
In vitro drug resistance in acute myeloid and chronic B-lymphocytic leukaemic blasts and in normal...
9
~Pergamon 0145-2126(94)00081-6 Leukemia Research Vol. 18, No. 9, pp. 683~91, 1994 Copyright © 1994Elsevier Science Ltd Printedin Great Britain. All rightsreserved 0145-2126/94 $7.00 + 0.00 IN VITRO DRUG RESISTANCE IN ACUTE MYELOID AND CHRONIC B-LYMPHOCYTIC LEUKAEMIC BLASTS AND IN NORMAL BLOOD AND MARROW POPULATIONS PAUL BAINES,* MEDHA LIMAYE,{ TERRY HOY,~ ROSE ANN PADUA,+ JACK WHITTAKER,+ ALA AL-SABAH'~ and ALAN BURNETT~" *Department of Haematology, University Hospital of Wales; and +University of Wales College of Medicine, Heath Park, Cardiff, U.K. (Received 7 February 1994. Revision accepted 23 May 1994) Abstract--The sensitivities of AML and BCLL blasts to daunorubicin have been determined, using an in vitro (MTT) assay of resistance, and compared with the sensitivities of normal haemopoietic populations and cells of the multidrug-resistant, T-lymphoid line CEM VLB10o. The role of the drug-efflux pump, P-glycoprotein, was determined by adding the 'modifier' cyclosporin and by measuring numbers of P-glycoprotein positive cells by immunofluo- rescence. IDh0S for 17 cases of de novo AML varied from 5 to 300 ng/ml giving a median of 105 ng/ml which was similar to the median of 11 normal marrow mononuclear cell preparations (80 ng/ml) but considerably less than the median It)so of eight blood lymphocyte samples (3500 ng/ml), it)s0Sfor five relapsed and two refractory AML samples ranged from 27 to 240 ng/ ml, well within the de novo range: we had obtained presentation samples for two of these and, in both cases, IDh0S were lower at relapse. IDh0S, however, were raised in seven marrow mononuclear cell populations taken soon after remission induction (It)50 for remission MNC and normal MNC = 200 and 80 ng/ml, respectively); this may reflect either a property of regenerating populations, or an activation of cellular resistance mechanisms following chemo- therapy, it)s0S for 17 cases of BCLL ranged from 7 to 200 ng/ml with a median of 48 ng/ml which was significantly lower than the IDs0 of AML blasts or of blood lymphocytes. Cyclosporin induced less than two-fold reductions in It)s0S of blood lymphocytes, marrow mononuclear cells and de novo AML and BCLL blasts despite giving log reversals in resistance in the CEM VLB100 line. This reflected numbers of P-glycoprotein positive cells in our samples, which were high in CEM VLBt00 but low in fresh normal or leukaemic cell suspensions. For both de novo AML and BCLL groups, however, the change in MD50, on addition of cyclosporin, was significant. These data imply a minor role for P-glycoprotein in drug resistance of leukaemic blasts. Nevertheless, there was a positive correlation between daunorubicin it)s0s in de novo AML and time to remission which confirms that in vitro chemosensitivity assays can provide a useful measure of in vivo resistance. Key words: P-glycoprotein, multidrug resistance, AML, BCLL, cyclosporin, in vitro chemo- sensitivity, M'IT. Introduction How LEUKAEMIC BLASTS evade cytotoxic chemo- therapy remains poorly understood. It is often dif- ficult to assign resistance to pharmacological or cellular mechanisms, although in vitro assays for drug sensitivity should aid this distinction. At the cellular Abbreviations: [Dh0,drug dose giving 50% inhibition of MTT absorbance ; M D R, multidrug resistance; Pgp (p170), P-glycoprotein; MTT, 3,(4,5-dimethylthiazol-2-yl)2,5- diphenyltetrazolium bromide. Correspondence to: Paul Baines, Department of Hae- matology, University Hospital of Wales, Heath Park, Car- diff, CF4 4XW, U.K. 683 level, many questions remain unanswered. Which mechanisms do cells use to survive cytotoxic drugs and are these enhanced in response to chemotherapy? Are leukaemic blasts from refractory disease or from relapsed patients really less sensitive? How many mechanisms might be involved in the acquisition of cross-resistance to several dissimilar drugs (multidrug resistance)? The detection of elevated mRNA transcripts for the MDR-I P-glycoprotein drug efflux pump across bulk leukaemic populations [1-5] suggests that reduced sensitivity may be expressed by leukaemic populations as a whole, and is not necessarily restric-
-
Upload
paul-baines -
Category
Documents
-
view
213 -
download
0
Transcript of In vitro drug resistance in acute myeloid and chronic B-lymphocytic leukaemic blasts and in normal...

~ P e r g a m o n
0145-2126(94)00081-6
Leukemia Research Vol. 18, No. 9, pp. 683~91, 1994 Copyright © 1994 Elsevier Science Ltd
Printed in Great Britain. All rights reserved 0145-2126/94 $7.00 + 0.00
IN VITRO DRUG RESISTANCE IN ACUTE MYELOID AND CHRONIC B-LYMPHOCYTIC LEUKAEMIC BLASTS AND IN NORMAL BLOOD
AND MARROW POPULATIONS
PAUL BAINES,* MEDHA LIMAYE,{ TERRY HOY,~ ROSE ANN PADUA,+ JACK WHITTAKER,+ ALA AL-SABAH'~ a n d ALAN BURNETT~"
*Department of Haematology, University Hospital of Wales; and +University of Wales College of Medicine, Heath Park, Cardiff, U.K.
(Received 7 February 1994. Revision accepted 23 May 1994)
Abstract--The sensitivities of AML and BCLL blasts to daunorubicin have been determined, using an in vitro (MTT) assay of resistance, and compared with the sensitivities of normal haemopoietic populations and cells of the multidrug-resistant, T-lymphoid line CEM VLB10o. The role of the drug-efflux pump, P-glycoprotein, was determined by adding the 'modifier' cyclosporin and by measuring numbers of P-glycoprotein positive cells by immunofluo- rescence. IDh0S for 17 cases of de novo AML varied from 5 to 300 ng/ml giving a median of 105 ng/ml which was similar to the median of 11 normal marrow mononuclear cell preparations (80 ng/ml) but considerably less than the median It)so of eight blood lymphocyte samples (3500 ng/ml), it)s0S for five relapsed and two refractory AML samples ranged from 27 to 240 ng/ ml, well within the de novo range: we had obtained presentation samples for two of these and, in both cases, IDh0S were lower at relapse. IDh0S, however, were raised in seven marrow mononuclear cell populations taken soon after remission induction (It)50 for remission MNC and normal MNC = 200 and 80 ng/ml, respectively); this may reflect either a property of regenerating populations, or an activation of cellular resistance mechanisms following chemo- therapy, it)s0S for 17 cases of BCLL ranged from 7 to 200 ng/ml with a median of 48 ng/ml which was significantly lower than the IDs0 of AML blasts or of blood lymphocytes. Cyclosporin induced less than two-fold reductions in It)s0S of blood lymphocytes, marrow mononuclear cells and de novo AML and BCLL blasts despite giving log reversals in resistance in the CEM VLB100 line. This reflected numbers of P-glycoprotein positive cells in our samples, which were high in CEM VLBt00 but low in fresh normal or leukaemic cell suspensions. For both de novo AML and BCLL groups, however, the change in MD50, on addition of cyclosporin, was significant. These data imply a minor role for P-glycoprotein in drug resistance of leukaemic blasts. Nevertheless, there was a positive correlation between daunorubicin it)s0s in de novo AML and time to remission which confirms that in vitro chemosensitivity assays can provide a useful measure of in vivo resistance.
