
In vivo biostability of polysiloxane polyether polyurethanes: Resistance to metal ion oxidation
10
In vivo biostability of polysiloxane polyether polyurethanes: Resistance to metal ion oxidation Bob Ward, 1 James Anderson, 2 Mike Ebert, 3 Rick McVenes, 3 Ken Stokes 3 1 The Polymer Technology Group, 2810 7th St., Berkeley, California 94710 2 Institute of Pathology, Case Western Reserve University, Cleveland, Ohio 44106 3 Medtronic, Inc., 7000 Central Avenue, NE Minneapolis, Minnesota 55432 Received 18 June 2005; accepted 25 July 2005 Published online 19 January 2006 in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/jbm.a.30553 Abstract: Polyether polyurethanes are subject to oxidation catalyzed by and through direct (redox) reaction with tran- sition metal ions (cobalt), released by corrosion of metallic parts in an implanted device. Replacing part of the polyether with polysiloxane appears to reduce susceptibility to metal ion oxidation (MIO). In vitro studies indicated that polyure- thanes containing 20 –35% polysiloxane (PS-20 and PS-35) are about optimum. We implanted tubing samples contain- ing cobalt mandrels in the subcutis of rabbits for periods up to 2 years. After 2 years, only traces of microscopic cracks were seen on half the PS-35 samples, PS-20 significantly delayed MIO, while the polysiloxane-free control was very severely degraded. Infrared spectroscopy established that polyether soft segment oxidation was occurring in PS-20. We could not directly evaluate oxidation in PS-35 because silox- ane bands mask the aliphatic ether. Indirect FTIR evidence suggests that there is very slight polyether oxidation that develops early, and then seems to stabilize. The molecular weight of degraded PS-20 decreased. That of microcracked PS-35 decreased negligibly while that of undamaged PS-35 increased slightly after 2-year in vivo. The polysiloxane-free control was profoundly degraded. PS-20 has much im- proved MIO resistance, while that for PS-35 is highly MIO resistant compared with its polysiloxane-free control. © 2006 Wiley Periodicals, Inc. J Biomed Mater Res 77A: 380 –389, 2006 Key words: silicone modified polyurethane; polyurethane; biostability; MIO INTRODUCTION Polyether polyurethane elastomers have long been considered ideal for many implantable de- vices, such as blood pump diaphragms, pacemaker lead insulation, shunts, spinal disks, and many more. These polymers are well known to have su- perior biocompatibility with mechanical properties ranging from soft and flexible to hard and rigid. All polymers appear to be susceptible to some form of biodegradation. 1 In the case of polyether polyure- thane elastomers, biologic oxidation and environ- mental stress cracking (ESC) can affect the lower modulus polymers such as Pellethane 2363– 80A (P80A). These mechanisms are intimately associated with macrophage and foreign body giant cell adhe- sion to the device surface. 2,3 Another degradation mechanism that may be unique to implantable pace- maker and defibrillator leads is oxidation catalyzed by and through direct reaction with transition metal corrosion products of metallic components within the device. The cause is cobalt ion released from MP35N conductors. Because the reaction is initiated at the soft segment ether’s carbon, the softer the polymer the more susceptible it is. Thus, the harder, more rigid materials, containing the lowest percent- age of polyether, are the most biostable. The harder, stiffer polyurethanes have been used with great suc- cess in some devices, such as cardiac pacing leads. 4 Nonetheless, the lack of a highly biostable, soft, flexible polyurethane places significant restrictions on design, and effectively eliminates the develop- ment of some devices intended for very long im- plant times. One approach to improve the biostability of the softer polyurethanes is to replace some or all of the polyether with more oxidation resistant polysiloxane. This study was aimed at evaluating the in vitro resis- tance to metal ion oxidation (MIO) of a series of Shore 80A polymers with various amounts of polyether re- placed with polysiloxane, and then verifying those results in vivo. Correspondence to: K. Stokes, Medtronic, Inc., 7000 Central Avenue, NE Minneapolis, MN 55432, USA; e-mail: [email protected] © 2006 Wiley Periodicals, Inc.
Transcript of In vivo biostability of polysiloxane polyether polyurethanes: Resistance to metal ion oxidation
In vivo biostability of polysiloxane polyetherpolyurethanes: Resistance to metal ion oxidation
Bob Ward,1 James Anderson,2 Mike Ebert,3 Rick McVenes,3 Ken Stokes3
1The Polymer Technology Group, 2810 7th St., Berkeley, California 947102Institute of Pathology, Case Western Reserve University, Cleveland, Ohio 441063Medtronic, Inc., 7000 Central Avenue, NE Minneapolis, Minnesota 55432
Received 18 June 2005; accepted 25 July 2005Published online 19 January 2006 in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/jbm.a.30553
Abstract: Polyether polyurethanes are subject to oxidationcatalyzed by and through direct (redox) reaction with tran-sition metal ions (cobalt), released by corrosion of metallicparts in an implanted device. Replacing part of the polyetherwith polysiloxane appears to reduce susceptibility to metalion oxidation (MIO). In vitro studies indicated that polyure-thanes containing 20–35% polysiloxane (PS-20 and PS-35)are about optimum. We implanted tubing samples contain-ing cobalt mandrels in the subcutis of rabbits for periods upto 2 years. After 2 years, only traces of microscopic crackswere seen on half the PS-35 samples, PS-20 significantlydelayed MIO, while the polysiloxane-free control was veryseverely degraded. Infrared spectroscopy established thatpolyether soft segment oxidation was occurring in PS-20. Wecould not directly evaluate oxidation in PS-35 because silox-
ane bands mask the aliphatic ether. Indirect FTIR evidencesuggests that there is very slight polyether oxidation thatdevelops early, and then seems to stabilize. The molecularweight of degraded PS-20 decreased. That of microcrackedPS-35 decreased negligibly while that of undamaged PS-35increased slightly after 2-year in vivo. The polysiloxane-freecontrol was profoundly degraded. PS-20 has much im-proved MIO resistance, while that for PS-35 is highly MIOresistant compared with its polysiloxane-free control. © 2006Wiley Periodicals, Inc. J Biomed Mater Res 77A: 380–389,2006
Key words: silicone modified polyurethane; polyurethane;biostability; MIO
INTRODUCTION
Polyether polyurethane elastomers have longbeen considered ideal for many implantable de-vices, such as blood pump diaphragms, pacemakerlead insulation, shunts, spinal disks, and manymore. These polymers are well known to have su-perior biocompatibility with mechanical propertiesranging from soft and flexible to hard and rigid. Allpolymers appear to be susceptible to some form ofbiodegradation.1 In the case of polyether polyure-thane elastomers, biologic oxidation and environ-mental stress cracking (ESC) can affect the lowermodulus polymers such as Pellethane 2363– 80A(P80A). These mechanisms are intimately associatedwith macrophage and foreign body giant cell adhe-sion to the device surface.2,3 Another degradationmechanism that may be unique to implantable pace-
maker and defibrillator leads is oxidation catalyzedby and through direct reaction with transition metalcorrosion products of metallic components withinthe device. The cause is cobalt ion released fromMP35N conductors. Because the reaction is initiatedat the soft segment ether’s � carbon, the softer thepolymer the more susceptible it is. Thus, the harder,more rigid materials, containing the lowest percent-age of polyether, are the most biostable. The harder,stiffer polyurethanes have been used with great suc-cess in some devices, such as cardiac pacing leads.4
Nonetheless, the lack of a highly biostable, soft,flexible polyurethane places significant restrictionson design, and effectively eliminates the develop-ment of some devices intended for very long im-plant times.
