Incidence and clinical significance of anti-PF4/heparin antibodies of the IgG, IgM, and IgA class in...
7
Incidence and clinical significance of anti-PF4/heparin antibodies of the IgG, IgM, and IgA class in 755 consecutive patient samples referred for diagnostic testing for heparin-induced thrombocytopenia Heparin-induced thrombocytopenia (HIT) is a severe adverse effect of heparin treatment. HIT is caused by platelet activating antibodies, usually directed against complexes of platelet factor 4 (PF4) and heparin. Typically HIT manifests 5– 14 d after start of heparin (1, 2) and is usually associated with a decrease of platelet counts >50% and/or new thromboembolic complications (TEC). Two types of assays are currently available to test for HIT antibodies (3). Functional (platelet activa- tion) assays such as the 14 C serotonin release test (4, 5) or the heparin-induced platelet activation (HIPA) test (6, 7), using washed platelets, primarily detect antibodies of the immunoglobulin (Ig)G Juhl D, Eichler P, Lubenow N, Strobel U, Wessel A, Greinacher A. Incidence and clinical significance of anti-PF4/heparin antibodies of the IgG, IgM, and IgA class in 755 consecutive patient samples referred for diagnostic testing for heparin-induced thrombocytopenia. Abstract: Background: Heparin-induced thrombocytopenia (HIT) is usually caused by anti-platelet factor 4 (PF4)/heparin antibodies, lead- ing to intravascular platelet activation. These antibodies can be detected by PF4/polyanion antigen assays or platelet activation assays. While antigen assays are very sensitive and recognize immunoglobulin (Ig)G, IgA, and IgM antibodies, the role of IgM and IgA HIT-antibodies is debated. Platelet activation assays recognize IgG and are more specific for clinical HIT. Methods: We analyzed sera from 755 consecutive patients referred for diagnostic testing for HIT using a PF4/heparin enzyme-linked immunosorbent assay (ELISA) for IgG, IgA, and IgM and by the heparin-induced platelet activation (HIPA) test. Clinical information was provided by the treating physicians. Results: A total of 108 of 755 (14.3%) patients tested positive, 105 (13.9%) in the PF4/ heparin IgG/A/M ELISA [28 (26.7%) only for IgM/A]; 53 (7.0%) sera were positive in the HIPA, of those 50 tested also positive in the ELISA. In 77 patients sufficient clinical information was provided. Available clinical information for 17 of the 28 patients who had only IgM and/or IgA detected showed plausible alternative (non-HIT) explanations in four of seven who had thromboembolic complications and in nine of 10 who had isolated HIT. Conclusion: Detection of IgG, IgM and IgA class antibodies by PF4/heparin ELISA yields a positive test result about twice as often as does a platelet activation assay, with only a minority of the additional patients detected likely having HIT. Thus, there is a potential for considerable over-diagnosis of HIT by laboratories that utilize only an ELISA for diagnostic testing. David Juhl, Petra Eichler, Norbert Lubenow, Ulrike Strobel, Antje Wessel, Andreas Greinacher Department of Immunology and Transfusion Medicine, Ernst-Moritz-Arndt University Greifswald, Greifswald, Germany Key words: heparin; heparin-induced thrombocytopenia; thrombosis; immunoglobulin classes; heparin-induced thrombocytopenia assays Correspondence: Dr Andreas Greinacher, Department of Immunology and Transfusion Medicine, Ernst-Moritz- Arndt-University Greifswald, Sauerbruchstr./ Diagnostikzentrum, 17487 Greifswald, Germany Tel: +49 3834 865482 Fax: +49 3834 865489 e-mail: [email protected] Accepted for publication 17 November 2005 Eur J Haematol 2006: 76: 420–426 doi:10.1111/j.1600-0609.2005.00621.x All rights reserved Ó 2006 The Authors Journal compilation Ó 2006 Blackwell Munksgaard EUROPEAN JOURNAL OF HAEMATOLOGY 420
-
Upload
david-juhl -
Category
Documents
-
view
212 -
download
0
Transcript of Incidence and clinical significance of anti-PF4/heparin antibodies of the IgG, IgM, and IgA class in...

Incidence and clinical significance ofanti-PF4/heparin antibodies of the IgG,IgM, and IgA class in 755 consecutivepatient samples referred for diagnostictesting for heparin-inducedthrombocytopenia
Heparin-induced thrombocytopenia (HIT) is asevere adverse effect of heparin treatment. HIT iscaused by platelet activating antibodies, usuallydirected against complexes of platelet factor 4(PF4) and heparin. Typically HIT manifests 5–14 d after start of heparin (1, 2) and is usuallyassociated with a decrease of platelet counts >50%
and/or new thromboembolic complications (TEC).Two types of assays are currently available to testfor HIT antibodies (3). Functional (platelet activa-tion) assays such as the 14C serotonin release test(4, 5) or the heparin-induced platelet activation(HIPA) test (6, 7), using washed platelets, primarilydetect antibodies of the immunoglobulin (Ig)G
Juhl D, Eichler P, Lubenow N, Strobel U, Wessel A, Greinacher A.Incidence and clinical significance of anti-PF4/heparin antibodies of theIgG, IgM, and IgA class in 755 consecutive patient samples referred fordiagnostic testing for heparin-induced thrombocytopenia.
