IN-SITU OPHTHALMIC GEL OF TIMOLOL MALEATE: …ejmanager.com/mnstemps/36/36-1418114354.pdf · Gellan...
20
www.iajpr.com Page5165 Indo American Journal of Pharmaceutical Research, 2014 ISSN NO: 2231-6876 IN-SITU OPHTHALMIC GEL OF TIMOLOL MALEATE: FORMULATION, RHEOLOGICAL STUDIES, IN-VITRO AND IN-VIVOEVALUATION Dhirajkumar Champalal Katariya, Poddar S. S K. M. Kundnani College of Pharmacy, Mumbai. Corresponding author Katariya Dhiraj Ap. Walaki, Tal: daund. Dist pune pin:412207. Copy right © 2014 This is an Open Access article distributed under the terms of the Indo American journal of Pharmaceutical Research, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. ARTICLE INFO ABSTRACT Article history Received 12/10/2014 Available online 30/11/2014 Keywords In-Situ Gel, Gellan Gum, Ophthalmic Drug Delivery System, Ophthalmic Formulations. The purpose of this study was to develop and characterize a series of gellan gum based in-situ gel forming solution of timolol maleate for its optimized application. The rheological behavior, gelling capacity, in-vitro drug release profile, anti-glaucoma study on rabbits and its mucoadhesive profile of gellan gum were evaluated. Gellan gum in-situ gel forming solution in the concentration range 0.25 to 1% w/v were prepared and evaluated to find out the optimum concentration of polymer to achieve formulation which would be liquid at non- physiological condition and became semi-solid at physiological condition. The rheological phenomenon showed shear thinning pseudoplastic behavior of gellan gum with timolol maleate. The results showed that the gellan gum can be used as an in-situ gelling vehicle to enhance the ocular bioavailability of timolol maleate.Through this work a meaningful platform for in-situ gelling type ophthalmic drops has been recommended. With further logistics, various API would be possible to be fitted in this. The suggestion has ample potential for scale up. Please cite this article in press as Dhirajkumar Ch. Katariya et al. In-situ ophthalmic gel of Timolol maleate: Formulation, rheological studies, in-vitro and in-vivoevaluation. Indo American Journal of Pharm Research.2014:4(11).
Transcript of IN-SITU OPHTHALMIC GEL OF TIMOLOL MALEATE: …ejmanager.com/mnstemps/36/36-1418114354.pdf · Gellan...

www.iajpr.com
Pag
e51
65
Indo American Journal of Pharmaceutical Research, 2014 ISSN NO: 2231-6876
IN-SITU OPHTHALMIC GEL OF TIMOLOL MALEATE: FORMULATION,
RHEOLOGICAL STUDIES, IN-VITRO AND IN-VIVOEVALUATION
Dhirajkumar Champalal Katariya, Poddar S. S K. M. Kundnani College of Pharmacy, Mumbai.
Corresponding author
Katariya Dhiraj
Ap. Walaki, Tal: daund.
Dist pune pin:412207.
Copy right © 2014 This is an Open Access article distributed under the terms of the Indo American journal of Pharmaceutical
Research, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
ARTICLE INFO ABSTRACT
Article history
Received 12/10/2014
Available online
30/11/2014
Keywords
In-Situ Gel,
Gellan Gum,
Ophthalmic Drug Delivery
System,
Ophthalmic Formulations.
The purpose of this study was to develop and characterize a series of gellan gum based in-situ
gel forming solution of timolol maleate for its optimized application. The rheological
behavior, gelling capacity, in-vitro drug release profile, anti-glaucoma study on rabbits and its
mucoadhesive profile of gellan gum were evaluated. Gellan gum in-situ gel forming solution
in the concentration range 0.25 to 1% w/v were prepared and evaluated to find out the
optimum concentration of polymer to achieve formulation which would be liquid at non-
physiological condition and became semi-solid at physiological condition. The rheological
phenomenon showed shear thinning pseudoplastic behavior of gellan gum with timolol
maleate. The results showed that the gellan gum can be used as an in-situ gelling vehicle to
enhance the ocular bioavailability of timolol maleate.Through this work a meaningful
platform for in-situ gelling type ophthalmic drops has been recommended. With further
logistics, various API would be possible to be fitted in this. The suggestion has ample
potential for scale up.
Please cite this article in press as Dhirajkumar Ch. Katariya et al. In-situ ophthalmic gel of Timolol maleate: Formulation,
rheological studies, in-vitro and in-vivoevaluation. Indo American Journal of Pharm Research.2014:4(11).

www.iajpr.com
Pag
e51
66
Vol 4, Issue 11, 2014. Dhirajkumar Ch. Katariya et al. ISSN NO: 2231-6876
INTRODUCTION Due to the specific anatomic structure and hydrodynamism, many challenges are faced in the development of effective
ophthalmic dosage forms. Most ophthalmic drugs are administered topically in the form of eye drops. Simplicity of such formulations
is the main reason. However, rapid turnover of lacrimal fluid and existence of efficient drainage apparatus make the ophthalmic
solutions to get eliminated rapidly, which causes a short precorneal residence and limitation of transcorneal penetration. All these lead
to the concerned ocular bioavailability that is commonly less than 10%[1-3]. Moreover, nasolacrimal drainage is the major route to
enter the circulatory system for drugs that are applied through topical administration [3,4]. For potent drugs, the systemic exposure
through this drainage after administration can be sufficiently high to cause systemic toxicityIn order to enhance the ocular
bioavailability, many ophthalmic drugs are applied in high concentrations or with increased frequency of administration [5]. But these
enhance the possibility of causing both ocular and systemic side-effects[6,7]. Some retentive options, such as inserts and ointments
have been considered. These dosage forms have proven to be of long duration and able to substantially modify drug bioavailability
compared to their solution dosage form counterparts[8,9]. However, these dosages could present some disadvantages, such as
noncompliance including irritation and blurred vision. An ideal ophthalmic formulation should be one that: (1) can be delivered in a
drop form without causing blurred vision or irritation; (2) has a suitable strength to endure the lacrimal fluid dilution without rapid
precorneal elimination after administration; (3) has an improved retentionin precorneal area through ability such as mucoadhesion.
This would facilitate the reservoir effect in the cul-de-sac and increasing the bioavailability of the drug.
In-situ gel forming formulations undergo phase transition from liquid to gel upon exposure to physiological environments
available in the lacrimal fluid. These formulations are free flowing liquids at room temperature to allow easy & reproducible
administration into the eye followed by a phase transition to form gel in the eye that is capable of withstanding shear forces and
dilution in the cul-de-sac resulting into sustenance of drug release. Due to decrease in nasolacrimal drainage,frequent instillation of
drug is not required[4, 10].The principle advantage of this type of formulations is the possibility of administering accurate and
reproducible quantities, in contrast to already gelled formulations and promoting precorneal retention[11].
Gellan gum which is a high molecular mass, linear anionic heteropolysaccharide produced aerobically from the
bacteriumSphingomonas paucimobilis. The polymer backbone is comprised of a tetrasaccharide repeat unit of glucose, glucuronic
acid and rhamnose in the molar ratio 2:1:1. It has a characteristic property of cation-induced gelation. During gelation a double helix
of gellan chains is formed by complexation with cations[12, 13]. Timolol maleate is a beta 1 as well as beta 2 (non selective)
adrenergic receptor blocking agent. Beta blockers reduce intraocular pressure by reducing the rate of formation of aqueous humor by
blocking the beta adrenoreceptors in the ciliary body. Systemic absorption of anti-glaucoma drugs like a beta blocking agent may
cause the reported side effects. Increasing the ocular/systemic ratio of drug absorption may decrease this. It has been shownthat ocular
absorption of timolol maleate increases but systemic absorption decreases with an increase in viscosity of formulation. These effects
are dependent on the drug concentration and the viscosity of the carrier solution. Systemic absorption can decrease due to high
viscosity reducing the probability of reaching nasal mucosa by a viscous product compared to non-viscous solutions [14].
The purpose of current work was to develop agellan gum based ion sensitive in-situ gelling liquid formulation containing
timolol maleate which would recommended to be used for anti-glaucoma ophthalmic therapy providing a sustained effect, helping in
reduction of frequency of administration.
MATERIALS AND METHODS
Materials:
Timolol maleate was gifted by the FDC Pvt. Ltd, Mumbai, India. Low-acetylated Gellan gum was courtesy Sun Pharma,
Vadodara, India. Mannitol, Sodium chloride, Sodium bicarbonate, Calcium chloride, Benzalkonium chloride, Glucose and other
chemicals were of GR grade and were procured from local market. Water used was of Millipore quality. Timolol maleate ophthalmic
solution (Timolet® 0.5% Sterile Eye Drops, Sun Pharma, India) was purchased from market. Rabbits were procured from Yash Farm,
Pune after taking permission from Animal ethical committee (25/1999/CPCSEA 29.07.2003).
Formulation of in-situgelling ophthalmic drop:
The in-situ gelwas formulated using timolol maleate, in-situ gel forming polymer gellan gum, benzalkonium chloride
(preservative) and mannitol (Tonicity contributor). Required quantity of the polymer was dispersed in water and heated at 900 C for
20 min to dissolve. The gum solution was cooled to room temperature and the drug was incorporated to dissolve. Formulations
batches are shown in table 1. Optimised batch was sterilized by moist heat sterilization at 1210C for 20 min[15-17].
Table 1: Details of batches of in-situ gelling formulations.
Sr. No Ingredients Concentration (% w/w)
G1 G2 G3 G4 G5 G6
1. Timolol maleate (equivalent to 0.5%
w/w of Timolol in formulation)
0.68 0.68 0.68 0.68 0.68 0.68
2. Gellan gum 0.25 0.50 0.75 0.50 0.75 1.0
3. Benzalkonium chloride 0.01 0.01 0.01 0.01 0.01 0.01
4. Mannitol* q.s. q.s. q.s. q.s. q.s. q.s.
5. Water q.s. q.s. q.s. q.s. q.s. q.s.
*: q.s. to produce310- 350 mOsm/L[18-29] (using Cryoscopic osmometer Osmomat 030, Gonotec, Germany).
Sterilization No No No Yes Yes Yes

