In humanitarian contexts Addressing Gender-Based Violence.
28
In humanitarian contexts Addressing Gender-Based Violence
-
Upload
isaac-wight -
Category
Documents
-
view
222 -
download
2
Transcript of In humanitarian contexts Addressing Gender-Based Violence.

In humanitarian contexts
Addressing Gender-Based Violence


RH entry point to work on GBV - especially in humanitarian contexts:
• In some specific situations GBV diagnosis is only possible in RH services (maybe RH visit is the only health visit for a woman during pregnancy and RH staff are the only people with whom to talk about intimate matters)

GBV exists everywhere in the world, but there are co-factors increasing the phenomenon:
• Conflict and post-conflict situations• Overpopulation• Religious fundamentalism
• Most GBV victims do not disclose the problem spontaneously as GBV is still generally considered as a private matter
• But it is difficult for many health operators to ask about sexual or domestic violence.

In reality GBV is a public health issue
• But it is a sensitive issue for everybody.• Psychological barriers, prejudices and limiting
beliefs (individual, family and social taboos).But, if operators are not able to talk about it, how can we expect that clients disclose the
problem?

GBV survivors: difficult clients
Domestic violence Perpetrators usually have emotional linkages with victims, are supposed to love and protect them, and are often loved by them.
Particular mix of love, fear and sense of guilty.
Double threat: from outside (aggression) and from inside (loss of object of love)
Very difficult for them to establish TRUST relationships

The key to addressGBV is to train Health Operators
To overcome their barriers
(MD, midwives, nurses, psychologists, social and field workers, lawyers, male counsellors)

Staff training based on experiential activities:
• Awareness of their personal prejudices and limiting beliefs about GBV
• Screening for all clients• Understanding of survivors’ needs, concerns and
their difficulties in asking for help• Trauma theory• On-site treatment • Referral• Burn out risk

To be in the survivor’s shoes: blindness

- Groups: to create a trust relationship with others; to train peer facilitators
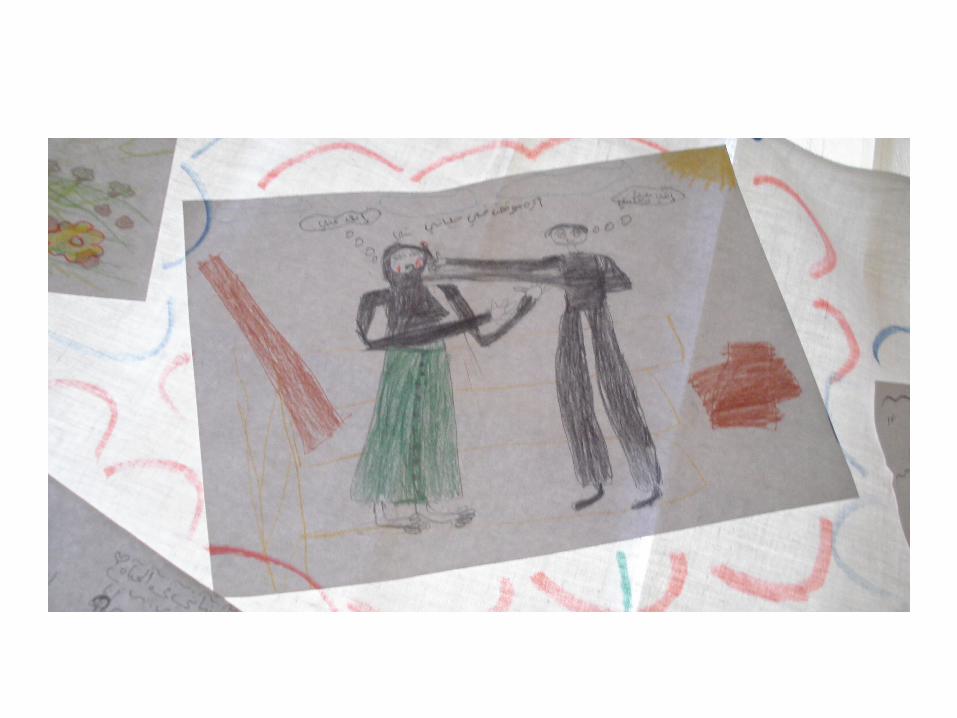
- Body work and Art: to elaborate traumatic experiences, to re-establish a contact with themselves, to enhance personal empowerment
Working with GBV survivors:Treatment

Groups: safe space to break loneliness and shame

• Drawing

PTSD in GBV survivors
Difficult to treat because the trauma is like a ”cyst" inside:
• individual psyche• family system with a strong prohibition to talk about it• social system (GBV: ”private problem”. Shame and
blame on the victim, particularly in sexual abuse. Social bias and honor killing risk)
GBV victims are thus silenced not only by the perpetrators
of the violence but also by society

PTSD Traumatic memories
When they appear they have a typical structure: - not verbal and narrative; - usually they are flashbacks, intrusive
memories and interfering feelings.
Many studies show that in PTSD some brain areas are blocked (speech areas), that’s why we have to focus on no-verbal approaches

Why body work?Verbal reconstruction of traumatic experiences is crucial
BUTthe body is the "container" of traumatic experiencesBody work can help to overcome traumatic feelings
and to re-elaborate themAttention to abreactions risk of re-experiencing the
trauma while working on the bodyAssess clients’ psychological sustainability

EYES
• In PTSD what is really important is to increase the client's control of her life more that trying to "relax”
• We usually start body work from eye level, crucial to understand and control the world around us

GBV survivor’s lost eyes






Neuroplasticity

Verbal elaboration after body and art work in order to take awareness and to integrate body and mind

European Association Body Psychotherapy
14° European and 10th international congress of body psychotherapy
The Body in Relationship SELF - OTHER – SOCIETY
11-14th September 2014Lisbon – Portugal
ISCTE www.lisbon2014.eabp-isc.eu

Mindfulness Based Stress Reduction (MBSR) developed in 1979 by Jon Kabat-Zinn, an MIT-educated scientist.