One approach to improve the biostability of thesofter polyurethanes is to replace some or all of thepolyether with more oxidation resistant polysiloxane.This study was aimed at evaluating the in vitro resis-tance to metal ion oxidation (MIO) of a series of Shore80A polymers with various amounts of polyether re-placed with polysiloxane, and then verifying thoseresults in vivo.
Correspondence to: K. Stokes, Medtronic, Inc., 7000 CentralAvenue, NE Minneapolis, MN 55432, USA; e-mail:[email protected]
© 2006 Wiley Periodicals, Inc.

MATERIALS
A series of Shore 80A thermoplastic polysiloxane poly-ether polyurethanes were synthesized by The Polymer Tech-nology Group, Berkley, CA. These were synthesized withtelechelic polydimethyl siloxane diol and 1000 Da polytet-ramethylene ether diol soft segments. The hard segmentswere diphenyl methane diisocyanate and butane diol. Thepolymers contained from 10 to 61% polysiloxane, as shownin Table I (PurSil-10, 20, 35, and 61; PS-10, PS-20, PS-35, andPS-61, respectively). A small percentage of the endgroupswere polydimethyl siloxane. Controls included the samepolymer, but with only polytetramethylene oxide soft seg-ment, Pellethane 2363–80A (P80A), Dow Chemical, Mid-land, MI.
METHODS
The polymers were desiccant hopper dried, and then ex-truded into �0.072 in. � 0.082 in. diameter tubing on a 5/8in. Randcastle Microtruder, Model 0625. A minimum of 2weeks laboratory ambient conditioning was allowed beforeany sample preparation or testing was done. Tensile prop-erties were measured on a Sintech Model 30/D machine.
One end of about a 0.75–1.0 in. long section of tubing wasplugged with medical adhesive and allowed to dry over-night. About 0.5-in. long, 0.060-in. diameter cobalt mandrelsmachined with acme grooves (see Fig. 1) were thoroughlycleaned and degreased, and then inserted into the tubing.The other end of the tubing was plugged with medicaladhesive (being careful not to make contact with the cobaltmandrel) and allowed to air dry. About a 1-mm diameterhole was made in one end of the specimen to assure accessof test fluid or exudate/transudate upon implant. The endsof the samples were pierced through the silicone rubber
plug with 2-O polyester suture material. The suture materialwas then tied together to form strings of up to five sampleseach. Each string was identified with a colored glass bead.All samples were packaged, ethylene oxide sterilized, andaerated.
Some specimens were immersed in 37°C, 3% H2O2 solu-tion in n-saline. The solution was changed three times perweek. Samples were examined microscopically at least onceper week with digital photos taken to document observa-tions. Samples of the entire series of polymers were testedwith observations at 105 days reported here. The samplesremained on test for up to 252 days, when significant deg-radation was seen on all materials, at which point they weredisassembled and scored, as shown in Table II.
Chronic animal implants were done with PS-20, PS-35,and controls. Four sterile strands were implanted in thedorsal subcutis of each of 23 rabbits under general anesthe-sia. NIH guidelines for the care and use of laboratory ani-mals (NIH Publication no. 85–23 Rev. 1985) were observed.Animals were sacrificed and samples explanted after 6, 12,18, and 24-month implant. After euthanasia, the animal’sskin was reflected to expose the specimens and the sur-rounding fibrotic capsules. The implant sites were photo-graphed and the photos archived. If no untoward resultswere observed, the samples were dissected free with theiradjacent tissues and stored in Bacteriostat/saline solutionuntil they could be debrided. All implant, explant, and dailyanimal care records were archived.
All explanted samples were debrided, allowed to air dry,and then were examined microscopically at 7.5–60� on anOlympus SXH binocular microscope. Digital micrographs ofeach sample were taken with a Hitachi HV-C20 camera. Thevisual depth and surface area affected by cracking wasscored with a number, as shown in Table II. All 24-monthexplants and controls were examined without any coatingon an Olympus S-4500 scanning electron microscope (SEM)at 500–700 V, with 10 �A emission current, and a 19-mmworking distance. All 2-year samples were photographed at250�, with maximum crack depth determined on cross sec-tions. After SEM, samples were removed from the conduc-tive adhesive. Any residual adhesive was removed by gentlerubbing with a Q-tip in water. Samples were then submittedfor Fourier Transform Infrared Spectroscopy (FTIR) and mo-lecular weight distribution.
Representative 2-year explants were examined on a Per-kin–Elmer System 1720-X FTIR Spectrometer equipped witha Spectra-Tech IR-PLAN IV microscope and an attenuatedtotal reflectance objective (ZnSe internal reflection element,45° angle of incidence). Spectra were baseline-flattened,
TABLE IPolysiloxane Concentrations in Experimental Polymers
Polymer P80A PS-10 PS-20 PS-35 PS-61
Siloxane (wt %) 0 10 20 35 61Polyether replaced
(wt %) 0 17 34 60 100
Figure 1. A 0.5-inch-long grooved cobalt mandrel is in-serted into tubing, which is sealed on both ends with med-ical adhesive. A 1-mm diameter hole is made in one end toassure ingress of exudate/transudate.
TABLE IIOptical Microscopic ESC Visual Score Chart
Percentage ofWall Cracked
Percentage of Surface Affected
1–20 21–40 41–60 61–80 81–100
No defect 0Possible defect 1 2 3 4 5Trace to 30% 6 7 8 9 1031–70% 11 12 13 14 1571–99% 16 17 18 19 20100% 21 22 23 24 25
IN VIVO BIOSTABILITY OF POLYSILOXANE POLYETHER POLYURETHANES 381
smoothed, and normalized on the peak between 1410 and1415 cm�1 (hard segment benzene ring in-plane CACstretch). Peak amplitude ratios were used for quantitativeanalyses. The hydrogen-bonding index is the ratio ofbonded carbonyl stretch (about 1705 cm�1) to free carbonylstretch (about 1730 cm�1). The ether index is the ratio ofaliphatic ether (COOOC) stretch (about 1107 cm�1) to theurethane ether stretch (NOCOOOC, about 1079 cm�1).
Molecular weight distributions were obtained with an HP1090A HPLC, using two Plgel-10 �m mixed bed columnsand a guard column. The solvent and mobile phases weredimethyl formamide and LiBr.
All explanted samples were stored in a freezer so thatcomparative analysis at later dates could assure minimaltime-related postexplant changes.
Statistical analysis used Excel 2000 data analysis package,two-tailed t-test assuming equal variances. p � 0.05 wasconsidered significant.