www.iajpr.com
Pag
e51
67
Vol 4, Issue 11, 2014. Dhirajkumar Ch. Katariya et al. ISSN NO: 2231-6876
Drug-Polymer interaction:
This study was performed through IR spectrophotometry and DSC which involved assessing the pure drug alone and in
combination with the excipients.For IR spectroscopy,sample was mixed with KBr in the proportion of 1:100. Sample cell was placed
in IR beam and scanned using Shimadzu IR spectrophotometer (AFFINITY-1, Toshvin Analytical, Japan). The resultant graphs were
analyzed for absorption bands. DSC studies were performed using Mettler ToledoDSC instrument (DSC 821, Switzerland.).About 3-5
mg sample was weighed and placed in an aluminium pan with lid, crimp sealed and heated from 30° C to 300° C at a rate of 10° C
/min. After completion of run time the procured graph was analyzed for endothermic peak temperatures[21, 22].
Rheology:
Gelation:Gelation is the primary requirement which is to be satisfied by the formulation. This study was performed in two
ways. Firstly, a drop of formulation was added to 2 mL of Simulated tear fluid (STF) (composition is given in table 2) freshly
prepared and equilibrated at 340 C in a watch glass to visually assess the gel formation with its retention. Secondly, by mixing the
formulation with the STF andwater separately in the proportion of 25:7 [23] to study the ability of the formulation to resist the change
of original viscosity and to study the rheologicalbehaviors post instillation.Brookfield rheometer (DV-III+, U.S.A.) in association of
spindle no 21 was employed to understand this. Sample was placed in the small volume adapter and shear stress was applied by the
spindle rotating at different rpm[15, 24, 25]. The ratio 25:7 was selected because one drop of formulation generally equates to 25-30
μL and the volume of tear fluid available in the cul-de-sac would be 7 μL. Though water would not be encountered by the product any
time, still it was included to have comparison with STF.
Table 2: Composition of STF[25].
Sr. No Ingredients Concentration (%w/w)
1. NaCl 0.67
2. NaHCO3 0.20
3. CaCl2 . 2H2O 0.008
4. H2O q.s
Viscosity:Viscosity of the formulation governs the behavior of the formulation in the cul-de-sac resisting against the
hydrodynamism and the blinking of the eye. Viscosity of the formulations was measured by employing the Brookfield Rheometer
using spindle no. 21 at three different conditions viz. only formulation (effect of non-physiological condition), formulation mixed with
STF in the ratio of 25:7 (effect of physiological condition) and formulation mixed with water in the ratio of 25:7 (effect of dilution
without ion activation).
Rheology:This class of study was performed to confirm the rheological behavior because it helps in deciding the behavior of
the formulation in the cul-de-sac; the same was followedby measuring shear stress of the formulation at various shear rates. A typical
run comprised of increasing the shear rate from 0-50 S-1 at controlled ramp speed, a 0.1 min wait at the highest i.e. 50 S-1 and finally
a decrease in shear rate back to 0 S-1 at the same controlled ramp speed[26].
Morphology:
This was done through scanning electron microscopy (SEM) characterization. The gelling ability and the gelled status of the
optimised formulation were proposed to be studied through the surface morphology of the formulation at liquid state (non-
physiological condition) and at gel state (physiological condition) by using SEM (JEOL JSM 6380LA, Japan)[27]. Sample was
mounted on double adhesive tape and dried in vacuum drier for 48 hrs. Then it was mounted on specimen stub. The mount was coated
with platinum. Imaging of the sample was performed applying voltage 5-20 kV under vacuum (10-4 Pascal).
Mucoadhesion:
The mucoadhesive force is an important physicochemical parameter for prolonging ocular retention time and thereby
ensuring better therapeutic effect. Mucoadhesive study was performed for the gellan gum in-situ gel on Universal Testing machine
(LS1, Lloyd Instruments Limited, UK) using Nexygen plus 3 software. This method determines the maximum force and work needed
to separate two surfaces in intimate contact. Goat eye was procured from slaughter house. Cornea was separated and washed carefully
with water. Tissue was fixed on the prob of diameter 25 mm and on a basement probe with mucosal sides facing towards each
other.Before start of experiment corneal membrane was dipped in the STF. Drop of formulation to be tested at physiological condition
then spread evenly on to the surface of the corneal membrane of basement probe. After that, the two corneal surfaces were kept in
contact separated by the product in between for two minutes by applying a pre-load of 10 N. Then the probewas raised at a speed of
0.5 mm/sec. The force and the work necessary to detach the gel from the surface of the mucous layer of the cornea were measured as
force versusdisplacement curves. Mucoadhesive strength was then derived from the plot as the maximum value expressed in
grams[28-32].
Drug content:
Formulation measuring 1 mL was diluted with distilled water to correspondtimolol maleate concentration 20μg/mL. This was
analyzed employing UV spectrophotometer (Jasco, V-550, Thermo Electron Corporation, Germany) at λmaxof 294 nm. The
concentration of sampleswas determined from a previouslyprepared calibration curve. The study was performed in triplicate.

