In the name of God Geriatric Psychiatry Mohamad Nadi. MD Psychiatrist.
59
In the name of God Geriatric Psychiatry Mohamad Nadi . MD Psychiatrist
-
Upload
derek-west -
Category
Documents
-
view
223 -
download
2
Transcript of In the name of God Geriatric Psychiatry Mohamad Nadi. MD Psychiatrist.
In the name of God
Geriatric Psychiatry
Mohamad Nadi . MDPsychiatrist
Geriatric population increasing
2000, estimated that 13% of Americans were over 65 years of age
By 2050, estimates are that 22% will be over the age of 65, and 5% over age 85.
The population is aging rapidly ; it is a global phenomenon
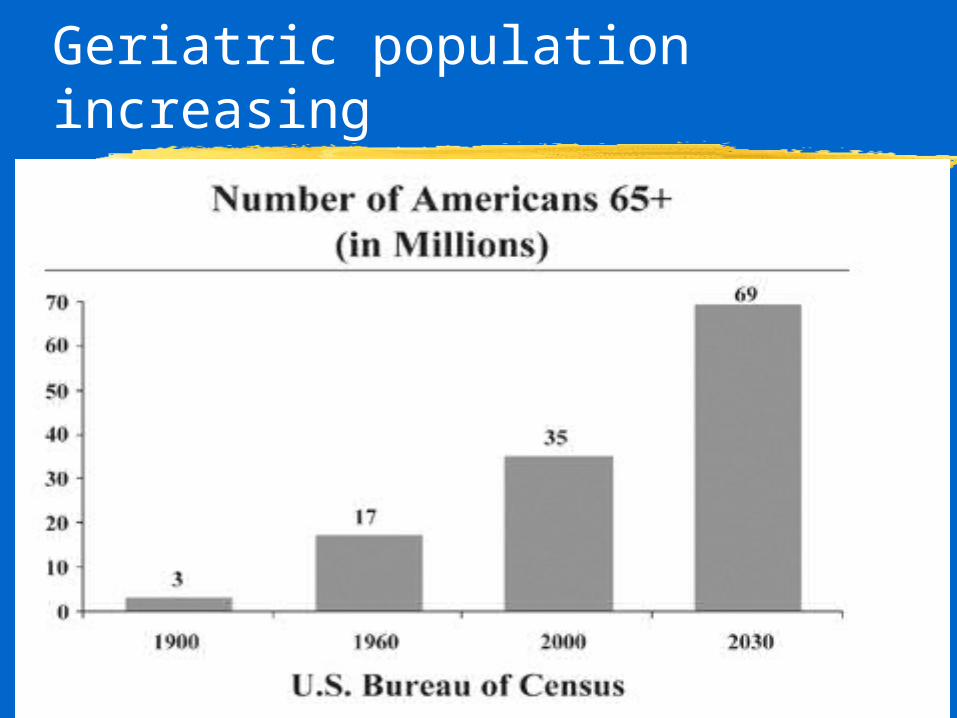
Geriatric population increasing
Why is it a subspecialty?
Mental disorders may have different manifestations, pathogenesis, and pathophysiology from younger adults
Coexisting chronic medical illnessMore medicinesCognitive impairmentsIncreased risk for social stressors,
including retirement and widowhood
What Is Normal Aging?
Some bodily functions decline with age, but health problems are not inevitable.
“Normal” aging must be differentiated from disease.
notion of chronological age (“how old are you?”) be abandoned, and instead that the stages of aging be considered.
Age cut-offs are artificial and arbitrary.
Prevalence of Mental Illnesses
Prevalence of psychiatric disorder (excluding dementia), was considerably lower in elderly compared younger adults.
Nearly 20 percent of persons older than age 65 years have diagnosable psychopathological symptoms.
