,proteinuria, coronaryartery disease
Hypertension, TIAs,*abdominal aorticaneurysm
COPD,* cardiacarrhythmia
Hypertension, TIAs,femoral occlusivedisease
Systemic lupuserythomatosus, TIAs
Hypertension, diabetesmellitus, dementia,coronary arterydisease
ck; COPD: chronic obstructive
1 month historyof anorexia andweight loss
Unstable angina
Angina
Abdominal mass
Chronic respiratoryfailure
Intermittentclaudication
Transverse myelitisof cervical cord
Died in nursinghome
pulmonary disease.
Acute renal failure
Myocardial infarction
Ventricular arrhyth-mia, possible sepsis,renal failure
Myocardial infarction(hours afterexcision of benignabdominal mass)
Congestive heartfailure, cardio-pulmonary decom-pensation
Myocardial infarction(1 day after lum-bar sympathectomy)
Acute renal failure
Myocardial infarction
by guest on July 2, 2018http://stroke.ahajournals.org/
Dow
nloaded from

1092 STROKE VOL 17, No 6, NOVEMBER-DECEMBER 1986
TABLE 2 Histopathological Correlation of Subcortical MRI Lesions in the Elderly
Arterial and arteriolar sclerosis
rtone
mild
severe
Arterial and venous ectasia
none
mild
severe
Dilated perivascular spaces
none
mild
severe
Combination of above changes
severe form of one or moreabove changes
severe form of two or moreabove changes
Pallor to myelin stains
none
mild
severe
Gliotic reaction
none
mild
severe
Other or unexpected pathology
lacunar infarction
capillary telangiectasia
Areas withoutMRI lesions
n = 15
12 (80%)
3 (20%)
0 (0%)
9 (60%)
2 (13.3%)
4 (26.7%)
12 (80%)
2 (13.3%)
1 (6.7%)
4 (26.7%)
1 (6.6%)
15 (100%)
0 (0%)
0 (0%)
14 (93.3%)
1 (6.7%)
0 (0%)
0 (0%)
1 (6.7%)
Areas withMRI lesions
n = 27
7 (26%)
8 (30%)
12 (44%)
4 (14.8%)
6 (22.2%)
17 (77%)
2 (7.4%)
9 (33.3%)
16 (59.3%)
27 (100%)
23 (85%)
2 (7.4%)
19 (70.4%)
6 (22.2%)
11 (40.7%)
12 (44.4%)
4 (14.9%)
1 (3.7%)
1 (3.7%)
Chi-squarecomparison
p value
0.190
0.699
0.303
0.280
0.592
0.251
0.082
0.497
0.162
0.033*
0.043*
0.034*
0.162
0.411
0.162
0.293
0.532
•Significant at the 0.05 level.
edema, enlarged perivascular spaces, lacunar infarc-tion, tract degeneration, gliosis, inflammation, macro-phage infiltration, arteriosclerosis or hyalinosis, arteri-al or venous ectasia, and myelin pallor. In addition,specific comments on the above changes or on otherhistologic findings were noted at the discretion of theexamining pathologist.
Data AnalysisThe slice code was subsequently broken, and each
slice was identified as to patient, area of origin, andcorresponding MRI findings. Descriptive clinical-ra-diological-pathological correlations were formulated.In addition, a computer assisted analysis was conduct-ed correlating specific histological features with thepresence of MRI lesions. The Chi-Square test was usedin each instance with 1 df and Yate's continuity correc-tion.
ResultsThere were three females and five males ranging in
age from 61 to 84 years (mean = 72 years). Theclinical background and cause of death for each case
are summarized in table 1. The brain weights at autop-sy ranged from 1140 g to 1790 g (mean = 1355 g).Four patients had a previous history of ischemic cere-brovascular disease: 3 were hypertensive, and 3 hadtransient ischemia without persisting neurologic signsor symptoms. The fourth patient (case 8) had multi-infarct dementia (by clinical criteria). All patients diedof nonneurologic causes, and none had a final hospital-ization of more than eleven days. No patient was on aventilator for more than 24 hours before death.