Key words: P-glycoprotein, multidrug resistance, AML, BCLL, cyclosporin, in vitro chemo- sensitivity, M'IT.
Introduction
How LEUKAEMIC BLASTS evade cytotoxic chemo- therapy remains poorly understood. It is often dif- ficult to assign resistance to pharmacological or cellular mechanisms, although in vitro assays for drug sensitivity should aid this distinction. At the cellular
Abbreviations: [Dh0, drug dose giving 50% inhibition of MTT absorbance ; M D R, multidrug resistance; Pgp (p170), P-glycoprotein; MTT, 3,(4,5-dimethylthiazol-2-yl)2,5- diphenyltetrazolium bromide.
Correspondence to: Paul Baines, Department of Hae- matology, University Hospital of Wales, Heath Park, Car- diff, CF4 4XW, U.K.
683
level, many questions remain unanswered. Which mechanisms do cells use to survive cytotoxic drugs and are these enhanced in response to chemotherapy? Are leukaemic blasts from refractory disease or from relapsed patients really less sensitive? How many mechanisms might be involved in the acquisition of cross-resistance to several dissimilar drugs (multidrug resistance)?
The detection of elevated mRNA transcripts for the MDR-I P-glycoprotein drug efflux pump across bulk leukaemic populations [1-5] suggests that reduced sensitivity may be expressed by leukaemic populations as a whole, and is not necessarily restric-

684 P. BAINES et al.
ted to minor populations of cells with unusual resist- ance. If so, it might be possible to relate the in
vitro assay of drug resistance of whole leukaemic populations to particular resistance mechanisms within cells of those populations and, perhaps, to clinical resistance too. There have been few reports of correlations between in vitro resistance and putative resistance mechanisms [6] but in vitro resistance has been reported to distinguish between responders and non-responders in de novo A M L [7, 8] and has been found to predict remission duration induced by thi- oguanine, daunorubicin and prednisolone in child- hood acute lymphatic leukaemia [9]. Poor remission rates correlated with high MDR-1 expression in a variety of leukaemias [10] and in A M L [11]. Similarly, raised numbers of P170-P-glycoprotein (Pgp) positive cells have been reported to predict poorer prognosis in A M L [12].
We have used an indirect (MTF) assay of cell survival in increasing concentrations of daunorubicin (anthracycline), to determine IDs0S for leukaemic blasts f rom chronic B-lymphocytic leukaemia (BCLL) and from de novo , refractory and relapsed acute myeloid leukaemia (AML) patients. These ~Ds0S are set in the context of those determined for normal blood and marrow populations and for the drug-selected CEM VLB100 (VLB) T-lymphoblastoid cell line. VLB cells were originally chronically exposed to vinblastine [13] resulting in amplification of the M D R - 1 gene with resultant elevated levels of membrane P170 P-glycoprotein which renders VLB cells a useful model of multidrug resistance. We have added the ~modifier' cyclosporin to our drug titrations to check whether Pgp is present and func- tioning. Cyclosporin blocks P170 function [5, 14, 15] which leads to marked sensitization of model VLB cells to cytotoxic drugs such as daunorubicin. Another way of checking for P170 function is to compare the IDs0 of daunorubicin with that of ida- rubicin which lacks a hydroxymethyl group and which escapes efflux by P170. The two ~Ds0S should differ radically where P170 is an important component of resistance. Finally, we have measured numbers of P170 positive cells in our normal and leukaemic sus- pensions as a way of substantiating any role for P- glycoprotein in in vitro resistance.
Methods
Patients Fresh marrow and blood from, respectively, 11 and 8
normal, healthy volunteers, from 17 patients with de novo AML, seven patients in remission, five at relapse and two with refractory disease, and 22 samples from 17 BCLL patients were collected into EDTA vacutainers, diluted as required in Hepes-buffered modified Eagles medium
(MEM, ICN Flow) and mononuclear cells (MNC) prepared by centrifugation over J-prep density solution (Tech Gen) at 500 g for 25 min. Leukaemic MNC containing more than 10% lymphocytes were discarded. Lymphocytes (median concentration 84%) were purified from normal blood samples by adherence removal of monocytes during incu- bation of MNC on plastic for 90min at 37°C in RPMI (Gibco) supplemented with 5% FCS (Imperial Labs) in a 5% CO2 environment. All procedures were approved by the Ethics Committee of South Glamorgan Health Auth- ority. Details of the AML patients are given in Table 1. Fifteen of the 17 BCLL patients had received prior chemotherapy (usually chlorambucil alone) for varying periods of time.
Drugs
Daunorubicin (Cerubidin, Rh6ne-Poulenc) and ida- rubicin (Zavedos, Farmitalia) were used over the range 2.4-5000 ng/ml and etoposide (Vepesid, Bristol-Meyers) over the range 0.125-128 gg/ml. The modifier cyclosporin (Sandoz) was titrated and used at maximally non-toxic doses to VLB cells (at 1.25 ~g/ml of culture). Twenty milligram aliquots of daunorubicin and 10 mg aliquots of idarubicin were dissolved in Hepes-buffered, modified Eagles medium (MEM, ICN°Flow). Cyclosporin was diluted in absolute alcohol to 5 mg/ml and further diluted to 63 gg/ml in MEM.
MTT assay
MNC samples containing more than 70% blasts and less than 10% lymphocytes were resuspended at 106 cells per ml in RPMI + 5% foetal calf serum (FCS, Imperial Labs). CEM and CEM VLB100 cells were suspended at 105/ml. Cells were then seeded into 96-well microtitre plates (Nunc, Gibco-BRL) and drugs then added to triplicate wells in five, four-fold dilutions. After 2 days of culture at 5% CO2 in air in a humidified incubator at 37°C, 10 ~tl of a 5 mg/ml solution of MTT (3,(4,5-dimethylthiazol-2-yl)2,5-diphenyl tetrazolium bromide; Sigma) was added to each well and the plates incubated a further 2h under the same conditions. Viable cells reduce this formazan dye to a purple precipitate which can be solubilized following addition of 25 ~tl of a 1 : 1 mixture of phosphate buffered saline and dimethylformamide (Sigma) containing 20% SDS (BDH), to each well and incubating the plates at 37°C for a further 2 h in a humidified environment. This procedure is taken from that published by Hansen et al. [16].
Absorbance at 570nm for each well was read on a Titertek microplate reader, and more recently on an Anthos HT2 microplate reader, and the mean absorbance for triplicates representing each drug concentration were expressed as a percentage of the mean absorbance of control triplicates containing cells but no drugs. IDs0S for cell populations were calculated by plotting the percent absorbance against drug concentration and taking the drug concentration required to reduce absorbance by 50%; in the case of the Anthos HT2 microplate reader the curves and calculation of IDs0s were handled by Mikrotek Labsoft software (Denley).
