
Incidence of Hardware-Related Pain and Its Effect on ... of Hardware... · come after ORIF of ankle...
4
Incidence of Hardware-Related Pain and Its Effect on Functional Outcomes After Open Reduction and Internal Fixation of Ankle Fractures Ouida L. Brown, Douglas R. Dirschl, and William T. Obremskey University of North Carolina School of Medicine, Raleigh, North Carolina, U.S.A. Objectives: To document the incidence of late pain and hard- ware removal after open reduction and internal fixation (ORIF) of ankle fractures. To test the hypothesis that late pain overly- ing the distal tibial and fibular hardware is associated with poorer functional outcomes. Design: Retrospective review. Setting: Level II trauma center. Patients: One hundred twenty-six skeletally mature patients undergoing ORIF of unstable malleolar fractures who were followed up for at least six months from injury were included. Main Outcome Measurements: Analog pain score, Short Form-36 Health Survey (SF-36), and Short Form Musculoskel- etal Functional Assessment (SMFA). Results: Thirty-nine (31 percent) of the 126 patients had lateral pain overlying their fracture hardware. Twenty-nine patients (23 percent) had had their hardware removed or desired to have it removed. Of the twenty-two patients with hardware-related pain who had undergone hardware removal, only eleven had improvement in their lateral ankle pain; the mean analog pain score decreased from 6 ± 3.16 (mean ± standard deviation) before hardware removal to 3 ± 2.9 after hardware removal (p 0.008). In general, SF-36 and SMFA scores at final follow- up were significantly lower for patients who had pain overlying their lateral hardware than for those who had no pain. For the group of patients who had lateral ankle pain, no significant difference was noted in SMFA or SF-36 scores for patients who had and who had not had their lateral hardware removed (p > 0.5). Conclusion: The incidence of late pain overlying the distal tibial and fibular plate or screws is not insignificant. Although pain is generally decreased after hardware removal, nearly half of patients continue to have pain even after hardware removal. Functional outcome scores are poorer for patients with pain overlying lateral ankle hardware than in those with no pain at this location; this poorer outcome seems to be independent of whether the hardware was removed. Although the results of this study do not support or condemn the routine removal of frac- ture hardware after healing of unstable ankle fractures, they give orthopaedic surgeons some information that may assist them in counseling patients as to the expected functional out- come after ORIF of ankle fractures and the likelihood of relief of pain after removal of fracture hardware from the distal tibia and fibula. Key Words: Ankle fracture, Hardware removal, Open reduc- tion and internal fixation, Pain, Painful hardware. Open reduction and internal fixation (ORIF) of frac- tures of the ankle is one of the most common fracture surgeries performed in general orthopaedic practice. Whereas the surgical treatment of this injury has clearly resulted in outcomes superior to those of closed reduc- tion and cast immobilization (3,4,6,8,9,12,15), the pres- ence of a plate or screws in a subcutaneous location on the distal tibia or fibula can result in long-term tender- ness and pain. This causes some patients to have elective removal of the plate or screws after fracture healing has occurred (5). The incidence of late pain at the site of fracture hardware in malleolar fractures has not been clearly documented in the orthopaedic literature, nor has the incidence of hardware removal for late pain (1,3,4, 7,8,9,10,14). The purpose of this investigation was to document the incidence of late pain related to the pres- ence of distal tibial and fibular plates or screws and to document the incidence of hardware removal after ORIF of ankle fractures. MATERIALS AND METHODS A retrospective review was conducted of 126 patients who had undergone ORIF for displaced ankle fractures during a five-year period from May 1994 to December 1998. Patients were included in the study if they had an unstable ankle fracture treated by ORIF of the Accepted August 2, 2000. Address correspondence and reprint requests to Dr. Douglas R. Dirschl, University of North Carolina School of Medicine, 3024 New Bern Avenue, Suite 300, Raleigh, NC 27610, U.S.A. No funds were received in direct support of this research. The au- thors have no financial conflict of interest related to the topic of this investigation. The devices reported in this investigation have been approved for use in humans by the United States Food and Drug Administration. Journal of Orthopaedic Trauma Vol. 15, No. 4, pp. 271–274 © 2001 Lippincott Williams & Wilkins, Inc., Philadelphia 271
Transcript of Incidence of Hardware-Related Pain and Its Effect on ... of Hardware... · come after ORIF of ankle...

Incidence of Hardware-Related Pain and Its Effect on FunctionalOutcomes After Open Reduction and Internal Fixation of
Ankle Fractures
Ouida L. Brown, Douglas R. Dirschl, and William T. Obremskey
University of North Carolina School of Medicine, Raleigh, North Carolina, U.S.A.