Prevalence and Distribution of MRI LesionsIncidental MRI lesions were encountered in every
case (fig. 1). In both instances where MRI was per-formed before and after brain fixation, MRI lesionswere identical in the fresh and fixed states (fig. 2). Allthe incidental MRI lesions were subcortical. Theymost frequently involved the white matter adjacent tothe frontal horns of the lateral ventricles (6 cases).Other frequently involved areas included the whitematter of the optic radiations (5 cases), the basal gan-glia (3 cases), and the centrum semiovale (2 cases).Lesions occasionally formed large patches involving
by guest on July 2, 2018http://stroke.ahajournals.org/
Dow
nloaded from

MRI IN THE ELDERLY: II. PATHOLOGICAL C O R R E L A T J O N S M H W et al 1093
MRI FINDINGS IN EIGHT ELDERLY PATIENTSSUBMITTED TO POSTMORTEM EXAMINATION
Case #261 M
Case #3
Case #5, 6 4 M
Case #665 M
'MRI done 11 days pre-mortem
FIGURE 1. Anatomical distribution of subcortical MRI lesionsin 8 elderly patients. In all but case 7, the findings are thosenoted on postmortem MRI of the fixed brain. The sections se-lected are those best highlighting the lesions.
the deep gray nuclei and adjacent white matter. NoMRI lesion corresponded to a clinical neurologicaldeficit or was suspected to be present during life.
Findings on Gross Pathological ExaminationRemarkably few gross abnormalities were noted in
the areas corresponding to the MRI lesions (figs. 3 and4). Subtle grayish discoloration was noted in the anglesof the lateral ventricles in 6 cases, and involved areasof MRI lesions in every instance. An indistinct sieve-like appearance of the brain parenchyma was noted inall cases and seemed to correspond to areas involvedby MRI lesions. On loupe magnification, these sieve-like areas represented prominent vessels and/or peri-vascular space within the parenchyma. One small areaof lacunar infarction (2 mm) was identified in the rightthalamus of case 8. Capillary telangiectasiae could bevisualized on gross examination of two other cases.The lacunar infarction and one telangiectasia corre-sponded to areas with MRI abnormality. The secondtelangiectasia (3 mm) involved a cortical gyrus, but didnot present an abnormal signal on MRI.
Findings on Histological Examination (table 2)Forty-two slices were sampled for histological ex-
amination. Twenty-seven corresponded to areas withMRI lesions, and 15 corresponded to areas withoutMRI lesions (control areas). Dilated perivascularspaces, vascular ectasia, and arteriosclerosis werefound more frequently in MRI positive areas (figs.5-7). A severe form of one or more of these alterationswas found in 27 of 27 MRI positive regions and in 4 of15 control regions (p < 0.05). A severe form of two ormore of these vascular changes was found in 23 of 27MRI positive areas and in 1 of 15 control areas (p <0.05).
In addition to the vascular changes noted above,there were other pathological alterations in some of theareas corresponding to MRI lesions. Patchy zones ofgliosis were encountered in 16 of 27 areas with MRI
FiauRE 2. Postmortem in vitro MRI of case 6. (A) scan performed in the fresh state (in saline); (B) scan performed in the fixedstate (in formalin). In each instance, the upper rows show "slightly T2 weighted" images (TR = 2 seconds, TE = 25 x W~3
seconds) and the lower rows show "heavily T2 weighted" images (TR = 2 seconds, TE = 80 X 10 ~3 seconds). Bilateral frontaland occipital periventricular MRI lesions are noted in the fresh and fixed states.
by guest on July 2, 2018http://stroke.ahajournals.org/
Dow
nloaded from

1094 STROKE VOL 17, No 6, NOVEMBER-DECEMBER 1986
FIGURE 3. (A& B) Gross sections of the brain of case 6. The two images correspond to the MRI sections in figure 2B. Note thesubtle grayish discoloration near the angles of the lateral ventricles (straight arrows), and the diffuse sieve-like appearance ofthe parenchyma (curved arrows).
abnormality (and in 1 of 15 control areas). Gliosis waslimited to subependymal white matter (fig. 5) and tothe zone surrounding a lacunar infarction. Pallor tomyelin stains was observed in the same areas exhibit-ing gliosis. Unlike demyelinating disease, severe pal-lor to myelin stains was not associated with axonalpreservation or peri vascular inflammation. Instead, itoccurred in conjunction with loss of myelinated fibersand gliosis. All areas exhibiting pallor to myelin stainsand gliosis also demonstrated dilated perivascularspaces, vascular ectasia, and arteriosclerosis.