Abstract: Background: Heparin-induced thrombocytopenia (HIT) isusually caused by anti-platelet factor 4 (PF4)/heparin antibodies, lead-ing to intravascular platelet activation. These antibodies can be detectedby PF4/polyanion antigen assays or platelet activation assays. Whileantigen assays are very sensitive and recognize immunoglobulin (Ig)G,IgA, and IgM antibodies, the role of IgM and IgA HIT-antibodies isdebated. Platelet activation assays recognize IgG and are more specificfor clinical HIT. Methods: We analyzed sera from 755 consecutivepatients referred for diagnostic testing for HIT using a PF4/heparinenzyme-linked immunosorbent assay (ELISA) for IgG, IgA, and IgMand by the heparin-induced platelet activation (HIPA) test. Clinicalinformation was provided by the treating physicians. Results: A totalof 108 of 755 (14.3%) patients tested positive, 105 (13.9%) in the PF4/heparin IgG/A/M ELISA [28 (26.7%) only for IgM/A]; 53 (7.0%) serawere positive in the HIPA, of those 50 tested also positive in the ELISA.In 77 patients sufficient clinical information was provided. Availableclinical information for 17 of the 28 patients who had only IgM and/orIgA detected showed plausible alternative (non-HIT) explanations infour of seven who had thromboembolic complications and in nine of 10who had isolated HIT. Conclusion: Detection of IgG, IgM and IgAclass antibodies by PF4/heparin ELISA yields a positive test result abouttwice as often as does a platelet activation assay, with only a minority ofthe additional patients detected likely having HIT. Thus, there is apotential for considerable over-diagnosis of HIT by laboratories thatutilize only an ELISA for diagnostic testing.
David Juhl, Petra Eichler, NorbertLubenow, Ulrike Strobel, AntjeWessel, Andreas GreinacherDepartment of Immunology and Transfusion Medicine,Ernst-Moritz-Arndt University Greifswald, Greifswald,Germany
Key words: heparin; heparin-induced thrombocytopenia;thrombosis; immunoglobulin classes; heparin-inducedthrombocytopenia assays
Correspondence: Dr Andreas Greinacher, Department ofImmunology and Transfusion Medicine, Ernst-Moritz-Arndt-University Greifswald, Sauerbruchstr./Diagnostikzentrum, 17487 Greifswald, GermanyTel: +49 3834 865482Fax: +49 3834 865489e-mail: [email protected]
Accepted for publication 17 November 2005
Eur J Haematol 2006: 76: 420–426doi:10.1111/j.1600-0609.2005.00621.xAll rights reserved
� 2006 The AuthorsJournal compilation � 2006 Blackwell Munksgaard
EUROPEAN JOURNAL OF HAEMATOLOGY
420

class and can detect antibodies to antigens otherthan PF4/heparin (8).Characterization of multimolecular PF4/heparin
complexes as the major antigen in HIT (9–11)allowed the development of antigen-based immuno-assays in which PF4/heparin- or PF4/polyvinylsulf-onate complexes are attached to a solid phase andbinding of antibodies is measured either by anenzyme immunoassay (9, 12, 13) or by agglutination(14, 15). These assays detect only antibodies againstPF4/heparin complexes but in contrast to thefunctional assays also detect anti-PF4/heparin anti-bodies of the IgM and IgA class.Intravascular platelet activation by anti-PF4/
heparin antibodies of IgG class (16, 17) is thoughtto be the main reason for thrombocytopenia andenhanced thrombin generation (18, 19) in HITpatients. This requires crosslinking of the plateletFcc receptor IIa (20), which results in formation ofprothrombotic microparticles and expression ofprocoagulatory surfaces (16, 21–23). As plateletFccRIIa should not be crosslinked by IgM and IgAantibodies, it remains unclear to what extent anti-PF4/heparin antibodies of the IgM and IgA classare pathogenic.Amiral et al. (24) suggested that anti-PF4/
heparin antibodies of the IgM and IgA class canbe associated with HIT-related thrombotic compli-cations based on 12 patients with putative clinicalHIT in the absence of anti-PF4/heparin antibodiesof the IgG class. In contrast, Lindhoff-Last et al.(25, 26) did not find an increased incidence of anti-PF4 antibodies of the IgM and IgA class in patientswith clinical HIT in a prospective trial. Also Suh etal. (27) reported that only the group of patientswith anti-PF4/heparin antibodies of the IgG classshowed clinical symptoms of HIT, while thepatients with anti-PF4/heparin antibodies of theIgM or IgA class did not. In accordance, Pouplardet al. (28) observed no symptoms of HIT in patientstreated with unfractionated heparin while havingantibodies of the IgM or IgA class. In addition,Warkentin et al. (29) found that detection of IgMand IgA antibodies in the commercial enzyme-linked immunosorbent assay (ELISA) decreasedtest specificity without an offsetting benefit ofincreased test sensitivity in a study of archivedblood samples obtained from prospective clinicaltrials.Data on the frequency of the different anti-PF4/
heparin immunoglobulin classes and how thesetests compare with the functional assays in largeseries of patients with clinically suspected HIT aresparse. The aim of this study was to determine thefrequencies of antibodies reactive in a sensitivefunctional assay using washed platelets and thefrequencies of anti-PF4/heparin antibodies of the
IgG, IgM, and IgA class as determined by a PF4/heparin antigen assay in patients referred to areference center for HIT antibody testing and toassess the association of clinical presentation ofHIT with the test outcomes.