Cell lines
CEM and CEM VLB100 cell lines were cultured in the absence of selecting drugs in RPMI + 5% FCS (Imperial Labs) supplemented with penicillin and streptomycin at 100 units/ml and 100 ~tg/ml, respectively.
Drug resistance in leukaemic blasts and normal cells
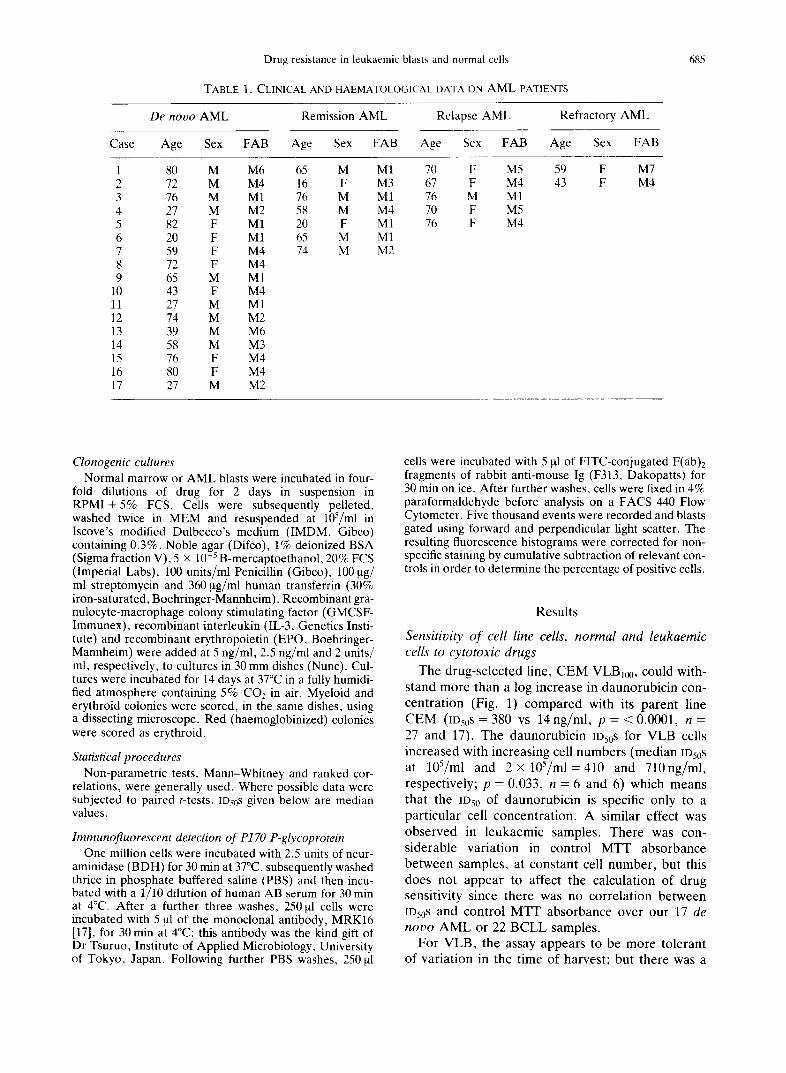
TABLE 1. CLINICAL AND HAEMATOLOGICAL DATA ON A M L PATIENTS
685
De novo AML Remission AML
Case Age Sex FAB Age Sex FAB
Relapse AML Refractory AML
Age Sex FAB Age Sex FAB
l 80 M M6 2 72 M M4 3 76 M M1 4 27 M M2 5 82 F M1 6 20 F M1 7 59 F M4 8 72 F M4 9 65 M M1
10 43 F M4 11 27 M M1 12 74 M M2 13 39 M M6 14 58 M M3 15 76 F M4 16 80 F M4 17 27 M M2
65 M M1 16 F M3 76 M M1 58 M M4 20 F M1 65 M M1 74 M M2
70 F M5 59 F M7 67 F M4 43 F M4 76 M M1 70 F M5 76 F M4
Clonogenic cultures Normal marrow or AML blasts were incubated in four-
fold dilutions of drug for 2 days in suspension in RPMI + 5% FCS. Cells were subsequently pelleted, washed twice in MEM and resuspended at 105/ml in Iscove's modified Dulbecco's medium (IMDM, Gibco) containing 0.3%, Noble agar (Difco), 1% deionized BSA (Sigma fraction V), 5 × 10 -5 B-mercaptoethanol, 20% FCS (Imperial Labs), 100 units/ml Penicillin (Gibco), 100 ~tg/ ml streptomycin and 360 ~tg/ml human transferrin (30% iron-saturated, Boehringer-Mannheim). Recombinant gra- nulocyte-macrophage colony stimulating factor (GMCSF- Immunex), recombinant interleukin (IL-3, Genetics Insti- tute) and recombinant erythropoietin (EPO, Boehringer- Mannheim) were added at 5 ng/ml, 2.5 ng/ml and 2 units/ ml, respectively, to cultures in 30 mm dishes (Nunc). Cul- tures were incubated for 14 days at 37°C in a fully humidi- fied atmosphere containing 5% CO2 in air. Myeloid and erythroid colonies were scored, in the same dishes, using a dissecting microscope. Red (haemoglobinized) colonies were scored as erythroid.
Statistical procedures Non-parametric tests, Mann-Whitney and ranked cor-
relations, were generally used. Where possible data were subjected to paired t-tests. ID50s given below are median values.
Immunofluorescent detection of P170 P-glycoprotein One million cells were incubated with 2.5 units of neur-
aminidase (BDH) for 30 min at 37°C, subsequently washed thrice in phosphate buffered saline (PBS) and then incu- bated with a 1/10 dilution of human AB serum for 30 min at 4°C. After a further three washes, 250 ~tl cells were incubated with 5 ~tl of the monoclonal antibody, MRK16 [17], for 30 min at 4°C: this antibody was the kind gift of Dr Tsuruo, Institute of Applied Microbiology, University of Tokyo, Japan. Following further PBS washes, 250 ~tl
cells were incubated with 5 btl of FITC-conjugated F(ab)2 fragments of rabbit anti-mouse Ig (F313, Dakopatts) for 30 min on ice. After further washes, cells were fixed in 4% paraformaldehyde before analysis on a FACS 440 Flow Cytometer. Five thousand events were recorded and blasts gated using forward and perpendicular light scatter. The resulting fluorescence histograms were corrected for non- specific staining by cumulative subtraction of relevant con- trois in order to determine the percentage of positive cells.
Results
Sensitivity of cell line cells, normal and leukaemic cells to cytotoxic drugs
The drug-selected line, C E M VLB100, could with- stand more than a log increase in daunorubicin con- centra t ion (Fig. 1) compared with its parent line C E M (ID50S = 380 vs 14 ng/ml , p = < 0.0001, n = 27 and 17). The daunorubic in IDs0S for VLB cells increased with increasing cell numbers (median Ds0s at 105/ml and 2 × 1 0 S / m l = 4 1 0 and 710ng /ml , respectively; p = 0.033, n = 6 and 6) which means that the 1950 of daunorubic in is specific only to a part icular cell concentra t ion. A similar effect was observed in leukaemic samples. There was con- siderable variat ion in control M T r absorbance between samples, at constant cell number , but this does not appear to affect the calculation of drug sensitivity since there was no correlat ion between IDs0S and control M T T absorbance over our 17 de nooo A M L or 22 B C L L samples.