Only one area of true infarction, a 2 mm lacune, wasnoted. It was surrounded by gliosis and myelin lossseveral millimeters beyond the zone of true brain ne-crosis. Aside from an incidental telangiectasia in oneother case, there were no additional pathological find-ings corresponding to the MRI lesions.
DiscussionSubcortical foci of increased signal intensity are fre-
quently identified on MRI in the elderly. While theselesions are associated with age, hypertension, and aprior history of brain ischemia, their clinical signifi-cance remains speculative.2 Furthermore, it is notknown if any pathologic changes are responsible forthe increased MRI signal in these lesions.
Conventional clinical-radiological-pathological cor-
relations have been performed on patients with clinicalevidence of advanced subcortical ischemic disease,who harbor such MRI lesions.7' " These studies do notexplain similar MRI findings in asymptomatic elderlypatients. In asymptomatic cases, accurate pathologiccorrelations require that each patient would have diedof nonneurologic causes shortly after an MRI scanrevealed incidental lesions.1 This scenario is quite un-likely and imposes an additional selection bias. Wehave only encountered one such case in over two yearsof clinical MRI experience. Pathological correlationsof MRI findings in this patient (case 7) were includedin this study.
An alternative approach to the problem was to iden-tify the MRI lesions on postmortem MRI scans. Thetechnique of postmortem in vitro MRI has not beendescribed previously. It provided images of compara-ble quality to those routinely obtained from the livingbrain using identical scanning protocols.2 Fixation ofthe brain did not impair the overall quality of imaging,the resolution of internal anatomical structures, or theappearance of subcortical parenchymal lesions. In allcases, the lesions were identified on the fixed brain justprior to sectioning, and precisely localized for patho-logical examination. The examination was performedin a blinded fashion, including control areas from thesame specimen.
by guest on July 2, 2018http://stroke.ahajournals.org/
Dow
nloaded from

MRI IN THE ELDERLY: II. PATHOLOGICAL C O R R E L A T I O N S / A H W et al 1095
The MRI lesions involved the white matter adjacentto the lateral ventricles, the optic radiations, the basalganglia, and the centra semiovale in decreasing fre-quency. The lesions were associated with a spectrumof histological alterations. Enlarged perivascularspaces and ectasia of small arteries and veins werefound in all areas with MRI lesions regardless of ana-
FIGURE 4. (A) Premortem MRI of case 7. At the time of thescan, the patient had neck pain, a mild cervical myelopathy(level at C5-C6), and normal mental status. The patient died 11days later of renal failure. (B) Gross section of the fixed brainfrom the same case. Note the subtle grayish discoloration(straight arrows) and the diffuse sieve-like appearance of theparenchyma (curved arrows).
FIGURE 5. (Left): Photomicrograph of the right occipitalperiventricular area of case 4, in an area devoid of MRI lesions.Note the normal (narrow) perivascular space, and the absenceof vascular ectasia and arteriosclerosis. (H & E; x 20).(Right): Photomicrograph of the right frontal periventriculararea of the same case corresponding to the MRI lesion illustrat-ed in figure 1. Note the dilated perivascular spaces (evident asprominent halos around small and large vessels), vascular ecta-sia, and sclerosis of arteries and arterioles. In addition, there isa patchy zone of gliosis (confirmed by GFAP stain) and degen-eration of myelinated axons (confirmed by myelin stain) in thesubependymal area (arrow) (H & E; X 20).
tomical location. These vascular changes were oftenassociated with mild pallor to myelin stains and arte-riosclerosis. A fraction of the lesions exhibited a moresevere pathological process consisting of degenerationof myelinated axons and gliosis. The latter were limit-ed to subependymal areas and the area surrounding asmall lacunar infarction. The MRI signal did not dif-ferentiate between the milder form of histologicalchanges (enlarged perivascular spaces and vascular ec-tasia) and the more severe form (myelinated fiber lossand gliosis).