www.iajpr.com
Pag
e51
68
Vol 4, Issue 11, 2014. Dhirajkumar Ch. Katariya et al. ISSN NO: 2231-6876
Drug release:
In case of solution formulation, the drug is immediately available for transport to the anterior chamber but hydrodynamic
behavior and tear output of the eye wash off the maximum amount through overflow and nasolacrimal drainage. The slow release of
the drug through a formulation would be able to reducethe nasolacrimal drainage. To confirm this it was necessary to study the
release, which would be diffusion behavior in the present case.Franz diffusion cell was employed for this. The recipient compartment
of the diffusion cell was filled with STF (18mL) which was stirred continuously using magnetic stirrer at 50 rpm. A pretreated (soaked
for 24 hrs in STF) dialysis membrane (DM001, Hi Media regenerated seamless cellulose, molecular cut off 12,000-14,000 D, India) of
appropriate diameter was mounted carefully on the rim of the recipient compartment. A sample of 2 mL of an ophthalmic solution
(marketed preparation) and the in-situ gel forming formulation at physiological condition were tested separately. The diffusion cell
assembly was connected to water bath to maintain the temperature of the STF at 34±2° C. Aliquots, 1 mL in volume were withdrawn
carefully from the side arm of the diffusion cell and were replaced immediately with the same volume of fresh STF. The samples were
diluted suitably and the content of timolol maleate in each was estimated using the UV spectrophometer at 294nm [15].
Ocular tolerance:
An irritant product may induceexcessive lacrimation and as well as blinking, which would decide the stay of a product in the
cul-de-sac. Thus, as a formulator it is a need to judge an ocular tolerance of a formulation for its better application. Qualitative as well
as quantitative assessment of ocular tolerance was studied following a single application of 25 μL of the formulated product to one eye
in three adult male New Zealand albino rabbits weighing2.0-2.5 kg. The animals were housed singly under standard conditions, which
included 12 hr dark / 12 hr bright cycle, 20-210 C temperature and 40-70% relative humidity having free access to water and standard
laboratory feed. During the experiment and for 1 hr afterwards, the animals were placed in restraining boxes and allowed to move
their heads freely. The eye movements were not restricted. Formulation 25 μL was instilledinto the lower cul-de-sac of the eyes of
three rabbits, using a micropipette. To prevent loss of instilled solution, the eyelids were gently held together for about 10 s. The
clinical observations and ocular reactions were scored by visually assessing the following conditions viz, redness, conjunctival
chemosis, discharge, iris and corneal lesionsat 1, 24, 48, 72, 96 hrs and 7 days after application.The study was done in a stepped
manner. Initially the study was done on one rabbit. On confirmation of non-irritancy the study was stepped up to the remaining two
animals[25, 33].
Anti-glaucoma activity:
A good formulation would be expected to control the intraocular pressure for a prolonged time upgrading the therapy and
patient compliance. Rabbits weighing 2.0-2.5 kg were used for the study. The basal intra ocular pressure (IOP) was measured using a
Schiotz tonometer (KN 30, KASHSURG, India). The formulations were instilled into the left eye while right eye received
onlywaterwhich served as a control. After 30 min of drug administration, the IOP was measured. Glucose solution (5% w/v) was
administered intravenously through the marginal ear vein at a dose of 15 mL/kg body weight to induce glaucoma.After this IOP
recording was carried out every 30 min for 360 min in both eyes [34-37].
A washout period of 5 days was allowed before reusing the same animal in the study. Change in IOP (ΔIOP) was expressed
as follows: ΔIOP = IOPcontrol eye ─ IOPtreatment eye.The efficiency of theformulations was estimated by the time required to
achieve peak ΔIOP (Tmax), the peak ΔIOP (ΔIOPmax), and the area under the ΔIOP-time-curve (AUC 0→6 h) after administration of
the respective formulation [12]. The AUC values were calculated by multiplying the time interval with mean ΔIOP for individual
observations and finally adding all together[26].
Results are expressed as mean ± standard error mean. All results were analyzed statistically using pair t-test. Values ofp <
0.05 were considered statistically significant[26].
RESULTS AND DISCUSSION:
Selection of formulation ingredients:
The two main rheological prerequisites of an in-situ gelling ophthalmic drops are viscosity and gelling capacity[38]. The
formulation should have an optimum viscosity that would allow easy instillation into the eye as a liquid which would undergo a rapid
sol-to-gel transformation triggered by the presence of mono and di valent cation in the tear fluid. Additionally, the gel formed in-situ
should sufficiently preserve its integrity resulting into reduced dissolution or erosion for a prolonged period of time. Deacetylated
polysaccharide forms stiff, brittle gels. The deacetylated material has good thermal stability[39, 40]. Its aqueous solutions are very
viscous, thixotropic and can form gels at concentrations as low as 0.04 % [40]. The shear modulus of gels of gellan gum is sensitive to
the type and concentration of cation [41]. High acetyl gellan gels are very weak mechanically because the bulky acetyl and glyceryl
groups prevent close association between gellan polymer chains in a double-helix formation and hinder compact packing of the cross-
linked double helix[42, 43]. Low-acetyl gellan gum forms clear gels in the presence of mono and divalent cations[44, 45]. Hence it
was decided to go for low-acetyl gellan gum further.In the preliminary study gellan gum system below 0.25% w/v, did not show
optimum gelation at physiological condition for its in-situ gel behavior, whereas formulation containing 0.75 % w/v of the polymer at
the non-physiological condition failed to form drop only. Hence, 0.25-0.75 % w/v range would be included for the further study to
achieve the two main rheological prerequisite. With the desirable rheological characteristic the formulation should have the required
osmolality was 310-350mOsm/L for which mannitol was used using Cryoscopic osmometer (Osmomat 030, Gonotec, Germany)
(shown in Table 3). Benzalkonium chloride was incorporated to preserve the formulation against the microbial damage.

www.iajpr.com
Pag
e51
69
Vol 4, Issue 11, 2014. Dhirajkumar Ch. Katariya et al. ISSN NO: 2231-6876
Table 3: Required mannitol concentration to achieve desired osmolality values.
Sr.
No
Formulation Osmolality
without mannitol
(mOsm/kg)
Mannitol Concentration
(%w/v) to achieve
desired osmolality
1. Timolol maleate (0.68% w/v) 31 4.6
2. 0.25% gellan gum 36 4.6
3. 0.5% unsterilized 38 4.3
4. 0.5% sterilised 36 4.3
5. 0.75% unsterilized 39 4.3
6. 0.75% sterilised 42 4.3
Drug polymer interaction:
The spectral results of interaction study are shown in Figs 1-3. The IR spectrum of timolol maleate (Fig 1) showed absorption
bands for hydroxyl group (3286 cm-1), NH group (3045 cm-1), C=N stretch (1703 cm-1) and C-O-C stretch (1120cm-1). The IR
spectrum of Gellan gum (Fig 2) exhibited characteristic absorption bands for hydroxyl group (3545 cm-1), carboxylic group (1668
cm-1) and unsaturation (1600 cm-1). Lastly, the IR spectrum of drug with polymer (Fig 3) showed absorption bands for hydroxyl
group (3284, 3543 cm-1), carboxylic group (1668 cm-1), unsaturation (1587 cm-1), NH group (3047 cm-1), C=N (1697 cm-1), C-O
(1201 cm-1) and C-O-C (1120 cm-1). The absence of theadditional peaks which also confirmed that opening of the ringdid not take
place. No interference observed among the absorption bands thus, there was nointeraction of the polymerwith thedrug. Fig 4-6 shows
the DSC spectra for drug, polymer and the physical mixture. In DSC spectrathe melting endothermic peaks of drug in pure form (Fig
4) and its physical mixture (Fig 6) with the in-situ gelling polymer are recorded.The spectra exhibited characteristic melting peak of
the drug.In the mixture of the drug polymer there was no shift in endothermic melting peakof the drug indicating absenceof significant
interaction amongst formulation ingredients. Hence from IR and DSC it could be concluded that timolol maleate had not reacted with
the polymer used in the formulation.
2505007501000125015001750200025003000350040004500
1/cm
-0
25
50
75
100
%T
32
86
.70
30
45
.60
28
54
.65
27
60
.14
17
03
.14
13
84
.89
13
54
.03
12
94
.24
12
63
.37
12
30
.58
12
01
.65
11
20
.64
10
55
.06
10
10
.70
98
9.4
8
35
8.7
6
35
1.0
4
Fig 1: IR spectra of Timolol maleate.
500750100012501500175020002500300035004000
1/cm
75
80
85
90
95
100
%T
35
99
.17
35
45
.16
33
09
.85
32
75
.13
32
42
.34
32
13
.41
16
64
.57
16
00
.92
15
79
.70
13
69
.46
13
38
.60
12
88
.45
12
71
.09
12
44
.09
12
26
.73
11
99
.72
11
36
.07
11
20
.64
10
80
.14
10
31
.92
10
10
.70
99
7.2
0 93
9.3
39
25
.83
88
7.2
68
37
.11
81
0.1
08
00
.46
77
3.4
66
71
.23
64
8.0
86
21
.08
54
5.8
55
18
.85
50
1.4
9
Fig 2: IR spectra of Gellan gum.

www.iajpr.com
Pag
e51
70
Vol 4, Issue 11, 2014. Dhirajkumar Ch. Katariya et al. ISSN NO: 2231-6876
500750100012501500175020002500300035004000
1/cm
60
70
80
90
100
%T
35
43
.23
32
84
.77
30
39
.81
30
32
.10
29
81
.95
29
66
.52
28
43
.07
17
03
.14
16
68
.43
15
87
.42
15
83
.56
15
35
.34
15
00
.62
14
50
.47 1
37
9.1
01
35
5.9
61
34
0.5
31
31
1.5
91
29
4.2
41
26
3.3
7
12
30
.58
12
01
.65
11
20
.64
10
56
.99
10
26
.13
10
10
.70
98
9.4
89
56
.69
89
1.1
1
86
4.1
1 76
9.6
0 74
8.3
8
65
1.9
46
19
.15
58
0.5
75
69
.00
53
6.2
15
18
.85
50
1.4
9
Fig 3: IR spectra of Timolol maleate with Gellan gum.
Fig 4: DSC spectra of timolol maleate.
Fig 5: DSC spectra of gellan gum.
Fig 6: DSC spectra of the physical mixture of timolol maleate with gellan gum.