RESULTS
Mechanical properties
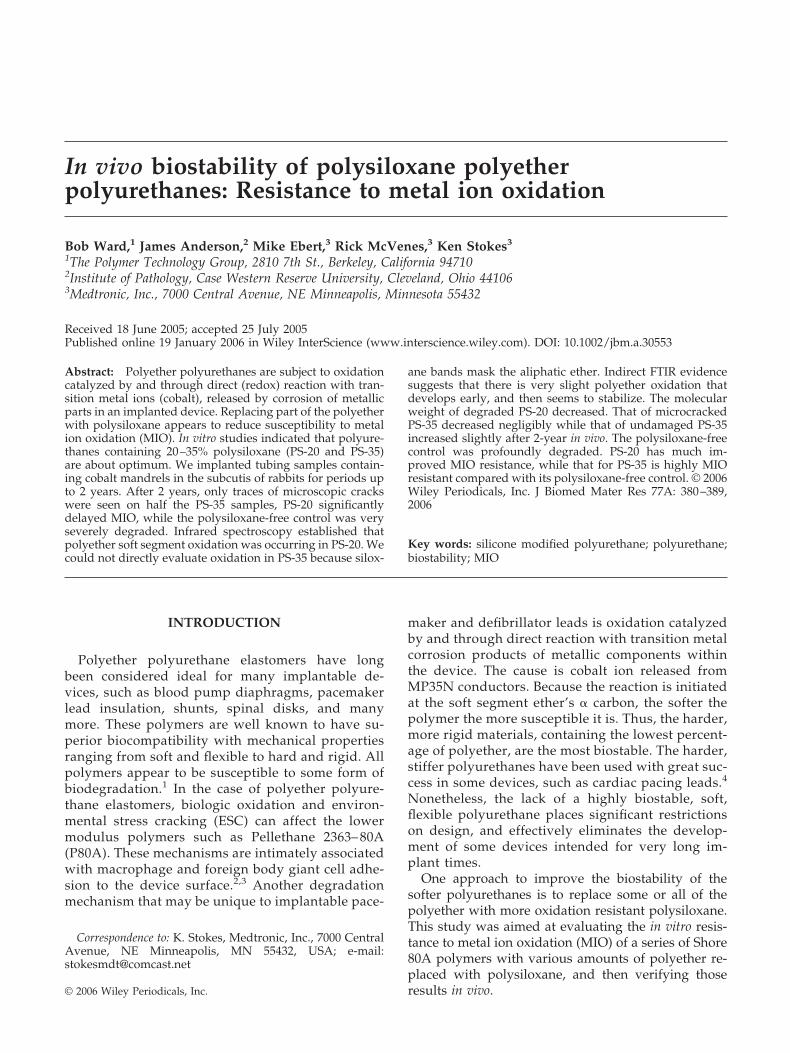
Tensile properties as a function of polysiloxane con-centration are shown in Figure 2. Increasing polysilox-ane concentration significantly decreases tensilestrength and increases elastic modulus. Elongationincreases slightly to 35% polysiloxane, and then de-creases. For example, PS-35 has 79% higher modulus,34% greater elongation, and 58% lower tensilestrength than unmodified P80A. PS-61 (with no poly-ether in the soft segment) has 200% higher modulus,78% lower tensile strength, and 17% lower elongationthan P80A.
In vitro screening study
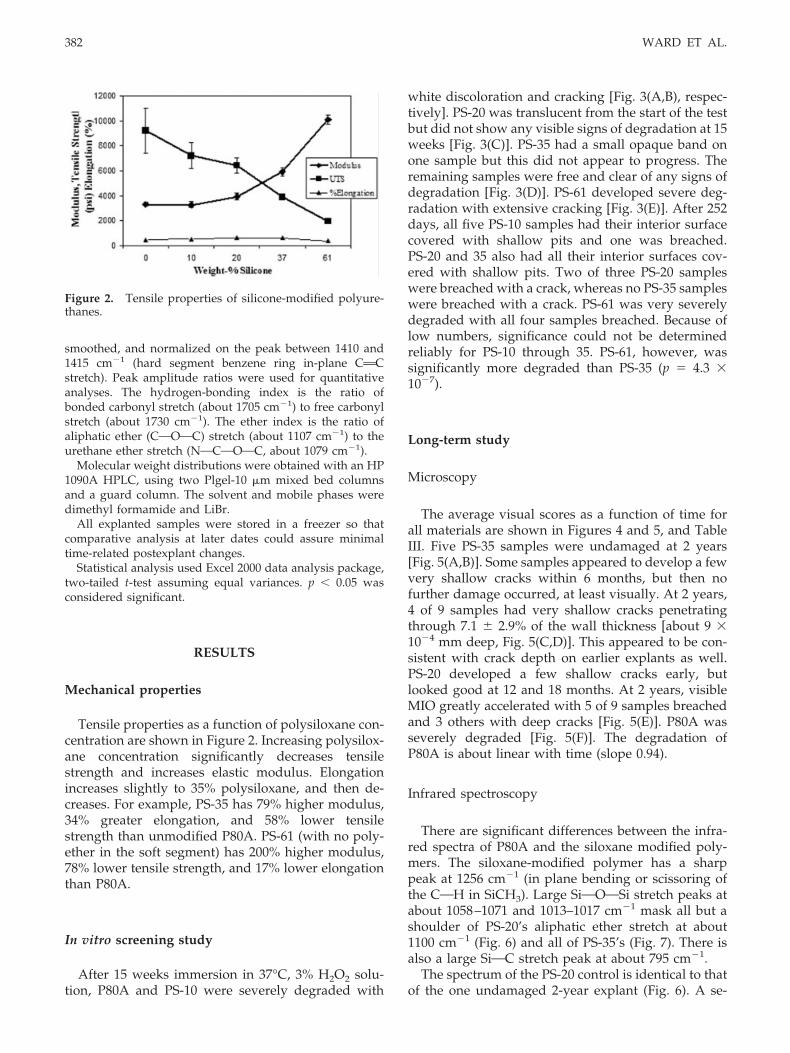
After 15 weeks immersion in 37°C, 3% H2O2 solu-tion, P80A and PS-10 were severely degraded with
white discoloration and cracking [Fig. 3(A,B), respec-tively]. PS-20 was translucent from the start of the testbut did not show any visible signs of degradation at 15weeks [Fig. 3(C)]. PS-35 had a small opaque band onone sample but this did not appear to progress. Theremaining samples were free and clear of any signs ofdegradation [Fig. 3(D)]. PS-61 developed severe deg-radation with extensive cracking [Fig. 3(E)]. After 252days, all five PS-10 samples had their interior surfacecovered with shallow pits and one was breached.PS-20 and 35 also had all their interior surfaces cov-ered with shallow pits. Two of three PS-20 sampleswere breached with a crack, whereas no PS-35 sampleswere breached with a crack. PS-61 was very severelydegraded with all four samples breached. Because oflow numbers, significance could not be determinedreliably for PS-10 through 35. PS-61, however, wassignificantly more degraded than PS-35 (p � 4.3 �10�7).
