IMS Magazine Winter 2012
44
IMS MAGAZINE WINTER THINK, LEARN, DISCOVER. 2012 NFL PLAYER’S PERSPECTIVE Forced into retirement because of concussions, Sean Morey now advocates strongly for athlete safety DR. CATHARINE WHITESIDE A look at her journey from IMS student to the Dean of the Faculty of Medicine BOOK REVIEWS Exclusive interview with Rebecca Skloot, author of “The Immortal Life of Henrietta Lacks” SPORTS-RELATED INJURIES Learn about how our experts are shaping concussion and spinal cord research
-
Upload
ims-magazine -
Category
Documents
-
view
220 -
download
3
description
A magazine highlighting the research, students and faculty at the Institute of Medical Science at the University of Toronto. This issue's feature focuses on sports-related injuries.
Transcript of IMS Magazine Winter 2012

IMSMAGAZINEWINTERT H I N K , L E A R N , D I S C O V E R . 2012
NFL PLAYER’S PERSPECTIVEForced into retirement because of concussions, Sean Morey now advocates strongly for athlete safety
DR. CATHARINE WHITESIDEA look at her journey from IMS student to the Dean of the Faculty of Medicine
BOOK REVIEWSExclusive interview with Rebecca Skloot, author of “The Immortal Life of Henrietta Lacks”
SPORTS-RELATED INJURIESLearn about how our experts are shaping concussion and spinal cord research


02IMS MAGAZINE WINTER 2012 SPORTS-RELATED INJURIES |
TABLE OF CONTENTS
Commentary ...................................03Letter from the Editor .....................06News at a Glance ...........................07Director’s Message ........................10Feature ............................................11Spotlight .........................................23Expert Opinion ................................25Book Reviews .................................27Close Up .........................................29Viewpoint .......................................31Behind the Scenes ..........................35Future Directions ............................37Funding ...........................................39Ask the Experts ...............................40Past Events .....................................41Diversions .......................................42
Sports-Related Injuries
Viewpoint: Religion and ScienceClose Up: Visualizing Science
Experts weigh in on the need for greater aware-ness, more accurate diagnostic measures, and
regulated treatment plans to protect our athletes from concussions and spinal cord injury.
By Minyan Wang and Tobi LamThe cover features one of hockey’s most talk-
ed about pieces of equipment: the helmet. Despite advances in technology, the modern
sports helmet is unable to protect against many of the forces that cause concussions
and spinal cord injuries.
Copyright © 2012 by Institute of Medical Science, University of Toronto. All rights reserved. Reproduction without permission is prohibited.
The IMS Magazine is a student-run initiative. Any opinions expressed by the author(s) are in no way affiliated with the Institute of Medical Science or the University of Toronto.
One student’s perspective on the age-old di-chotomy between religion and science.
BMC lecturer Michael Corrin uses his design talents to communicate and explain scientific concepts.
FEATURE
Cover Art
11
3329
MAGAZINE STAFFNatalie VenierNina BahlAllison RosenAdam SantoroKamila LearTobi LamAndreea MargineanuMerry WangMinyan WangCorinne DalySalvador AlcaireS. Amanda AliRickvinder BeslaDanielle DesouzaMelanie GuenetteAaron KucyiRosa MarticorenaLaura Seohyun ParkTetyana PekarMeghna RajaprakashJennifer RilstoneZeynep YilmazYekta DowlatiLaura FeldcampPaulina RzeczkowskaMohammed SabriBrett Jones, Wenjun Xu
Editor-in-Chief
IN THISISSUE...
Managing EditorAssistant Managing Editors
Departmental Advisor
Advertising ManagerMagazine Committee
Design Editors
Photography
Acknowledgements
Phot
o by
Pau
lina
Rzec
zkow
ska.
Imag
e of
“Go
d cr
eate
s Ad
am”:
Sis
tine
Chap
el, M
iche
lang
elo
Buon
arro
ti.15
10.

03 | IMS MAGAZINE WINTER 2012 SPORTS-RELATED INJURIES
COMMENTARY
Quotes and Commentary
Tell us what you think
What to look for next issue:
“I love reading through the IMS Magazine. I always find the articles interesting and informative. This past issue, I particularly enjoyed reading the philosophy of science article, Darwin. Newton. Einstein. Popper? It was very well written and made me view science in a different light.”-Xianfeng Ge, IMS Student
“Once again... fantastic issue!”- Dr. Karen Davis, IMS Associate Director “[The magazine] is professionally done and the articles are interesting. It’s an extremely hard thing to pull off, and as a previous edi-tor-in-chief of a UofT journal, I greatly appre-ciate the amount of effort you have put in.” - Kirill Zaslavsky, University of Toronto stu-dent
“Great issue on prostate cancer. I wish I knew where to find the magazines in hard copy, though!”- S.B., IMS Student
Once the magazine has been released, you can find hard copies at the IMS office and at IMS events/seminars while they’re still available. - IMS Magazine
1) A look into the Krembil Neuroscience Centre (KNC) Sports Concussion project: a Canadian study investigating the potential correlation between repeated concussive incidents and late deterioration of brain function. Researchers are currently study-ing long-term concussion effects on profes-sional football and hockey players.
2) The neurological significance of subclini-cal blast exposure by Dr. Andrew Baker.
Dear Editor,
I found the last edition of the IMS magazine very informative. I was particularly inter-ested in the feature section because I recently completed a summer research project on prostate cancer under the supervision of Dr. Neil Fleshner. As I reviewed the literature, I realized that there were mixed findings on whether testosterone plays an etiological role in the development of prostate cancer. I think it is of benefit to bring this controversial topic to light.
Prostate cancer (PCa) is the third most com-mon cause of cancer related death among Canadian men, with 25,500 cases diagnosed in 20111. The prostate has three main func-tions: 1) fluid production for semen, 2) con-trolling the flow of urine and 3) manufactur-ing a protein called prostate specific antigen (PSA)1. Currently, PSA testing remains the most common diagnostic biomarker used in
the detection of PCa, since prostate cancer cells stimulate more PSA production than healthy prostate cells1. In addition, circulat-ing male androgens, primarily testosterone (mediated by the hypothalamic-pituitary-testicular axis), have also been shown to play an essential role in the development of pros-tate tumour growth.
As early as 1941, Hudgins and Hodges dem-onstrated that testosterone acts as a fuel for prostate cancer cell growth1,2. This observa-tion raised questions about the possible role of androgens as an etiological factor in the development of PCa3. The underlying im-portance of assessing serum testosterone lev-els and its association with PCa risk has been contradictory. Some researchers have shown that lower levels of serum testosterone are associated with increased PCa risk, while others indicate no correlation between these
Pho
to b
y La
ura
Feld
cam
p

04IMS MAGAZINE WINTER 2012 SPORTS-RELATED INJURIES |
COMMENTARY
Dear Editor,
I enjoyed reading a recent version of the IMS Magazine (Summer 2011). In particular, the article “Sexism in Biomedical Research” dis-cussed a fascinating topic.
I recently heard about an event that focuses on the same problem. Hosted by Women of Baycrest, Sex, Aging and Memory is described as “Canada’s first women’s brain health con-ference.” The event, held on October 18, 2011, addressed the fact that male mice are preferentially used in medical research, de-spite the fact that many diseases do not occur preferentially in men. For example, the con-ference described how 70% of new Alzheim-er’s disease patients are women.
With special guest speaker Hilary Swank and host Christine Bentley, this high-profile con-ference may help shine light on a big problem facing medical research today. Since women’s health and mental health are becoming top research priorities, I hope that articles like yours and conferences like this can help over-come this research disparity.
Sincerely,
Allison RosenMSc Candidate, IMS, University of Toronto
We really appreciate all of the encouraging comments and messages we have received since the release of the IMS Magazine’s inaugural issue. We encourage our readers to send their feedback -- comments, questions, corrections, or letters to the editor -- to [email protected]
@IMSMagazinewww.facebook.com/groups/imsmagazine/
variables4. Nevertheless, a significant num-ber of epidemiological studies have failed to ascertain a consistent relationship between higher serum androgen levels and its poten-tial as a risk factor for prostate cancer3.
Research on the role of testosterone in PCa sparked interest in androgen deprivation therapy (ADT) for the management of PCa3. The most common form of ADT is medical castration with the use of luteinizing hor-mone releasing hormone (LHRH) agonists. Individuals diagnosed with advanced PCa during the latter stages of the disease are more likely to be treated with hormonal therapy1. LHRH agonists block the systemic production of testosterone, aiding in reduc-tion of tumour size and lowering PSA levels.Previous studies have suggested that fol-lowing castration with LHRH, there are still considerable levels of testosterone in the sys-tem5. There is also speculation about the “cut point” level of serum testosterone achieved during hormonal intervention6. Expert pan-els have indicated that the new benchmark for serum testosterone levels for patients on ADT should be lower than 20 ng/dL. The recommendation is that serum testosterone levels be measured in patients using LHRH analogues, regardless of a rising PSA, since a clinically significant number of individuals fail to achieve castrate levels of testosterone6.
From a review of the literature, it is quite
evident that there is an incomplete under-standing about the precise relationship be-tween PCa and testosterone, thus warranting further investigation3. In comparison, the area of androgenic potential of PCa remains active with increasing discoveries. Future clinical practice should focus on measuring serum testosterone levels in combination serum PSA to evaluate the effectiveness of LHRH therapy, which is the current focus of our research6.
Sincerely,
Seetha Venkateswaran,IMS Summer Student
Corrections: IMS Magazine Fall 2011
IMS Summer Student Research Article: The National Chiao Tung University was listed in Japan instead of Taiwan. Also, Kyoto University participants were not listed in the map/demographics. The IMS Magazine regrets these errors.
References1. http://www.prostatecancer.ca/2. Huggins C and Hodges CV. Studies on prostatic cancer. I. The effect of castration, of estrogen and of androgen injection on se-rum phosphatases in metastatic carcinoma of the prostate. 1941. Journal of Urology. 2002;167:948-951.3. Schmitt CD, Rhoden EL, Almeida GL. Serum levels of hy-pothalamic-pituitary-testicular axis hormones in men with or without prostate cancer or atypical small acinar proliferation. Clinics. 2011;55(22):183-187. 4. Koo JM and Shim BS. Significance of Serum Testosterone for Prostate-Specific Antigen (PSA) Elevation and Prediction of Prostate Cancer in Patients with PSA Above 10 ng/ml. Korean Journal of Urology. 2010;51:831-835.5. Pai HH, Pickles T, Keyes M, Jones S, McDonald RE, Lesper-ance M, Berthelet E. Randomized study evaluating testosterone recovery using short-versus long-acting luteinizing hormone re-leasing hormone agonists. CUAJ. 2011 Jun;5(3):173-179. 6. Gomella LG. Effective Testosterone Suppression for Prostate Cancer: Is There a Best Castration Therapy. Reviews in Urology. 2009;11(2):52-60.
Contact Us

