
Inadvertent Intrathecal Injection of Ionic Contrast â•fi ...
2
Henry Ford Health System Henry Ford Health System Scholarly Commons Case Reports Medical Education Research Forum 2019 5-2019 Inadvertent Intrathecal Injection of Ionic Contrast – Seeing is Believing! Gaurav Chauhan Henry Ford Health System Aman Upadhyay Henry Ford Health System Mun Choe Henry Ford Health System Joseph Salama Hanna Henry Ford Health System Follow this and additional works at: hps://scholarlycommons.henryford.com/merf2019caserpt is Poster is brought to you for free and open access by the Medical Education Research Forum 2019 at Henry Ford Health System Scholarly Commons. It has been accepted for inclusion in Case Reports by an authorized administrator of Henry Ford Health System Scholarly Commons. For more information, please contact [email protected]. Recommended Citation Chauhan, Gaurav; Upadhyay, Aman; Choe, Mun; and Salama Hanna, Joseph, "Inadvertent Intrathecal Injection of Ionic Contrast – Seeing is Believing!" (2019). Case Reports. 9. hps://scholarlycommons.henryford.com/merf2019caserpt/9
Transcript of Inadvertent Intrathecal Injection of Ionic Contrast â•fi ...

Henry Ford Health SystemHenry Ford Health System Scholarly Commons
Case Reports Medical Education Research Forum 2019
5-2019
Inadvertent Intrathecal Injection of Ionic Contrast– Seeing is Believing!Gaurav ChauhanHenry Ford Health System
Aman UpadhyayHenry Ford Health System
Mun ChoeHenry Ford Health System
Joseph Salama HannaHenry Ford Health System
Follow this and additional works at: https://scholarlycommons.henryford.com/merf2019caserpt
This Poster is brought to you for free and open access by the Medical Education Research Forum 2019 at Henry Ford Health System ScholarlyCommons. It has been accepted for inclusion in Case Reports by an authorized administrator of Henry Ford Health System Scholarly Commons. Formore information, please contact [email protected].
Recommended CitationChauhan, Gaurav; Upadhyay, Aman; Choe, Mun; and Salama Hanna, Joseph, "Inadvertent Intrathecal Injection of Ionic Contrast –Seeing is Believing!" (2019). Case Reports. 9.https://scholarlycommons.henryford.com/merf2019caserpt/9
Abstract CLINICAL VIGNETTE
INTRODUCTION
DISCUSSION
REFERENCES
Inadvertent intrathecal injection of ionic contrast – seeing is believing !
Gaurav Chauhan, MD, Aman Upadhyay, MD, Mun Choe, MD, Joseph M Salama-Hanna, MD
Department of Anesthesiology, Pain Management and Perioperative Medicine
Henry Ford Health System, Detroit, Michigan
The intravenous administration of gadopentetate dimeglumine (GD) is relatively safe and rarely causes
systemic toxicity in the course of routine imaging studies. However, the general safety of intrathecal GD has
not been established. We report a very rare case of an overdose intrathecal GD injection presenting with
neurotoxic manifestations, including a decreased level of consciousness, global aphasia, rigidity, and visual
disturbance. In our case due to his shellfish allergy the physician elected to use a gadolinium based contrast
rather than the standard iodinated contrast dye. The patient’s epidural resulted in an inadvertent intrathecal
injection of GD. In this case report the authors will discuss the pathophysiology and neurological sequlae of
intrathecal GD injection along with the current guidelines for management.
• Gadolinium is a rare paramagnetic metal and GD3 + ion is he most
effective paramagnetic ion. Gadolinium based contrast agents (GBCAs)
are widely used in medicine since 1988.
• GD3 + is a toxic ion which is chelated with organic ligands to create
GBCAs with either a linear or macrocyclic structure. Following
intravenous injection, all GBCAs distribute in the blood and
extravascular–extracellular space. GBCAs are biologically inert and
rapidly eliminated by the kidneys.
• GBCA are administered in about 25% of all MRI examinations. They
are also widely used to facilitate chronic pain procedures under
fluoroscopy. The intravenous application of GD is relatively safe and
rarely causes systemic toxicity in the course of routine imaging studies
• But the impact of GBCA on human health and its mechanism of toxicity
remains unknown. Efforts are underway to understand the mechanisms
of gadolinium toxicity and to therapeutic and preventive solutions for
patients presenting signs and symptoms of gadolinium toxicity. We
present a case report of acute Gadobutrol neurotoxicity and its sequlae.