FIGURE 6. High magnification photomicrograph of the rightfrontal periventricular area of case 4 corresponding to the MRIlesion noted in Figs. I and 5B. Note the dilated perivascularspaces (evident as prominent halos around small and largevessels), and arteriosclerosis (curved arrows). (H&E; x 40).
by guest on July 2, 2018http://stroke.ahajournals.org/
Dow
nloaded from
1096 STROKE VOL. 17, No 6, NOVEMBER-DECEMBER 198$
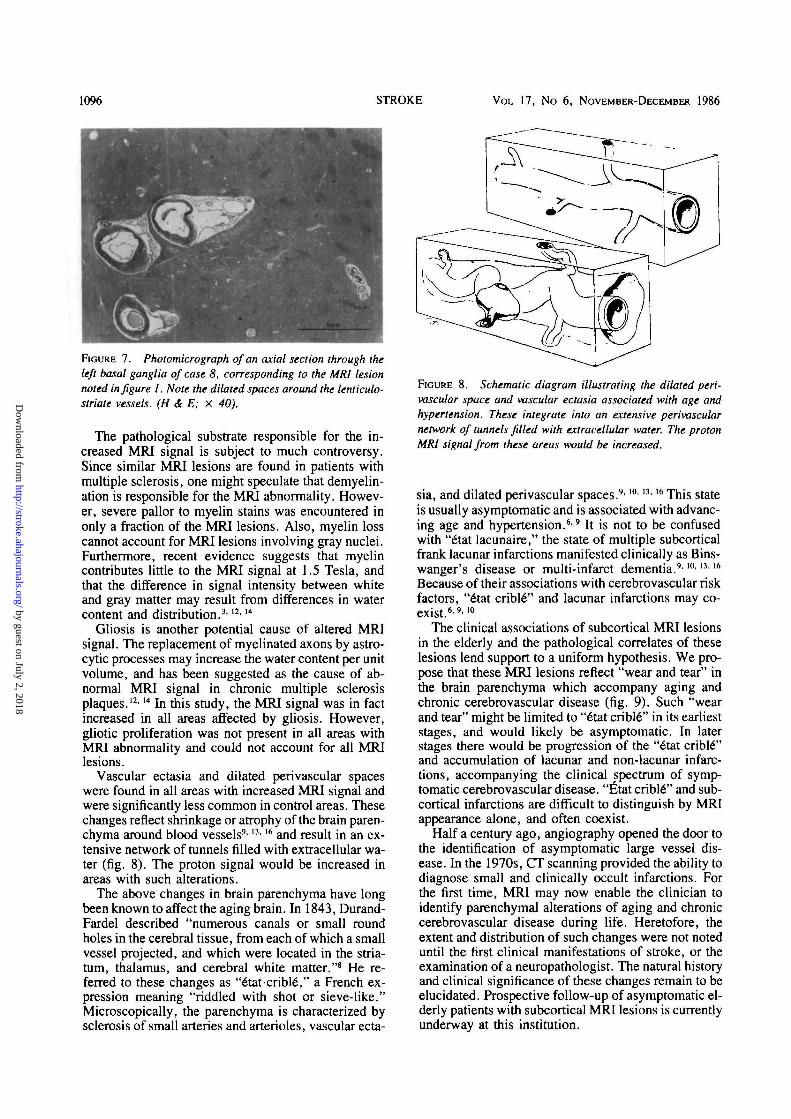
FIGURE 7. Photomicrograph of an axial section through theleft basal ganglia of case 8, corresponding to the MRI lesionnoted in figure I. Note the dilated spaces around the lenticulo-striate vessels. (H & E; X 40).
The pathological substrate responsible for the in-creased MRI signal is subject to much controversy.Since similar MRI lesions are found in patients withmultiple sclerosis, one might speculate that demyelin-ation is responsible for the MRI abnormality. Howev-er, severe pallor to myelin stains was encountered inonly a fraction of the MRI lesions. Also, myelin losscannot account for MRI lesions involving gray nuclei.Furthermore, recent evidence suggests that myelincontributes little to the MRI signal at 1.5 Tesla, andthat the difference in signal intensity between whiteand gray matter may result from differences in watercontent and distribution.3'12'14
Gliosis is another potential cause of altered MRIsignal. The replacement of myelinated axons by astro-cytic processes may increase the water content per unitvolume, and has been suggested as the cause of ab-normal MRI signal in chronic multiple sclerosisplaques.12'l4 In this study, the MRI signal was in factincreased in all areas affected by gliosis. However,gliotic proliferation was not present in all areas withMRI abnormality and could not account for all MRIlesions.
Vascular ectasia and dilated perivascular spaceswere found in all areas with increased MRI signal andwere significantly less common in control areas. Thesechanges reflect shrinkage or atrophy of the brain paren-chyma around blood vessels9' 13> 16 and result in an ex-tensive network of tunnels filled with extracellular wa-ter (fig. 8). The proton signal would be increased inareas with such alterations.