Long-term study
Microscopy
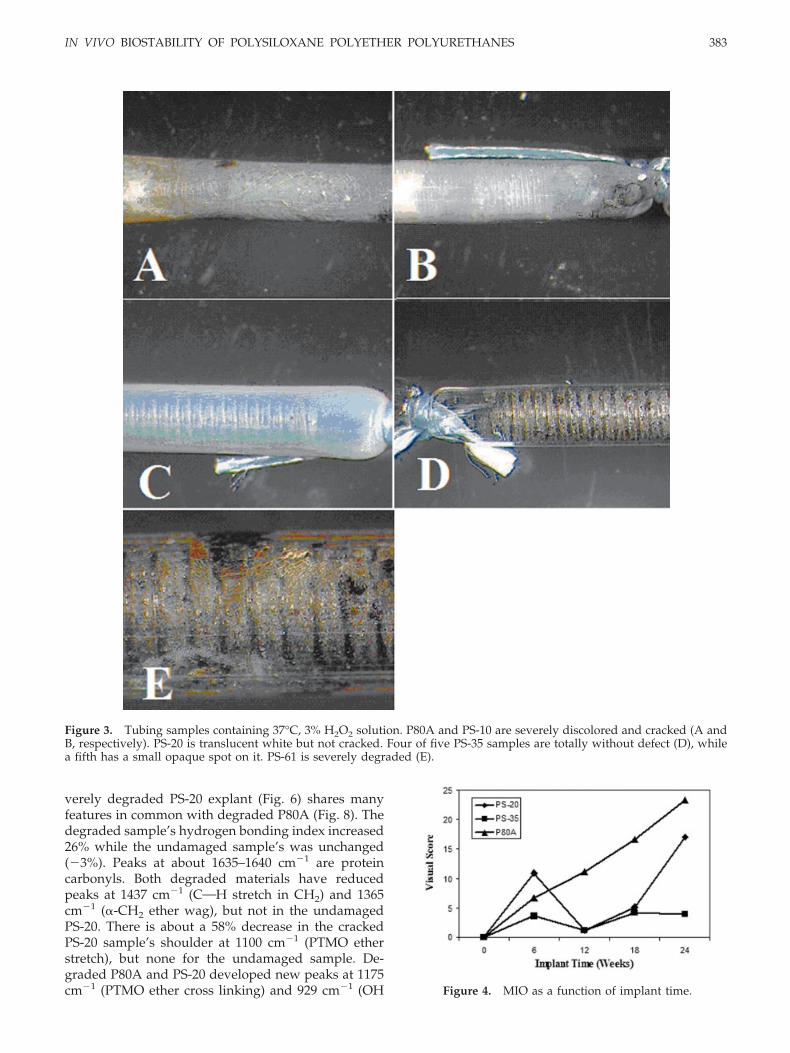
The average visual scores as a function of time forall materials are shown in Figures 4 and 5, and TableIII. Five PS-35 samples were undamaged at 2 years[Fig. 5(A,B)]. Some samples appeared to develop a fewvery shallow cracks within 6 months, but then nofurther damage occurred, at least visually. At 2 years,4 of 9 samples had very shallow cracks penetratingthrough 7.1 � 2.9% of the wall thickness [about 9 �10�4 mm deep, Fig. 5(C,D)]. This appeared to be con-sistent with crack depth on earlier explants as well.PS-20 developed a few shallow cracks early, butlooked good at 12 and 18 months. At 2 years, visibleMIO greatly accelerated with 5 of 9 samples breachedand 3 others with deep cracks [Fig. 5(E)]. P80A wasseverely degraded [Fig. 5(F)]. The degradation ofP80A is about linear with time (slope 0.94).
Infrared spectroscopy
There are significant differences between the infra-red spectra of P80A and the siloxane modified poly-mers. The siloxane-modified polymer has a sharppeak at 1256 cm�1 (in plane bending or scissoring ofthe COH in SiCH3). Large SiOOOSi stretch peaks atabout 1058–1071 and 1013–1017 cm�1 mask all but ashoulder of PS-20’s aliphatic ether stretch at about1100 cm�1 (Fig. 6) and all of PS-35’s (Fig. 7). There isalso a large SiOC stretch peak at about 795 cm�1.
The spectrum of the PS-20 control is identical to thatof the one undamaged 2-year explant (Fig. 6). A se-
Figure 2. Tensile properties of silicone-modified polyure-thanes.
382 WARD ET AL.
verely degraded PS-20 explant (Fig. 6) shares manyfeatures in common with degraded P80A (Fig. 8). Thedegraded sample’s hydrogen bonding index increased26% while the undamaged sample’s was unchanged(�3%). Peaks at about 1635–1640 cm�1 are proteincarbonyls. Both degraded materials have reducedpeaks at 1437 cm�1 (COH stretch in CH2) and 1365cm�1 (�-CH2 ether wag), but not in the undamagedPS-20. There is about a 58% decrease in the crackedPS-20 sample’s shoulder at 1100 cm�1 (PTMO etherstretch), but none for the undamaged sample. De-graded P80A and PS-20 developed new peaks at 1175cm�1 (PTMO ether cross linking) and 929 cm�1 (OH
Figure 3. Tubing samples containing 37°C, 3% H2O2 solution. P80A and PS-10 are severely discolored and cracked (A andB, respectively). PS-20 is translucent white but not cracked. Four of five PS-35 samples are totally without defect (D), whilea fifth has a small opaque spot on it. PS-61 is severely degraded (E).
Figure 4. MIO as a function of implant time.
IN VIVO BIOSTABILITY OF POLYSILOXANE POLYETHER POLYURETHANES 383
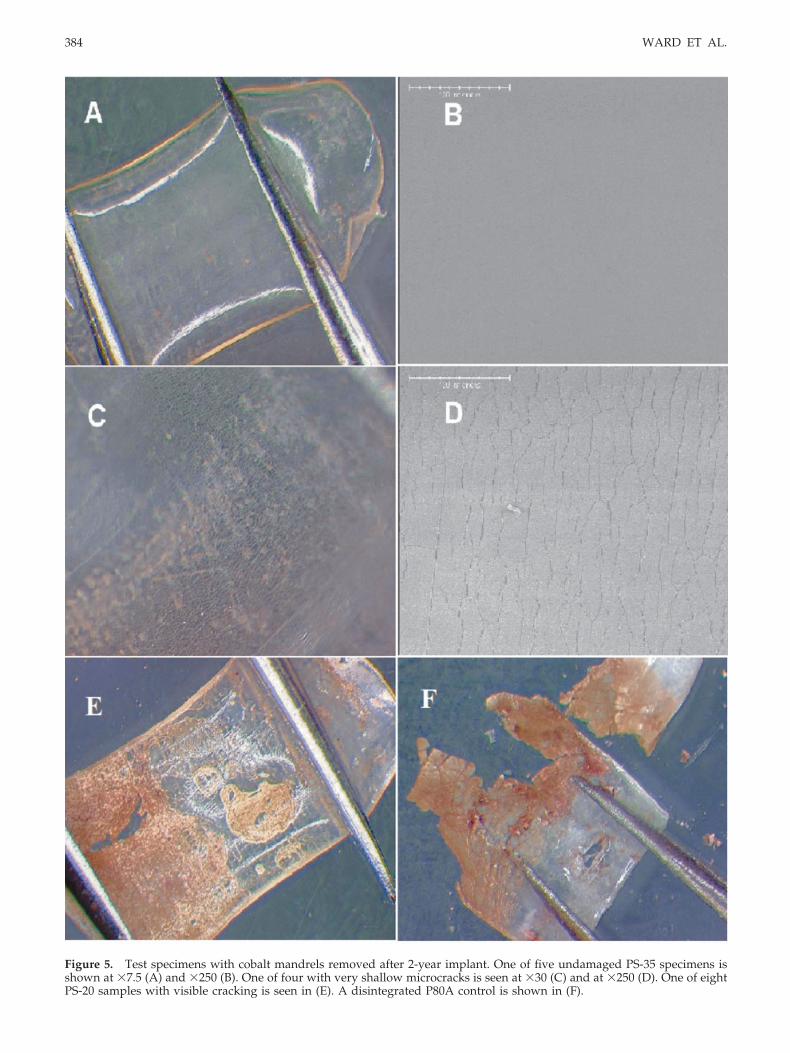
Figure 5. Test specimens with cobalt mandrels removed after 2-year implant. One of five undamaged PS-35 specimens isshown at �7.5 (A) and �250 (B). One of four with very shallow microcracks is seen at �30 (C) and at �250 (D). One of eightPS-20 samples with visible cracking is seen in (E). A disintegrated P80A control is shown in (F).