www.iajpr.com
Pag
e51
71
Vol 4, Issue 11, 2014. Dhirajkumar Ch. Katariya et al. ISSN NO: 2231-6876
Influence of sterilization:
In preliminary study Batch G2 was found to be optimum for the in-situ gel formulation. Since the formulation was proposed
for ophthalmic use, assurance of sterility of the finished product was of concern. During manufacturing, ophthalmic solutions need to
be processed to ensure sterility of the finished products. It can be made by using recommended methods like sterilization by filtration
or autoclaving (steam sterilization) [46]. Although autoclaving is the first choice for most of the products because of its convenience
and assurance in large-scale production it might have thermal degradation related issues. Nevertheless steam sterilization was used in
the current work to assess the feasibility. Batch G4 (sterilised formulation containing 0.5% gellan gum) after sterilization showed
viscosity drop from 250 cP to 65 cP. Since 65 cP would be unacceptable it was decided to go for sterilization of 0.75% gellan gum
(before sterilization too viscous to drop). Batch G6 did not form drops for instillation. Hence, batch G5 was considered optimum for
further study. In case of Batch G5, as seen in table 4, viscosity drop was found to be from 1130 to 210 cP at 5 rpm spindle speed. For
this batch, viscosity at non-physiological condition was 210 cP and at physiological condition 200 cP, whereas after dilution with
water the viscosity dropped to 90 cP. Shear stress value for G5 at physiological condition (i.e dilution with the STF) was 2.1 times
more than shear stress after dilution of formulation with water. The mucoadhesive strength for G3 batch was found to be 8.89 gm. For
G5, mucoadhesive strength drops to 6.6 gm. The thermal effect encountered during moist heat sterilization had an effect on the
viscosity and mucoadhesive strength. But this could be compensated by making suitable changes in formulation. Batch G2 & G5
appeared to be having desirable properties.
Gelation:
Results of transparency, gelling capacity & dilution effect are shown in Table 4. All the formulations were found to be
transparent. Except G1, all formulations under study showed desirable behavior as far as gel formation and its retention was
concerned. In case of dilution effect study all the formulations showed viscosity gain in the range of 2 to 13 times. An optimized
formulation should exhibit immediate gel formation after addition to the STF which is expected to retain its nature for extended period
of time. The same was demonstrated by formulation G2 to G5.
Table 4: Properties of the formulations.
Sr. No Formulation Transparency a Gelling capacity b Dilution effect
(viscosity gain) c
1. G1 + ++ 13X
2. G2 + +++ 03X
3. G3 + +++ 02X
4. G4 + +++ 3.2X
5. G5 + +++ 2.2X
a: All samples were evaluated at physiological condition (340C, pH 7.4 and dilution by STF), +: transparent, ++: translucent, +++:
turbid.
b: +: gels after a few minutes, dissolves within 1-2 hrs, ++: gelation immediate, remains for 3-4 hrs, +++: gelation immediate,
remains for more than 6 hrs.
c: This was performed to understand the component of resistance shown by the formulation towards dilution effect, this value is in
terms of viscosity gain after mixing with STF in comparison to that with water in the ratio of 25:7 (viscosity at 5 rpm was
considered) (refer to Table. 4).
Rheology:
As indicated in Table 5 and Fig 7a – 7e, with increasing concentration of polymer at liquid state it was observed that
viscosity increased correspondingly. In table 5 the Viscosity and Shear stress are expressed as centipoises (cP) and Dyne per
centimeter square (D/cm2) respectively.For comparison, in the following discussion the viscosity and shear stress values are
considered at the 5 rpm spindle speed. Ophthalmic agitation is rhythmic and pulsatile. May be 5 rpm for ½ sec followed bystagnancy
for 5sec.This was attempted to be matched in-vitro by selecting 5 rpm continuous agitation. Batches G1, G2, G3, G4 and G5 showed
viscosity 25.7, 250, 1130, 65 and 210 cP respectively whichwas at non-physiological condition. At physiological condition that isby
adding formulation into the STF in the ratio of 25:7 [23]batches G1, G2, G3, G4 and G5 showed viscosities as 65, 380, 950, 80 and
200 cP respectively. After instillation of any formulation, generally it tends to loose its viscosity because of dilution by tear fluid
which would further clear up by the nasolacrimal drainage. Whereas in-situ gel formulations maintained viscosity to its original value
irrespective of dilution. This actually can be said to be rise in viscosity because the total volume was increased after dilution.To
understand the same that is at what extent the formulation showedresistance against viscosity fall could be understood by diluting the
formulation with water (instead of STF) in the proportion of 25:7. After water dilution the viscosity was found to be 5, 120, 570, 25
and 90 cP respectively for batches G1, G2, G3, G4 and G5. This indicated that the formulations resisted the fall in viscosity after
instillation in to the condition simulating cul-de-sac. This would give the sustained release effect of the formulation. Dilution with
STF showedthat there was increase in shear stress values 7.9, 3.4, 1.8, 3.2 and 2.2 times for batches G1, G2, G3, G4 and G5
respectively in comparison with water dilution.
The ideal in-situ gel formulation is known for its capacity or the extent to which it shows the resistance against viscosity drop
because of tear fluid after instillation. This behavior ultimately gives strength to the formulation against the hydrodynamism of the
eye. Dilution studies have given precisely the idea of the formulation for its extent of resistance against dilution. The comparison of
viscosity of the formulation after its dilution with STF (condition simulating cul-de-sac) and water (control situation, simulating the