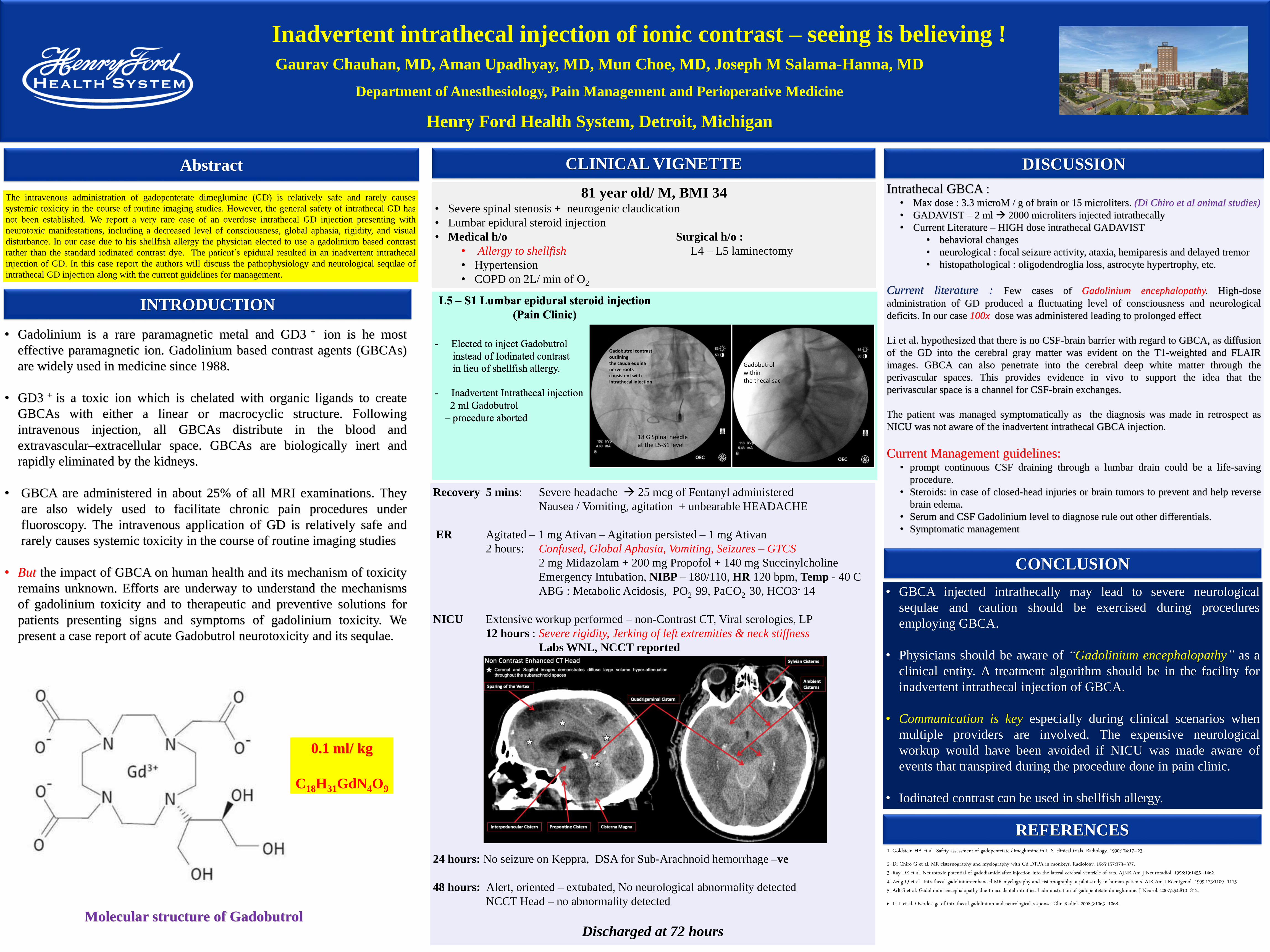
Molecular structure of Gadobutrol
0.1 ml/ kg
C18H31GdN4O9
81 year old/ M, BMI 34 • Severe spinal stenosis + neurogenic claudication
• Lumbar epidural steroid injection
• Medical h/o Surgical h/o :
• Allergy to shellfish L4 – L5 laminectomy
• Hypertension
• COPD on 2L/ min of O2
Gadobutrol contrast outlining the cauda equina nerve rootsconsistent with intrathecal injection.