384 WARD ET AL.
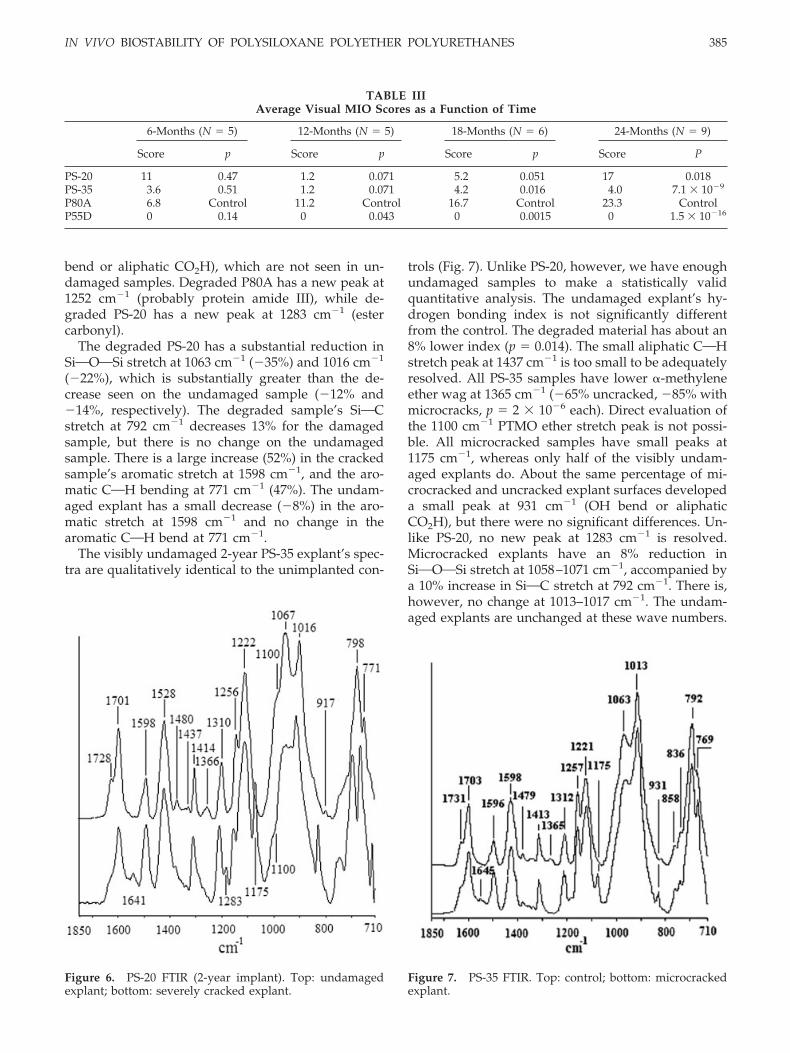
bend or aliphatic CO2H), which are not seen in un-damaged samples. Degraded P80A has a new peak at1252 cm�1 (probably protein amide III), while de-graded PS-20 has a new peak at 1283 cm�1 (estercarbonyl).
The degraded PS-20 has a substantial reduction inSiOOOSi stretch at 1063 cm�1 (�35%) and 1016 cm�1
(�22%), which is substantially greater than the de-crease seen on the undamaged sample (�12% and�14%, respectively). The degraded sample’s SiOCstretch at 792 cm�1 decreases 13% for the damagedsample, but there is no change on the undamagedsample. There is a large increase (52%) in the crackedsample’s aromatic stretch at 1598 cm�1, and the aro-matic COH bending at 771 cm�1 (47%). The undam-aged explant has a small decrease (�8%) in the aro-matic stretch at 1598 cm�1 and no change in thearomatic COH bend at 771 cm�1.
The visibly undamaged 2-year PS-35 explant’s spec-tra are qualitatively identical to the unimplanted con-
trols (Fig. 7). Unlike PS-20, however, we have enoughundamaged samples to make a statistically validquantitative analysis. The undamaged explant’s hy-drogen bonding index is not significantly differentfrom the control. The degraded material has about an8% lower index (p � 0.014). The small aliphatic COHstretch peak at 1437 cm�1 is too small to be adequatelyresolved. All PS-35 samples have lower �-methyleneether wag at 1365 cm�1 (�65% uncracked, �85% withmicrocracks, p � 2 � 10�6 each). Direct evaluation ofthe 1100 cm�1 PTMO ether stretch peak is not possi-ble. All microcracked samples have small peaks at1175 cm�1, whereas only half of the visibly undam-aged explants do. About the same percentage of mi-crocracked and uncracked explant surfaces developeda small peak at 931 cm�1 (OH bend or aliphaticCO2H), but there were no significant differences. Un-like PS-20, no new peak at 1283 cm�1 is resolved.Microcracked explants have an 8% reduction inSiOOOSi stretch at 1058–1071 cm�1, accompanied bya 10% increase in SiOC stretch at 792 cm�1. There is,however, no change at 1013–1017 cm�1. The undam-aged explants are unchanged at these wave numbers.
TABLE IIIAverage Visual MIO Scores as a Function of Time
6-Months (N � 5) 12-Months (N � 5) 18-Months (N � 6) 24-Months (N � 9)
Score p Score p Score p Score P
PS-20 11 0.47 1.2 0.071 5.2 0.051 17 0.018PS-35 3.6 0.51 1.2 0.071 4.2 0.016 4.0 7.1 � 10�9
P80A 6.8 Control 11.2 Control 16.7 Control 23.3 ControlP55D 0 0.14 0 0.043 0 0.0015 0 1.5 � 10�16
Figure 6. PS-20 FTIR (2-year implant). Top: undamagedexplant; bottom: severely cracked explant.
Figure 7. PS-35 FTIR. Top: control; bottom: microcrackedexplant.