www.iajpr.com
Pag
e51
72
Vol 4, Issue 11, 2014. Dhirajkumar Ch. Katariya et al. ISSN NO: 2231-6876
absence of polymer activation). Batch G1, G2, G3, G4 and G5 showed resistance against dilution on comparing STF and water
dilution of formulation as 13, 3, 2, 3.2 and 2.2 times. Batch G1 showed the maximum resistance against the viscosity fall. From the
dilution study it could be noted that, as the concentration of the polymer increased its resistance against viscosity fall decreased. To
optimize the batch the two parameters were considered viz, capacity of the formulation to show resistance against the viscosity fall
due to dilution as well as resultant viscosity. G1 was best for its capacity of resistance against viscosity fall. In the context, viscosity, it
was important to understand where formulation could show maximum resistance against hydrodynamic drag and blinking, at the same
time should have been droppable. Rise in viscosity or its maintenance after instillation, both the phenomena would be supporting the
requirement depending on the viscosity value that would come after instillation. Whether rise in viscosity after instillation or
maintenance of viscosity after instillation, higher the ultimate viscosity better would be retention against the hydrodynamic drag and
blinking. Therefore, looking at both viscosity and the resistance against viscosity fall upon instillation, G5 was found to be optimum.
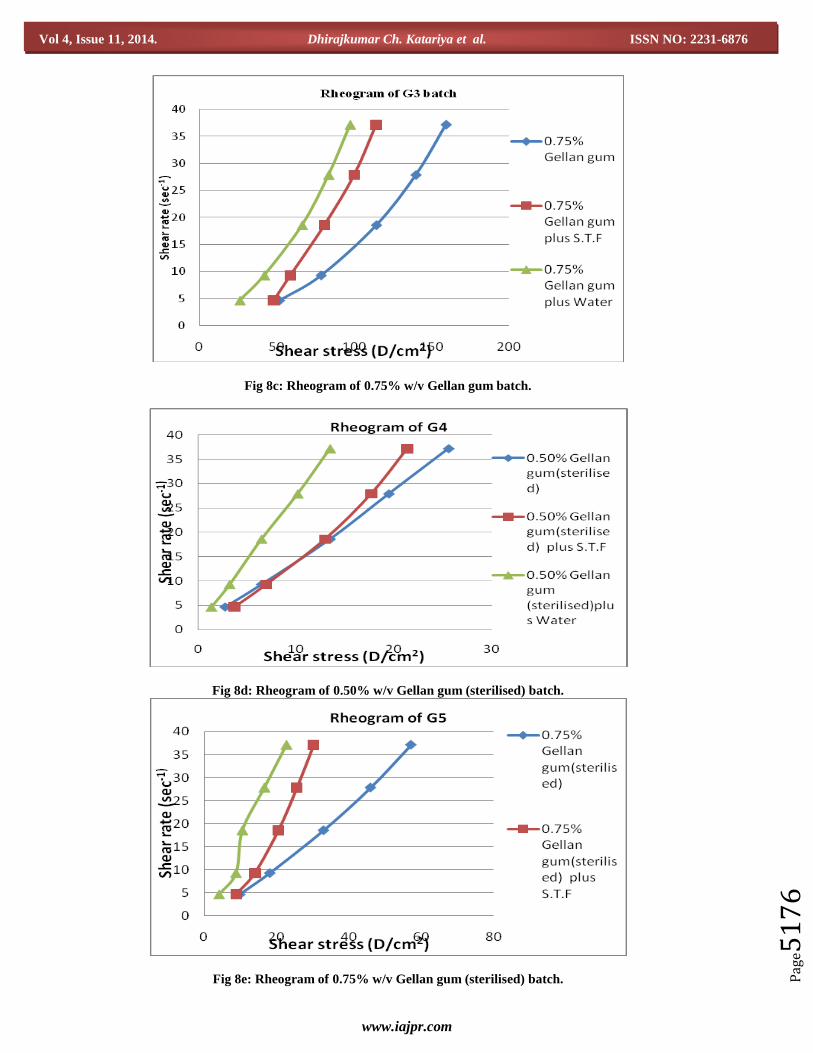
All gellan gum formulations, whether in the state of sol or in gel, showed pseudo plastic behavior.The viscosity of the gels increased
with increasing concentrations of gellan gum, and a significant change in viscosity was found when gellan gum underwent sol–gel
transition at relatively lower concentrations (G1 and G2 batch). Due to anexcessively viscous solution obtained with G3 (75%) gellan
gum, a slight viscosity drop was observed after addition of STF (which was much less than that of dilution with water). The observed
drop in viscosity at condition simulating cul-de-sac has been noted previously for gellan gum and is attributed to a consequence of
increasing chain interaction with rise in polymer concentration[47]. When shear is applied through blinking action of eye on in-situ
gels, the particle contacts begin to break down, the particles become aligned and the flow starts. On being exposed to shearing force,
the gel tends to lose its viscosity[16]followed by restoration to the same when the stress is removed. With the increase in concentration
of polymer, the number of interactions between polymer chain increases leading to a three dimensional network structure and hence,
exhibition of non- Newtonian flow. Despite the shearing force on the preparation being largelyeffective during blinking, if the
viscosity is too high, it may not thin down enough and in addition may induce discomfort and irritation [38]. On the other hand, if that
is too low, it will give rise to increased drainage. The pseudoplastic property of these formulations is in favor of slowed drainage of
drug from the cul-de-sac of the eye, simultaneously facilitating difficult free blinking[38, 48]. The most satisfactory representation for
a pseudoplastic material however is probably a graphic plot of the entire consistency curve. The consistency curve[49] for
pseudoplastic material showed a beginningapproaching origin (or at least approaches it) at low rates of shear. Absence of yield value
and linearity was noted in Fig8a-8e. Viscosity of pseudoplastic substances decreases with increase in the rate of shear.The curved
nature of the rheogram might be explained through the very polymeric nature of the gellan gum. This gum consists of long chain
linear polymers. Such materials are known to beproducing the mentioned curvature. As shearing stress is increased, normally
disarranged molecules begin to align their long axes in the direction of flow. This orientation reduces the internal resistance of the
material and allows a greater rate of shear at each successive shearing stress. In addition some of the solvent associated with the
molecules may be released, resulting in an effective lowering of both the apparent concentration and size of the dispersed molecules.
This, too, is known to decrease apparent viscosity. It was seen that as the shear rate was reduced and once a level of maximum had
been reached, the down curve for non-Newtonian systems was displaced relative to the up-curve (Fig 9). With the shear thinning
systems (i.e. pseudoplastic), the down- curve is frequently displaced to the left of the up-curve. The same was seen for the G5 batch.
Viscoelastic fluids with a viscosity that is high under low shear rate and low under high shear rate conditions that is pseudoplastic
would be preferred for ophthalmic drug delivery. The same was noted with the gellan gum batches as shown in Fig 8a-8e. In the
present case, gellan gum chains are localized with a certainintermolecular distance imparting particular viscosity to the formulation.
Ordinarily, after dilution formulations are likely to show fall in viscosity due to increase in distance between the polymer chains. But
in case of ophthalmic application of gellan gum, after instillation of formulation, polymer chains nullified the effect of dilution.
Explanation for this might be in the involvement of formation of double helical gellan chains by the complexation with mono and di
valent cations[38, 50, 51]and with it there might be enforcement due to formation of hydrogen bonding with water by the gellan
chains. These formed double helical gellan chains aggregate to result in to a 3D network[38, 52-54]. Formulation of such structure
took care to nullify the dilution effect by maintaining viscosity whichinfact meantactual rise in viscosity as there was increase in the
totalvolume. As the concentration of gellangum increased, the polymer chains approached closer arrangement and the number of
interactions between polymer chains increased leading to more dense three-dimensional network structure[16, 55].
Formulation at non-physiological condition was in liquid state which would help in easy product handling during production,
packaging and administration. Also product at liquid form would drop properlyresulting into reliable dose administration while
administration. After this, because of its particular nature,product would show resistance to the viscosity drop. The same behavior of
formulation would suit the ophthalmic condition like hydrodynamism&blinking. From rheological behavior it was concluded that
optimised formulation could assure its enhanced retention in the cul-de-sac against hydrodynamism and blinking of the eye.

www.iajpr.com
Pag
e51
73
Vol 4, Issue 11, 2014. Dhirajkumar Ch. Katariya et al. ISSN NO: 2231-6876
Table 5: Viscosity and rheological study.
Sr. No Batch Spindle speed (rpm)
5 10 20 30 40
1. Batch G1
(0.25%)
Viscosity (cP) 25.7 30 32.5 32.5 31.5
Shear stress (D/cm2) 0.93 2.79 5.58 8.84 12.1
2. Batch G1 : S.T.F (25:7)
(0.25%)
Viscosity (cP) 65 67.5 60 55 51.3
Shear stress (D/cm2) 3.26 6.05 11.2 15.3 19.1
3. Batch G1 : Water (25:7)
(0.25%)
Viscosity (cP) 5 10 13.7 16.7 16.3
Shear stress (D/cm2) 0.41 0.93 2.79 4.65 6.05
4. Batch G2
(0.5%)
Viscosity (cP) 250 230 200 176.7 161.2
Shear stress (D/cm2) 11 21.9 37.2 49.3 60
5. Batch G2 : S.T.F (25:7)
(0.5%)
Viscosity (cP) 380 285 215 173.3 150
Shear stress (D/cm2) 17.7 26.5 40 48.4 55.8
6. Batch G2 : Water (25:7)
(0.5%)
Viscosity (cP) 120 117.5 108.5 100 93.8
Shear stress (D/cm2) 5.12 11.2 20 28.4 34.9
7. Batch G3
(0.75%)
Viscosity (cP) 1130 847.5 617.5 501.7 428.7
Shear stress (D/cm2) 51.6 78.6 114.4 140 159.5
8. Batch G3 : S.T.F (25:7)
(0.75%)
Viscosity (cP) 950 635 380 296 240
Shear stress (D/cm2) 47.8 58.6 80.7 100 114.2
9. Batch G3 : Water (25:7)
(0.75%)
Viscosity (cP) 570 455 357.5 290.3 234
Shear stress (D/cm2) 26 41.9 66.5 83.7 97.7
10. Batch G4
(0.5% sterilised)
Viscosity (cP) 65 70 72.5 70 68.8
Shear stress (D/cm2) 2.79 6.51 13.5 19.5 25.6
11. Batch G4 : STF
(25:7)
(0.5% sterilised)
Viscosity (cP) 80 75 70 63.3 58.7
Shear stress (D/cm2) 3.72 6.98 13 17.7 21.4
12. Batch G4 : Water
(25:7)
(0.5% sterilised)
Viscosity (cP) 25 32.5 36.2 36.7 36.3
Shear stress (D/cm2) 1.4 3.26 6.51 10.2 13.5
13. Batch G5
(0.75% sterilised)
Viscosity (cP) 210 195 177.8 165 155
Shear stress (D/cm2) 9.76 18.1 33.0 46 57.2
14. Batch G5 : S.T.F (25:7)
(0.75% sterilised)
Viscosity (cP) 200 147.5 110 93.3 81.3
Shear stress (D/cm2) 8.84 14 20.5 25.6 30.2
15. Batch G5 : Water (25:7)
(0.75% sterilised)
Viscosity (cP) 90 80 70 61.3 59.0
Shear stress (D/cm2) 4.18 8.84 10.6 16.7 22.8
Fig 7 a: Effect of shear rate on viscosity.

www.iajpr.com
Pag
e51
74
Vol 4, Issue 11, 2014. Dhirajkumar Ch. Katariya et al. ISSN NO: 2231-6876
Fig 7 b: Effect of shear rate on viscosity.
Fig 7 c: Effect of shear rate on viscosity.
Fig 7d d: Effect of shear rate on viscosity.