The above changes in brain parenchyma have longbeen known to affect the aging brain. In 1843, Durand-Fardel described "numerous canals or small roundholes in the cerebral tissue, from each of which a smallvessel projected, and which were located in the stria-tum, thalamus, and cerebral white matter."8 He re-ferred to these changes as "e"tatcribl6," a French ex-pression meaning "riddled with shot or sieve-like."Microscopically, the parenchyma is characterized bysclerosis of small arteries and arterioles, vascular ecta-
FIGURE 8. Schematic diagram illustrating the dilated peri-vascular space and vascular ectasia associated with age andhypertension. These integrate into an extensive perivascularnetwork of tunnels filled with extracellular water. The protonMRI signal from these areas would be increased.
sia, and dilated perivascular spaces.9'l0' "• '6 This stateis usually asymptomatic and is associated with advanc-ing age and hypertension.69 It is not to be confusedwith "6tat lacunaire," the state of multiple subcorticalfrank lacunar infarctions manifested clinically as Bins-wanger's disease or multi-infarct dementia.9-10'13-16
Because of their associations with cerebrovascular riskfactors, "6tat criblS" and lacunar infarctions may co-exist.69'10
The clinical associations of subcortical MRI lesionsin the elderly and the pathological correlates of theselesions lend support to a uniform hypothesis. We pro-pose that these MRI lesions reflect "wear and tear" inthe brain parenchyma which accompany aging andchronic cerebrovascular disease (fig. 9). Such "wearand tear" might be limited to "6tat cribl6" in its earlieststages, and would likely be asymptomatic. In laterstages there would be progression of the "6tat crible""and accumulation of lacunar and non-lacunar infarc-tions, accompanying the clinical spectrum of symp-tomatic cerebrovascular disease. "Iitat cribl6" and sub-cortical infarctions are difficult to distinguish by MRIappearance alone, and often coexist.
Half a century ago, angiography opened the door tothe identification of asymptomatic large vessel dis-ease. In the 1970s, CT scanning provided the ability todiagnose small and clinically occult infarctions. Forthe first time, MRI may now enable the clinician toidentify parenchymal alterations of aging and chroniccerebrovascular disease during life. Heretofore, theextent and distribution of such changes were not noteduntil the first clinical manifestations of stroke, or theexamination of a neuropathologist. The natural historyand clinical significance of these changes remain to beelucidated. Prospective follow-up of asymptomatic el-derly patients with subcortical MRI lesions is currentlyunderway at this institution.
by guest on July 2, 2018http://stroke.ahajournals.org/
Dow
nloaded from

MRI IN THE ELDERLY: II. PATHOLOGICAL C O R R E L A T I O N S M H W et al 1097
SYSTEMICATHEROSCLEROSIS
(Conauiy VH CtnxU M m
AGINGHYFERTENSION
(Ortv. Rkt Faaon . .)
MULTUNFARCTSTATE
, HYAUNE SCLEROSISANDECTAS1AOF _ ^ . LACUNARSMAU ARTERIES ^ I N F A R C T I O N SANDABTERKXES
SYMPTOMATIC CEREBllOVASCULAR DISEASE
FIGURE 9. Schematic diagram illustrating a spectrum of
chronic cerebrovascular disease. There is a gradual appear-ance of subcortical MRI lesions as the patient ages and riskfactors accumulate. Subcortical MRI lesions increase as thevarious clinical manifestations of cerebrovascular disease be-come evident. The end stage of the process involves severe MRIlesions and a clinical form of the multi-infarct state.
AcknowledgmentsThis work would not have been possible without the dedicated and
competent help of the technical staff of the Division of Neuropathology(Larry Suchocki, B.S., morgue supervisor and Doris Johnson, histolo-gy technician), Division of Neuroradiology (James C. Winters,B.S.R.T. and Kevin King, R.T., MRI technicians), Department of Artand Photography, and Editorial Office of the Barrow NeurologicalInstitute of St. Joseph's Hospital and Medical Center. Steven Harrison,Medical Illustrator, is particularly acknowledged for his most expres-sive art work. Laura Mason, B.S., supervised the collection of photo-graphic and pathologic data and coordinated the coding for blindedexaminations. Burton P. Drayer, M.D., and Alvin D. Sidell, M.D.,read and critiqued the manuscript and gave invaluable suggestionsthroughout the project.