IN VIVO BIOSTABILITY OF POLYSILOXANE POLYETHER POLYURETHANES 385
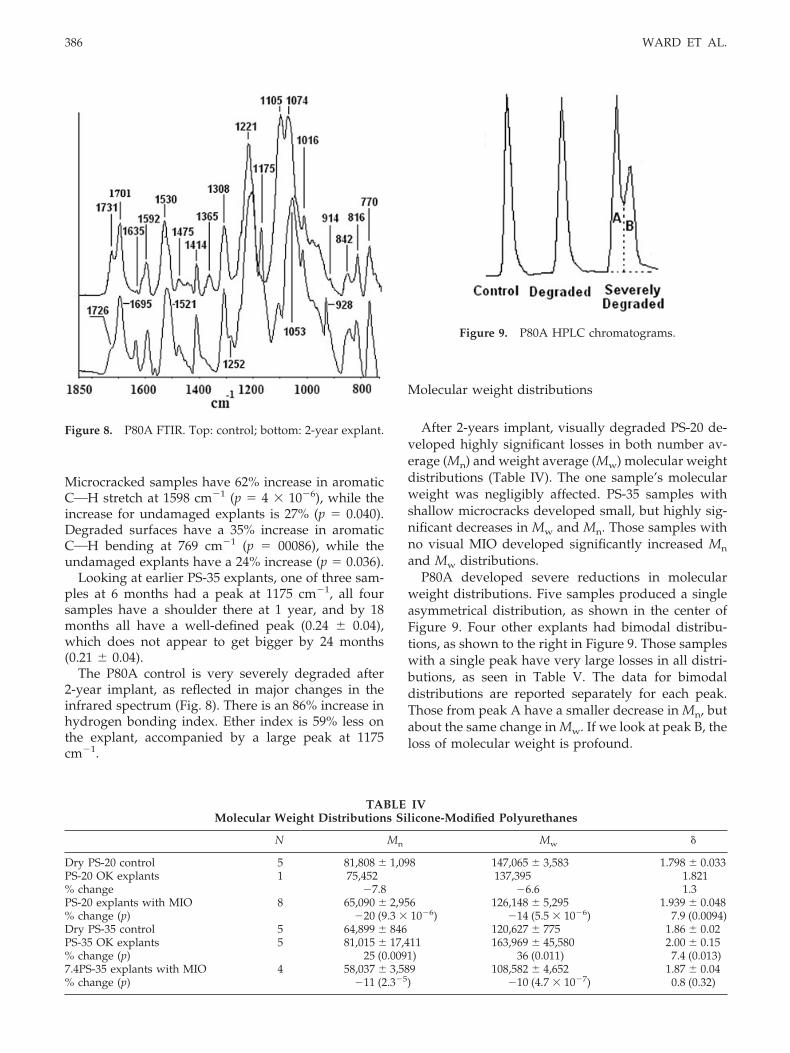
Microcracked samples have 62% increase in aromaticCOH stretch at 1598 cm�1 (p � 4 � 10�6), while theincrease for undamaged explants is 27% (p � 0.040).Degraded surfaces have a 35% increase in aromaticCOH bending at 769 cm�1 (p � 00086), while theundamaged explants have a 24% increase (p � 0.036).
Looking at earlier PS-35 explants, one of three sam-ples at 6 months had a peak at 1175 cm�1, all foursamples have a shoulder there at 1 year, and by 18months all have a well-defined peak (0.24 � 0.04),which does not appear to get bigger by 24 months(0.21 � 0.04).
The P80A control is very severely degraded after2-year implant, as reflected in major changes in theinfrared spectrum (Fig. 8). There is an 86% increase inhydrogen bonding index. Ether index is 59% less onthe explant, accompanied by a large peak at 1175cm�1.
Molecular weight distributions
After 2-years implant, visually degraded PS-20 de-veloped highly significant losses in both number av-erage (Mn) and weight average (Mw) molecular weightdistributions (Table IV). The one sample’s molecularweight was negligibly affected. PS-35 samples withshallow microcracks developed small, but highly sig-nificant decreases in Mw and Mn. Those samples withno visual MIO developed significantly increased Mn
and Mw distributions.P80A developed severe reductions in molecular
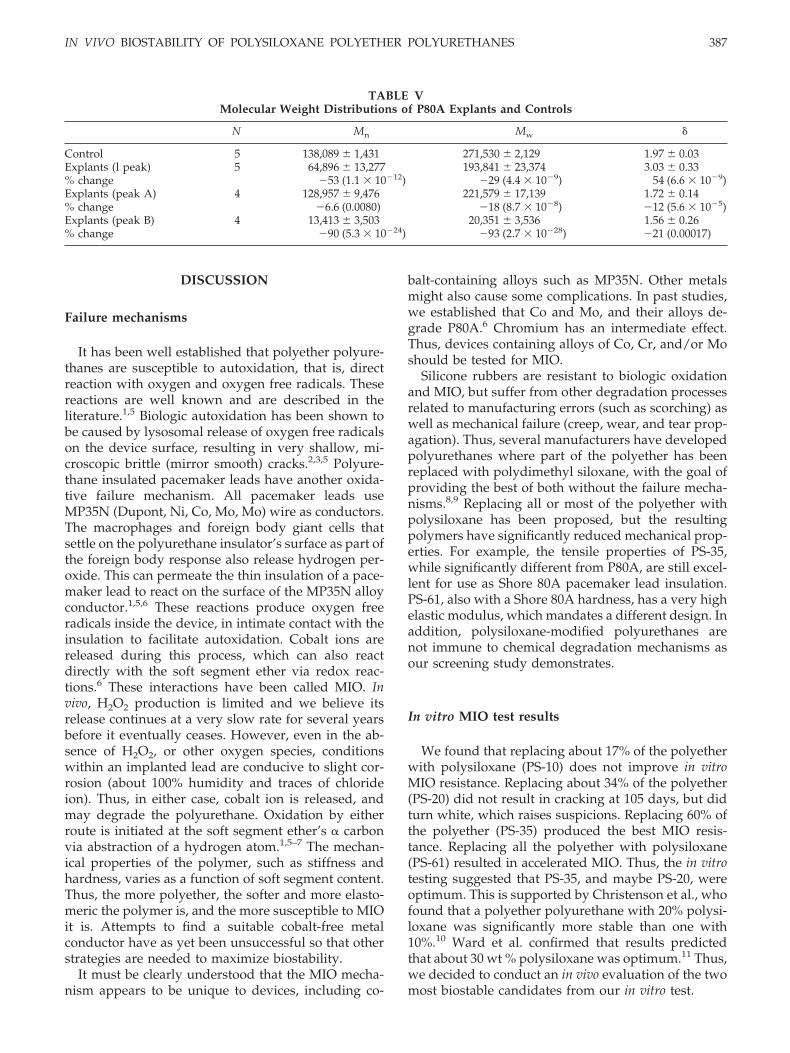
weight distributions. Five samples produced a singleasymmetrical distribution, as shown in the center ofFigure 9. Four other explants had bimodal distribu-tions, as shown to the right in Figure 9. Those sampleswith a single peak have very large losses in all distri-butions, as seen in Table V. The data for bimodaldistributions are reported separately for each peak.Those from peak A have a smaller decrease in Mn, butabout the same change in Mw. If we look at peak B, theloss of molecular weight is profound.
Figure 8. P80A FTIR. Top: control; bottom: 2-year explant.
TABLE IVMolecular Weight Distributions Silicone-Modified Polyurethanes
N Mn Mw
Dry PS-20 control 5 81,808 � 1,098 147,065 � 3,583 1.798 � 0.033PS-20 OK explants 1 75,452 137,395 1.821% change �7.8 �6.6 1.3PS-20 explants with MIO 8 65,090 � 2,956 126,148 � 5,295 1.939 � 0.048% change (p) �20 (9.3 � 10�6) �14 (5.5 � 10�6) 7.9 (0.0094)Dry PS-35 control 5 64,899 � 846 120,627 � 775 1.86 � 0.02PS-35 OK explants 5 81,015 � 17,411 163,969 � 45,580 2.00 � 0.15% change (p) 25 (0.0091) 36 (0.011) 7.4 (0.013)7.4PS-35 explants with MIO 4 58,037 � 3,589 108,582 � 4,652 1.87 � 0.04% change (p) �11 (2.3�5) �10 (4.7 � 10�7) 0.8 (0.32)
Figure 9. P80A HPLC chromatograms.