Gadobutrol within the thecal sac
18 G Spinal needle at the L5-S1 level
Recovery 5 mins: Severe headache 25 mcg of Fentanyl administered
Nausea / Vomiting, agitation + unbearable HEADACHE
ER Agitated – 1 mg Ativan – Agitation persisted – 1 mg Ativan
2 hours: Confused, Global Aphasia, Vomiting, Seizures – GTCS
2 mg Midazolam + 200 mg Propofol + 140 mg Succinylcholine
Emergency Intubation, NIBP – 180/110, HR 120 bpm, Temp - 40 C
ABG : Metabolic Acidosis, PO2 99, PaCO2 30, HCO3- 14
NICU Extensive workup performed – non-Contrast CT, Viral serologies, LP
12 hours : Severe rigidity, Jerking of left extremities & neck stiffness
Labs WNL, NCCT reported
24 hours: No seizure on Keppra, DSA for Sub-Arachnoid hemorrhage –ve
48 hours: Alert, oriented – extubated, No neurological abnormality detected
NCCT Head – no abnormality detected
Discharged at 72 hours
CONCLUSION
Intrathecal GBCA :• Max dose : 3.3 microM / g of brain or 15 microliters. (Di Chiro et al animal studies)
• GADAVIST – 2 ml 2000 microliters injected intrathecally
• Current Literature – HIGH dose intrathecal GADAVIST
• behavioral changes
• neurological : focal seizure activity, ataxia, hemiparesis and delayed tremor
• histopathological : oligodendroglia loss, astrocyte hypertrophy, etc.
Current literature : Few cases of Gadolinium encephalopathy. High-dose
administration of GD produced a fluctuating level of consciousness and neurological
deficits. In our case 100x dose was administered leading to prolonged effect
Li et al. hypothesized that there is no CSF-brain barrier with regard to GBCA, as diffusion
of the GD into the cerebral gray matter was evident on the T1-weighted and FLAIR
images. GBCA can also penetrate into the cerebral deep white matter through the
perivascular spaces. This provides evidence in vivo to support the idea that the
perivascular space is a channel for CSF-brain exchanges.
The patient was managed symptomatically as the diagnosis was made in retrospect as
NICU was not aware of the inadvertent intrathecal GBCA injection.
Current Management guidelines:• prompt continuous CSF draining through a lumbar drain could be a life-saving
procedure.
• Steroids: in case of closed-head injuries or brain tumors to prevent and help reverse
brain edema.
• Serum and CSF Gadolinium level to diagnose rule out other differentials.
• Symptomatic management
• GBCA injected intrathecally may lead to severe neurological
sequlae and caution should be exercised during procedures
employing GBCA.
• Physicians should be aware of “Gadolinium encephalopathy” as a
clinical entity. A treatment algorithm should be in the facility for
inadvertent intrathecal injection of GBCA.
• Communication is key especially during clinical scenarios when
multiple providers are involved. The expensive neurological
workup would have been avoided if NICU was made aware of
events that transpired during the procedure done in pain clinic.
• Iodinated contrast can be used in shellfish allergy.
1. Goldstein HA et al Safety assessment of gadopentetate dimeglumine in U.S. clinical trials. Radiology. 1990;174:17–23.
2. Di Chiro G et al. MR cisternography and myelography with Gd-DTPA in monkeys. Radiology. 1985;157:373–377.3. Ray DE et al. Neurotoxic potential of gadodiamide after injection into the lateral cerebral ventricle of rats. AJNR Am J Neuroradiol. 1998;19:1455–1462.4. Zeng Q et al Intrathecal gadolinium-enhanced MR myelography and cisternography: a pilot study in human patients. AJR Am J Roentgenol. 1999;173:1109–1115.5. Arlt S et al. Gadolinium encephalopathy due to accidental intrathecal administration of gadopentetate dimeglumine. J Neurol. 2007;254:810–812.
6. Li L et al. Overdosage of intrathecal gadolinium and neurological response. Clin Radiol. 2008;3:1063–1068.


