www.iajpr.com
Pag
e51
75
Vol 4, Issue 11, 2014. Dhirajkumar Ch. Katariya et al. ISSN NO: 2231-6876
Fig 7 e: Effect of shear rate on viscosity.
Fig 8a: Rheogram of 0.25% w/v Gellan gum batch.
Fig 8b: Rheogram of 0.50% w/v Gellan gum batch.
www.iajpr.com
Pag
e51
76
Vol 4, Issue 11, 2014. Dhirajkumar Ch. Katariya et al. ISSN NO: 2231-6876
Fig 8c: Rheogram of 0.75% w/v Gellan gum batch.
Fig 8d: Rheogram of 0.50% w/v Gellan gum (sterilised) batch.
Fig 8e: Rheogram of 0.75% w/v Gellan gum (sterilised) batch.

www.iajpr.com
Pag
e51
77
Vol 4, Issue 11, 2014. Dhirajkumar Ch. Katariya et al. ISSN NO: 2231-6876
Fig 9: Thixotropic curve of optimised formulation.
Timolol maleate content:
Estimation of drug content in ophthalmic solutions was carried out using UV spectrophotometer. The content of drug in the
selected systems was found to be 97.2-100.6 % w/v. Referring to the United States Pharmacopoeia which though does not have in-situ
gelling formulations, gives the limit for drug content in timolol maleate ophthalmic drops as NLT 90.0% and NMT 110.0%, the
formulated products satisfied this.
In-vitro release:
The in-vitro drug release profiles are shown in Fig 10it was seen that marketed timolol maleate formulation showed 40%
drug release at the end of 6 hrs. The optimised formulation showed only 17.38% drug release for 6 hrs. Optimised ophthalmic
formulations at ophthalmic condition showed 2.3 times reduced drug release in comparison to marketed solution formulation of
timolol maleate. It meant that in-situ gel formulation showedextended release of the timolol maleate. From this release, it could be
suggested that there was formation of 3D network of gellan chains, which reduces the drug release from the formed network. This was
the reason for reduced availability of the drug for the release, from the polymer network and also for the precorneal elimination. This
reduce availability of drug in the cul-de-sac may cause reduced bioavailability also. The same thing is ruled out (results are included in
coming sections) and it was seen that formulation behavior was very beneficial for the optimised application of the timolol maleate
from in-situ gel formulation.
In order to investigate drug release mechanism, the release data were fitted to models representing first order, Higuchi and
Ritger–Peppas equation. The linear regression analyses were summarized in Table 6. The examination of coefficient of determination
(r2) values for the optimised formulation was obtained by the use of KinetDS3 software indicated that Ritger–Peppas equation was a
more suitable fit to drug release mechanism from in-situ gelling system. Ritger-Peppas equation: F = KTn . F is the fractional release
of the drug; K is the proportionality constant; n is the diffusional exponent and T is the time. The diffusional exponent was calculated
from the slope of the natural logarithmic values (ln) of the fractional release as a function of time (Table 6). The release mechanism
for semisolid vehicles containing dissolved drug was found to be non-fickian involving both diffusion and polymer relaxation (0.5 < n
< 1). The data of release mechanism indicated that timolol maleate release was dependent on two simultaneous processes: water
migration into the in situ gelling system and drug diffusion through continuously swelling gelling system. Similar result was also
obtained by other researchers in other gelling system[56, 57].

www.iajpr.com
Pag
e51
78
Vol 4, Issue 11, 2014. Dhirajkumar Ch. Katariya et al. ISSN NO: 2231-6876
Fig 10: Release profiles of optimised in-situ gel formulation and marketed solution formulation of timolol maleate.
Table 6: In-vitro release kinetic of timolol maleate from in-situ gel system.
Formulation First order
r2
Higuchi
r2
Ritger- Peppas
r2 n
Optimised formulation 0.2744 -0.8076 0.975 0.708
Morphological Analysis:
As may be noted from Fig 11 and 12, shows the SEM image of optimised formulation at non-physiological condition
indicating loose morphology or arrangement of the polymer chains at Х 1500 magnification whereas, at physiological condition
demonstrating compact morphological structure even at higher magnification at Х 5000 magnification which was even higher
magnification than that of previous image, which signifies is most probably due to formation of double helical gellan chain aggregates
as a result of formation of 3D network. The observation also supported that formulation nullifies the dilution effect which would be
concern after administration in to the cul-de-sac, there by forming compact structure. The SEM equipment demanded the scanning of
dry sample. The samples were dries in vacuum before Pt coating. Thus, the samples might have had the probability of getting
distorted. As may be noted, in spite of such condition, change was noted in non physiological & physiological representations. As
compared to Fig 9, Fig 10 was required be done at higher magnification to demonstrate the finer striated conformation. The
compactness & change from larger entities to finer could be connected to the process of the particular gelling.
Fig 11: SEM image of optimised batch at non-physiological condition.

www.iajpr.com
Pag
e51
79
Vol 4, Issue 11, 2014. Dhirajkumar Ch. Katariya et al. ISSN NO: 2231-6876
Fig 12: SEM image of optimised formulation at physiological condition.
Mucoadhesion analysis:
The results of mucoadhesive studies are given in table 7. It was noted that, mucoadhsion was found to be increasing with
increase in concentration of gellan gum. From fig 13 it was seen that G5batch’s mucoadhsion was found to be corresponding to 6.60
g. There is speculation that bioadhesion is the net effect of many physicochemical factors that include attractive forces such as
hydrophobic interactions, hydrogen bonding and van der Waals attraction; physical entanglement of polymer chains via diffusional
processes and electrostatic interaction of an attractive or repulsive nature all contribute to the bioadhesive process. It appears that the
inherent rheological properties of ophthalmic gels may also have a decisive role to play with respect to improved residence on the eye
[58]. The mucoadhesive force is an important physicochemical parameter for prolonging ocular retention time and there by better
therapeutic effects[59]. This is probably due to the better rheological gel characteristics. Usually systems with higher elastic
components possess a greater mucoadhesion [28]. Thus, in the present case formulations showed optimum mucoadhesion which
further reflects the optimum rheological behavior.
Table 7: Mucoadhesive results for different gellan gum in-situ ophthalmic gel batches.
Sr. No Formulation Mucoadhesive force (g)
1. G1 1.54
2. G2 3.56
3. G3 8.89
4. G5 6.60
5. G6 11.48
Load (gf)
0.0
5.0
10.0
Machine Extension (mm)0 10 20 30 40
Maximum Load: 6.60 gfSAMPLE ID: formltn 0.75% autoclaved
Fig 13: Mucoadhesion graph for optimised in-situ ophthalmic gel formulation.

www.iajpr.com
Pag
e51
80
Vol 4, Issue 11, 2014. Dhirajkumar Ch. Katariya et al. ISSN NO: 2231-6876
Ocular tolerance:
The animals were exposed to the test for tolerance in a stepped manner to minimize their probable un-necessary exposure
to the irritancy. Ocular irritation study results are showed in Table 8. Obtained score for optimised formulation was found to be zero
which signified that the formulation was non-irritant to eye. From this study, it was concluded that the gellan gum base can be used
safely for the ophthalmic applications as far as its ocular tolerance is concerned.
Table 8: Ocular irritation scores.
Lesion Assigned
score
Obtained
score
A- Cornea
- No ulceration or opacity
- Scattered or diffuse areas of opacity (other than slight dulling of normal
lustre); details of iris clearly visible.
- Easily discernible translucent area; details of iris slightly obscured
- Nacrous area; no details of iris visible; size of pupil barely discernible
- Opaque cornea; iris not discernible through the opacity
0
1
2
3
4
0
B- Iris
- Normal
- Markedly deepened rugae, congestion, swelling, moderate
circumcorneal hyperaemia; or injection; iris reactive to light
- Hemorrhage, gross destruction, or no reaction to light
0
1
2
0
C- Conjunctivae (Redness)
- Normal
- Some blood vessels hyperaemic
- Diffuse, crimson colour; individual vessels not easily discernible
- Diffuse beefy red
0
1
2
3
0
D- Chemosis (Swelling refers to lids and/or nictating membranes)
- Normal
- Some swelling above normal
- Obvious swelling, with partial eversion of lids
- Swelling, with lids about half closed
- Swelling, with lids more than half closed
0
1
2
3
4
0
Antiglaucoma activity:
Ideal formulation should show the maximum control over the increased intra ocular pressure for longer time. To study
whether the formulationreflected a better optimised use or not, it was necessary to study the parameters like onset time, ΔIOP, Tmax
(time required to achieve peak ΔIOP), ΔIOPmax (the peak ΔIOP) and Area under the curve (AUC). From the Figs 14 and 15, it was
concluded that, for timolol maleate solution formulation the onset time was 1 hr and the duration of effect was till 3.5 hrs. From the
IOP reading it was seen that after 3.5 hrs formulation was no longer present in the cul-de-sac. In case of timolol maleate ophthalmic
in-situ gel formulation onset time was 1.5 hr and the effect continued against rise in ocular pressure till the total study period, which
was for 6 hrs. Results are provided in table 9, it may be noted from the study that though Tmax for the in-situ gel formulation was
more than that of the timolol maleate solution formulation and the onset for the solution formulation was more in comparison with the
in-situ gel formulation, the ΔIOPmax for in-situ gel formulation was found to be more than that of the solution formulation of timolol
maleate. The AUC values were calculated by multiplying the time interval with mean ΔIOP for individual observations and finally
adding all together. In case of AUC values, in-situ gel formulation showed 1.67 times more than that of solution formulation, which
confirmed that the in-situ gel formulation had a longer duration of its antiglaucomaeffect in comparison with the solution. In
comparison with solution formulation, optimised formulation could show the achievement of better outcome.The increased duration of
action in case of in-situ gelling product compared to solution might be due to high viscosity as one of the reason. Low residence time
for a solution formulation is known to be creating the problem of frequent administration. In case of the in-situ gel formulation the
anti-glaucoma effect was prolonged which signified that the residence time of the formulation was enhanced because of the
formulation art. With the in-situ gel formulation patient would get relief from the glaucoma for longer duration. Further this could
reduce the dosing frequency of the formulation which would confirm the patient compliance.