Objectives: To document the incidence of late pain and hard-ware removal after open reduction and internal fixation (ORIF)of ankle fractures. To test the hypothesis that late pain overly-ing the distal tibial and fibular hardware is associated withpoorer functional outcomes.Design: Retrospective review.Setting: Level II trauma center.Patients: One hundred twenty-six skeletally mature patientsundergoing ORIF of unstable malleolar fractures who werefollowed up for at least six months from injury were included.Main Outcome Measurements: Analog pain score, ShortForm-36 Health Survey (SF-36), and Short Form Musculoskel-etal Functional Assessment (SMFA).Results: Thirty-nine (31 percent) of the 126 patients had lateralpain overlying their fracture hardware. Twenty-nine patients(23 percent) had had their hardware removed or desired to haveit removed. Of the twenty-two patients with hardware-relatedpain who had undergone hardware removal, only eleven hadimprovement in their lateral ankle pain; the mean analog painscore decreased from 6 ± 3.16 (mean ± standard deviation)before hardware removal to 3 ± 2.9 after hardware removal (p� 0.008). In general, SF-36 and SMFA scores at final follow-up were significantly lower for patients who had pain overlying
their lateral hardware than for those who had no pain. For thegroup of patients who had lateral ankle pain, no significantdifference was noted in SMFA or SF-36 scores for patients whohad and who had not had their lateral hardware removed (p >0.5).Conclusion: The incidence of late pain overlying the distaltibial and fibular plate or screws is not insignificant. Althoughpain is generally decreased after hardware removal, nearly halfof patients continue to have pain even after hardware removal.Functional outcome scores are poorer for patients with painoverlying lateral ankle hardware than in those with no pain atthis location; this poorer outcome seems to be independent ofwhether the hardware was removed. Although the results of thisstudy do not support or condemn the routine removal of frac-ture hardware after healing of unstable ankle fractures, theygive orthopaedic surgeons some information that may assistthem in counseling patients as to the expected functional out-come after ORIF of ankle fractures and the likelihood of reliefof pain after removal of fracture hardware from the distal tibiaand fibula.Key Words: Ankle fracture, Hardware removal, Open reduc-tion and internal fixation, Pain, Painful hardware.
Open reduction and internal fixation (ORIF) of frac-tures of the ankle is one of the most common fracturesurgeries performed in general orthopaedic practice.Whereas the surgical treatment of this injury has clearlyresulted in outcomes superior to those of closed reduc-tion and cast immobilization (3,4,6,8,9,12,15), the pres-ence of a plate or screws in a subcutaneous location onthe distal tibia or fibula can result in long-term tender-ness and pain. This causes some patients to have elective
removal of the plate or screws after fracture healing hasoccurred (5). The incidence of late pain at the site offracture hardware in malleolar fractures has not beenclearly documented in the orthopaedic literature, nor hasthe incidence of hardware removal for late pain (1,3,4,7,8,9,10,14). The purpose of this investigation was todocument the incidence of late pain related to the pres-ence of distal tibial and fibular plates or screws and todocument the incidence of hardware removal after ORIFof ankle fractures.
MATERIALS AND METHODS
A retrospective review was conducted of 126 patientswho had undergone ORIF for displaced ankle fracturesduring a five-year period from May 1994 to December1998. Patients were included in the study if they hadan unstable ankle fracture treated by ORIF of the
Accepted August 2, 2000.Address correspondence and reprint requests to Dr. Douglas R.
Dirschl, University of North Carolina School of Medicine, 3024 NewBern Avenue, Suite 300, Raleigh, NC 27610, U.S.A.
No funds were received in direct support of this research. The au-thors have no financial conflict of interest related to the topic of thisinvestigation.
The devices reported in this investigation have been approved foruse in humans by the United States Food and Drug Administration.
Journal of Orthopaedic TraumaVol. 15, No. 4, pp. 271–274© 2001 Lippincott Williams & Wilkins, Inc., Philadelphia
271
distal fibula with plates and screws (with or withoutstabilization of the medial malleus), were skeletallymature at the time of injury, and had been followed upfor at least six months after injury. The mean age ofpatients at the time of surgery was 49 ± 18 years (mean± standard deviation) (range 17 to 85 years). The meaninterval to follow-up was 27 ± 17 months (range 6 to 64months). According to the Orthopaedic Trauma Associa-tion classification system (11), there were seven 44Afractures, eighty-nine 44B fractures, and thirty 44C frac-tures.