05 | IMS MAGAZINE WINTER 2012 SPORTS-RELATED INJURIES
NEWS AT A GLANCE

06IMS MAGAZINE WINTER 2012 SPORTS-RELATED INJURIES |
ertainly most of us have heard about Sidney Crosby (also referred to as ‘Sid the Kid’) and his battle with concussions, which has prevented him from returning to play in the National Hockey League. While the general public might miss seeing this phenomenal
player on the ice, developing a clear understanding of the physiological repercussions of his concussions should help us truly understand and appreciate the precautions being taken before Crosby can return to the game.
In light of the impact that concussion research has recently had on the sports world, we have brought together a collection of our very own experts—including Dr. Charles Tator and Senior Scientist Molly Verrier—in hopes of improving your scientific literacy on the topic of sports-related concussions and spinal cord injuries.
In this issue, we have had the privilege to highlight Sean Morey, the Pro Bowl Special Teams Player of the Decade and one of the captains of the Super Bowl XL Champion Pittsburgh Steelers and 2008 NFC Champion Arizona Cardinals. He sat down with us to explain how concussions have personally affected him, the game of football, and his strong advocacy for player protection. I hope this can provide insight into how concussion research can transcend the laboratory and have international impact.
It is also my pleasure to introduce to you our new Book Reviews section, where you will find reviews to novels read by the IMS community. In this first section, we have a special article by Rebecca Skloot, the famous author one of the best-selling novels The Immortal Life of Henrietta Lacks. I encourage you to read through some of the top picks from our community. If you have a book that you would like to review, we strongly encourage your feedback and book suggestions.
To conclude, I would like to thank Dr. Allan Kaplan and the IMS department for their on-going support with the IMS Magazine. Additionally, I must acknowledge the amazing IMS Magazine Team, whose contributions are invaluable to its production. I would like to wish you a wonderful new year filled with many great discoveries.
Enjoy!
Natalie VenierEditor-In-ChiefNatalie Venier is a third year PhD Candi-date at the Institute of Medical Science. She is currently studying prostate cancer chemoprevention at Sunnybrook Health Sciences Centre.
C
Letter fromthe Editor
Natalie VenierEditor-In-Chief, IMS Magazine
LETTER FROM THE EDITORPh
oto
by P
aulin
a Rz
eczk
owsk
a

07 | IMS MAGAZINE WINTER 2012 SPORTS-RELATED INJURIES
at a glance...
IMS STAFF ANNOUNCEMENTS
MARCH
FEBRUARY
JANUARY
For more information on IMSSA/IMSSA-related events, please visit: http://imssa.sa.utoronto.ca
For information on IMS news and events, please see: http://www.ims.utoronto.ca
Please send your comments and suggestions to: [email protected]
1219
18 IMS Graduate Open House
Career Development Series
IMSSA Yoga Fundraiser Event
Student Link Event
IMS Strategic Planning Retreat
IMSSA Pub Night
Orientation Day TBA Career Development Series
Transfer to PhD Workshop
Student-Supervisor Relationship Workshop
NEWS&VIEWS
IMS Strategic Planning Retreat
The Institute of Medical Science is currently in the midst of a very important, first-ever strategic planning initiative. Through an engaging and interactive process, we are exploring high level questions, such as: What impact does the Institute of Medical Science want to have in the world? What will we contribute to translational research and the training of researchers that is most meaningful? How can we harness all of our unique resources most fully, and what will we focus on over the next few years, to make a meaningful difference?
Through this work, the IMS will create a five-year strategic plan that takes into account our many diverse voices and needs, and will provide the IMS with the integrity needed for our decision making over the next five years. Representatives on a core planning team have been conducting interviews with people connected with the IMS to gather insights and ideas about the current status of the IMS, and where the IMS should focus its work over the next few years. Themes collected from these interviews will be used to shape the strategic plan that will be further developed at a full-day Retreat.
The IMS invites all faculty members and students to participate in this Retreat and be part of this critical conversation.
The Retreat will take place on Thursday, January 19, 2012 at the Bram & Bluma Appel Salon at the Toronto Reference Library, 2nd Floor, 789 Yonge Street (1 street north of Bloor) from 8:30 a.m. – 4:30 p.m. Breakfast and lunch will be served. For directions, please access the following link: http://g.co/maps/mdhxu.
TBA
TBA
NEWS AT A GLANCE
IMS Scientific Day – Mark your calendars!
This year’s IMS Scientific Day will be held on Tuesday, May 15, 2012. It will feature Bernard Langer keynote lecturer Dr. Thomas R. Insel, Director of the National Institute of Mental Health (NIMH).

08IMS MAGAZINE WINTER 2012 SPORTS-RELATED INJURIES |
IMSSA ANNOUNCEMENTS
New Faculty Members
AWARDS & SCHOLARSHIPSIMS Scientific Day Awards
Adalsteinn BrownAssociate Professor of Dalla Lana School
of Public Health, St. Michael’s Hospital
Katharina ManassisProfessor of Psychiatry,
Hospital for Sick Children
Susanna MakAssistant Professor of Medicine,
Mount Sinai Hospital
David GladstoneAssistant Professor of Medicine,
Sunnybrook Health Science Centre
Amna HusainAssociate Professor of Family and Com-
munity Medicine,Mount Sinai Hospital
Antonio FinelliAssociate Professor of Surgery,
Princess Margaret Hospital
Andrea DoriaAssociate Professor of Medical Imaging,
Hospital for Sick Children
Carol-anne MoultonAssistant Professor of Surgery,
Toronto General Hospital
Matthew MullerAssistant Professor of Medicine,
St. Michael’s Hospital
You can stay up to date on IMSSA events and workshops by checking out the IMSSA
website at http://imssa.sa.utoronto.ca, or you can join their Facebook
group at Institute of Medical Science (U of T).
The IMSSA would like to welcome all new and returning IMS students to 2012 with a FREE IMSSA pub night. The event will be held in late January at Grace O’Malley’s - stay tuned to your weekly IMSSA mail for further details.
Coming up in February, we will be hosting a winter IMSSA Graduate Student Mentorship Program where upper year IMS students will be available to field questions about life in graduate school and provide you with valuable insight. Light refreshments and snacks will be served. Please RSVP to [email protected].
Throughout the next few months, the IMSSA will be hosting Career-Related Events to help you explore a variety of careers selected by IMS students to be of greatest interest. If you have not already done so, please complete the following survey to help inform us of your career-related interests: http://app.fluidsurveys.com/surveys/ilyse/ims-students-career-interests-4.
Tickets are still available at $22 each for the Canadian Opera Company: Love From Afar dress rehearsal (featuring the director who has worked with Cirque du Soleil) on January 30th at The Four Seasons Centre for the Performing Arts. Please RSVP to [email protected] if you would like to attend.
NBA tickets for Raptors games will soon be available. Stay tuned for updates!
Laidlaw Manuscript Competition
Top rated students submitting manuscripts for the Laidlaw competition will be invited to give an oral presentation at IMS Scientific Day. Awards conferred at that time will be:
Laidlaw Prize – Clinical Science - $750Laidlaw Prize – Basic Science - $750Laidlaw Prize – Honourable Mention - $400
Manuscripts should be submitted electronically as a PDF file in the format of a letter to “Nature: International Weekly Journal of Science.” This is a mandatory format for this competition (even if the content of the manuscript has already been published in other formats). For information on Nature article formatting, length, etc., please visit: http://www.nature.com/nature/submit/index.html1#.
When there are multiple authors, a letter from your supervisor confirming that the majority of the work presented in the manuscript is your own must accompany the submission.
Send your electronic (PFD file) submissions to Kaki Narh Blackwood [email protected] by February 3, 2012.
NEWS AT A GLANCE
Alan Wu Poster Competition
The Alan Wu Poster Prizes are presented to the most outstanding basic science and clinical science abstracts and poster presentations.
All competitors are expected to prepare an abstract and poster (work must have been completed within the last 12 months of graduate studies), and to give a brief oral presentation at Scientific Day. Awards conferred at that time will be:
Alan Wu Poster Prize - Clinical Science - $250 + IMS Academic Development AwardAlan Wu Poster Prize – Basic Science - $250 + IMS Academic Development Award
An IMS Academic Development Award, valued at $500, is awarded to each finalist. The purpose of the IMS award is to encourage students to attend national or international conferences by partially covering travel/academic expenses, with supervisors covering the remainder of the cost.
Send your electronic (Word file) submissions to Kaki Narh Blackwood [email protected] by February 3, 2012.