For VLB, the assay appears to be more tolerant of variat ion in the time of harvest; but there was a

686 P. BAINES et al.
ID50 to Daunorubicin - ng/ml 10000
1000
,oo !11 1o BN ~
VLB CFM LY B M N C AML CLL
FIG. 1. Drug sensitivity of haemopoietic cell populations. IDs0s (solid columns) to daunorubicin for CEM VLB100 cell line cells (VLB), CEM cell line cells (CEM), blood lymphocytes (LY), marrow mononuclear cells (BMNC), de n o v o AML blasts (AML) and B-lymphocytic leukaemic blasts (BCLL). Hatched columns are IDs0s calculated with
both daunorubicin and cyclosporin present.
significant change in IDs0 for leukaemic AML samples harvested after 2 or 3 days of culture (medians: 198 and 105 ng/ml, respectively; p = 0.02).
CEM VLB10 o proved much less resistant to ida- rubicin than to daunorubicin 0Ds0S = 40 and 380 ng/
ID50 to drug - ng/ml
1000 I
100
10
VLB Dr VLB Ida CEM Dr CEM Ida
FIG. 2. Sensitivity of VLB and CEM cell populations to daunorubicin or idarubicin (solid columns) and the com- parative effect of cyclosporin (hatched columns) on [Ds0s
to both drugs in VLB cells.
I D 5 0 to Etoposide - ug/ml 100
10
0.1 ~ VLB CEM LY AML CLL
FIG. 3. Sensitivity of haemopoietic cell populations to etoposide. Legend as for Fig. 1.
ml, respectively; p = 0.0005) and this was only twice as great as the IDs0 of CEM parent cells to idarubicin (20ng/ml) (Fig. 2); the IDs0 of CEM cells to daunorubicin = 14 ng/ml. CEM VLB100 cells proved four-fold more resistant than parent CEM cells to etoposide 0Ds0S = 1.2 and 0.28 ~tg/ml, respectively; p = 0.0086) (Fig. 3).
Blood lymphocytes were markedly more resistant to daunorubicin than were even VLB cells (ID50 med ians=3500ng /ml vs 380ng/ml, p<0.0001) (Fig. 1). Marrow mononuclear cells, comprising vari- able mixtures of immature granulocytes, monocytes and lymphocytes were far more sensitive (Fig. 1, median IDs0 = 80 ng/ml). The distribution of normal cell sensitivities to etoposide paralleled those for daunorubicin: median etoposide IOs0S (Fig. 3) were 64 ~tg/ml for blood lymphocytes, 4.5 ~tg/ml for mar- row mononuclear cells (not shown) but only 1.2 ~tg/ ml for VLB. No data were collected for idarubicin toxicity towards normal cells.
IDs0S for d e n o v o AML blasts varied from 5 to 300 ng/ml of daunorubicin (Fig. 4) with a median of 105 ng/ml (Fig. 1) and from 0.12 to 60 ~tg/ml of etoposide; median 2.3 ~tg/ml (Fig. 3). There was a positive correlation between II)50s for daunorubicin and etoposide (r = 0.724, p = < 0.01; n = 13). IDs0S for idarubicin were available for only three AML samples and were always close to the ID50S for dau- norubicin. (IDs0S for the three samples were, for daunorubicin and idarubicin, respectively, 28 and 25 ng/ml; 240 and 200ng/ml; 105 and 105 ng/ml). Irrespective of drug, ID50S for d e n o v o AML blasts were similar to those of normal marrow mononuclear

Drug resistance in leukaemic blasts and normal cells 687
IDSO to Daunorubicin - n g l m l
350 -
300 "
250 "
200 •
1 5 0
100 -
5 0 -
O -
P P P P P P P P P P P P P P P P RI RI RI RI RI Rf Rf
Patient Type
FIG. 4. Daunorubicin sensitivity of individual AML samples (hatched columns) and the effect of adding cyclo- sporin on IDso (speckled columns): black columns denote the change in IDs0 on addition of cyclosporin as a percentage of the ID50 in daunorubicin alone. P = presentation samples; R1 = relapse samples; Rf = refractory samples.
cells (median IDsoS for daunorubicin = 105, 80 ng/ml respectively: Fig. 1; median IDs0S for etoposide = 2.6, 4.5 lxg/ml, respectively: Fig. 3) but de n o v o blasts were considerably more sensitive than blood lym- phocytes (median IDs0s for daunorubicin = 105, 3500ng/ml , respectively, p = <0.0001; and for etoposide = 2.6, 64 Ixg/ml, p = 0.0112).
There was no correlation between IDs0S for dau- norubicin or etoposide and CD34 positive cell num- bers in samples f rom de n o v o A M L patients. IDs0S for the five relapsed samples and two refractory samples, received during the time of the study, ranged from 27 to 240 ng/ml for daunorubicin and 0.9-2.8 Ixg/ml for etoposide. These values are distributed through- out the range of de n o v o AMLs and are not sig- nificantly more resistant nor more sensitive. Remission marrow MNC, taken 2-8 weeks after chemotherapy, were significantly more resistant to daunorubicin (Fig. 5) than were normal marrow MNC (ms0s for remission and normal MNC = 200 and 80 ng/ml, respectively; p = 0.03).
Daunorubicin ID50S of three untreated BCLLs were 150, 190 and 26ng /ml (Fig. 6). Median IDs0s for BCLL samples taken within 10 weeks, or 20 weeks after, chemotherapy were 54 and 49 ng/ml, respect- ively, and were not significantly different. Dau- norubicin IDs0S of all BCLL samples ranged from 7 to 200 ng/ml (Fig. 6), with a median of 48 ng/ml (Fig. 1). These values were significantly lower than the daunorubicin IDs0S of blood lymphocytes (p = <0.0001) or A M L blasts (p = 0.04). There was no correlation between IDs0S tO daunorubicin and those to etoposide which varied f rom 0.4 to 21.5 ~tg/ml (Fig. 3), giving a median of 2 Ixg/ml etoposide. This
ID50 to Daunorubicin - ng/ml 250
200
1 5 0
100
50
0
B M N C R E M I S ' N MNC
FIG. 5. Relative resistance to daunorubicin (solid columns) of mononuclear cells from normal donors or remission AML patients, 2-8 weeks after chemotherapy. Hatched columns are IDs0s to daunorubicin in the presence of cyclo-
sporin.
was significantly lower than the etoposide ID50 for blood lymphocytes (p = 0.007). IDs0S to idarubicin were available for five BCLL samples and were sig- nificantly lower than those for daunorubicin (IDs0S = 62 and 37 ng/ml for daunorubicin and idarubicin, respectively, over these five patients; p = 0.037); these data are not illustrated.