Information was obtained from the patient (interview,pain score, Short Form-36 Health Survey [SF-36], andShort Form Musculoskeletal Functional Assessment[SMFA]), from the hospital chart (injury and treatmentinformation), and from the postoperative radiographs(healing of the fracture, type of plate and screws, andprominence of the hardware). Each patient was inter-viewed by one of the investigators to determine the pres-ence and severity of pain overlying the ankle hardware,whether the hardware had been removed, and whetherthe patient desired to have the hardware removed. Ananalog pain scale was used to rate pain; patients wereasked to rate their distal fibular pain on a scale from one(no pain) to ten (the most pain imaginable). An analogpain score of five or more was considered to representpain, and a score less than five was considered to repre-sent no pain. Patients who had undergone hardware re-moval were asked to give two analog pain scores, oneeach corresponding to pain before and after hardwareremoval.
Pain scores were correlated with functional out-come scores in all patients, which were assessed usingthe SF-36 (13,16) and the SMFA. Statistical analysis offunctional outcome and pain scores was performedusing the Student t test for two samples assuming un-equal variances. All other means were tested by the Stu-dent t test for paired samples. The results were consid-ered significant if p was less than 0.05 in a two-tailedstudy.
RESULTS
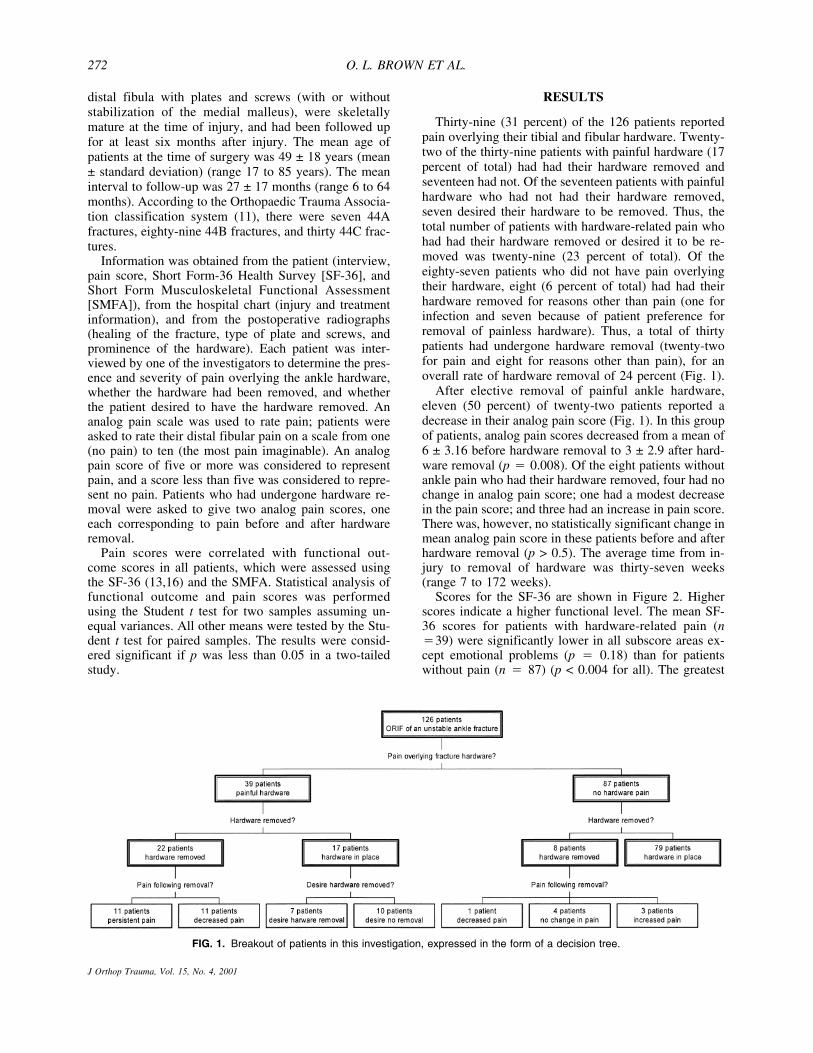
Thirty-nine (31 percent) of the 126 patients reportedpain overlying their tibial and fibular hardware. Twenty-two of the thirty-nine patients with painful hardware (17percent of total) had had their hardware removed andseventeen had not. Of the seventeen patients with painfulhardware who had not had their hardware removed,seven desired their hardware to be removed. Thus, thetotal number of patients with hardware-related pain whohad had their hardware removed or desired it to be re-moved was twenty-nine (23 percent of total). Of theeighty-seven patients who did not have pain overlyingtheir hardware, eight (6 percent of total) had had theirhardware removed for reasons other than pain (one forinfection and seven because of patient preference forremoval of painless hardware). Thus, a total of thirtypatients had undergone hardware removal (twenty-twofor pain and eight for reasons other than pain), for anoverall rate of hardware removal of 24 percent (Fig. 1).