09 | IMS MAGAZINE WINTER 2012 SPORTS-RELATED INJURIES

10IMS MAGAZINE WINTER 2012 SPORTS-RELATED INJURIES |
Allan S Kaplan MD FRCP(C)Director, Institute of Medical Science
This fifth issue of the IMS magazine focuses on the important area of sports-related concussions and spinal cord injuries, reflecting some of the critical research that IMS faculty are conducting. Congratulations to Natalie Venier and her team for their continued hard work and collective creative energies in producing this wonderful publication. Thanks as well to Kamila Lear for her ongoing assistance in this project.
In terms of IMS news, Dr. Mary Seeman completes her decades-long period of service as an IMS Graduate Coordinator as of December 31. We at the Institute of Medical Science are very sorry to see her leave. She has made an enormous contribution to the IMS in general, and in particular, to the well-being of our students. She is truly a beloved member of our team; her wisdom and sensitivity that she brings to her role will be sorely missed. We all wish her well.
As mentioned in my previous Director’s Message, the IMS is now in the midst of an extensive strategic planning initiative. Towards that end, we will have a strategic planning retreat on Thursday, January 19, 2012 at the Bram & Bluma Appel Salon at the Toronto Reference Library, 2nd Floor, 789 Yonge Street (1 street north of Bloor) from 8:30 a.m. – 4:30 p.m. Breakfast and lunch will be served. All faculty of IMS and all students are invited to attend this important event. Please RSVP to Kamila Lear ([email protected]) by Monday, January 9 at the latest if you plan to attend.
I wish to also announce that IMS Scientific Day will be taking place on Tuesday, May 15 at McLeod Auditorium. The theme of this Scientific Day will be Translational Research. With that in mind, I am most pleased to tell you that Dr. Thomas Insel—a world-renowned translational neuroscientist and Director of the National Institute of Mental Health in the USA—will be delivering the Plenary Address on May 15. Please make sure to mark this day in your calendars.
The IMS Magazine has been a tremendous success and is just one of the many wonderful student-initiated projects that makes the IMS such a very special institute. I fully support the ongoing publication of the IMS magazine and look forward to the many opportunities the magazine can afford us for recruitment and for publicizing the outstanding research that in being conducted by our faculty and our trainees.
On behalf of everyone at the IMS, I hope you have all had a very happy and healthy holiday season. We look forward to the new year ahead.
Sincerely,
Director’sMessage
Allan S Kaplan, MSc, MD, FRCP(C)Director, IMS
Dr. Allan Kaplan became the IMS Director in July 2011. He is the Chief of Clinical Research and Director of Research Training at the Centre for Addiction and Mental Health (CAMH), and a Senior Clinician-Scientist in CAMH’s Mood and Anxiety Program. He is also the Vice Chair of Research, Director of the Clinician Scientist Program and Professor of Psychiatry at the University of Toronto.
Phot
o by
Moh
amm
ed S
abri
DIRECTOR’S MESSAGE

11 | IMS MAGAZINE WINTER 2012 SPORTS-RELATED INJURIES
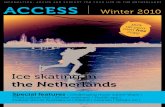
SPORTS INJURIES AN OVERVIEW
71%34%24%23%22%22%20%18%
FREQUENCY OF CONCUSSION SYMPTOMS
EFFECTS OF SPORTS INJURIES IN YOUTHSYMPTOMS & SIGNS OF CONCUSSION
* These statistics are drawn from a detailed analysis of concussions in the National Hockey League over a span of seven regular seasons (1997-2004), based on physician reports from every team in the league.
Benson BW, Meeuwisse WH, Rizos J, Kang J, Burke CJ. (2011). A prospective study of concussions among National Hockey League players during regular season games: the NHL-NHLPA Concussion Program. Canadian Medical Association Journal, 183(8): 905-911.
Centers for Disease Control and Prevention, USA (www.cdc.gov/concussion/sports/facts.html)
Johnson LSM. (2011). Concussion in youth ice hockey: It’s time to break the cycle. Canadian Medical Association Journal, 183(8): 921-924.
headache
dizziness
nausea
neck pain
low energy, fatigue
blurred vision
amnesia
loss of consciousness
10%80%207,830ER visits per year
of head & spinal cord injuries are due to sports related activities.
of professional ath-letes do not realize they have been concussed.
due to nonfatal sports-related head injuries between 2001-2005.
10.2
Saffary R, Chin LS, Cantu RC. (2011). Sports Medicine: Concussions in Sports. American Journal of Lifestyle Medicine, DOI: 10.1177/1559827611411649.
ThinkFirst Canada (www.thinkfirst.ca)
Centers for Disease Control and Prevention (www.cdc.gov/concussion/sports/facts.html)
Emergency department visits for sports- and recreation-related traumatic brain injuries (TBIs), including concus-sions, has increased by 60% among children and adolescents between 2001-2009. These increases might reflect an increased participation in sports and recreation, an increased incidence of TBI among partici-pants, and/or an increased awareness of the importance of early diagnosis.
The activities associated with the greatest number of TBI-related emergency department visits between 2001-2009 include bicycling, football, playground activi-ties, basketball, and soccer.
An estimated 500,000+ youths play organized minor ice hockey in Canada. Since it is known that the pediatric population is more vulnerable to concussion and slower to recover than adults, examining concussion in the context of ice hockey is important to Canadian research.
Loss of consciousness Blurred vision Memory problems Seizures or convulsions Balance problems Dizziness Fatigue or low energyAmnesia Sensitivity to light Sensitivity to noise Confusion Headache Drowsiness Feeling “pressure in the head” Feeling slowed down More emotionalNervous or anxiousSadness Neck pain Feeling “in a fog” Irritability Nausea or vomitingDifficulty concentrating Don’t “feel right”
ThinkFirst Canada (www.thinkfirst.ca)
FEATURE

12IMS MAGAZINE WINTER 2012 SPORTS-RELATED INJURIES |
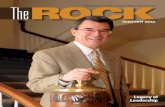
grey matter (cortex)
white matter
grey matter (deeper structures)
SPINAL CORD INJURYIn North America, sports activity is the second most common cause of spinal cord injury (SCI) and the fourth most common cause of spinal column fracture, which may subsequently damage the spinal cord itself.
Cervical spinal cord injury, occurring at the level of the neck, is a common type of SCI in athletes. Most cervical SCIs are the result of axial loading (force directed through the top of the head and through the spine), forcing the head into hyperflexion and/or rotation.Source: Bahr R. & Maehlum S. (2004). Clinical Guide to Sports Injuries. Human Kinetics: Champaign, IL.
CONCUSSIONA concussion is a common form of traumatic brain injury (TBI) caused by a direct or indirect hit to the head. Whether due to a direct blow, a fall, or sudden jolt, the brain shifts suddenly within the skull and can knock against the skull’s hard surface and brush against its bony protuberances within.
Exactly what happens to neurons in a concussion remains unclear. Brain cells appear to enter into a susceptible state following the injury; while the precise length of this period is unknown, evidence suggests that chemical changes underlie the brain’s increased sensitivity to stress. During this time, the brain does not function normally and is more vulnerable to a second head injury.Sources: ThinkFirst Canada; USA Centers for Disease Control and Prevention
Some researchers believe that tissue deformation, caused by rotational acceleration, translates into a shearing force between grey matter and white matter in the brain. Furthermore, many studies support the idea that at lower acceleration forces associated with concussion, the microtubules and other internal structures of axons become damaged, which can lead to swelling and potential disconnection.
The outer edges and internal portions of the brain consist of grey matter, nervous tissue highly populated with cell bodies. Between these regions is white matter, which is predominantly composed of axons. These axons form connections between different areas of grey matter, transmit action potentials, and transport important factors.
ABOUT THE ILLUSTRATORPaul Kelly recently completed his master's degree in Biomedical Communications from the University of Toronto. “While the discipline is rooted in the traditions of medical illustration, the BMC program trains artists with a background in science to create visual resources for a wide range of audiences using a variety of both traditional and digital tools, including high-end 3D animation and web-based applications.” - Paul Kelly
His research focus was 3D visualization in the field of mild traumatic brain injury and its effects on the brain and neural networks.
Paul has generously provided several illustrations and animation stills from his final project, most of which have been featured in this issue of the IMS Magazine. To view his entire animation or for further inquiries please visit his website at:http://bmc.erin.utoronto.ca/~paul/
During impact, the deep grey matter of the brain can rotate and shift, disrupting white matter tracts.
The brain can shift suddenly within the skull and knock against bony protuberances, disrupt-ing cortical structures and the tracts connecting different areas. Traction and shearing forces may also play a role in damage to cortical structures.
FEATURE

13 | IMS MAGAZINE WINTER 2012 SPORTS-RELATED INJURIES
FEATURE
Phot
o by
Yek
ta D
owla
ti
and Parkinson’s diseases, respectively9. Thus, virtually everyone should know the princi-ples of recognition and management of con-cussions: there should be widespread knowl-edge of the physical, cognitive and emotional effects of concussion, and also knowledge of the guidelines for return to play, work or school. It is in the public interest for all health care professionals—including nurses, thera-pists, chiropractors, physicians and others—to be proficient in this field. Recently, there have been major advances in our under-standing of concussion and its consequences which have created the additional burden of keeping all practitioners “up to speed.”
Although it is highly desirable for all pos-sible witnesses and bystanders to recognize the signs and symptoms, a medical doc-tor should be responsible for the actual di-agnosis. At present, the diagnosis must be made clinically because there is no proven biomarker, such as an imaging or computer-ized mini-neuropsychological test; thus, the diagnosis of concussion is made by a knowl-edgeable medical doctor and a compliant pa-tient. Unfortunately, in the absence of either ingredient, accurate diagnosis and manage-ment may be impossible. For example, the practitioner may not be “up to speed” or the concussed person may lie about symptoms or disregard management advice, frequent occurrences with athletes aiming to avoid removal from play1,3. The current defini-tion of concussion is any alteration of mental function due to a blow to the head or other part of the body8; loss of consciousness oc-curs only in a minority of cases. A useful
What You Need to Know to Recognize & Manage
oncussions are frequent in all age groups and can have serious consequences, and therefore, every
health care professional should know how to recognize and manage them. Parents should also be educated about concussions so that they can recognize them in their offspring. Everyone must be especially vigilant with older people who frequently sustain concus-sions through falls at home. Emergency per-sonnel are frequently required to recognize concussion symptoms after motor vehicle crashes. Employers must be aware of concus-sion at work, and appreciate their effect on return to work. Coaches, trainers, referees and teachers must also be knowledgeable to provide the best care for those concussed un-der their supervision in sports, and to guide them back to their athletic activities and dai-ly routine.
The sports medicine field has led the way in concussion research and management through international expert panels that have refined and clarified the definition and management guidelines for concussion10. The health care field has acknowledged the importance of accurate, timely recognition and appropriate management of concussions because misdiagnosis or faulty management can lead to serious short- and long-term consequences, including major disability and death. The second impact syndrome oc-curs when a concussed person, especially a younger person, returns to play before com-plete recovery and then sustains a second concussion12. Repetitive concussions can also potentially cause delayed post-traumatic brain degeneration, leading to dementia and movement disorders similar to Alzheimer’s
Dr. Charles H. TatorMD, PhD
Professor of Neurosurgery, Toronto Western Hospital
CConcussions
Diagnosis of Concussion