The Aging Brain
Structural Changes
Neurochemical Changes
Changes in Cognitive and Motor
Abilities
Structural Changes Associated with Brain Aging
Decline of brain weight Neuron loss Neuronal atrophy Synaptic loss Pruning of dendritic trees White matter changes Gliosis
Neurochemical Changes in Aging
marked changes in dopaminergic neurons
decrease in the levels of markers of the cholinergic system
Changes in Motor Abilities
Gait slowing
Reaction time slowing
Balance changes (vestibular, sensory, motor, and brain)
Changes in Cognitive Abilities
Mental speed Executive function Retrieval Episodic memory vs procedural
memory Free recall worse than recognition
Changes in Cognitive Abilities
Cognition includes learning, memory, &. . .
Learning is the ability to gain new skills and information. It may be slower in elderly, especially verbal learning.
Changes in Cognitive Abilities
Memory : immediate, short- and long- term memory.
Immediate and Short-term memory remain intact, however, there ar affected by concentration which may be less in older adults.
Long-term memory is most affected by aging. Retrieval is less efficient; the elderly need more cues
Prospects for Healthy Brain Aging
Control hypertension Treat diabetes and vascular risk
factors Mental activity
Cognitively demanding pastimes Social networks
Prospects for Healthy Brain Aging
Regular physical activity
Diet : Similar components to a heart-healthy diet Relatively low fat and cholesterol Anti-oxidant rich diet
Mental Disorders of old age
Most common : cognitive disorders , depressive disorders, substances use.
Risk factors include loss of social roles, loss of autonomy, deaths, declining health, increased isolation, financial constraints, and decreased cognitive functioning.
Mental Disorders of old age
Most common : cognitive disorders
depressive disorders substances use.
Cognitive Disorders
Include: Delirium Dementia Amnestic Disorders Psychiatric disorders due to a Medical Condition
Postconcussional Syndrome
Delirium
Altered state of consciousness (reduced awareness of and ability to respond to the environment)
Cognitive deficits in attention, concentration, thinking, memory, and goal-directed behavior are almost always present
Usually acute and fluctuating
Features of delirium
May be accompanied by hallucinations, illusions, emotional lability, alterations in the sleep-wake cycle, psychomotor slowing or hyperactivity
Features of delirium
Types:Hyperactive , hyperalert delirium: almost always consultation
Hypoactive, hypoalert delirium: no consultation
Prevalence of delirium
The prevalence of delirium at hospital admission ranges from 10 to 35 percent Furthermore prevalence increases with multiple factors such as age, medication use, and comorbidities
prevalence of delirium
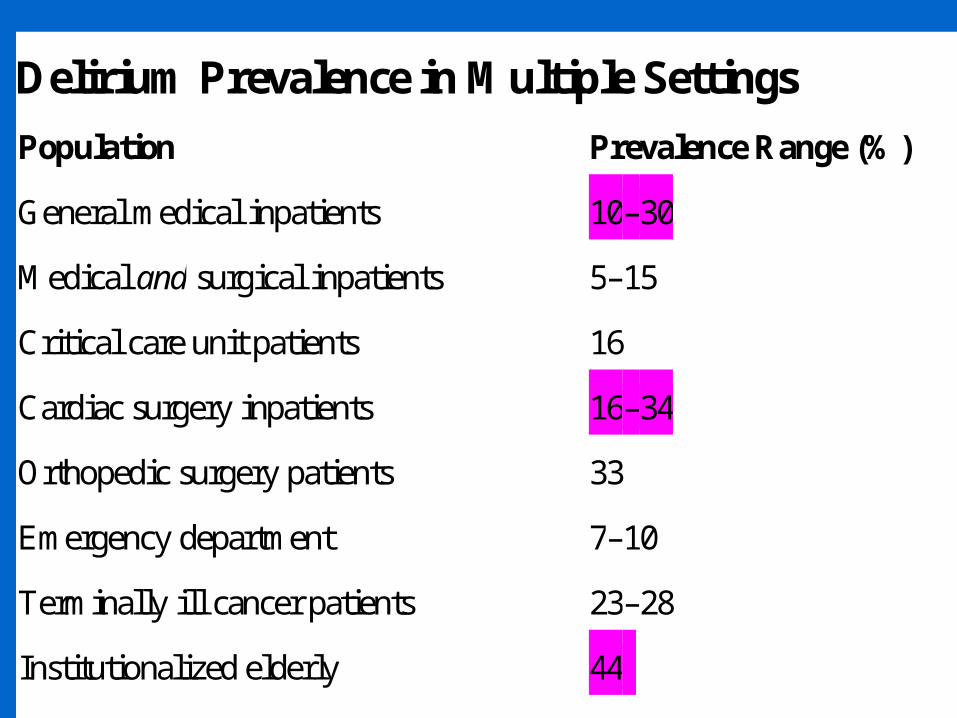
Delirium Prevalence in Multiple Settings
Population Prevalence Range (%)
General medical inpatients 10–30
Medical and surgical inpatients 5–15
Critical care unit patients 16
Cardiac surgery inpatients 16–34
Orthopedic surgery patients 33
Emergency department 7–10
Terminally ill cancer patients 23–28
Institutionalized elderly 44
N/A, not available.