References1. Awad I, Modic M, Little JR, et al: Focal parenchymal lesions in
transient ischemic attacks — correlation of CT and MRI. Stroke17: 399-403, 1986
2. Awad IA, Spetzler RF, Hodak JA, et al: Incidental subcorticallesions identified on magnetic resonance imaging in the elderly: I.Correlation with age and cerebrovascular risk factors. Stroke 17:
, 19863. Bottomly PA, Hart HR Jr, Edelstein WA et al: Anatomy and
metabolism of the normal human brain studied by magnetic reso-nance at 1.5 Tesla. Radiology 150: 441^446, 1984
4. Bradley WG Jr, Waluch V, Brant-Zawadzki M, et al: Patchy,periventricular white matter lesions in the elderly: a common obser-vation during NMR imaging. Noninvasive Medical Imaging 1:35-41, 1984
5. Brant-Zawadzki M, Fein G, Van Dyke C, et al: MR imaging of theaging brain: patchy white-matter lesions and dementia. AJNR 6:675-682, 1985
6. Cole FM, Yates PO: Comparative incidence of cerebrovascularlesions in normotensive and hypertensive patients. Neurology 18:255-259, 1968
7. Dougherty JH, Simmons JD, Parker J: Subcortical ischemic dis-ease: clinical spectrum and MRJ correlation. Stroke 17: 146(ab-stract), 1986
8. Durand-Fardel M: Traite du ramollissement du cefveau. Paris.Bailliere 1843
9. Escourolle R, Poirier J: Other cerebrovascular lesions of ischemicnature, in Escourolle R, Poirier J: (eds) Manual of Basic Neuro-pathology. Philadelphia: W.B. Saunders, 1978, pp 101-103
10. Fisher CM: Lacunes: Small deep cerebral infarcts. Neurology 15:774-784, 1965
11. Kinkel WR, Jacobs L, Polachini I, et al: Subcortical arterioscleroticencephalopathy (Binswanger's disease). Computed Tomographic,nuclear magnetic resonance, and clinical correlations. Arch Neurol42: 951-959, 1985
12. McDonald WI: The mystery of the origin of multiple sclerosis. JNeurol Neurosurg Psychiatry 49: 113-123, 1986
13. Okazaki H: Cerebrovascular disease: effects of arteriolar (and arte-rial) sclerosis on brain parenchyma, in Okazaki H: (ed) Fundamen-tals of Neuropathology. New York: Igaku-shein, 1983, pp 57-62
14. Ormerod LEC, Du Boulay EPGH, Callanan MM, et al: NMR inmultiple sclerosis and cerebral vascular disease. Lancet 2:1334-1335, 1984
15. Salgado ED, Weinstein M, Furlan AJ, et al: Proton magnetic reso-nance imaging in ischemic cerebrovascular disease. Ann of Neurol-ogy (In press), 1986
16. Stehbens WE: Thrombosis, infarction, embolism, and vascularinsufficiency; other ischemic lesions, in Stehbens WE: (ed) Pathol-ogy of the Cerebral Blood Vessels. St. Louis: C.V. Mosby, 1972,pp 177-178
17. Tomlinson BE, Blessed G, Roth M: Observations on the brains ofdemented old people. J Neurol Sci 11: 205-242, 1970
18. Tomlinson BE, Blessed G, Roth M: Observations on the brains ofnon-demented old people. J Neurol Sci 7: 331-356, 1968
by guest on July 2, 2018http://stroke.ahajournals.org/
Dow
nloaded from
I A Awad, P C Johnson, R F Spetzler and J A HodakPostmortem pathological correlations.
Incidental subcortical lesions identified on magnetic resonance imaging in the elderly. II.
Print ISSN: 0039-2499. Online ISSN: 1524-4628 Copyright © 1986 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Stroke doi: 10.1161/01.STR.17.6.1090
1986;17:1090-1097Stroke.
http://stroke.ahajournals.org/content/17/6/1090World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://stroke.ahajournals.org//subscriptions/
is online at: Stroke Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer available in the
Permissions in the middle column of the Web page under Services. Further information about this process isOnce the online version of the published article for which permission is being requested is located, click Request
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Stroke Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on July 2, 2018http://stroke.ahajournals.org/
Dow
nloaded from