14IMS MAGAZINE WINTER 2012 SPORTS-RELATED INJURIES |
FEATUREAn
imat
ion
still
s pr
ovid
ed b
y Pa
ul K
elly
diagnostic aid for practitioners is the clinical testing protocol known as the Sport Concus-sion Assessment Tool, Version 2 (SCAT2) that lists 22 possible symptoms of concus-sion, the presence of only one of which is re-quired to qualify a positive diagnosis8. (For more information about SCAT2 and other management information, please visit the ThinkFirst website: www.thinkfirst.ca) As in-dicated above, the absence of proven imaging and neuropsychological biomarkers makes concussions difficult to diagnose. For ex-ample, CT and MRI scans are almost always normal after concussions, even repetitive concussions. Several different computerized neuropsychological tests are being promoted commercially, and at best, serve as an adjunct to clinical examination, but cannot be used as a stand-alone test to diagnose concussion. SCAT2 is free and contains a combination of clinical tests—including balance tests—and is just as accurate as a widely advertised mini-neuropsychological test2. Much infor-mation about concussion has evolved during the last 10 years, such as the fact that females appear to be more susceptible to concussion than males4, and that there may be a genetic factor underlying concussion susceptibility6.
Also, it is now known that after one concus-sion, there is greater susceptibility to another concussion, and subsequent concussions occur with less force and take longer to re-cover5.
With the recognition of the importance of concussions and their potential for life-taking or lifelong consequences, the responsibility for making the diagnosis falls to the medical practitioner. Thus, it is a standard of practice for every concussed person to be evaluated by a medical doctor, a position first advo-cated by the Canadian Association of Sport Medicine (CASM Position Statement, 2002) and reaffirmed by international panels of concussion experts8. The medical examina-tion should occur within a reasonably short interval, a principle not easily achieved in remote areas of the country. Rest is the most important aspect of initial management, and now includes both physical and mental rest; the inclusion of mental rest is a major change from previous recommendations. Unfortu-nately, there is no other measure proven to be successful for early treatment.
Achieving physical and mental rest is step one of the six-step return to play guidelines. When all symptoms have completely disap-peared, step two is instituted, which allows light physical exercise such as walking. The six graduated steps can be sport-specific with at least 24 hours between steps (see www.thinkfirst.ca for a complete description). Pro-gressive exercise is used as a measure of brain recovery rather than as a therapy, because as indicated above, there is no proven treatment for acute concussion other than rest. With six steps and at least one day between steps, the earliest a concussed athlete can return to play is one week, and most experts double that for children and youth.
The coup-contrecoup model of traumatic brain injury is the idea that the brain smacks against the inside surface of the skull on the opposite side from impact.
Management of Concussions

15 | IMS MAGAZINE WINTER 2012 SPORTS-RELATED INJURIES
FEATURE
With continuing residual symptoms, the athlete should not return to play. If the post-concussion syndrome lasts several weeks or months, then permanent non-return to colli-sion sports should be considered. Permanent non-return is recommended for persisting cognitive dysfunction revealed by detailed neuropsychological testing requiring sev-eral hours to perform. There is a major role here for detailed neuropsychological evalua-tion, which is much more accurate than the 20-minute computerized variety. The crite-ria for permanent non-return also include permanent neurological deficits, movement disorders, and lesions seen on CT or MRIs11. Worrisome features of multiple concussions for return to play decisions include number and frequency of concussions, interval be-tween concussions, length of time to recov-ery, patient age, and severity of forces to the head. For example, a young athlete who has sustained several concussions over a short time interval, such as 3-6 months, caused by decreasing levels of force and with persistent symptoms, such as cognitive deficits, should never resume collision sports. Although there is no known treatment other than rest to accelerate recovery from a single concus-sion or to treat most symptoms of repetitive concussions, posttraumatic depression can be successfully treated with the same meth-ods as non-traumatic depression.
Chronic traumatic encephalopathy (CTE) is the term given to posttraumatic degenera-tion of the brain after repeated concussions. Prominent clinical features include demen-tia, personality change, emotional disorders (especially depression) and movement dis-orders. The latent period post-concussion is usually decades, but some cases have shorter latent periods. The brain degeneration is a specific type of tauopathy with abnormal de-position of tau protein in neurons leading to functional loss, neuron destruction and neu-rofibrillary tangles. Although CTE shares several neuropathological features with Al-zheimer’s disease, it appears to be a distinct entity9. There are still many unknowns about CTE, which was first described in boxers in 19287. The Canadian Sport Concussion Proj-ect centered at the Toronto Western Hospital reported in a media release in 2011 that CTE was present in two of the first four brains ex-amined of Canadian Football League players who had willed their brains to the project. Although all four sustained multiple concus-sions in football, only two had CTE, and thus further research on CTE is required. Howev-er, it is clear that CTE is not confined to box-ers, and has now been identified in a variety of athletes with repeated concussions includ-ing football, hockey and soccer players.
Although concussions are being recognized more accurately and management has im-proved, there is a need for continuing edu-cation of health care professionals and the public. There are major shortcomings in our knowledge about the acute and chronic phases of single and repetitive concussions. Further research is needed to elucidate bio-markers of concussion based on imaging, neuropsychology, electrophysiology and ge-netics for the acute and chronic stages.
Anim
atio
n st
ills
prov
ided
by
Paul
Kel
ly
Research in injury biomechanics suggests ro-tational acceleration causes brain tissue defor-mation. Movements at the neck, and anchoring structures within the braincase will produce rotational acceleration of the brain even from a linear impact force.
Conclusions
1. Ackery A, Provvidenza C, Tator CH: Concussion in hockey: compliance with return to play advice and follow-up status. Can J Neurol Sci 36:207-212, 20092. Echlin PS, Tator CH, Cusimano MD, Cantu RC, Taunton JE, Upshur RE, et al: Return to play after an initial or recurrent con-cussion in a prospective study of physician-observed junior ice hockey concussions: implications for return to play after a con-cussion. Neurosurg Focus 29:E5, 20103. Echlin PS, Tator CH, Cusimano MD, Cantu RC, Taunton JE, Upshur RE, et al: A prospective study of physician-observed concussions during junior ice hockey: implications for incidence rates. Neurosurg Focus 29:E4, 20104. Gessel LM, Fields SK, Collins CL, Dick RW, Comstock RD: Concussions among United States high school and collegiate athletes. J Athl Train 42:495-503, 20075. Guskiewicz KM, McCrea M, Marshall SW, Cantu RC, Ran-dolph C, Barr W, et al: Cumulative effects associated with recur-rent concussion in collegiate football players: the NCAA Con-cussion Study. Jama 290:2549-2555, 20036. Kristman VL, Tator CH, Kreiger N, Richards D, Mainwaring L, Jaglal S, et al: Does the apolipoprotein epsilon 4 allele predis-pose varsity athletes to concussion? A prospective cohort study. Clin J Sport Med 18:322-328, 20087. Martland HS: Punch drunk. JAMA 91:1103-1107, 19288. McCrory P, Meeuwisse W, Johnston K, Dvorak J, Aubry M, Molloy M, et al: Consensus Statement on Concussion in Sport: the 3rd International Conference on Concussion in Sport held in Zurich, November 2008. Br J Sports Med 43 Suppl 1:i76-90, 20099. McKee AC, Cantu RC, Nowinski CJ, Hedley-Whyte ET, Ga-vett BE, Budson AE, et al: Chronic traumatic encephalopathy in athletes: progressive tauopathy after repetitive head injury. J Neuropathol Exp Neurol 68:709-735, 200910. Tator CH: Let’s standardize the definition of concussion and get reliable incidence data. Can J Neurol Sci 36:405-406, 200911. Tator CH: Spinal Cord and Brain Injuries in Ice Hockey, in Bailes JE, Day AL (eds): Neurological Sports Medicine: A guide for Physicians and Athletic Trainers. Rolling Meadows, Ill.: American Association of Neurological Surgeons, 2001, pp 261-27112. Wetjen NM, Pichelmann MA, Atkinson JL: Second impact syndrome: concussion and second injury brain complications. J Am Coll Surg 211:553-557
References
Brain Degeneration Related to Concussions