386 WARD ET AL.
DISCUSSION
Failure mechanisms
It has been well established that polyether polyure-thanes are susceptible to autoxidation, that is, directreaction with oxygen and oxygen free radicals. Thesereactions are well known and are described in theliterature.1,5 Biologic autoxidation has been shown tobe caused by lysosomal release of oxygen free radicalson the device surface, resulting in very shallow, mi-croscopic brittle (mirror smooth) cracks.2,3,5 Polyure-thane insulated pacemaker leads have another oxida-tive failure mechanism. All pacemaker leads useMP35N (Dupont, Ni, Co, Mo, Mo) wire as conductors.The macrophages and foreign body giant cells thatsettle on the polyurethane insulator’s surface as part ofthe foreign body response also release hydrogen per-oxide. This can permeate the thin insulation of a pace-maker lead to react on the surface of the MP35N alloyconductor.1,5,6 These reactions produce oxygen freeradicals inside the device, in intimate contact with theinsulation to facilitate autoxidation. Cobalt ions arereleased during this process, which can also reactdirectly with the soft segment ether via redox reac-tions.6 These interactions have been called MIO. Invivo, H2O2 production is limited and we believe itsrelease continues at a very slow rate for several yearsbefore it eventually ceases. However, even in the ab-sence of H2O2, or other oxygen species, conditionswithin an implanted lead are conducive to slight cor-rosion (about 100% humidity and traces of chlorideion). Thus, in either case, cobalt ion is released, andmay degrade the polyurethane. Oxidation by eitherroute is initiated at the soft segment ether’s � carbonvia abstraction of a hydrogen atom.1,5–7 The mechan-ical properties of the polymer, such as stiffness andhardness, varies as a function of soft segment content.Thus, the more polyether, the softer and more elasto-meric the polymer is, and the more susceptible to MIOit is. Attempts to find a suitable cobalt-free metalconductor have as yet been unsuccessful so that otherstrategies are needed to maximize biostability.
It must be clearly understood that the MIO mecha-nism appears to be unique to devices, including co-
balt-containing alloys such as MP35N. Other metalsmight also cause some complications. In past studies,we established that Co and Mo, and their alloys de-grade P80A.6 Chromium has an intermediate effect.Thus, devices containing alloys of Co, Cr, and/or Moshould be tested for MIO.
Silicone rubbers are resistant to biologic oxidationand MIO, but suffer from other degradation processesrelated to manufacturing errors (such as scorching) aswell as mechanical failure (creep, wear, and tear prop-agation). Thus, several manufacturers have developedpolyurethanes where part of the polyether has beenreplaced with polydimethyl siloxane, with the goal ofproviding the best of both without the failure mecha-nisms.8,9 Replacing all or most of the polyether withpolysiloxane has been proposed, but the resultingpolymers have significantly reduced mechanical prop-erties. For example, the tensile properties of PS-35,while significantly different from P80A, are still excel-lent for use as Shore 80A pacemaker lead insulation.PS-61, also with a Shore 80A hardness, has a very highelastic modulus, which mandates a different design. Inaddition, polysiloxane-modified polyurethanes arenot immune to chemical degradation mechanisms asour screening study demonstrates.
In vitro MIO test results
We found that replacing about 17% of the polyetherwith polysiloxane (PS-10) does not improve in vitroMIO resistance. Replacing about 34% of the polyether(PS-20) did not result in cracking at 105 days, but didturn white, which raises suspicions. Replacing 60% ofthe polyether (PS-35) produced the best MIO resis-tance. Replacing all the polyether with polysiloxane(PS-61) resulted in accelerated MIO. Thus, the in vitrotesting suggested that PS-35, and maybe PS-20, wereoptimum. This is supported by Christenson et al., whofound that a polyether polyurethane with 20% polysi-loxane was significantly more stable than one with10%.10 Ward et al. confirmed that results predictedthat about 30 wt % polysiloxane was optimum.11 Thus,we decided to conduct an in vivo evaluation of the twomost biostable candidates from our in vitro test.
TABLE VMolecular Weight Distributions of P80A Explants and Controls
N Mn Mw
Control 5 138,089 � 1,431 271,530 � 2,129 1.97 � 0.03Explants (l peak) 5 64,896 � 13,277 193,841 � 23,374 3.03 � 0.33% change �53 (1.1 � 10�12) �29 (4.4 � 10�9) 54 (6.6 � 10�9)Explants (peak A) 4 128,957 � 9,476 221,579 � 17,139 1.72 � 0.14% change �6.6 (0.0080) �18 (8.7 � 10�8) �12 (5.6 � 10�5)Explants (peak B) 4 13,413 � 3,503 20,351 � 3,536 1.56 � 0.26% change �90 (5.3 � 10�24) �93 (2.7 � 10�28) �21 (0.00017)
IN VIVO BIOSTABILITY OF POLYSILOXANE POLYETHER POLYURETHANES 387

In vivo test results
Visual analysis
After 2-year implant, it is clear that while PS-20 maydelay significant MIO, it eventually succumbs within18–24 months in this severe test. In comparison, PS-35had spectacular performance visually, far exceedingthat of its polysiloxane-free control, P80A. In fact,P80A had very poor MIO performance. Thus, the pre-dictions resulting from Ward et al. and our in vitrotesting were confirmed—PS-35 is about optimum forvisual MIO resistance in this series of Shore 80A poly-mers.
Ftir analysis
It is clear that degradation of PS-20 occurs in thepolyether soft segment. Increased hydrogen bondingindices are typically seen in explanted polyurethaneelastomers. This could be the result of increased mo-lecular mobility because of polyether soft segmentchain scission. It could also be due to residual stressrelaxation as suggested by decreases in the �-ethermethylene wag at about 1365 cm�1.12 Note that thedecrease in amplitude at 1365 cm�1 could also be dueto loss of polyether. The large increase in aromaticfunctionality on/near the surface is indicative of mor-phological changes, which could also explain thechanges in hydrogen bonding indices and loss of�-methylene ether wag at the surface. Thus, thesechanges per se are circumstantial evidence, but notnecessarily indicative of the degradation mechanism.The large decrease in the PS-20 PTMO ether shoulderat 1100 cm�1, however, is indicative of oxidation. Thisis confirmed by the appearance of peaks at 1175 cm�1,which are attributed to soft segment cross-linking ofdegradation products. The development of a peak at929 cm�1 (OH) is consistent with this since polymerhydroperoxide is a well-known part of the oxidationprocess. The decrease in SiOOOSi and SiOC stretchpeak amplitudes is suggestive of some degradation inthe polysiloxane soft segment as well. We postulatethat the oxidizing cobalt ion may be causing cross-linking or branching, in a manner similar to thatcaused by peroxide catalysts. It is interesting that thesingle PS-20 sample that survived 2-year implant withno visual MIO had no indications of degradation at allby FTIR.
The situation with PS-35 has substantial similaritiesto PS-20, and substantial differences. Remember thatPS-20 underwent severe bulk degradation, whilePS-35 had very shallow microcracking on the surfacesof some samples. FTIR only penetrates 1–2 �m into thesurface so that it tells us what is present in the material
with shallow cracks and not the bulk. Thus, regardlessof the FTIR, the PS-35 MIO resistance is far superior toPS-20 in this test. The major difference from PS-20 isthat PS-35 did not reveal any changes in the siliconesoft segment. Degradation, to the extent that it occurs,appears to be limited to the polyether soft segment.That said, degradation of PS-35 appears to occur early,then stabilize, being of no concern for devices such aspacemaker leads.