The mortality of Delirium
The mortality outcome at 6 months post discharge for delirious patients not identified was three times higher than the delirious patients who were identified and treated.
25 percent of delirius postoperative patient had a lethal outcome; control population 13%
Burden of Delirium
Increased mortalityIncreased nursing careIncreased length of stayIncreased risk of cognitive declineIncreased risk of functional
decline
Burden of Delirium
Delay in postoperative mobilizationPrevention of early rehabilitationIncreased need for home care
servicesIncreased distress to caregiversBarrier to psychosocial closure in
terminally ill patient
Etiologies of Delirium in Elderly Patients
Systemic illnessesInfections: Pneumonia, urinary tract infection, sepsis, influenza
Cardiovascular conditions: Arrhythmia, congestive heart failure, myocardial infarction, severe hypertension
Etiologies of Delirium in Elderly Patients
MedicationsAnticholinergicsBenzodiazepines, other sedative-hypnotics (e.g., barbiturates)Antiarrhythmics, DigoxinCertain antibiotics (e.g., fluoroquinolones, clarithromycin)Interferons
Etiologies of Delirium in Elderly Patients
Primary brain diseases
Stroke or transient ischemic attackTrauma: Brain injury, subdural
hematomaInfection/inflammation: Abscess,
meningitis, encephalitis,
Etiologies of Delirium in Elderly Patients
Metabolic derangements:
Dehydration, hypoxia, hypoglycemia, hyperammonemia, uremia, hyponatremia, thiamine deficiency, hyperthyroidism
Etiologies of Delirium in Elderly Patients
Surgery or traumaHip fracture repairOpen heart surgery (e.g., coronary artery
bypass grafting)
Withdrawal states Alcohol Benzodiazepines, other sedative-hypnotics
Treatment of delirium
Look for underlying cause Close supervision, especially by
familyReorient frequentlyTry not to use restraints, as it can
worsen confusion.
Treatment of delirium
Medication Avoid polypharmacy
Low dose neuroleptic is treatment of choice, unless the delirium is due to withdrawal. If due to withdrawal, use a long-acting benzodiazepine.