IMS MAGAZINE WINTER 2012 SPORTS-RELATED INJURIES | 16
FEATURE
ports related concussions are a hot topic in public health circles. The increased prevalence of these inju-
ries has prompted a call for action; however, identifying the most effective strategy for re-ducing the negative consequences associated with concussions is an extremely complex matter. Concussions result from head inju-ries, which are an inherent risk in any sport that incorporates physical contact. While it is impossible to eliminate head injuries in sports without altering the fundamentals of the game, it is possible to significantly reduce the morbidity and mortality associated with these injuries. With proper diagnosis and treatment of concussions and established protocols for returning to play, we can sig-nificantly improve health outcomes.
Recognizing this opportunity to improve health outcomes for those who sustain sports-related concussions, several states within the USA have enacted concussion laws that require 1) ample education on con-cussions for players, coaches, and parents, 2) appropriate documentation after each inci-dent, and 3) official medical clearance before the athlete is returned to play after a suspect-ed or diagnosed concussion.
In theory, these laws will protect players and improve health outcomes, and they offer a logical approach to how we should proceed in Canada. In fact, a similar bill was re-cently proposed in British Columbia. How-ever, there are significant unintended con-sequences that must be better understood before implementing such laws.
It is important to consider how such a law will impact opportunities for, and involve-ment in, physical activity. The increased pa-
perwork associated with the law is frequently cited as a disincentive for volunteer coaches to organize sports, thereby potentially re-ducing the already limited opportunities for youth and children to be physically active. In addition, the educational component of the law may induce fear and deter parents from enrolling their children in team sports. In Canada, where more than 1 in 4 children are overweight or obese, it would be irrespon-sible to implement such a law without fully understanding its effects on physical activity.
Additionally, given that Public Health re-sources are extremely limited, allocating financial and human capital towards the development of a law should only be un-dertaken if there is evidence of its cost-ef-fectiveness. With numerous other initiatives being pursued by Public Health profession-als, appropriate allocation of resources is a complex and controversial matter. In a talk at the Harvard School of Public Health, Dr. Lauren Smith, Medical Director of the Mas-sachusetts Department of Public Health and a key player in the Massachusetts concussion law, stressed the challenges of developing the State regulation without additional funding.
The impact of sports related concussions is too profound and pervasive to ignore. Can-ada will have the benefit of learning from states like Massachusetts and New York, both of which have enacted concussion laws within the last two years. Until the effects of these laws are understood, however, it might be premature to jump on the concussion law bandwagon.
Law Implementation for Concussion Diagnosisand Treatment:
A Public Health Perspective
S
Disclaimer: The opinions expressed by the author(s) are in no way affiliated with the Institute of Medical Science or the Uni-versity of Toronto. Comments are welcome at [email protected].
By Adam Santoro and Sherene Chinfatt

17 | IMS MAGAZINE WINTER 2012 SPORTS-RELATED INJURIES
FEATURE
line. Persistent vertigo continued to plague Morey, as his symptoms were exacerbated under exertion, costing him critical days of competition, as well as the new coaching staff ’s confidence in him. He was cut from the roster at the end of training camp.
The short- and long-term consequences of multiple concussive incidents (also referred to as mild traumatic brain injuries) and sub-concussive incidents have received increased media attention amid reports of depression and dementia in retired athletes. These is-sues are recognized prominently in former boxers, wrestlers, football and hockey play-ers, and others who sustain repetitive head injuries. Chronic traumatic encephalopathy (CTE) is a progressive, degenerative disease that is characterized by the accumulation of tau protein in the brain. Years after retire-ment, these athletes may experience head-aches, confusion, memory problems, irrita-bility and aggressiveness, anxiety, depression, and other neurobehavioural manifestations.
Sean Morey, now retired from the NFL, is a member of the NFL Player’s Association
(NFLPA) elected Executive Committee. He also co-chaired the Mackey-White Traumatic Brain Injury Committee until stepping down recently. After being advised to retire imme-diately before the 2010 season as the result of post-concussion syndrome, Morey has remained committed to advocating for the health, safety, and welfare of the NFL play-ers he represents. “We have commissioned a team of independent neurological experts to help our players interpret the science, so that they may be afforded the opportunity to make informed decisions about the risks they assume moving forward.”
Informed consent is the crux of the issue. Be-yond the later-life risk of developing symp-toms of brain damage or CTE, players risk shortening their seasons or careers through the more immediate, debilitating symptoms of post-concussion syndrome. Morey warns, “We’d like to convince players that it’s no longer a badge of courage or loyalty to play through a concussion, but rather reckless and selfish. [You] increase the risk of suffering prolonged symptoms, delaying your recov-ery, and you won’t be there when your team
n the second year of his NFL career, Sean Morey remembers knock-ing himself unconscious during a
one-on-one tackling drill in practice. “It was probably the worst concussion of my career,” he explains. “I hit him as hard as I could—I knocked myself out cold.” While the train-ers took his helmet away and had to hide it to prevent him from rejoining practice, he was later able to convince them that he was perfectly alright. “I practiced that afternoon,” Morey recalls. The next morning, however, he remembers waking up, falling over getting dressed, being unable to balance his tray at breakfast, and could not even jog in a straight
IPh
otos
cou
rtesy
of S
ean
Mor
ey
Get your head in the game:
By Jennifer Rilstone
NFL player Sean Morey discusses his personal struggle with concussions and his strong advocacy for athlete safety.
a player’s perspective

IMS MAGAZINE WINTER 2012 SPORTS-RELATED INJURIES | 18
Sean Morey was a Pro Bowl Special Teams Player of the Decade who captained the Super Bowl XL Champion Pitts-burgh Steelers and 2008 NFC Champion Arizona Cardinals. He graduated with honors from Brown University as an All-American Wide Receiver, and is the only athlete in the history of Brown to have their jersey retired, #24. See p.5 for some of Morey’s work as part of the Mackey-White TBI Committee.
needs you the most down the stretch, and go-ing into the playoffs.” The NFLPA has worked hard to help players understand the inherent risks, recognize their symptoms, and manage their injuries properly, while also looking out for their teammates. Of his own experience, Morey tells, “I know what it takes to win in the NFL, and I just couldn’t hit anymore without getting hurt. Experts advised me to retire, and I felt my only option was dis-closing that to the team.” Had he not walked away, he felt he would have had to change the way he played the game, taken a roster spot from somebody else, or become a liability to the team. “We understand player’s competi-tive interests; they want to win,” he says, “but in the end, you don’t want these players to sacrifice more than what their families are willing to let them.”
This change in perspective is an important complement to the rule changes that have been instituted in the NFL over the past few years, such as the defenseless player rule. “What experts are starting to understand is that the mechanism of injury is not direct force, but unexpected shock to the head and rotational acceleration causing twisting and shearing of axons,” Morey clarifies. “Essen-tially, the goal of the rule is to eliminate initi-ating contact with the crown of your helmet on defenseless players.” Without inhibiting a coach’s ability to gain a competitive advan-tage, the NFL has also limited the exposure to hitting in practice. By changing the way they prepare to play the game, the league reduces the cumulative impacts sustained by linemen. Finally, while modern helmets are optimized for linear impact—to reduce the risks of sub-dural hematoma and skull fracture—a recent study showed that the older style, leather hel-mets are actually better at transferring energy from smaller, concussive impacts. “Players have been given a false sense of security from the perceived innovation in helmet design,” Morey explains. “When concussions were only considered a transient injury, players felt invulnerable because it hurts less to lead with your head.”
The ability to educate players at the profes-sional level comes down to expanding re-search efforts to better define risk factors and the mechanisms underlying concussive processes. “Every injury is unique and differ-ent, and every player and how they recover from concussion is unique and different. The
variability between athletes makes it utterly impossible to generalize,” Morey says. “Can we quantify the incremental risk of further impacts, as players try to extend their ca-reers? How do we advise players to recover after concussions to interrupt processes lead-ing to long-term damage?” The downstream consequences of repetitive brain trauma are still poorly understood. Do clinical symp-toms arise when players who have sustained repetitive brain trauma reach a critical limit of functioning neurons as they age? Or is this a neurodegenerative, necrotic disease pro-cess that manifests in dementia? In terms of athletes in the later stages of their career and those who are retired, research needs to ad-dress early diagnosis and treatment of CTE. At present, conclusive diagnosis is limited to post-mortem pathology. Early diagnosis is critical to being able to intervene, delay, or prevent the onset of dementia in those who may be at risk. Beyond the borders of athletics, post-concussion syndrome is now considered a signature injury of the Iraq war, so the impetus for addressing these questions is even greater. “I think that sport provides a great environment to understand the injury recovery process and the best practices for treating the post-concussion syndrome ex-perienced by our returning soldiers.”
Informed consent is a realistic criterion for professional athletes, but Morey is also very concerned with the risk associated with concussions in youth athletes. Children and teenagers, as minors, are not qualified to provide informed consent to play. “Sport has evolved. Kids are becoming more specialized and one-dimensional in their sport at a young age. What is the cumulative, compounding effect of repetitive brain trauma sustained over a lifetime for a child who starts playing football at age 6? How young can we expose our kids to brain injury?” In this vulnerable group, it is the role of coaches, parents, and educators to protect children from the po-tential downstream consequences of contact sport. This involves a combination of rule changes, changing the goals of practice, and educating coaches, parents, and educators to develop a holistic model for managing con-cussions properly, so that kids can return to the sport when their injury has healed. For young players, research still needs to address the particular vulnerabilities of the develop-ing brain, and furthermore, how brain trau-ma interferes with critical windows of neural
FEATURE
development. Should there be more conser-vative return to play guidelines for younger kids, especially considering the increased risk of second impact syndrome in develop-ing brains? “Sport was intended to enrich the lives of student athletes. We need to keep this issue in proper perspective, recognizing that there are risks, but also understanding and appreciating the valuable experience that competitive sports have on the development of our youth.”
While some may question the value of play-ing a high impact sport at all, Morey speaks highly of his own NFL experience: “It’s hard to articulate the range of emotions you expe-rience playing in the NFL. There’s a constant pendulum of elation and despair, but it also provides a platform to demonstrate cour-age and loyalty, resiliency, leadership and teamwork, and you play for something big-ger than yourself. There’s nothing you can do to recreate that.” Morey summarizes, “We’ll never take the risk out of playing football, but we have to make a more concerted effort to reduce the risk and prioritize players’ health, safety, and welfare as we move forward. Edu-cate them, inform them, try to protect them, and inspire them to protect each other, and you can still have a very competitive game for decades to come.”