I D 5 0 to D a u n o r u b i c l n - n g / m l
2 5 0 -
2 0 0 -
1 5 0 -
1 0 0 -
5 0 -
O -
U U U T T T T T T T T T T T R R R R R R R O
Pa t ien t type
FIG. 6. Daunorubicin sensitivity of individual BCLL samples (hatched columns) and the effect of adding cyclo- sporin on IDs0 (speckled columns): black columns denote the change in ID50 on addition of cyclosporin as a percentage of the IDs0 in daunorubicin alone. U = samples from untreated patients: T = samples from patients treated more than 20 weeks ago; R = samples from patients treated less
than 10 weeks ago; O = treatment history unknown.
688 P. BAINES et al.
Reversal of resistance with cyclosporin
Suitable non-cytotoxic doses of cyclosporin were chosen from titrations of this modifier alone against VLB and leukaemic cells. Cyclosporin at 1.25 ~tg/ ml, induced an approximate log reversal of VLB's resistance to daunorubicin (median IDs0S without and with cyclosporin = 380 and 21 ng/ml, respectively, p = <0.0001; Fig. 1). Cyclosporin reduced VLB's median IDs0 to etoposide only two-fold (from 1.2 to 0.59 ~tg/ml, p = 0.0044; Fig. 3). The modifier had a smaller, non-significant effect on CEM cells (median IDs0S for daunorubicin alone and daunorubicin + cyclosporin were 14 and 13 ng/ml, respectively.
Cyclosporin failed to reverse the high resistance exhibited by blood lymphocytes to daunorubicin 0Ds0S without and with cyclosporin = 3500 ng/ml, 2835ng/ml; Fig 1) or to etoposide 0Ds0s, respectively = 64 ~tg/ml, 56.4 ~tg/ml; Fig. 3). Simi- larly, cyclosporin had little impact on the IDs0S of normal marrow mononuclear cells for daunorubicin (80ng/ml vs 66.4ng/ml) (Fig 1). The modifier reduced daunorubicin IDs0S in 14 of 17 de novo AML samples (Fig. 4) but there was no correlation between daunorubicin Ios0s and the increase in sensitivity achieved by cyclosporin. Median ]Ds0s (Fig. 1) for daunorubicin without and with cyclosporin were 105 and 64 ng/ml, respectively (p = 0.0013). Cyclospo- rin, however, did not significantly change the IDs0S of de novo AML samples to etoposide 0Ds0S to eto- poside without and with cyclosporin =2 .3 and 1.9 ~tg/ml, respectively; Fig. 3). Unlike normal mar- row MNC, cyclosporin appeared to increase drug sensitivity in seven remission samples collected 2-8 weeks after chemotherapy (Fig. 5) although this did not attain significance at the 5% level; ID50S for remission samples with daunorubicin alone, or with cyclosporin = 200 vs 110 ng/ml; p = 0.078).
Cyclosporin decreased daunorubicin ID50S in 16 of 22 BCLL samples (Fig. 6). There was a significant correlation (r = 0.465, n = 22; p < 0.05) between daunorubicin IDs0S and the increase in sensitivity achieved by cyclosporin in BCLL samples. The median ]Dso fell from 48 to 31 ng/ml (Fig. 1). This decrease was significant (p = 0.016).
Effect of daunorubicin on normal colony growth
ID50S were similar for myeloid and erythroid col- ony-forming cells (median = 20 ng/ml for both pro- genitor types; n = 10) and were not significantly different from the median IDs0 of 26 ng/ml for leu- kaemic clonogenic cells in the four samples which would grow in our semi-solid culture conditions. IDs0S for myeloid and erythroid colony-forming cells from five recently induced remission marrows were similar
I D 5 0 to Daunorublcin - n g / m l % P 1 7 0 + ve ceils 4 0 0 r ~ 1 0 0
300
2 0 0
1 0 0
8 0
6 0
40
20
0 ~ 0 P P P P P P P P P P P P P P RI RI Rf VLB CEM BM
Patient Type
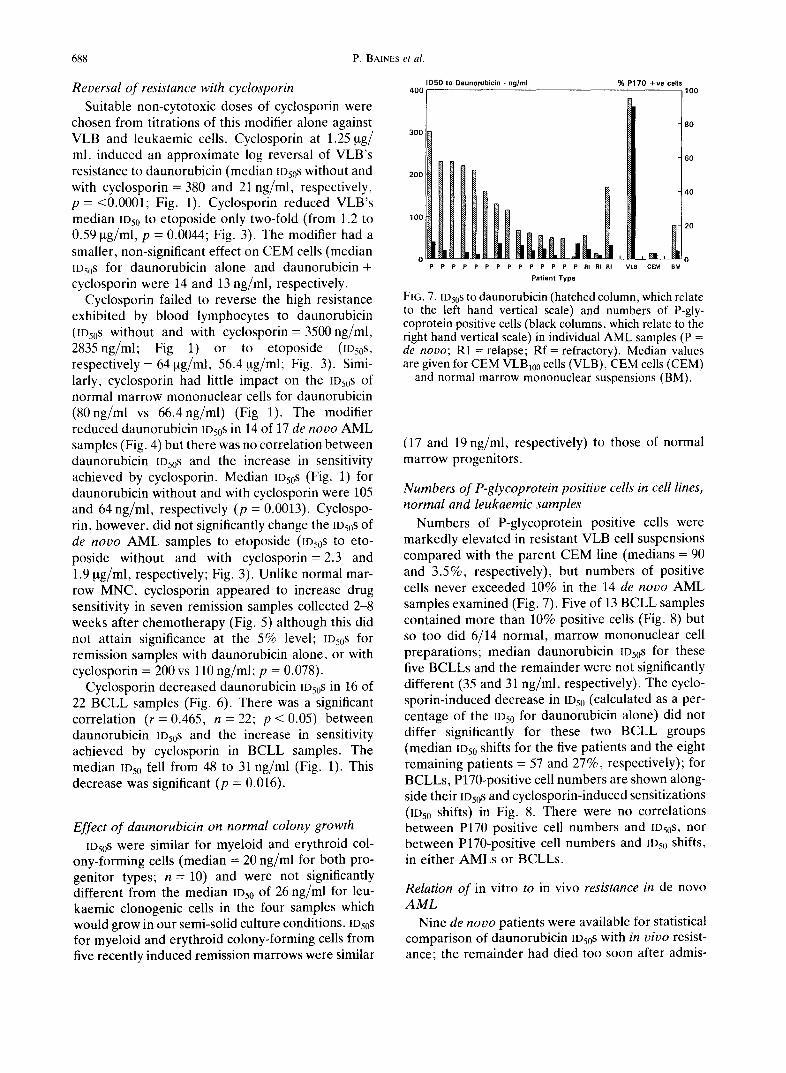
FIG. 7. ID50s to daunorubicin (hatched column, which relate to the left hand vertical scale) and numbers of P-gly- coprotein positive cells (black columns, which relate to the right hand vertical scale) in individual AML samples (P = de novo; R1 = relapse; Rf = refractory). Median values are given for CEM VLB100 cells (VLB), CEM cells (CEM)
and normal marrow mononuclear suspensions (BM).
(17 and 19 ng/ml, respectively) to those of normal marrow progenitors.