Dementing Disorders
Only arthritis more common in geriatric population
5% have severe dementia, and 15% mild dementia in those over 65
Over 80, 20% have severe dementia
Dementing Disorders
Most common causes: Alzheimer’s disease, vascular dementia, alcoholism, and a combination of these 3
Risk factors are age, family history, and female sex
Dementia
ChangesCognition, memory, languagePersonality, abstract thinking, aphasiasHowever, level of awareness and alertness usually intact in early stages (differentiates dementia from delirium)
Noncognitive symptoms accompanying dementia
Depressive disorder Pathological laughter and crying Irritability and explosivenessDelusions or hallucinations occur
during the course of dementias in nearly 75%
Behavior problems in dementia
Agitation, restlessness, wandering, violence, shouting
Social and sexual disinhibition, impulsiveness
Sleep disturbances
Dementia and treatable conditions
10-15% from: heart disease, renal disease, and congestive heart failure
endocrine disorder, vitamin deficiency,
medication misuse primary mental disorders
Alzheimer’s Disease
50-60% of patients with dementia
5% of those who reach 65 have Alzheimer’s Disease
15-25% of those 85 or olderMore common in women
Alzheimer’s Disease
General sequence is memory, language, then visuospatial functions
On autopsy: neurofibrillary tangles and neuritic plaques
Involves cholinergic system arising in basal forebrain
Death occurs in about 7 yrs
Vascular Dementia
Second most common typeCan reduce known risk factors:
hypertension, diabetes, cigarette smoking, and arrhythmias
Other types of dementia
Multiple sclerosis is characterized by multifocal lesions in the white matter. May show early mood lability
Vitamin B12 deficiency--neurologic changes may occur before megaloblastic changes
HypothyroidismWilson’s disease
Treatment of behavior problems
Consider the likelihood of depression and anxiety first
Neuroleptics should not be first choice, and should be on a “prn” basis ,unless the patient is psychotic
Medicines for behavioral problems
Valproic acid, trazodone, and buspirone may be of benefit
BZDs may aggravate confusion
Drug treatment for Alzheimer’s Disease
Most current ones affect acetylcholine Tacrine Donepezil (Aricept) Rivastigmine (Exelon) Galantamine (Reminyl)Early intervention may prevent or slow decline
Depression
15% of all older adult community residences and nursing home patients
Accounts for 50% of older adult admissions to a psychiatric facility
Age is not a risk factor, but widowhood and chronic medical illness are
Depression
May have more somatic complaints such as decreased energy, sleep problems, pain, weakness, GI disturbances
Increases use of primary care medical resources
Depression
For those with a medical condition, depressive symptoms significantly reduce survival
Increases risk of suicide
Depression in medical illness
Medicines or the medical illness may cause depression
Rule out medical causesUse psychological symptoms
such as hopelessness, worthlessness, guilt
Depression in older adults
May have delusions which are usually persecutory or hypochondriacal in nature
Need treatment with both an antidepressant and an antipsychotic
ECT may be treatment of choice
Bereavement
Normal grief starts with shock, proceeds to preoccupation, then to resolution
May be prolonged in elderly, but consider major depression if there is marked psychomotor retardation, lasts over 2 months, marked impairment, or if suicidal ideation
Bipolar Disorder
Do organic workup if onset is over 65Usually more irritable than euphoric,
and paranoid rather than grandioseMay have dysphoric mania, with
pressured speech, flight of ideas, and hyperactivity, but thought content is morbid and pessimistic
Schizophrenia
Usually before 45, but there is a late onset type beginning after age 65
Paranoid type more commonResidual type occurs in 30% of those
affected: Emotional blunting, social withdrawal, eccentric behavior, and illogical thinking predominate
Delusional Disorder
Onset between 40 and 55Persecutory or somatic delusions
most commonMay be precipitated by stress,
loss, social isolation , visual impairment, deafness, immigrant status
Anxiety Disorders
Very common in elderlyMay occur first time after age
60, but not usuallyMost common are phobias,
especially agoraphobiaMay be due to medical causes or
depression
Substances and Alcohol
Brain is more sensitive as agesDue to changes in metabolism, a
given amount may produce a higher blood level
May worsen normal changes in sleep and sexual functioning
Sudden onset delirium in hospitalized patients usually from withdrawal
Personality disorders
Borderline, narcissistic, and histrionic personality disorders may become less intense
Before diagnosing a personality disorder, verify that it is not an improperly treated Axis I disorder
Some personality traits may become more pronounced
Sleep disorders
Advanced age is associated with increased prevalence of sleep disorders
REM sleep behavior disorder occurs among elderly men
Advanced sleep phase Dementia associated with more
arousals, increased stage I sleep; decreased stages 3/4