19 | IMS MAGAZINE WINTER 2012 SPORTS-RELATED INJURIES
FEATURE
Dr. David CadotteMD, PhD Candidate
Supervisor: Dr. Michael Fehlings
he spinal cord is responsible for integrating and transmitting a vast amount of sensory information
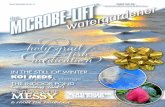
from the environment to the brain and for transmitting signals of motor activity from the brain to the body. When an individual sustains a spinal cord injury, this flow of in-formation is abruptly altered and can have devastating consequences. Take for example the case illustrated in Figure 1 that shows a mid-sagittal MRI picture of a 40-year-old male who sustained a spinal cord injury while diving in a lake. Unfortunately, this in-dividual lost the ability to move both his legs and the majority of his arms. He also lost the ability to perceive sensation (touch, vibra-tion, heat) on most of his body. The arrow in Figure 1 points to the specific area of the spinal cord that was damaged in the accident. This is a typical case of traumatic spinal cord injury; it often happens to relatively young, healthy adults who are in the prime of their life. Within the time span of a few seconds, whether it is from a diving accident, sports injury or otherwise, a person’s life can change forever.
The central nervous system, composed of the brain and spinal cord, is a fascinating part of the human body. After it is injured it contin-ues to change and adapt to its new environ-
ment. Reorganization of the spinal cord after traumatic injury is clinically evident along a spectrum of changes. We term these changes either adaptive plasticity – whereby an indi-vidual can regain some or all of both motor and sensory function; and maladaptive plas-ticity – whereby an individual, in addition to losing motor and sensory abilities, can develop spasticity (where muscles contract involuntarily) and neuropathic pain (where pain is present without a typical cause). Our research group, led by Dr. Michael Fehlings at the Toronto Western Hospital, is devel-oping novel spinal functional MRI technol-ogy (fMRI) to study how these populations of neurons change over time. Eventually, we hope to use this technology to study the ef-fect of different treatment options on the function of cells in the spinal cord.
To do this, we activate specific populations of neurons in the spinal cord over a 7-minute period while acquiring a series of MRI pic-tures. For example, to study the cells of the spinal cord that are responsible for transmit-ting temperature information from the envi-ronment to the brain (via the spinothalamic tract in the spinal cord), we apply a mild heat stimulus to the skin in an ‘on’ and ‘off ’ pat-tern. By carefully analyzing the MRI data rel-ative to the ‘on’ and ‘off ’ periods, we are able to tell if the cells of interest are functional or not. By applying different stimulation para-digms, we can test different cell populations of the spinal cord.
For example, we are able to test the motor neurons of the spinal cord by having an indi-vidual move their finger. In the case of spinal cord injury, where an individual may not be able to move their finger, we are testing a de-vice that will passively move it for them. One way that we display these results is shown in Figure 2, where a grey silhouette of the brain-stem and spinal cord is seen with superim-posed coloured lines. This figure was gener-ated by applying heat stimulation to the hand of a healthy 32-year-old volunteer; we then correlated the activity in the hand region of the spinal cord to other regions of the brain-stem known to receive information from the Ph
oto
by P
aulin
a Rz
eczk
owsk
a. F
igur
e im
ages
cou
rtesy
of D
r. Ca
dotte
.
T
Imaging and spinal cord injuries

IMS MAGAZINE WINTER 2012 SPORTS-RELATED INJURIES | 20
FEATURE
dorsal horn of the spinal cord. In this way, we can infer how the spinal cord and brainstem work together to transmit information to the brain.
Spinal fMRI has overcome major techno-logical hurdles in recent years. While these results are extremely exciting, we have a lot of work to do before we can use spinal fMRI technology to determine circuit reorganiza-tion in the setting of spinal cord injury. We have just finished conducting the world’s largest clinical trial comparing healthy indi-viduals to chronic spinal cord injury patients as a joint venture between Dr. Patrick Stro-man’s laboratory at Queens University and Dr. Michael Fehlings’ laboratory at the Uni-versity of Toronto. The results of this study will serve as a platform to refine our methods with the ultimate goal of helping people re-gain the ability to walk, use their arms, and restore the ability to perceive sensation from their environment.
Figure 1. A mid-sagittal T2 weighted MRI of a 40 year-old individual who sustained a diving accident. The white arrow points to the damaged area of the spinal cord that resulted in loss of his ability to move his legs, most of his arms, and a loss of sensation over the majority of his body.
Figure 2. A spinal fMRI connectivity analysis gen-erated from heating the skin of a healthy 32-year-old’s hand and correlating the activity observed in the spinal cord to other regions of the brainstem. From this activity map, we can infer how the spinal cord and brainstem are working together to transmit information to the brain.
Difficulty focusing on everyday tasks is a hallmark consequence of traumatic brain injury (TBI). These impairments in sustained attention are potentially caused by disruption of a set of regions along the brain’s midline known as the “default mode net-work.” This network is activated during periods of mind wandering and self-focus, but deactivated during cognitive task performance.
In a recently published Journal of Neuroscience study, the structure and function of the default mode network was investigated in 28 patients with TBIs. Functional MRI scans were performed while these patients completed cognitive tasks requiring continued attention over long periods
A column by Aaron Kucyi
Pick Your Brain...of time. TBI patients underperformed compared to non-injured subjects and showed an abnormal pattern of activity in the default mode network during the early phases of the task. The more ir-regular the pattern, the more likely a patient had difficulty maintaining attention over the course of the task. Additionally, diffusion MRI images of patients with the most severe attentional deficits showed increased abnormal structural connectiv-ity within the default mode network when com-pared to those with lesser impairments and those without injuries.
These findings provide important insight into how brain injuries can result in impairments in atten-
tion. Although previous studies of TBI have largely focused on brain regions outside the default mode network, this study puts forward a strong impetus for further investigation of this network as a po-tential target for neuro-rehabilitative strategies.
Reference:Bonnelle V, Leech R, Kinnunen KM, Ham TE, Beckmann CF, De Boissezon X, Greenwood RJ, Sharp DJ (2011) Default mode network connectivity predicts sustained attention deficits after traumatic brain injury. J Neurosci 31(38):13442-13451.

21 | IMS MAGAZINE WINTER 2012 SPORTS-RELATED INJURIES
FEATURE
espite sustaining devastating spinal cord injuries that left him paralyzed from the waist down,
Rick Hansen used drive and determination to wheel himself through 34 countries in 26 months to complete his now-famous Man In Motion World Tour 25 years ago. He sought to raise awareness of the physical potential of people with disabilities, accelerate prog-ress in building inclusive communities, and achieve breakthroughs in spinal cord injury (SCI) research.
This 25th anniversary of the amazing Rick Hansen Man in Motion Tour makes one reflect on the magnitude of what can be ac-complished given the right circumstances following catastrophic neurotrauma. For health professionals in particular, it is a time to reflect on the secondary consequences and complications in individuals following spinal cord injury (SCI), how these sequelae persist throughout patients’ lives, and how essential rehabilitative care is to improving their phys-ical outcomes. In Ontario, approximately 250 individuals will sustain a traumatic spinal cord injury each year1. Significantly, 22% of these injuries are related to sports and recre-ation accidents, with the largest proportion involving all-terrain vehicles and cycling2. In these cases, medical and rehabilitative care is most often funded exclusively by the public health care system, making efficient delivery of treatment crucial in this fiscal climate.
Phot
os c
ourte
sy o
f Mol
ly V
errie
r
D
Secondary Complications in Traumatic Spinal Cord Injury and Rehabilitation Research
“...it is a time to reflect on the secondary consequences and complications in indi-viduals following spinal cord injury, how these sequelae persist throughout patients’ lives, and how essential reha-bilitative care is to improving their physical outcomes.”
By Molly Verrier
Verrier’s IMS PhD student, Sharon Gabison, uses ultrasound imaging data in conjunction with other measures to better under-stand why some spinal cord injury patients develop pressure ulcers.