Numbers of P-glycoprotein positive cells in cell lines, normal and leukaemic samples
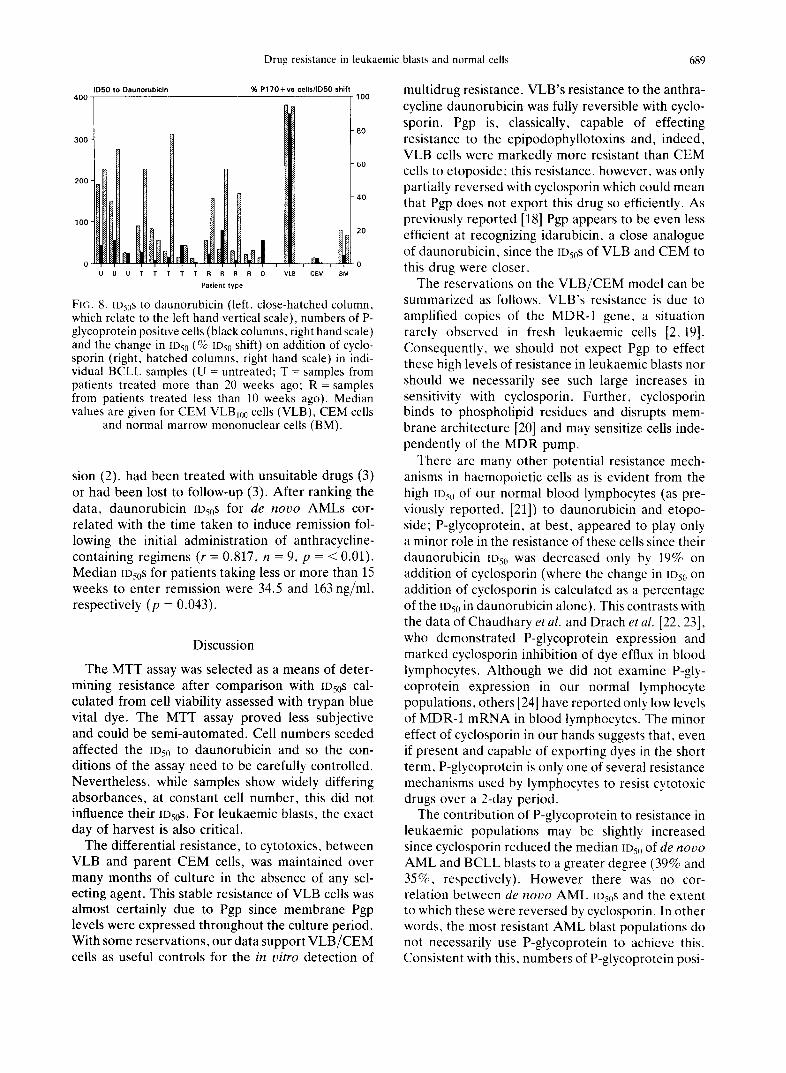
Numbers of P-glycoprotein positive cells were markedly elevated in resistant VLB cell suspensions compared with the parent CEM line (medians = 90 and 3.5%, respectively), but numbers of positive cells never exceeded 10% in the 14 de novo AML samples examined (Fig. 7). Five of 13 BCLL samples contained more than 10% positive cells (Fig. 8) but so too did 6/14 normal, marrow mononuclear cell preparations; median daunorubicin IDs0S for these five BCLLs and the remainder were not significantly different (35 and 31 ng/ml, respectively). The cyclo- sporin-induced decrease in IDs0 (calculated as a per- centage of the IOs0 for daunorubicin alone) did not differ significantly for these two BCLL groups (median ID50 shifts for the five patients and the eight remaining patients = 57 and 27%, respectively); for BCLLs, P170-positive cell numbers are shown along- side their Ios0s and cyclosporin-induced sensitizations (IDs0 shifts) in Fig. 8. There were no correlations between P170 positive cell numbers and IOs0S, nor between P170-positive cell numbers and 1Ds0 shifts, in either AMLs or BCLLs.
Relation of in vitro to in vivo resistance in de novo AML
Nine de novo patients were available for statistical comparison of daunorubicin IDs0S with in vivo resist- ance; the remainder had died too soon after admis-
Drug resistance in leukaemic blasts and normal cells 689
I D 5 0 t o D a u n o r u b i c i n
4 0 0 7
3 0 0 -
200 •
1 0 0 "
O "
% P 1 7 0 + v e ce l ls / lD50 shift r 1 0 0
" 8 0
" 6 0
- 4 0
- 2 0
0
VLB CEM BM U U U T T T T T R R R R 0
P a t i e n t type
FIG. 8. [Ds~S to daunorubicin (left, close-hatched column, which relate to the left hand vertical scale), numbers of P- glycoprotein positive cells (black columns, right hand scale) and the change in IDs0 (% [Ds~j shift) on addition of cyclo- sporin (right, hatched columns, right hand scale) in indi- vidual BCLL samples (U = untreated; T = samples from patients treated more than 20 weeks ago: R = samples from patients treated less than 10 weeks ago). Median values are given for CEM VLBj00 cells (VLB), CEM cells
and normal marrow mononuclear cells (BM).
sion (2), had been treated with unsuitable drugs (3) or had been lost to follow-up (3). After ranking the data, daunorubicin [Ds0S for de n o v o AMLs cor- related with the time taken to induce remission fol- lowing the initial administration of anthracycline- containing regimens (r = 0.817, n = 9, p = < 0.01). Median IDs0s for patients taking less or more than 15 weeks to enter remission were 34.5 and 163 ng/ml, respectively (p = 0.043).
Discussion
The MTT assay was selected as a means of deter- mining resistance after comparison with tDs0S cal- culated from cell viability assessed with trypan blue vital dye. The MTT assay proved less subjective and could be semi-automated. Cell numbers seeded affected the IDs0 to daunorubicin and so the con- ditions of the assay need to be carefully controlled. Nevertheless, while samples show widely differing absorbances, at constant cell number, this did not influence their [Ds0S. For leukaemic blasts, the exact day of harvest is also critical.
The differential resistance, to cytotoxics, between VLB and parent CEM cells, was maintained over many months of culture in the absence of any sel- ecting agent. This stable resistance of VLB cells was almost certainly due to Pgp since membrane Pgp levels were expressed throughout the culture period. With some reservations, our data support VLB/CEM cells as useful controls for the in vitro detection of
multidrug resistance. VLB's resistance to the anthra- cycline daunorubicin was fully reversible with cyclo- sporin. Pgp is, classically, capable of effecting resistance to the epipodophyllotoxins and, indeed, VLB cells were markedly more resistant than CEM cells to etoposide: this resistance, however, was only partially reversed with cyclosporin which could mean that Pgp does not export this drug so efficiently. As previously reported [18] Pgp appears to be even less efficient at recognizing idarubicin, a close analogue of daunorubicin, since the ID50S of VLB and CEM to this drug were closer.
The reservations on the V L B / C E M model can be summarized as follows. VLB's resistance is due to amplified copies of the MDR-1 gene, a situation rarely observed in fresh leukaemic cells [2, 19]. Consequently, we should not expect Pgp to effect these high levels of resistance in leukaemic blasts nor should we necessarily see such large increases in sensitivity with cyclosporin. Further, cyclosporin binds to phospholipid residues and disrupts mem- brane architecture [20] and may sensitize cells inde- pendently of the MDR pump.