www.iajpr.com
Pag
e51
81
Vol 4, Issue 11, 2014. Dhirajkumar Ch. Katariya et al. ISSN NO: 2231-6876
Fig. 14: Effect of timolol maleate solution in acute glaucoma model.
Each value is the mean ±Standard error mean of three determinations. X - P<0.001- ***
Fig. 15: Effect of timolol maleate in-situ gel formulation in acute glaucoma model.
Each value is the mean ±Standard error mean of three determinations.X - P<0.001-***; Y - P<0.01-**.
Table 9: Pharmacokinetic parameters of timolol maleate solution and in-situ gel formulation.
Formulation Tmax (h) ΔIOPmax (mmHg) AUC0→6 h (mmHg hr)
Timolol maleate solution 3 8.57 17.45
In-situ gel formulation of timolol maleate 4 9.43 29.25
CONCLUSION
The gellan gum based in-situ gelling systems containing timolol maleatean antiglaucoma agent and various concentration of
the gum for ocular administration have been designed and evaluated successfully. The gel formed in-situ provided sustained drug
release which was much better than a solution formulation. It could be concluded that 0.75% w/v polymer showed better potential for
sustained topical drug delivery to eyes for rational drug therapy as supported by in-vivo test studies. The system exhibited physically
entangled polymer networks, which rendered it favorable for ocular use as the network could easily disentangle upon shear stress
www.iajpr.com
Pag
e51
82
Vol 4, Issue 11, 2014. Dhirajkumar Ch. Katariya et al. ISSN NO: 2231-6876
associated with blinking, hence preventing induced lacrimation, which is usually provoked by more viscous systems. The designed
product exhibited the most favorable characteristics in terms of phase transition, rheological and mucoadhesive properties. The
optimised formulation showed satisfactory viscosity which was free flowing liquid at non-physiological condition and would shift to
firm gel after administration. This would ensure suitable gel strength and prevent rapid precorneal elimination. Further, mucoadhesive
study confirmed that formulation attached to the ocular mucosal surface for a relatively long time, which would improve the retention
of the drug promising a high bioavailability. Thus, prolonging corneal residence time and reducing nasolacrimal drainage. In vivo eye
irritation test of optimised formulation showed that it could be accepted as safe for ophthalmic use. Both in vitro and in vivo results
indicated that the optimised formulation performed better in retaining the drugcompared to drug solution. The optimized formulations
showed satisfactory viscosity, release behavior and antiglaucoma activity. It also promised to reduce the frequency of drug
administration, thus improving patient compliance. The methodology adopted for preparation of in-situ gel solution was very simple
and cost effective. Therefore, the proposed formulation of ion activated timolol maleate ophthalmic in-situ gel developed in this study
would have potential for using as an alternative to conventional timolol maleate solution eye drop to increase patient compliance.
Thus, through this work a meaningful platform for in-situ gelling type ophthalmic drops has been recommended. With further
logistics, various API would be possible to be fitted in this. The suggestion has ample potential for scale up.
Aknowledgement:
Thanks to Dr. Arjun S. Ahuja Eye Surgeon, Seth G.S.Medical College and K.E.M Hospital for providing a Schiotz tonometer
for Anti-glaucoma study. Special thanks to Kedar Cikhalikar for his valuable guidance during research work.
Conflict of Interest:
Conflict of interest declared none.
REFERENCES
1. Katariya D.C et al, .Current status of Ophthalmic In-situ forming hydrogel, Int J Pharm Bio Sci 2012;3:3: 372 – 388.
2. Spandana Vemireddy, B. Chandrashekar Reddy. Formulation and in vitro evaluation of acetazolamide ophthalmic inserts. Indo
American Journal of Pharmaceutical Research. 2013; 3: 6235-6247.
3. Lee, V.H., Robinson, J.R., Mechanistic and quantitative evaluation of precorneal pilocarpine disposition in albino rabbits. J.
Pharm. Sci. 1979; 68: 673–684.
4. Nanjawade et al, In-situ forming hydrogels for sustained ophthalmic drug delivery, Journal of Controlled Release 2007; 122: 119-
134.
5. M. A. Kalam, Yasmin Sultana, A. Samad, Asgar Ali, Gelrite-Based In Vitro Gelation Ophthalmic Drug Delivery System of
Gatifloxacin,Journal of Dispersion Science and Technology 2008; 29: 89–96.
6. Urtti, A., Salminen, L., Minimizing systemic absorption of topicallyadministered ophthalmic drugs. Surv. Ophthalmol.1993; 37:
435–456.
7. Usitalo H, Kahonen M, Improved systemic safety and risk benefit ratio of topical 0.1% timolol hydrogel compared with 0.5%
timolol aqueous solution in the treatment of glaucoma, Graefes Arch Clinical Exp Ophthalmol, 2006;244:11: 1491-6.
8. Mundada AS, Shrikhande BK. Formulation and evaluation of ciprofloxacin hydrochloride soluble ocular drug insert. Curr Eye
Res.2008;33:469–75.
9. Higuchi WI. The analysis of data on the medicament release from ointments. J Pharm Sci. (1962);51: 802–4.
10. Katrizky AR, Fali C.N and Li J, General synthesis of polysubstituted Benzo (b) furans. J.Org. Chem. 1997;62: 8205-209,.
11. J. Padma Preetha, K. Karthika, Rekha. NR and Khalid Elshafie, J. Chem. Pharm. Res. 2010; 2:3:528-535.
12. Jansson PE, Lindberg B, Sandford PA. Structural studies of gellan gum an extracellular polysaccharide elaborated by
Pseudomonas elodea. Carbohydr Res. 1983;124:135–9.
13. Karen J. Quigley, Rheological evaluation of deacetylated gellan gum (Gelrite) for pharmaceutical use,International Journal of
Pharmaceutics1991; 13: 117-123.
14. K.D.Tripathi, Essential of pharmacology, Edition-5. Jaypee Publication; 2003, 85-89.
15. Formulation and evaluation of ion activated ocular gels of ketorolac tromethamine, sirish vodithala, sadhna khatry, 2010; 2: 3: 33-
38.
16. Amal El-Kamel, Heba Al-Dosari, and Fahad Al-Jenoobi, Environmentally Responsive Ophthalmic Gel Formulation of Carteolol
Hydrochloride,Drug Delivery2006;13:55–59.
17. Deasy PB, Quigley KJ. Rheological evaluation of deacetylated gellan gum (Gelrite) for pharmaceutical use. Int J Pharm. 1991;73:
117–23.
18. Gilbard J.P, Human tear film electrolyte concentrations in health and dry eye disease, Inv . ophthalmol Clin, 1994;34: 27-36.
19. Gilbard J. P, Farris R L, Osmolarity of tear mmicrovolumes in keratoconjunctivitis sicca, Arch Ophthalmol 1978; 96: 677-681.
20. Mishima S, Kubota Z, The tear flow dynamics in normal and keratoconjunctivitis sicca cases, In Solan M.P, Proceddings of the
XXI, International congress, Mexico, 1970: 1801-1805.
21. Mohanambal E, Arun K. and Abdul Hasan Sathali A, Formulation and Evaluation of pH-triggered in-situ Gelling System of
Levofloxacin, Ind J Pharm Edu Res.2011; 45:1: 58-64.
22. Himanshu Gupta, Sanyog Jain, Rashi Mathur, Pushpa Mishra, Anil K. Mishra and T. Velpandian, Sustained Ocular Drug Delivery
from a Temperature and pH Triggered Novel In-situ Gel System, Drug Delivery 2007; 14: 507–515.
23. Daijad R. C, Gatifloxacin sustain ophthalmic, Indian journal of pharmaceutical sciences 2006;68:06: 809-814.