IMS MAGAZINE WINTER 2012 SPORTS-RELATED INJURIES | 22
FEATURE
eral density in the knee and hip regions in the first 12-18 months following a complete motor injury. Toronto Rehab’s Bone Density Laboratory currently provides a high-quality diagnostic, clinical and research laboratory3; here, Dr. Catharine Craven and collaborator Dr. Lora Giangregorio have developed a site-specific procedure around the knee to detect fractures using Peripheral Quantitative Com-puted Tomography (pQCT), a diagnostic technique that measures bone structure and volumetric Bone Mineral Density (vBMD in g/cm3). pQCT can assess lower limb sites with no need to transfer from a wheelchair, and it provides more information about bone strength indices in only 1-2 scans and at a lower radiation dose than similar DXA scans, another means of measuring bone mineral density. Their research compares the diag-nostic utility of DXA to pQCT for the SCI population.
Toronto Rehab’s Senior Scientist Molly Ver-rier—along with Drs. Nussbaum, Mathur, Popovic and Sharon Gabison, a physical therapist and PhD student in the Institute of Medical Science—are using a new methodol-ogy to assess deep tissue injury using ultra-sound imaging to predict whether an indi-vidual is prone to developing ischial PUs4.
In addition, a novel method is being investi-gated for oxygenating tissue using functional electrical stimulation and a custom-designed feedback device—the SensiMat, designed by Dr. Popovic. Specifically, the goal of this device is to determine temporal behavioural patterns of the much required pressure relief for weight bearing surfaces involved in sitting in the sub-acute phase post SCI. Individuals with SCI experience PUs as compromised mobility and sensation, and reduced body awarenessvv increases trauma risk of weight bearing tissues. Unfortunately, limited stud-ies have characterized the health of weight bearing tissues and the relationship to trunk impairments in SCI. Gabison is establish-ing novel protocols for assessing individuals
Four teams of clinicians and rehabilitation researchers at the Toronto Rehabilitation In-stitute—Lyndhurst SCI Centre, part of the University Health Network and U of T Aca-demic Health Science Complex, are focused on minimizing the secondary complications that limit optimal health, well-being, and full participation in life for people with varying degrees of SCI. These integrated teams of physiatrists, physical therapists, occupational therapists, nurses, rehabilitation engineers, as well as other health professionals are fo-cussing on:
Altered body composition after SCI pres-ents significant health risks. Typical changes in body composition include monthly bone mass reductions of 3-4% post-injury, de-creased lean muscle mass of up to 45-80% in the chronic SCI population, and increased fat mass, which contributes to the development of several disease states. In particular, the increase in fat mass can impact sublesional osteoporosis and sublesional fragility frac-tures with a prevalence of 25-26%, and pres-sure ulcers (PUs) with a prevalence of 50%. Overall, these risks can result in significant morbidity, mortality, reduction in quality of life and productivity, and extensive health care utilization over a lifetime.
Toronto Rehab scientists have therefore placed a particular emphasis on optimizing physical activity and mobility with the goal of minimizing secondary complications, such as the reported decline in bone min-
1. Couris CM, Guilcher SJT, Munce SEP, Fung K, Cra-ven BC, Verrier M, Jaglal SB. Characteristics of adults with incident traumatic spinal cord injury in Ontario, Canada. Spinal Cord 2010; 48: 39-44.2. Verrier M, Ahn H, Craven C, Drew B, Fehlings M, Ford M, et al. Ontario spinal cord injury informatics: informing practice, research and innovations. Ontario Neurotrauma Foundation. November 2009; [cited 2011 October 24]. Available at http://www.onf.org/docu-ments/OSCIR.pdf. 3. Craven BC, Robertson LA, McGillivray CF, Adachi JD. Detection and Treatment of Sublesional Osteopo-rosis Among Patients with Chronic Spinal Cord Inju-ry: Proposed Paradigms. Top Spinal Cord Inj Rehabil. 2009;14(4):1-22.4. Gabison S Verrier M.C Nussbaum E Popovic, M.R Mathur, S. A Method to Determine the Relationship of Trunk Postural Control, Tissue Integrity and Pressure Ulcers in Spinal Cord Injury (SCI).Toronto Rehabilita-tion Institute; 7th Annual Research Day Conference Ab-stracts November 2011; p 47.
References
with SCI using data from ultrasound imag-ing, erythema indexing, skin temperature, and sensitivity testing collected over the is-chial tuberosities. These data are collected at 3 time points: at admission, 1 week prior to discharge, and 4 months post-discharge from rehabilitation. This information can be used to develop a predictive capacity to determine which patients are at risk for developing PUs. High frequency ultrasound scanning has the ability to evaluate skin thickness, muscle size and quality, spatial orientation of blood ves-sels, identification of areas of calcification, necrosis, and changes in inflammation over time.
Verrier is assessing patients’ mobility and postural control in both Popovic’s Rehabilita-tion Engineering Laboratory and the clinical setting during rehabilitation. Scanning mus-cle morphology and soft tissue integrity to non-invasively assess healing in damaged tis-sue is suitable for the research laboratory and clinical use at the bedside. Both approaches enable the research to be translational from the start.
Techno-Behavioral Approaches for En-hanced Recovery and Minimization of Secondary Complications
Evolving Technologies, Assessments and Practice Innovations
SCI Health Services Research and SCI In-formatics
Single/Multi-Site SCI Clinical Trials and Interventional Studies

23 | IMS MAGAZINE WINTER 2012 SPORTS-RELATED INJURIES
Phot
o by
Lau
ra F
eldc
amp
SPOTLIGHT
Dr. Anne Agur BSc (OT), MSc, PhD
written materials and help with 3D learning when dissections or prosected specimen are unavailable. Students find her unique teach-ing style for anatomy inspirational. Indeed, many become so inspired that they decide to conduct projects under her supervision. Some even created a Facebook group “in ap-preciation of all things Anne” to honour their mentor.
In addition to her teaching contributions, Agur also conducts highly innovative re-search as a member and founder of the Mus-culoskeletal Anatomy Laboratory. While she supervises both basic and clinical research projects, her most unique studies involve digital modeling of muscle structure and function. By developing models capable of mimicking human muscle, her research has accomplished what others have been unable to do: depict entire muscles in 3D, from fibre bundles to blood supply. One of Agur’s ob-jectives is to conduct basic research that can be applied clinically: “From the mathemati-cal end, you can look at modeling in normal subjects, then eventually look at pathological models, but you need to understand what the normal structure is before you can apply it to pathology.” She also highlighted the im-portance of collaborations with her peers in computer science, engineering and medical imaging as being essential in expanding our understanding of anatomy.
Agur is known worldwide for her contribu-tions to anatomical literature. She is current-ly the President of the American Association of Clinical Anatomists and has been an edi-tor for Grant’s Atlas of Anatomy since 1991. She has co-authored two textbooks, Essential Clinical Anatomy (1995, 2002, 2007, & 2011) and Clinically Oriented Anatomy (2010) with Professor Emeritus K.L. Moore. These books have been translated into numerous languag-es and adopted internationally by both stu-dents and medical professionals.
Considering her many successes, I asked Dr. Agur to explain her greatest accomplishment to date: “I have been able to balance work and family and be happy with both.” Her enthu-siasm, dedication and passion for anatomy are second to none: “Since 1978, I have come to work everyday with a smile on my face—I love what I do!”
or over 30 years, Dr. Anne Agur has been doing what many consider a challenging task: she has been
making anatomy exciting. Whether lecturing in classrooms, demonstrating dissections or mentoring trainees, Agur’s passion for anato-my is not only apparent, it is contagious.
As a Professor in the University of Toronto’s Department of Surgery (Division of Anato-my), a graduate faculty member in the IMS and the Graduate Departments of Rehabili-tation Science and Dentistry, and a cross-ap-pointed faculty member in the Departments of Occupational Therapy, Physical Therapy and Biomedical Communications, Agur en-thusiastically teaches hundreds of students each year. When she is not lecturing on gross anatomy, histology, neuroanatomy and em-bryology, she spends her time facilitating hands-on laboratory sessions and supervis-ing graduate students, medical residents and fellows.
Although she initially planned for a career in occupational therapy (OT), Agur’s inter-est in anatomy led her in a different direc-
tion. During the course of her undergradu-ate OT training, she greatly enjoyed the basic sciences, especially the functional aspects of anatomy. With the guidance of her mentors, she enrolled in the Master’s program in the Department of Anatomy under the supervi-sion of Dr. Ian Taylor and then much later completed a doctorate degree in the IMS, supervised by Dr. Nancy McKee. While com-pleting her Master’s work, Agur was hired by the university as a Lecturer and quickly earned numerous awards for her outstanding teaching abilities.
In collaboration with her colleague Professor Pat McKee, Agur recently developed an edu-cational tool that allows individuals to learn anatomical structures by personally relating them to their own bodies. Specifically, learn-ers use a covering or an “envelope,” placed over their own body area to draw the corre-sponding structures underneath their skin. To study hand anatomy, for example, a fabric glove depicting the bones of the human hand is used as a guide to draw internal structures such as nerves, muscles, and tendons. This alternative learning tool can supplement
F
By Danielle DeSouza
FACULTY VIEW

24IMS MAGAZINE WINTER 2012 SPORTS-RELATED INJURIES |
SPOTLIGHT
Tiziana VolpeThe convergence of art and science
STREAM PhDSUPERVISOR Dr. Katherine Boydell
“I thought it would give me the knowledge that I could not get through more traditional qualitative methods,” she states.
Under the supervision of Dr. Katherine Boy-dell, Volpe investigated the experiences of young people who were identified as being at ultra-high risk for psychosis. Using a tech-nique called “photo elicitation,” she studied the manner in which five participants con-structed and interpreted their daily experi-ences through photographs. She was also interested in understanding the effects of being labeled with a potential mental health condition.
“We found that young people reject their at-risk status and redefine their experiences to fit with more acceptable and familiar notions of health. Participants are also conscious of the stigma associated with psychosis and actively undertake strategies of resistance to avoid stigmatization and uphold a normal self-conception and social impression,” she explains.
The novelty of Volpe’s research and other arts-based qualitative studies lies in the ac-tive involvement of participants in the re-search process, which includes study design, data collection, analysis, and dissemination strategies. This allows for the investigation of emotional aspects of patient experiences in an inclusive manner.
“It’s not research on young people, but rather research with young people,” Volpe states.
Arts-based qualitative research provides an exciting new lens into facets of people’s ill-ness experiences that cannot be quantitative-ly described. The field is expanding rapidly with the emergence of new methods such as the use of dance, visual art and video tech-nology to capture experiences that serve as data for research as well as knowledge trans-lation and exchange activities. Volpe and her team at The Hospital for Sick Children are collaborating with researchers around the world to further explore the application and ethics of arts-based approaches to health re-search. This revolutionary research method offers great promise for facilitating diagno-ses, monitoring, and intervention in numer-ous health fields.
iziana Volpe, a recent IMS PhD graduate, is part of an innovative new movement that promotes the
use of art to analyze scientific phenomena. This arts-based qualitative approach is gain-ing momentum and is applied increasingly to health research worldwide. Volpe combines two of her life passions in her work; she uses photography to investigate young people’s experiences with mental health.
Volpe first became interested in understand-ing mental health when she worked with
T schizophrenia patients as a research assistant. This experience inspired her to pursue a Mas-ter’s degree in Social Science and Medicine, during which she studied attention-deficit/hyperactivity disorder (ADHD) from the perspective of adolescents diagnosed with the disorder. Shortly thereafter, upon starting her PhD at the Institute of Medical Science Volpe sought a more innovative method to delve into the experiences of young people in mental health settings. She found this ap-proach in photography, one of her lifelong hobbies.
By Meghna Rajaprakash Phot
o by
Lau
ra F
eldc
amp