After elective removal of painful ankle hardware,eleven (50 percent) of twenty-two patients reported adecrease in their analog pain score (Fig. 1). In this groupof patients, analog pain scores decreased from a mean of6 ± 3.16 before hardware removal to 3 ± 2.9 after hard-ware removal (p � 0.008). Of the eight patients withoutankle pain who had their hardware removed, four had nochange in analog pain score; one had a modest decreasein the pain score; and three had an increase in pain score.There was, however, no statistically significant change inmean analog pain score in these patients before and afterhardware removal (p > 0.5). The average time from in-jury to removal of hardware was thirty-seven weeks(range 7 to 172 weeks).
Scores for the SF-36 are shown in Figure 2. Higherscores indicate a higher functional level. The mean SF-36 scores for patients with hardware-related pain (n�39) were significantly lower in all subscore areas ex-cept emotional problems (p � 0.18) than for patientswithout pain (n � 87) (p < 0.004 for all). The greatest
FIG. 1. Breakout of patients in this investigation, expressed in the form of a decision tree.
O. L. BROWN ET AL.272
J Orthop Trauma, Vol. 15, No. 4, 2001

difference was observed in the area of bodily pain, inwhich patients with hardware-related pain had a meanscore of 49.9 ± 24.8, whereas patients without pain hada mean score of 72.5 ± 24.8 (p � 0.00007).
Scores for the SMFA are shown in Figure 3. Lowerscores indicate a higher functional level. The meanSMFA scores for patients with hardware-related pain (n� 39) were significantly higher in all subscore areasexcept arm and hand function (p � 0.6) than for patientswithout pain (n � 87) (p < 0.006 for all). The mostsignificant subscores for the SMFA were average botherindex score and average emotional score. The averagebother index score was 29.72 ± 21.1 for patients withpain and 13.84 ± 15.3 for patients without pain (p �0.0004). The average emotional status was 36.79 ± 22.0for patients with pain and 21.76 ± 15.9 for patients with-out pain (p � 0.001).
DISCUSSION
Retrospective analysis of the 126 patients in this studyshowed that 31 percent of patients had significant pain
with hardware and 17 percent had had their hardwareremoved at a mean follow-up of twenty-seven months.These results indicate that painful hardware is a signifi-cant issue after ORIF of unstable ankle fractures andthat the incidence of hardware removal is higher thanpreviously reported (1,2,7). Although some pain reliefafter removal of painful hardware was observed, a de-crease in pain occurred in only approximately one half ofpatients. That there was a wide range in the interval frominjury to hardware removal suggests that the time toremoval may not be a significant factor in regards to painor function.
The results of this study also support the contentionthat patients without ankle pain after ORIF of unstableankle fractures have better functional outcomes than dopatients experiencing significant hardware-related pain.All subscores in SF-36 and SMFA show higher func-tional levels for patients who did not experience pain(Fig. 2 and 3). The performance of patients with andwithout pain was inconsistent in the area of emotionalfunctioning between the two outcome measures; theseinconsistent results indicate that emotional problemsmay or may not be a major determinant of function afteroperative treatment of an unstable ankle fracture. Allother SF-36 subscores, however, showed statistically sig-nificant differences between patients with pain and thosewithout pain. In addition, all the SMFA subscores, withthe exception of hand and arm function, showed signifi-cant better functioning in the group of patients withoutankle pain. The lack of correlation of ankle pain withhand and arm function is to be expected in patients beingexamined after an ankle fracture.
In one recent study, 75 percent of patients with com-plaints after ORIF of an ankle fracture reported improve-ment after hardware removal (5). These results contrastwith those of this study, in which only 50 percent ofpatients had improvement in pain scores after hardwareremoval. Another recent report concluded that removalof hardware after operative treatment of a fracture wasassociated with neither an optimal functional result nor areduction in long-term complications (7), a statementthat our results confirm. Although our study attempted todefine precisely hardware-related pain, there is no way ofknowing that the patients in the study did not also reportpain caused by other factors. Similarly, the poor perfor-mance on the functional outcome measures may havebeen related to factors other than the previous ankle frac-ture; it was our assumption, however, that the incidenceof these confounding conditions was nearly equal in thegroups with and without pain.