Materials and methods
Patients
Consecutive patients for whom blood samples weresent to our laboratory between January andNovember 2002 were enrolled. Clinical data of allpatients tested positive in the PF4/heparin ELISAand/or the HIPA test such as start of heparintherapy, platelet counts, TEC, and underlyingdisease were obtained from the information provi-ded by the referring physicians and analyzed.
PF4/heparin ELISA
Microtiter plates (Nunc, Roskilde, Denmark) werecoated with 200 lL m-maleimidobenzoyl-n-hydrox-ysulfosuccinimideester (sulfo-MBS; Pierce, Rock-ford, Ireland) 0.125 mg/mL in coating buffer (0.1 m
NaH2PO4, 0.15 m NaCl, 1 mm EDTA Triplex, pH7.5), incubated [5 h, room temperature (RT)],washed five times (0.1 m NaH2PO4, 0.15 m NaCland 9.8 mm MgCl2, pH 7.5) and incubated with200 lL PF4 (20 lg/mL; Chromatec, Greifswald,Germany) and heparin (0.5 IU/mL; Braun, Mel-sungen, Germany) in 0.05 m NaH2PO4, 0.1%,NaN3 (RT, overnight), washed five times (0.15 m
NaCl, 0.1% Tween 20, pH 7.5), and incubated (1 h,RT) with 200 lL patient serum [1 : 50 in 0.05 m
NaH2PO4, 0.15 m NaCl, 7.5% goat normal serum(Dianova, Hamburg, Germany), pH 7.5], washedfive times and incubated (1 h, RT) with thepolyspecific anti-human IgG/A/M peroxidase-con-jugate (Dianova). Plates were washed five times andincubated (3 min, RT) with 100 lL 1,2-o-pheny-lenediamine (Dako, Glostrup, Denmark). Thereaction was stopped by 100 lL of 0.5 m H2SO4,and optical density (OD) was measured at 492 nm.
All sera with a positive result in the polyspecificPF4/heparin-ELISA were analyzed by anti-humanIgG, anti-human IgM or anti-human IgA conju-gates separately (Dianova). An OD above 0.5 wasconsidered positive based on validation using seraof 100 patients with clinical HIT containing HITantibodies in the HIPA test and in a commercialPF4/heparin ELISA, 20 healthy blood donors, and20 non-HIT patients. Results were compared withtwo commercially available PF4/heparin ELISA’s(GTI, Brookfield, WI, USA; Stago, Asnieres,France), the ID-H/PF4 antibody test (DiaMed,Cressier sur Morat, Switzerland), the HIPA test
Laboratory testing for HIT
421

(6, 7) and the 14C-SRA (4, 5) regarding sensitivityand specificity.
HIPA test
The HIPA test was performed as described (6, 7). Itwas considered positive if at least three of fourdonor platelets showed activation in the presence ofpatient serum and low (0.2 IU/mL) but not high(100 IU/mL) heparin concentrations with a lagtime of 30 min or less and all the control wellsreacting as expected. If donor platelets were acti-vated in the presence of both heparin concentra-tions, the HIPA test was indeterminate.
Statistical analysis
Statistical analysis was performed using the SASpackage, version 9.1 (SAS Institute, Cary, NC,USA). Comparisons were performed by the Wilc-oxon rank-sum test and the chi-square test. A P-value <0.05 was considered statistically significant.
Results
Validation of the in-house PF4/heparin ELISA
Using sera of 100 patients with clinical HITcontaining HIT antibodies in the HIPA test and acommercial PF4/heparin ELISA, 20 healthy blooddonors, and 20 non-HIT patients, in the in-houseELISA 96 of 100 positive sera reacted whencompared with 100% in two commercial ELISAs(GTI; Stago). None of the 20 normal sera gave apositive result in the in-house ELISA (mean value:OD 0.093; mean value +2 SD: OD 0.222), but oneof 20 gave an OD >0.5 in the one commercialELISA (GTI; mean value: OD 0.117; meanvalue +2 SD: OD 0.301), and even six of 20 inthe other commercial ELISA (Stago; mean value:OD 0.337; mean value +2 SD: OD 0.604). Withnon-HIT patient sera we obtained for the threeassays: in-house: mean value: OD 0.095; mean value+2 SD: OD 0.227; GTI: mean value: OD 0.210;mean value +2 SD: OD 0.724; Stago: mean value:OD 0.459; mean value +2 SD: OD 1.106). Nodifferences in reactivity were observed between thein-house ELISA and the ID-H/PF4 antibody test.Cutoff values for separate detection of Ig-classes G,A or M were defined >0.5 OD based on plasmasamples from 100 healthy blood donors.