There are many other potential resistance mech- anisms in haemopoietic cells as is evident from the high IDs0 of our normal blood lymphocytes (as pre- viously reported, [21]) to daunorubicin and etopo- side; P-glycoprotein, at best, appeared to play only a minor role in the resistance of these cells since their daunorubicin IDs0 was decreased only by 19% on addition of cyclosporin (where the change in IDs0 on addition of cyclosporin is calculated as a percentage of the IDsI, in daunorubicin alone). This contrasts with the data of Chaudhary et al. and Drach et al. [22, 23], who demonstrated P-glycoprotein expression and marked cyclosporin inhibition of dye efflux in blood lymphocytes. Although we did not examine P-gly- coprotein expression in our normal lymphocyte populations, others [24] have reported only low levels of MDR-1 mRNA in blood lymphocytes. The minor effect of cyclosporin in our hands suggests that, even if present and capable of exporting dyes in the short term, P-glycoprotein is only one of several resistance mechanisms used by lymphocytes to resist cytotoxic drugs over a 2-day period.
The contribution of P-glycoprotein to resistance in leukaemic populations may be slightly increased since cyclosporin reduced the median tDs0 of de n o v o
AML and BCLL blasts to a greater degree (39% and 35%, respectively). However there was no cor- relation between de n o v o AML IDs0S and the extent to which these were reversed by cyclosporin. In other words, the most resistant AML blast populations do not necessarily use P-glycoprotein to achieve this. Consistent with this, numbers of P-glycoprotein posi-
690 P. BAINES et al.
tive cells, where measured, were low (10% or less) and did not correlate with IDs0 s either. This is similar to the conclusions of Pieters et al. [25], in childhood ALL. A low incidence of P-glycoprotein-positive cells in AML has also been reported by others [26].
Earlier publications had suggested that in vitro
chemosensitivity assays [7, 8] as well as MDR-1 mRNA levels [10,27] and P-glycoprotein-positive cell numbers [12] in de n o v o leukaemic AML samples, could be related to clinical resistance. Although our data suggest that there is no simple relationship between Pgp function and in vitro resist- ance in AML there was a positive correlation between daunorubicin ID50S, in our de n o v o AMLs, and time to remission. This confirms that in vitro
chemosensitivity assays provide a useful measure of in v i vo resistance.
Despite their low resistance to daunorubicin, a role for P-glycoprotein appears firmer in BCLLs since the cyclosporin-induced increase in sensitivity (IDs0 shifts) correlated with their lDs0S and numbers of P- glycoprotein positive cells exceeded 10% in a greater proportion of patients (5/13); that the median IDs0 shift for these five BCLL samples were not sig- nificantly different from the median value for the remaining eight samples (57 and 27%, respectively) may well reflect the small sample size. Furthermore, BCLLs were significantly more sensitive to idarubicin than to daunorubicin, as would be expected if P- glycoprotein was partly responsible for resistance. Increased levels of MDR1 mRNA and P-gly- coprotein have previously been reported in BCLL [4, 24, 28].
Blasts from relapsed or refractory AML patients did not show increased IDs0S, nor were numbers of P170 positive cells increased, and this is in accord with an earlier report [29]. Yet mononuclear cells from remission marrows collected 2-8 weeks after chemotherapy which included adriamycin, were both significantly more resistant to daunorubicin and more responsive to cyclosporin than were normal marrow mononuclear cells. This could mean that the regen- erative process enhances the resistance of marrow cells. Alternatively Pgp-mediated resistance may be elevated for a few weeks, at least, following chemo- therapy. This would explain the raised MDR-1 mRNA levels frequently reported in heavily treated refractory disease [1, 2, 4, 5, 11]. Nevertheless, we found no difference between daunorubicin IDs0S for samples from recently treated, untreated BCLLs and BCLLs which had not been treated for 5 months or more. Nor was there a correlation between ID50S a n d
the time that had elapsed following treatment. This is consistent with published data showing no clear relationship between MDR-1 mRNA transcript or P-
glycoprotein levels and prior chemotherapy in BCLL [24, 30].
The relative resistance of remission marrows is not expressed in the progenitor populations which were as sensitive as normal, untreated myeloid or eryth- roid progenitors and whose IDs0S to daunorubicin were similar to leukaemic clonogenic cells. It has been reported that primitive haemopoietic pro- genitor cells, expressing CD34, possess high levels of Pgp [31]. If so, this does not appear to unduly protect clonogenic cells. Over our 17 de n o v o AMLs, there was no correlation between CD34 and blast ~Ds0S despite CD34 positivity being associated with a low remission rate in de n o v o AML [12].
P-glycoprotein appears to be only one of several mechanisms conferring drug resistance on de n o v o
AML and BCLL blasts. Its role in myeloid popu- lations regenerating following chemotherapy may be increased, which would explain the insensitivity of early-remission AML samples. While the underlying mechanisms of resistance in leukaemic blasts remain unresolved, detection of resistance in chemosen- sitivity assays does reflect in v ivo resistance in de n o v o AML. AML blasts, though, were not par- ticularly resistant in vitro, not even when from relapsed or refractory disease and BCLL blasts were more sensitive still, even when taken from recently treated patients.
Acknowledgements--We are indebted to Carol Tang and Louise Truran for technical assistance, to Dr Mike Morgan for advice on assay automation and software, to Steve Couzens for the CD34 data, to Sian Edwards for typing the manuscript and to the continued support of the clinical, technical and nursing staff. Recombinant factors were gen- erous gifts; GMCSF from Immunex, Seattle and recom- binant IL3 from the Genetics Institute, Massachusetts. MRK 16 monoclonal antibody was the kind gift of Dr Tsuruo, Institute of Applied Microbiology, University of Tokyo, Japan. Carol Tang and authors RAP and AA were supported by the Leukaemia Research Fund for Great Britain. Author ML was supported by the Welsh Scheme for the Development of Health and Social Research and the Leukaemia Research Fund for Great Britain.
References
1. Goldstein L. J., Galski H., Fojo A., Willingham N., Lai S. L., Gazdar A., Pirker R., Green A., Crist W., Brodeur G. M., Lieber M., Cossmann J., Gottesman M. M. & Pastan I. (1989) Expression of a multidrug resistance gene in human cancer. J. Natl Cancer Inst. 81, 116.
2. Holmes J. A., Jacobs A., Carter G., Janowska-Wie- czorek A. & Padua R. A. (1989) Multidrug resistance in haemopoietic cell lines, myelodysplastic syndromes and acute myeloblastic leukaemia Br. J. Haemat. 72, 40.
3. Sato H., Gottesman M. M., Goldstein L. J., Pastan I., Block A. M., Sandberg A. A. & Preisler H. D. (1990)
Drug resistance in leukaemic blasts and normal cells 691
Expression of the multidrug resistance gene in myeloid leukaemias. Leukemia Res. 14, 11.
4. Herweijer H., Sonneveld P., Baas, F. & Nooter K. (1990) Expression of mdrl and mdr3 multidrug genes in human acute and chronic leukaemia and association with stimulation of drug accumulation by cyclosporin. J. Natl Cancer Inst. 82, 1133.