The results of this study indicate that the incidence oflate ankle pain overlying the fracture hardware is notinsignificant. Also, whereas pain is often decreased afterhardware removal, some patients, particularly those un-dergoing hardware removal in the absence of lateral pain,may have increased pain after hardware removal. Func-tional outcome scores are poorer for patients with painoverlying ankle hardware than in those with no pain at
FIG. 2. Selected SF-36 subscores for patients with and withouthardware-related ankle pain. Higher scores mean better function.Statistical significance was reached for each subscore presented(p < 0.004 for all). The difference in role limitations attributable toemotional problems between the two patient groups (data notshown) did not reach statistical significance (p = 0.19).
FIG. 3. Selected SMFA subscores for patients with and withouthardware-related ankle pain. Lower scores mean better function.Statistical significance was reached for each subscore presented(p < 0.006 for all). The difference in arm and hand function be-tween the two patient groups (data not shown) was not statisti-cally significant (p = 0.6).
HARDWARE PAIN AFTER ANKLE FRACTURES 273
J Orthop Trauma, Vol. 15, No. 4, 2001

this location. This poorer outcome seems to be indepen-dent of whether the hardware was removed. Although theresults of this study do not support or condemn the rou-tine removal of fracture hardware after healing of un-stable ankle fractures, they give orthopaedic surgeonssome information that may assist them in counselingpatients as to the expected functional outcome afterORIF of ankle fractures and the likelihood of relief ofpain after removal of fracture hardware from the ankle.
REFERENCES
1. Alldredge RH. Diastasis of distal tibiofibular joint and associatedlesions. JAMA 1940;115:2136–2140.
2. Bostman O, Pihlajamake H. Routine implant removal after fracturesurgery: a potential reducible consumer of hospital resources intrauma units. J Trauma 1996:41;846–849.
3. Brodie AD, Denham RA. The treatment of unstable ankle frac-tures. J Bone Joint Surg Br 1974;56:256–262.
4. Griiend RV, Michelson JD, Bone LB. Fractures of the ankle andthe distal part of the tibia. J Bone Joint Surg Am 1996;78:1772–1783.
5. Jacobsen S, Lichtenberg MH, Jensen CM, et al. Removal of inter-nal fixation–the effect on patients’ complaints: a study of 66 casesof removal of internal fixation after malleolar fractures. Foot AnkleInt 1994;15:170–171.
6. Mast JW, Teipner WA. A reproducible approach to the internal
fixation of adult ankle fractures: rationale, technique, and earlyresults. Orthop Clin North Am 1980;11:661–679.
7. Michelson J. Current concepts review. Fractures about the ankle. JBone Joint Surg Am 1995;77:142–152.
8. Mitchell WG, Shaftan GW, Sclanfani SJ. Mandatory open reduc-tion: its role in displaced ankle fractures. J Trauma 1979;19:602–615.
9. Muller ME, Allogover M, Schneider R, et al. Manual of InternalFixation. Technique Recommended by the AO Group, 3rd ed. NewYork, Springer-Verlag, 1991, pp 282–299.
10. Needleman RL, Skrade DA, Stiehl JB. Effect of the syndesmoticscrew on ankle motion. Foot Ankle 1989;10:17–24.
11. Orthopaedic Trauma Association Committee for Coding and Clas-sification. Fracture and dislocation compendium. J Orthop Trauma1996;10(suppl 1):i–ix.
12. Pankovich AM. Fractures of the fibula proximal to the distal tib-iofibular syndesmosis. J Bone Joint Surg Am 1978;60:221–229.
13. Ponz S, Nasell H, Bergman B, et al. Functional outcome andquality of life in patients with type ankle fractures: a two-yearfollow-up study. J Orthop Trauma 1999;13:363–368.
14. Praemer A, Furner S, Rice DP. Musculoskeletal conditions in theUnited States. Park Ridge, Illinois, The American Academy ofOrthopaedic Surgeons, 1992, pp 85–124.
15. Solonen K, Lauttamus L. Operative treatment of ankle fractures.Acta Orthop Scand 1968;39:223–237.
16. Ware JE, Gandex B. Overview of the SF-36 and the InternationalQuality of Life Assessment (IQQLA) Project. J Clin Epidemiol1998;51:903–912.
O. L. BROWN ET AL.274
J Orthop Trauma, Vol. 15, No. 4, 2001


