Results of HIT antibody tests
Of 755 patient sera, 108 (14.3%) tested positive forHIT antibodies in the HIPA test and/or in the PF4/heparin ELISA (Table 1). Fifty of 108 (46.3%)
positive samples were positive in both assays, threeof 108 (2.8%) samples were positive in the HIPAtest only, 55 of 108 (50.9%) samples were positivein PF4/heparin ELISA only. Nineteen samples gaveindeterminate results in the HIPA test, of thosefour were positive in the PF4/heparin ELISA.
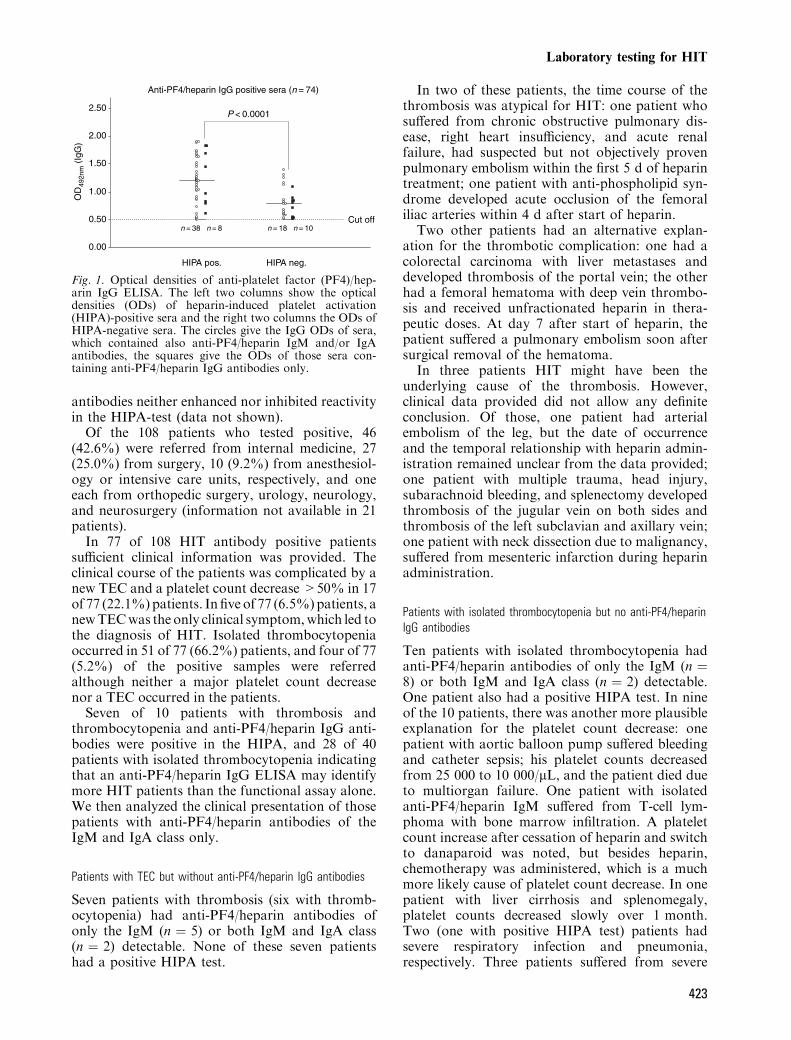
Seventy-four of 105 (70.5%) ELISA-positive serahad anti-PF4/heparin antibodies of the IgG class,either alone or together with IgM or IgA antibodies(Table 2). Anti-PF4/heparin IgM antibodies weredetectable in 74 of 105 (70.5%) patient sera, andanti-PF4/heparin IgA antibodies were present in 39of 105 (37.1%) patients. Of the 74 anti-PF4/heparinIgG-positive sera, 46 were also positive in the HIPAtest (62.2%) when compared with only three of 28(10.7%) sera containing only anti-PF4/heparinantibodies of the IgA or IgM class (P < 0.0001,Table 2). Anti-PF4/heparin IgG-positive serawhich also reacted in the functional assay had ahigher median OD in the ELISA than those whichdid not (Fig. 1). Thus, detectability of IgG classantibodies and high antibody levels (greater ODlevels) were strongly associated with a positiveplatelet activation assay. Coexisting IgM or IgA
Table 1. Results of heparin-induced thrombocytopenia (HIT) antibody tests in theheparin-induced platelet activation (HIPA) test and in the platelat factor (PF4)/heparin IgG/A/M ELISA of 755 patients referred for diagnosis of HIT
HIPA test, n (%)
PF4/heparin IgG/A/M ELISA, n (%)
Positive Negative Total
Positive 50 (6.6) 3 (0.4) 53 (7.0)Indeterminate 4 (0.5) 15 (2.0) 19 (2.5)Negative 51 (6.7) 632 (83.7) 683 (90.4)Total 105 (13.9) 650 (86.1) 755
Table 2. Prevalence of antibodies of the IgG-, IgM-, and IgA-class in 105 patientswith clinically suspected heparin-induced thrombocytopenia (HIT) and positive IgG/M/A platelet factor (PF4)/heparin ELISA
Immunoglobulinclasses of HITantibodies
Monospecific PF4/heparinELISA positive,
n (%)
HIPA positive of 105ELISA positive patients,
n (%)
IgG only 18 (17.1) 8 (7.6)IgG and IgA 10 (9.5) 7 (6.7)IgG and IgM 23 (21.9) 14 (13.3)IgG, IgA, and IgM 23 (21.9) 17 (16.2)All IgG 74 (70.5) 46 (43.8)IgM only 22 (20.9) 2 (1.9)IgM and IgA 6 (5.7) 1 (1)IgA only 0 0Indeterminate1 3 (2.8) 1 (1)Total 105 (100) 502 (47.6)
1In one sample, the immunoglobulin classes could not be determined because oflack of material; two sera were positive in the IgG/M/A PF4/heparin ELISA butnegative in the monospecific ELISA.2Three additional sera were positive in the heparin-induced platelet activation(HIPA) test only.