5. Nooter K., Sonneveld P., Oostrum R., Herweijer H., Hagenbeek T. & Valerio D. (1990) Over expression of the mdrl gene in blast cells from patients with acute myelocytic leukaemia is associated with decreased anthracycline accumulation that can be restored by cyclosporin A. Int. J. Cancer 45, 263.
6. Salmon S. E., Grogan T. M., Miller T., Schener R. & Dalton W. S. (1989) Prediction of doxorubicin resist- ance in vitro in myeloma, lymphoma and breast cancer by P-glycoprotein staining. J. Natl Cancer Inst. 81,696.
7. Santini V., Bernabei P. A., Silvestro R., Silvestro L., Pozzo O. D., Bezzini R., Viano I., Gattei V., Saccardi R. & Ferrini P. R. (1989) In vitro chemosensitivity testing of leukaemic cells: prediction of response to chemotherapy in patients with acute non-lymphocytic leukaemia. Haemat. Oncol. 7, 287.
8. Sargent J. M. & Taylor C. G. (1989) Appraisal of the MTT assay as a rapid test of chemosensitivity in acute myeloid leukaemia. Br. J. Cancer 60, 206.
9. Pieters R., Huismans D. R. & Loonen A. H. (1991) Relation of cellular drug resistance to long-term clinical outcome in childhood acute lymphoblastic leukaemia. Lancet 338, 399.
10. Marie J. P., Zittoun R. & Sikic B. I. (1991) Multidrug resistance (mdrl) gene expression in adult acute leu- kaemias: correlations with treatment outcome in vitro dIug sensitivity. Blood 76, 586.
11. Sato H., Preisler H., Day R., Raza A., Lassan R., Browman G., Goldberg I., Vogler R., Grunwald H., Gottlieb A., Bennett J., Gottesman M. & Pastan I. (1990) MDR1 transcript levels as an indication of resist- ant disease in acute myelogenous leukaemia. Br. J. Haemat. 75, 340.
12. Campos L., Guyotat D., Archimbaud E., Calmard- Orial P., Tsuruo T., Trony J., Treille D. & Fiere D. (1992) Clinical significance of multidrug resistance P- glycoprotein expression on acute nonlymphoblastic leukaemia cells at diagnosis. Blood 79, 473.
13. Beck W. T., Cirtain M. C., Danks M. K., Felsted R. L., Safa A. R., Wolverton J. S., Parker Suttle D. & Trent J. M. (1987) Pharmacologic, molecular and cytogenetic analysis of 'atypical' multidrug resistant human leukaemic cells. Cancer Res. 47, 5455.
14. Keller R. P., Altermatt H. J., Nooter K., Poschmann G., Laissue J. A., Bollinger P. & Hiestand P. C. (1992) SDZPSC833, a non-immunosuppressive cyclosporin: its potency in overcoming P-glycoprotein-mediated multidrug resistance of murine leukaemia. Int. J. Can- cer 50, 593.
15. Keller R. P., Altermatt H. J., Donatsch P., Zihlmann H., Laissue J. A. & Hiestand P. C. (1992) Phar- macologic interactions between the resistance mod- ifying cyclosporin SDZPSC833 and etoposide (VP 16- 213) enhance in vivo cytostatic activity and toxicity. Int. J. Cancer 51,433.
16. Hansen M. B., Nielsen S. E. & Berg K. (1989) Re- examination and further development of a precise and rapid dye method for measuring cell growth/cell kill. J. lmmun. Meth. 119, 203.
17. Hamada H. & Tsuruo T. (1986) Functional role for the 170-180 kDa glycoprotein specific to drug resistant tumour cells as revealed by monoclonal antibodies. Proc. natn. Acad. Sci. U.S.A. 83, 7785.
18. Berman E. & McBride M. (1992) Comparative cellular pharmacology of daunorubicin and idarubicin in human multidrug-resistant leukaemia cells. Blood 79, 3267.
19. Ito Y., Tanimoto M., Kumazawa T., Okumura M., Morishima Y., Ohno R. & Saito H. (1989) Increased P-glycoprotein expression and multidrug resistant gene (mdrl) amplification are infrequently found in fresh acute leukaemia cells. Cancer 63, 1534.
20. Haynes M., Fuller L., Haynes D. H. & Miller J. (1985) Cyclosporin partitions into phospholipids resides and disrupts membrane architecture. Immun. Lett. 11, 343.
21. Kaspers G. J. L., Pieters R., Van Zantwijk C. H., De Latt P. A. S. M., De Waal F. C., Van Wering E. R. & Veerman A. J. P. (1991) bz vitro drug sensitivity of normal peripheral blood lymphocytes and childhood leukaemic cells from bone marrow and peripheral blood. Br. J. Cancer 64, 469.
22. Chaudharv P. M., Mechetner E. B. & Roninson I. B. (1992) Expression and activity of the multidrug resistance P-glycoprotein in human peripheral blood lymphocytes. Blood 80, 2735.
23. Drach D., Zhao S., Drach J., Machadevia R., Gat- tringer C., Huber H. & Andreef M. (1992) Sub- populations of normal peripheral blood and bone marrow cells express a functional multidrug resistant phenotype. Blood 80, 2729.
24. Holmes J. A., Jacobs A., Carter G., Whittaker J. A., Bentley D. P. & Padua R. A. (1990) Is the mdrl gene relevant in chronic lymphocytic leukemia. Leukemia 4, 216.
25. Pieters R., Hongo T., Loonen A. H., Huismans D.R., Broxterman H. J., Hahlen K. & Veerman A. J. P. (1992) Different types of non-P-glycoprotein mediated multiple drug resistance in children with relapsed acute lymphoblastic leukaemia. Br. J. Cancer 65, 691.
26. Muller M. R., Lennartz K., Nowrousian M. R., Dux R., Tsuruo T., Rajewsky M. F. & Seeber S. (1994) Improved flow-cytometric detection of low P-gly- coprotein expression in leukemic blasts by histogram subtraction analysis. Cvtometrv 15, 64.
27. Pirker R., Wallner J., Geissler K., Linbesch W., Haas O. A., Bettelheim P., Hopfner M., Scherrer R., Valent P., Havelec L., Ludwig H. & Lechner K. (1991) MDR1 gene expression and treatment outcome in acute myeloid leukaemia. J. Natl Cancer Inst. 83, 708.
28. Cumber P. M., Jacobs A., Hoy T.. Whittaker J. A., Tsuruo T. & Padua R. A. (1991) Increased drug accumulation ex vivo with cyclosporin in chronic lym- phatic leukaemia and its relationship to epitope mask- ing of P-glycoprotein. Leukemia 5, 1050.
29. Gruber A., Vitols S., Norgren S., Arestrom 1., Pet- erson C., Bjorkholm M., Reizenstein P. & Luthman It. (1992) Quantitative determination of mdrl gene expression in leukaemic cells from patients with acute leukaemia. Br. J. Cancer 66, 266.
30. Shustik C., Groulx N. & Gros P. (199l) Analysis of multidrug resistance (mdrl) gene expression in chronic lymphocytic leukaemia (CELL Br. J. Haemat. 79, 50.
31. Chaudhary P. M. & Roninson I. B. (1991) Expression and activity of P-glycoprotein, a multidrug efflux pump, in human haemopoietic stem cells. Cell 66, 85.


