Molecular weight
Degraded samples of PS-20 do show significant de-creases in molecular weight distributions, while thatfor the undegraded sample is within the instrumentalerror. Degraded PS-35 explants also develop slightlyreduced Mn, but the decrease is about half that seen inPS-20. Mw decrease is similar to PS-20. Those samplesthat had no visible MIO actually had significantlyincreased molecular weight. This would support ahypothesis that there are competing mechanisms oc-curring, polyether chain scission and polydimethylsiloxane branching/cross linking.
Test methods
One must always question the validity of in vitrotests, since it is not possible to duplicate the in vivoenvironment. Based on these results, it appears thatthe in vitro test does predict in vivo performance. Inpast attempts to validate the in vitro results, we tried tomimic what happens in a pacemaker lead.7 That is,there was no hole in the specimen and fluid had toenter the specimen by diffusion. We found thatMP35N produced no visible MIO in 2 years. The co-balt mandrels had a slight visible effect at 2 years onsome of the specimens. We do know that the oxidationpotential of Co2 is too low to oxidize the polyether,and Co3 is too high, oxidizing water before it canpermeate the insulation. Cobalt complexes, however,can be potent oxidizers without interference from theenvironment.5 Thus, in this test we added a hole in thepolyurethane to allow ingress of exudate, transudate,and possibly even a few cells. The result is substan-tially accelerated MIO on the polymers susceptible toMIO, as compared with the actual device perfor-mance. Can we use these results to predict devicelongevity? The actuarial survival rates of implantedleads vary widely with design and materials.4 Forexample, the harder, stiffer Pellethane 2363–55D(P55D) is much more MIO resistant than P80A. If usedin too thin a wall thickness, however, P55D can de-grade relatively quickly. MP35N is more resistant toproducing MIO than composites with silver that cor-
388 WARD ET AL.

rode much more readily.5,6 Thus, while we can saythat PS-35 will make an excellent insulator for long-term implants, we cannot say that PS-20 is acceptableor not acceptable on the basis of this test alone. Can weestablish an acceleration factor for either the in vitro orin vivo test? At this point, the answer is no, for thesame reasons cited earlier. In addition, the kinetics ofthe in vitro reaction are quite different from those of invivo, and there is substantial biologic variation. Thus,this test tells us that the MIO resistance of PS-35 ��PS-20 �� P80A. It also tells us that PS-35 is clearlyacceptable for use in long-term implants as far as MIOis concerned.
Why run the in vivo test for 2 years? This was aninitial experiment to establish test parameters and, ifnecessary, to examine degradation rates. We ran thetest long enough to detect significant differences,which is clearly the case by 2 years, but not at 18months.
We have learned that long-term testing with inter-mediate explants requires special care. Over a 2-yearperiod, new instruments may be obtained, softwareand technicians may change and results from analysesdone years apart may not be compatible. Thus, westore the intermediate specimens in a freezer to slowor stop any continuing degradation, then do the anal-yses all at once. In this case, we had such a significantdifference at 2 years that we felt it was sufficient forthe purposes of the experiment. The samples are stillin the freezer in case we do decide to do more analy-ses. In future experiments, it is likely that we willreduce the explant intervals and increase N per interval.
CONCLUSIONS
Polyether polyurethanes are susceptible to oxida-tive degradation through reaction with cobalt ion(MIO). PS-35 is a spectacular improvement in MIOresistance compared with its polysiloxane-free control(the industry standard), P80A. Its use in implantabledevices such as cardiac pacing leads is clearly a majorimprovement over P80A or other silicone-modifiedpolyurethanes. PS-20 delays MIO significantly, but isnot a resistant as PS-35. The MIO resistance of polysi-loxane polyether polyurethanes is PS-35 � PS-20 ��PS-10 � P80A �� PS-61. Thus, PS-35 appears to haveoptimum MIO resistance. If these results can be ex-trapolated, it is probable that polyurethanes similar toPS-35, but with stoichiometry to minimize the poly-ether content even further (as in a Shore 90A or 55Dhardness) would provide even greater MIO resistance
over very long implant times. Of course, MIO is not anissue for any of the materials tested here in devicesthat do not include Co, Cr, and/or Mo alloys, or usebenign metals such as Pt, Ni, Ti, Ag, and Fe, and theiralloys. Any polyurethane devices that do contain Co,Cr, and/or Mo alloys should be evaluated for MIO.
Thanks to the following people at PTG and Medtronic,who’s work made this study possible: Yuan Tian for poly-mer synthesis, Rich Molacek for his extrusion expertise, JohnUrban and Kent Wika for making the specimens and coor-dinating implant/explant, Sue Okerstrom for SEM, SteveSkorich for FTIR, and Sally Anzelc and Kevin Hansen formolecular weight distributions.
References
1. Stokes K. Biodegradation. Cardiovasc Pathol 1993;2 (Suppl3):111S–119S.
2. Zhao Q, Agger MP, Fitzpatrick M, Anderson JM, Stokes K,Urbanski P. In vivo studies of stress-cracking in polyetherure-thanes using the cage implant system. In: Transactions of the15th Annual Meeting of the Society for Biomaterials, LakeBuena Vista, FL, 1989. p 203.
3. Zhao Q, Agger MP, Fitzpatrick M, Anderson JM, Stokes K,Urbanski P. Cellular interactions with biomaterials: In vivocracking of stressed polyetherurethanes. J Biomed Mater Res1990;24:621–637.
4. Medtronic. CRM Product Performance Report, 2004, 1st ed.Minneapolis, MN: Medtronic; 2004.
5. Stokes K, Coury A, Urbanski, P. Autooxidative degradation ofimplanted polyether polyurethane devices. J Biomater Appl1987;1:411–448.
6. Stokes K, Urbanski P, Coury A. In vivo autooxidation of poly-ether polyurethanes in the presence of metals: Preliminaryresults. In: Transactions of the 13th Annual Meeting of theSociety for Biomaterials, New York, 1987. p 10.
7. Schubert MA, Wiggins MJ, Defife KM, Hiltner A, AndersonJM. Vitamin E as an antioxidant for poly(etherurethane urea):In vivo studies. J Biomed Mater Res 1996;32:493–504.
8. Ward RS. Thermoplastic silicone-urethane copolymers: A newclass of biomedical elastomers. Med Device Diagn Ind 2000;22(4):68–77.
9. Hyvarinen A, Odell RA, Martin DJ, Gunatillake PA, Nobel KR,Pool-Warren LA. Long-term in vivo biostability of poly(dim-ethylsiloxane)/poly(hexamethylene oxide) mixed macrodiol-based polyurethane elastomers. Biomaterials 2004;20:4887–4900.
10. Christenson EM, Dadestan M, Wiggins MJ, Ebert M, Ward R,Hiltner A, Anderson JM. The effect of silicone on the biosta-bility of poly(ether urethane). In: Transactions of the 28thAnnual Meeting of the Society for Biomaterials, 2002. p 111.
11. Ward R, Tian Y, McCrea K, Christenson C, Anderson J, EbertM, Stokes K. Optimizing silicone content in thermoplastic sil-icone-urethanes used in chronically-implanted medical de-vices. In: Transactions of the 30th Annual Meeting of theSociety for Biomaterials, 2005. p 160.
12. Schubert MA, Wiggens MJ, Anderson JM, Hiltner A. The effectof strain state on the biostability of a poly(etherurethane urea)elastomers. J Biomed Mater Res 1997;35:319–328.
IN VIVO BIOSTABILITY OF POLYSILOXANE POLYETHER POLYURETHANES 389


