Juhl et al.
422
antibodies neither enhanced nor inhibited reactivityin the HIPA-test (data not shown).Of the 108 patients who tested positive, 46
(42.6%) were referred from internal medicine, 27(25.0%) from surgery, 10 (9.2%) from anesthesiol-ogy or intensive care units, respectively, and oneeach from orthopedic surgery, urology, neurology,and neurosurgery (information not available in 21patients).In 77 of 108 HIT antibody positive patients
sufficient clinical information was provided. Theclinical course of the patients was complicated by anew TEC and a platelet count decrease >50% in 17of 77 (22.1%)patients. In five of 77 (6.5%)patients, anewTECwas the only clinical symptom,which led tothe diagnosis of HIT. Isolated thrombocytopeniaoccurred in 51 of 77 (66.2%) patients, and four of 77(5.2%) of the positive samples were referredalthough neither a major platelet count decreasenor a TEC occurred in the patients.Seven of 10 patients with thrombosis and
thrombocytopenia and anti-PF4/heparin IgG anti-bodies were positive in the HIPA, and 28 of 40patients with isolated thrombocytopenia indicatingthat an anti-PF4/heparin IgG ELISA may identifymore HIT patients than the functional assay alone.We then analyzed the clinical presentation of thosepatients with anti-PF4/heparin antibodies of theIgM and IgA class only.
Patients with TEC but without anti-PF4/heparin IgG antibodies
Seven patients with thrombosis (six with thromb-ocytopenia) had anti-PF4/heparin antibodies ofonly the IgM (n ¼ 5) or both IgM and IgA class(n ¼ 2) detectable. None of these seven patientshad a positive HIPA test.
In two of these patients, the time course of thethrombosis was atypical for HIT: one patient whosuffered from chronic obstructive pulmonary dis-ease, right heart insufficiency, and acute renalfailure, had suspected but not objectively provenpulmonary embolism within the first 5 d of heparintreatment; one patient with anti-phospholipid syn-drome developed acute occlusion of the femoraliliac arteries within 4 d after start of heparin.
Two other patients had an alternative explan-ation for the thrombotic complication: one had acolorectal carcinoma with liver metastases anddeveloped thrombosis of the portal vein; the otherhad a femoral hematoma with deep vein thrombo-sis and received unfractionated heparin in thera-peutic doses. At day 7 after start of heparin, thepatient suffered a pulmonary embolism soon aftersurgical removal of the hematoma.
In three patients HIT might have been theunderlying cause of the thrombosis. However,clinical data provided did not allow any definiteconclusion. Of those, one patient had arterialembolism of the leg, but the date of occurrenceand the temporal relationship with heparin admin-istration remained unclear from the data provided;one patient with multiple trauma, head injury,subarachnoid bleeding, and splenectomy developedthrombosis of the jugular vein on both sides andthrombosis of the left subclavian and axillary vein;one patient with neck dissection due to malignancy,suffered from mesenteric infarction during heparinadministration.
Patients with isolated thrombocytopenia but no anti-PF4/heparinIgG antibodies
Ten patients with isolated thrombocytopenia hadanti-PF4/heparin antibodies of only the IgM (n ¼8) or both IgM and IgA class (n ¼ 2) detectable.One patient also had a positive HIPA test. In nineof the 10 patients, there was another more plausibleexplanation for the platelet count decrease: onepatient with aortic balloon pump suffered bleedingand catheter sepsis; his platelet counts decreasedfrom 25 000 to 10 000/lL, and the patient died dueto multiorgan failure. One patient with isolatedanti-PF4/heparin IgM suffered from T-cell lym-phoma with bone marrow infiltration. A plateletcount increase after cessation of heparin and switchto danaparoid was noted, but besides heparin,chemotherapy was administered, which is a muchmore likely cause of platelet count decrease. In onepatient with liver cirrhosis and splenomegaly,platelet counts decreased slowly over 1 month.Two (one with positive HIPA test) patients hadsevere respiratory infection and pneumonia,respectively. Three patients suffered from severe
Anti-PF4/heparin IgG positive sera (n = 74)
0.00
0.50
1.00
1.50
2.00
2.50
HIPA pos. HIPA neg.