www.iajpr.com
Pag
e51
83
Vol 4, Issue 11, 2014. Dhirajkumar Ch. Katariya et al. ISSN NO: 2231-6876
24. B. Srividya, Rita M. Cardoza, P. D Amin, Sustained Ophthalmic delivery of ofloxacin from pH triggered in-situ gelling system,
Journal of Controlled Release2001;73: 205-211.
25. Optimization and evaluation of thermoresponsive diclofenac sodium ophthalmic in situ gels Rathapon Asasutjarita, Suthira
Thanasanchokpibullb, Asira Fuongfuchatc, Sukitaya Veeranondhad, International Journal of Pharmaceutics 2011;411: 128–135.
26. Hongyi Qi, Wenwen Chen, Chunyan Huang, Li Lib, Chuming Chen, Wenmin Li , Chunjie Wu, Development of a poloxamer
analogs/carbopol-based in situ gelling and mucoadhesive ophthalmic delivery system for puerarin, International Journal of
Pharmaceutics 2007;337:178-187.
27. Basavaraj K. Nanjwade, Manjappa A.S, Murthy R.S.Rb, Yuvaraj. D. Pol, A novel pH-triggered in-situ gel for sustainedophthalmic
delivery of ketorolac tromethamine, Asian Journal of Pharmaceutical Sciences2009; 4 :3: 189-199.
28. Giulia Bonacucina, Sante Martelli, Giovanni F. Palmieri, Rheological, mucoadhesive and release properties of Carbopol gels in
hydrophilic cosolvents, International Journal of Pharmaceutics 2004; 282: 115–130.
29. Blanco-Fuente, H., Anguiamo-Igea, S., Otero-Espinar, F.J., Blanco- M´endez, J, In vitro bioadhesion of carbopol hydrogels, Int. J.
Pharm.1996; 142: 169–174.
30. Ponchel, G., Touchard, F., Duchene, D., Peppas, N.A., Bioadhesive analysis of controlled release systems. I. Fracture and
interprenetration analysis an poly(acrylic acid)-containing systems, J. Control. Release1996; 5:129–141.
31. D. S. Jones, A. D. Woolfsom, A. F. Brown, Textural, viscoelastic and mucoadhesive properties of pharmaceutical gels composed
of cellulose polymers, International Journal of Pharmaceutics1997; 151: 223-233.
32. D. S. Jones, A. D. Woolfson, J. Djokin, W. A. Coulter, Development and mechanical characterization of bioadhesive semisolid,
polymeric systems containing tetracycline for the treatment of periodontal diseases, Pharm. Res. 1996; 13: 1734-1738.
33. Vandamme T.F, Journal of controlled release 2005; 102: 23-38.
34. Sunil sharma, Dharampal pathak, Studies on Corneal Permeation and Oculo-Hypotensive Effect of Benazepril in Chronic and
Acute Models of Glaucoma, Iranian journal of pharmacology & therapeutics 2006; 5:2: 145-149.
35. Ashutosh jani, Ramesh k goyal, Effect of Calcium Channel Blockers on Intraocular Pressure in Rabbits, Iranian journal of
pharmacology & therapeutics 2005; 4:2: 95-99.
36. Sears D, Blood-aqueous barrier and alpha chymotrypsin glaucoma in rabbits. Am J Ophthalm 1974; 77: 378–383.
37. Bonomi L, Tomazzoli L, An emproved model of experimentally induced ocular hypertension in the rabbit, Invest Ophthalmol.
1976; 15:781-784.
38. Yuejiang Liu, Jinpeng Liu, In-situ gelling gelrite/alginate formulations as vehicles for ophthalmic drug delivery, AAPS Pharm
SciTech 2010; 2 : 2 : 610- 620.
39. Kang, K. S., Veeder, G. T. and Cottrell, I. W. Progress in Industrial Microbiology1983; l8: 231.
40. C. Upstill, E. D. T. Atkins and P. T. Attwooi, Helicalconformations of gellan gum, Int. J. Biol. Macromol. 1986; 8: 275-288.
41. Sanderson, G. R. and Clark, R. C. Food Technol. 1983; 37: 63.
42. Crescenzi, M. Dentini, and T. Coviello, Novel Biodegradable Microbial PolymersKluwer Academic Publishers, The Netherlands,
1990.
43. Dhiren P. Shah, Girish K. Jani , Modification and Characterization of Gellan Gum, , Pharmaceutical Technology 2003; 33: 7: 48-
58.
44. Moorhouse R., Colegrove G.T., Sandford P.A., Baird J.K. and Kang K.S., PS-60: a new gel-forming polysaccharide. In D.A.
Brandt (Ed.), Solution Properties of Polysaccharides,Washington, DC, 1981: 111-124.
45. A. Rozier, C. Mazuel, J. Grove and B. Plazonnet,Gelrite®: A novel, ion-activated, in-situ gelling polymer for ophthalmic vehicles.
Effect on bioavailability of timolol,International Journal of Pharmaceutics1989;57: 163-168.
46. Banker, G.S., Rhodes, C.T.,. Modern Pharmaceutics. Marcel Dekker, New York; 2002: 415–423,.
47. Shi-lei Caoa, et al,In- situ gel based on gellan gum as new carrier for nasal administration of mometasone furoate,International
Journal of Pharmaceutics 2009; 365: 109–115.
48. Bothner, H., Waaler, T., and Wik, O. Drug Dev. Ind. Pharm. 1990; 16: 755–768.
49. Patrick J Sinko, Martin’s Physical pharmacy and pharmaceutical sciences, 6th
edition, Lippincott Williams and Wilkins Publisher;
2011 : 459-491.
50. Grasdalen H, Smidsroed O. Gelation of gellan gum. Carbohydr Polym. 1987;7:371–93.
51. Moritaka H, Kimura S, Fukuba H. Rheological properties of matrix-particle gellan gum gel: effects of calcium chloride on the
matrix. Food Hydrocolloids 2003;17:653–60.
52. Yuguchi Y, Urakawab H, Kajiwarab K. The effect of potassium salt on the structural characteristics of gellan gum gel. Food
Hydrocolloids 2002;16:191–5.
53. Chanrasekaran, R., Puigjaner, L.C., Joyce, K.L., Arnott, S, Cation interaction in gellan: an X-ray study of the potassium salt.
Carbohydr. Res. 1988; 181: 23–40.
54. Chanrasekaran, R., Thailambal, V.G., The influence of calcium ions, acetate and l-glycerate groups on the gellan double helix.
Carbohydr. Polym. 1990; 12, 431–432,.
55. Lodge, A. S., A network theory of flow birefringence and stress in concentrated polymer solutions. Trans. Faraday Soc.
1956;52:120–130.
56. Haoyun Wu, Zhidong Liu, Junjie Peng, Lin Li, Nan Li, Jiawei Li, Hao Pan, Design and evaluation of baicalin-containing in situ
pH-triggered gelling system for sustained ophthalmic drug delivery, International Journal of Pharmaceutics 2011; 410: 31–40.
57. Anumolu, S., Singh, Y., Gao, D., Design and evaluation of novel fast forming pilocarpine-loaded ocular hydrogels for sustained
pharmacological response. J. Control Rel. 2009; 137: 152–159.

www.iajpr.com
Pag
e51
84
Vol 4, Issue 11, 2014. Dhirajkumar Ch. Katariya et al. ISSN NO: 2231-6876
58. Barbara Buchan, Graeme Kay, Anne Heneghan, Kerr H. Matthews, Donald Cairns, Gel formulations for treatment of the
ophthalmic complications in cystinosis,International Journal of Pharmaceutics 2010; 392: 192–197.
59. Maheswara Reddy C. et al, Design and Evaluation of Chloramphenicol Thermoreversible Insitu Gels for Occular, International
Journal of Innovative Pharmaceutical Research. Drug Delivery 2011; 2:2: 131-138.
54878478451141020