OD
492n
m (
IgG
)
Cut off
P < 0.0001
n = 38 n = 8 n = 18 n = 10
Fig. 1. Optical densities of anti-platelet factor (PF4)/hep-arin IgG ELISA. The left two columns show the opticaldensities (ODs) of heparin-induced platelet activation(HIPA)-positive sera and the right two columns the ODs ofHIPA-negative sera. The circles give the IgG ODs of sera,which contained also anti-PF4/heparin IgM and/or IgAantibodies, the squares give the ODs of those sera con-taining anti-PF4/heparin IgG antibodies only.
Laboratory testing for HIT
423

sepsis, two of them showed heparin independent,but Fc receptor-dependent platelet activation in theHIPA test compatible with circulating immune-complexes. One patient had a metastatic carcinomaof the kidney and one had arterial occlusive disease.
Discussion
The present study on 755 consecutive patientsreferred for laboratory diagnosis of HIT has severalimplications for interpretation of HIT test results.Only 14.3% of patients tested positive in any of theantibody tests applied. Moreover, only about halfof these (about 7% overall) had the typical sero-logical profile of HIT (positive platelet activationassay and positive ELISA with IgG antibodies).This strongly indicates that HIT is either overdiag-nosed clinically or (more likely) clinicians uselaboratory tests frequently for purposes of �rulingout� HIT as a precautionary measure. Interestingly,only one patient with HIT antibodies followingorthopedic surgery was detected within the 9-month study period, whereas more than 50% ofthe patients testing positive were medical (42.6%)or intensive care patients (9.2%). This contrastswith our study of HIT during 1994–1997 (30) inwhich almost one-third of patients recognized withHIT were postorthopedic surgery. This majordecline in the relative frequency of HIT in thispatient population is most likely the result of theuse of low-molecular weight heparin, rather thanunfractionated heparin, in Germany for postoper-ative thrombosis prophylaxis (31). Thus, todayHIT seems to be more predominant in other patientgroups in whom unfractionated heparin is stillfrequently used. While a decrease in platelet countin an otherwise healthy patient following electiveorthopedic surgery is rather indicative for HIT (32),medical, and ICU patients often have many poten-tial reasons besides HIT for a decrease in plateletcount or TEC.
Our study shows that antigen assays are suitablefor ruling out HIT in the vast majority of patients.Only three patients tested positive in the functionalassay only (2.8% of all positive sera or 0.4% of allreferred sera). In these patients other antigens asNAP-2 or IL-8 may have been involved (8). Incontrast, antigen assays seem to be problematic forconfirming the diagnosis of HIT. About twice asmany patients tested positive in the ELISA whencompared with the functional assay, and 28(26.7%) of them had anti-PF4/heparin antibodiesof the IgM and IgA class only. Considering thatanti-PF4/heparin antibodies of the IgG class arenecessary to cause activation of platelets, theclinical relevance of anti-PF4/heparin antibodiesof the IgM or IgA class is unclear. Using a
laboratory test for HIT-diagnosis, which is highlysensitive but which detects clinically irrelevantantibodies in these patients bears the risk tooverdiagnose HIT and to switch patients to newanticoagulants such as lepirudin and argatrobanunnecessarily. This may even harm patients, asthese new anticoagulants had a risk for majorbleeding of approximately 20% in prospective trials(33).
We therefore correlated the available clinicalinformation with the class of the HIT antibodies inthe 77 patients in whom sufficient clinical informa-tion was provided. Of those 22 patients with a newTEC during heparin treatment, 14 had anti-PF4/heparin IgG antibodies, of which nine were positivein the platelet function assay. Of the 51 patientswith thrombocytopenia only, 40 had anti-PF4/heparin IgG, of which 28 also tested positive in thefunctional assay. Those testing positive in theplatelet functional assay had a higher mean ODin the PF4/heparin IgG ELISA (Fig. 1), which is inline with the data of previous studies (34) andindicates that an anti-PF4/heparin IgG ELISAprovides relevant additional information to thefunctional assay. Three sera tested positive in thefunctional assay but contained only anti-PF4/hep-arin IgM and/or IgA. Potentially these sera alsocontained anti-IL-8 or NAP-2 IgG antibodies.Assessing the thrombotic complications (n ¼ 7)and the decrease in platelet counts (n ¼ 10) inthose patients with anti-PF4/heparin IgM and IgAantibodies only, suggests that the antibodies detec-ted are often an epiphenomenon and probably notthe cause of the decrease of platelet counts or thenew thrombotic complication. Thrombosis oc-curred in two patients before day 5, which isatypical for HIT and in two further patients therewere likely alternative explanations for the throm-botic complication. Also, in nine patients withisolated thrombocytopenia, sepsis/infection, anti-neoplastic chemotherapy, and cirrhosis were morelikely reasons for the decrease of platelet countsthan HIT.
This is in line with a prospective trial (35), inwhich none of the patients with a negative func-tional assay presented with clinical symptoms ofHIT. Although the retrospective nature of ourstudy and the partly limited information providedby the treating physicians do not allow definitiveconclusions, it strongly indicates in a large group ofpatients with clinically suspected HIT that PF4/heparin antigen assays are a useful first-line tool torule out HIT. However, our study also indicatesthat results of the antigen assays alone should beinterpreted with caution and only in the context ofthe clinical presentation of the patient. By usingantigen assays detecting also anti-PF4/heparin
Juhl et al.
424
antibodies of the IgM, and IgA class, HIT may belargely overdiagnosed. Studies systematically link-ing detailed information on the clinical presenta-tion of the patient and anti-PF4/heparin test resultsare urgently needed to further understand theimpact of anti-PF4/heparin antibodies of the IgMand IgA class on clinical HIT.
Acknowledgments
This work was supported by Deutsche Forschungsgemeinsc-haft, Gr 1096/2-4; German Federal Ministry for Education andResearch (CAN04/006; NBL3 program, reference 01-ZZ0403),Forschungsverbund Molekulare Medizin, Projekt An-schubforderung �Untersuchungen zur klinischen Relevanz derImmunglobulinklassen IgG, -A, -M bei Heparin-induzierterThrombozytopenie (HIT) und weitere Charakterisierung derAntikorper�; and is part of the Department of CardiovascularMedicine of the Medical Faculty at the Ernst-Moritz-Arndt-University Greifswald.
References
1. Warkentin TE, Kelton JG. Temporal aspects of heparin-induced thrombocytopenia. N Engl J Med 2001;344:1286–1292.
2. Lubenow N, Kempf R, Eichner A, Eichler P, CarlssonLE, Greinacher A. Heparin-induced thrombocytopenia:temporal pattern of thrombocytopenia in relation to initialuse or reexposure to heparin. Chest 2002;122:37–42.
3. Warkentin TE, Greinacher A. Laboratory testing forheparin-induced-thrombocytopenia. In: Warkentin TE
and Greinacher A, eds. Heparin-induced Thrombocy-topenia, 3rd edn. Basel, New York: Marcel Dekker Inc.,2004:271–313.
4. Sheridan D, Carter C, Kelton JG. A diagnostic testfor heparin-induced thrombocytopenia. Blood 1986;67:27–30.
5. Warkentin TE, Hayward CPM, Smith CA, Kelly PM,Kelton JG. Determinants of donor platelet variabilitywhen testing for heparin-induced thrombocytopenia. J LabClin Med 1992;120:371–379.
6. Greinacher A,Michels I,Kiefel V,Mueller-Eckhardt
C. A rapid and sensitive test for diagnosing heparin-asso-ciated thrombocytopenia. Thromb Haemost 1991;66:734–736.
7. Eichler P, Budde U, Haas S, et al. First workshop fordetection of heparin-induced antibodies: validation of theheparin-induced platelet-activation test (HIPA) in com-parison with a PF4/heparin ELISA. Thromb Haemost1999;81:625–629.
8. Amiral J, Marfaing-Koka A, Wolf M, Alessi MC,Tardy B, Boyer-Neumann C, Vissac AM, Fressinaud E,Poncz M, Meyer D. Presence of autoantibodies to inter-leukin-8 or neutrophil-activating peptide-2 in patients withheparin-associated thrombocytopenia. Blood 1996;88:410–416.
9. Amiral J, Bridey F,Dreyfus M, Vissac AM, FressinaudE, Wolf M, Meyer D. Platelet factor 4 complexed toheparin is the target for antibodies generated in heparin-induced thrombocytopenia [letter]. Thromb Haemost1992;68:95–96.
10. Greinacher A, Poetzsch B, Amiral J, Dummel V,Eichner A, Mueller-Eckhardt C. Heparin-associatedthrombocytopenia: isolation of the antibody and charac-terization of a multimolecular PF4-heparin complex as themajor antigen. Thromb Haemost 1994;71:247–251.
11. Kelton JG, Smith JW, Warkentin TE, Hayward CPM,Denomme GA, Horsewood P. Immunoglobulin G frompatients with heparin-induced thrombocytopenia binds to acomplex of heparin and platelet factor 4. Blood1994;83:3232–3239.
12. Amiral J, Bridey F, Wolf M, Boyer-Neumann C,Fressinaud E, Vissac AM, Peynaud-Debayle E, Drey-
fus M, Meyer D. Antibodies to macromolecular plateletfactor 4-heparin complexes in heparin-induced thrombo-cytopenia: a study of 44 cases. Thromb Haemost1995;73:21–28.
13. Visentin GP, Ford SE, Scott JP, Aster RH. Antibodiesfrom patients with heparin-induced thrombocytopenia/thrombosis are specific for platelet factor 4 with heparin orbound to endothelial cells. J Clin Invest 1994;93:81–88.
14. Meyer O, Salama A, Pittet N, Schwind P. Rapiddetection of heparin-induced platelet antibodies with par-ticle gel immunoassay (ID-HPF-4). Lancet 1999;354:1525–1526.
15. Eichler P, Raschke R, Lubenow N, Meyer O, SchwindP, Greinacher A. The new ID-heparin/PF-4 antibody testfor rapid detection of heparin-induced antibodies in com-parison with functional and antigenic assays. Br J Hae-matol 2002;116:887–891.
16. Warkentin TE, Hayward CP, Boshkov LK, Santos AV,Sheppard JA, Bode AP, Kelton JG. Sera from patientswith heparin-induced thrombocytopenia generate platelet-derived microparticles with procoagulant activity: anexplanation for the thrombotic complications of heparin-induced thrombocytopenia. Blood 1994;84:3691–3699.
17. Chong BH, Pilgrim LR, Cooley MA, Chesterman CN.Increased expression of platelet IgG Fc receptors in im-mune heparin-induced thrombocytopenia. Blood1993;81:988–993.
18. Warkentin TE. Heparin-induced thrombocytopenia.Pathogenesis. Frequency, avoidance and management.Drug Saf 1997;17:325–341.
19. Greinacher A. Heparin-induced thrombocytopenia-path-ogenesis and treatment. Thromb Haemost 1999;82(Suppl.1): 148–156.
20. Kelton JG, Sheridan D, Santos A, Smith J, Steeves K,Smith C, Brown C, Murphy WG. Heparin-inducedthrombocytopenia: laboratory studies. Blood 1988;72:925–930.
21. Lee DH, Warkentin TE, Denomme GA, Hayward CPM,Kelton JG. A diagnostic test for heparin-inducedthrombocytopenia: detection of platelet microparticlesusing flow cytometrie. Br J Hematol 1996;95:724–731.
22. Tomer A. A sensitive and specific functional flow cyto-metric assay for the diagnosis of heparin-induced thromb-ocytopenia. Br J Haematol 1997;98:648–656.
23. Hughes M, Hayward CPM, Warkentin TE, Horsewood
P, Chorneyko KA, Kelton JG. Morphological analysis ofmicroparticle generation in heparin-induced thrombo-cytopenia. Blood 2000;96:188–194.
24. Amiral J, Wolf M, Fischer AM, Boyer-Neumann C,Vissac AM, Meyer D. Pathogenicity of IgA and/or IgMantibodies to heparin- PF4 complexes in patients withheparin-induced thrombocytopenia. Br J Haematol1996;92:654–659.
25. Lindhoff-Last E, Gerdsen F, Ackermann H, Bauer-
sachs R. Determination of heparin-platelet factor 4-IgGantibodies improves diagnosis of heparin-induced thromb-ocytopenia. Br J Haematol 2001;113:886–890.
26. Lindhoff-Last E, Eichler P, Stein M, Plagemann J,Gerdsen F, Wagner R, Ehrly AM, Bauersachs R. Aprospective study on the incidence and clinical relevance ofheparin-induced antibodies in patients after vascular sur-gery. Thromb Res 2000;97:387–393.
Laboratory testing for HIT
425

27. Suh JS, Malik MI, Aster RH, Visentin GP. Characteri-zation of the humoral immune response in heparin-inducedthrombocytopenia. Am J Hematol 1997;54:196–201.
28. Pouplard C, May MA, Iochmann S, Amiral J, VissacAM, Marchand M, Gruel Y. Antibodies to platelet fac-tor 4-heparin after cardiopulmonal bypass in patientsanticoagulated with unfractionated heparin or a low-molecular weight heparin: clinical implications for heparin-induced thrombocytopenia. Circulation 1999;99:2530–2536.
29. Warkentin TE, Sheppard JI, Moore JC, Moore KM,Sigouin CS, Kelton JG. Laboratory testing for the anti-bodies that cause heparin-induced thrombocytopenia: howmuch class do we need? J Lab Clin Med 2005;146:341–346.
30. Greinacher A, Farner B, Kroll H, Kohlmann T,Warkentin TE, Eichler P. Clinical features of heparin-induced thrombocytopenia including risk factors forthrombosis. A retrospective analysis of 408 patients.Thromb Haemost 2005;94:132–135.
31. Greinacher A, Eichler P, Lietz T, Warkentin TE.Replacement of unfractionated heparin by low-molecular
weight heparin for postorthopedic surgery antithromboticprophylaxis lowers the overall risk of symptomatic throm-bosis because of a lower frequency of heparin-inducedthrombocytopenia. Blood 2005, 106:2921–2922.
32. Warkentin TE, Roberts RS, Hirsh J, Kelton JG. Animproved definition of immune heparin-induced thrombo-cytopenia in postoperative orthopedic patients. Arch InternMed 2003;163:2518–2524.
33. Greinacher A, Warkentin TE. Recognition, treatment,and prevention of heparin-induced thrombocytopenia:review and update. Thromb Res 2006 (in press). Epubahead of print August 2005.
34. Zwicker JI, Uhl L, Huang WY, Shaz BH, Bauer KA.Thrombosis and ELISA optical density values in hospital-ized patients with heparin-induced thrombocytopenia. JThromb Haemost 2004;2:2133–2137.
35. Warkentin TE, Sheppard JI, Horsewood P, Simpson PJ,Moore JC, Kelton JG. Impact of patient population onthe risk for heparin-induced thrombocytopenia. Blood2000;96:1703–1708.
Juhl et al.
426