25 | IMS MAGAZINE WINTER 2012 SPORTS-RELATED INJURIES
EXPERT OPINION
Surgical Management of ObesityEarly bariatric operations from the 1950s, termed jejunocolic and jejunoileal bypasses, worked based on a principle of malabsorp-tion. Patients experienced substantial weight loss, but there were very high rates of post-operative complications including liver and/or renal failure, severe infections, and nu-tritional impairments7. Modern bariatric surgeries are divided into restrictive, malab-sorptive and combined procedures. Gastric banding, sleeve gastrectomy and vertical banded gastroplasty fall into the first cat-egory while biliopancreatic diversion with or without duodenal switch fall into the sec-ond. Roux-en-Y gastric bypass is considered a combined technique. Percent excess weight loss and mortality data for each type of pro-cedure are listed in Table 1.
Prior to today’s minimally invasive surgical techniques, access to the abdominal cav-ity was achieved through a large abdominal incision. This often resulted in elevated rates of surgical site infections, incisional hernias and respiratory complications. Laparoscopic techniques, where probes with cameras and/or lights on the ends are guided into the ab-dominal cavity through small incisions, af-ford patients better scar healing, reduced blood loss and infection rates, shorter hos-pitalization times, and less post-operative pain8,9. Several randomized control studies have confirmed similar mortality rates with both open and laparoscopic approaches, with
besity is defined by a body mass index (BMI) of 30kg/m2 or greater. It is a serious public health concern
not only in Canada, but also in many other developed countries of the world. Morbid obesity (BMI > 40) is associated with early mortality, type 2 diabetes, hypertension, heart disease, cerebrovascular disease, mus-culoskeletal disorders, and certain types of cancers. A recent review found that for ev-ery five-point increase in BMI over 25kg/m2, there was a 30% increase in overall mortal-ity1. According to the World Health Organi-zation, in 2008 there were approximately 200 million obese men and nearly 300 million obese women worldwide2. In Canada, the self-reported rate of adult obesity was 17% in 20073, with obesity-related chronic condi-tions costing our system approximately $4.3 billion annually3.
Exercise, diet, lifestyle modifications and pharmaceutical agents comprise the first line of treatment for obesity; however, these in-terventions are often not effective in achiev-ing sustained weight loss4. Bariatric (weight loss) surgery is the only treatment with prov-en long-term weight loss results5. Such radi-cal treatment is indicated in individuals with a BMI over 40 kg/m2, or a BMI over 35 kg/m2 if comorbidities are present6.
By Dr. Teodor P. Grantcharov (above) and Dr. Boris Zevin O
Phot
o by
Lau
ra F
eldc
amp,
Imag
es c
ourte
sy o
f Dr.
Teod
or G
rant
char
ov
Figure 1: The above photo depicts the sleeve gastrec-tomy procedure.

26IMS MAGAZINE WINTER 2012 SPORTS-RELATED INJURIES |
all but two attained normalized glucose levels within ten days of surgery10. In a follow-up study, 83% of patients with pre-operative type 2 diabetes and 99% of those with impaired glucose tolerance were able to maintain nor-mal levels of plasma glucose and insulin eight years after surgery11. In the Swedish Obese Subjects study, 72% of surgically treated pa-tients were no longer considered diabetic two years after surgery, compared to 21% of controls. Remarkably, after eight years, the prevalence of diabetes in the surgical group remained relatively stable, compared to an increase within the control group12. Several studies have shown a significant reduction in dangerous, low-density lipoprotein and tri-glycerides complemented with an increase in good, high-density lipoprotein after bariatric surgery13-15.
While every surgical procedure carries some level of risk, today’s bariatric interventions are shown to have fewer and less severe post-operative complications than prior surgical techniques. Bariatric surgery also provides significant and sustained weight loss and reduces the rates of dangerous comorbidi-ties; considering these factors, it is clear that bariatric surgery is an effective treatment for morbid obesity.
similar effectiveness in providing weight loss and reducing medical comorbidities8,9. As a result, the laparoscopic method has become the gold standard in bariatric surgical inter-vention.
In addition to providing significant weight loss, bariatric surgery also results in improve-ment of previous medical comorbidities such as obstructive sleep apnea, type 2 diabetes and dyslipidemia. A study by Buchwald et al. found that 85.7% of treated patients in their cohort saw resolution of obstructive sleep apnea5. In a separate study of 141 patients with diabetes or impaired glucose tolerance that underwent a Roux-en-Y gastric bypass,
References1. Whitlock G, Lewington S, Sherliker P, et al. Lancet 2009; 373:1083–96.2. World Health Organization. Obesity and overweight. Fact sheet N°311. Accessed on October 7, 2011 http://www.who.int/mediacentre/factsheets/fs311/en/ 3. Obesity in Canada – Snapshot. Accessed on October 7, 2011 http://www.phac-aspc.gc.ca4. The practical guide: Identification, evaluation, and treatment of overweight and obesity in adults. US De-partment of Health and Human Service, National In-
EXPERT OPINION
stitute of Health; National Heart, Lung, and Blood In-stitute; North American Association for the Study of Obesity. NIH Publication Number 00-4084 2000 (http://www.nhlbi.nih.gov/guidelines/obesity/prctgd_c.pdf)5. Buchwald H, Avidor Y, Braunwald E, et al. JAMA 2004; 292(14):1724-37.6. National Institute for Health and Clinical Excellence. National Institute for Health and Clinical Excellence, Clinical Guideline 2006;43.7. Jaunoo SS, Southall PJ. Bariatric surgery. Int J Surg 2010; 8(2):86-9.8. Puzziferri N, Austrheim-Smith IT, Wolfe BM, et al. Ann Surg 2006; 243(2):181-8.9. Nguyen NT, Goldman C, Rosenquist CJ, et al. Ann Surg 2001; 234(3):279-89; discussion 289-91.10. Pories WJ, Caro JF, Flickinger EG, et al. Ann Surg 1987; 206(3):316-23.11. Pories WJ, Swanson MS, MacDonald KG, et al. Ann Surg 1995; 222(3):339-50; discussion 350-2.12. Sjostrom CD, Peltonen M, Wedel H, et al. Hyperten-sion 2000; 36(1):20-5.13. Bouldin MJ, Ross LA, Sumrall CD, et al. Am J Med Sci 2006; 331(4):183-93.14. Sjostrom L, Lindroos AK, Peltonen M, et al. N Engl J Med 2004; 351(26):2683-93.15. Zlabek JA, Grimm MS, Larson CJ, et al. Surg Obes Relat Dis 2005; 1(6):537-42.16. Cottam D, Qureshi FG, Mattar SG, et al. Surg Endosc 2006; 20(6):859-63.17. Akkary E, Duffy A, Bell R. Obes Surg 2008; 18(10):1323-9.18. Hess DS. Surg Obes Relat Dis 2005; 1(3):329-33.19. Buchwald H, Estok R, Fahrbach K, et al. Surgery 2007; 142(4):621-32; discussion 632-5.20. Gumbs AA, Gagner M, Dakin G, et al. Obes Surg 2007; 17(7):962-9
LAGB SG BPD+ DS RYGB
Excess weight loss
47.5% @ 2 yrs post-op5 33%-83% @ 1 yr post-op16.17 74%18 61.6%5
Mortality<30d : >30d
0.06% : 0.00%19 0.6%20 1.11% : n/a19
0.57%18 0.16% : 0.09%19
Legend: LAGB = laparoscopic adjustable gastric band; SG = sleeve gastrectomy; BPD+DS = biliopancreatic diversion with/out duodenal switch; RYGB = roux-en-y gastric bypass. Table 1: Comparison of excess weight loss and mortality for bariatric procedures.
Figure 2: The Roux-en-Y gastric bypass procedure is outlined above.

27 | IMS MAGAZINE WINTER 2012 SPORTS-RELATED INJURIES
Rebecca SklootThe Immortal Life of Henrietta Lacks
Crown, 2010; 384 pages
Book Reviews
n the multiple award-winning non-fiction book The Immortal Life of Henrietta Lacks (2010), author Rebec-
ca Skloot shares a very personal narrative of her relationship with the descendants of Henrietta Lacks—the woman whose cancer cells were cultured to create the first immor-talized human cell line. These HeLa cells, named after their unsuspecting donor, have revolutionized medical research. They un-derlie advances in vaccine development, in vitro fertilization, cloning, and gene map-ping, and they spawned an industry commit-ted to selling human biological materials. Yet the Lacks family—poor, living in Baltimore, and unable to afford healthcare—were en-tirely unaware of Henrietta’s legacy. Skloot intertwines her personal story of gaining the
Lacks family’s trust and teaching them about their mother’s cells with a broader discussion of the development of ethical guidelines for using patient tissues in medical research and industry.
For those in the medical field, Skloot’s book provides a critical human perspective on the impact that participating in a research study can have on patients and their families. The book is also a solid primer on the origins of the bioethical protocols followed today. In an interview with IMS Magazine, Rebecca Skloot discusses her personal connection to the hopes and fears of medical research, reviews the ethical issues she feels still need to be addressed, and offers advice to our re-searchers who work with tissue samples.
Rebecca Skloot first learned of HeLa cells in her community college biology class. She be-came determined to learn more about their origin and the woman from whom they were derived. “I realize now that my questions about the cells weren’t obvious ones for a sixteen-year-old to ask, but something was happening in my life that I think primed me to ask questions.” That factor was a mysteri-ous illness that incapacitated her father—an illness that turned out to be a virus that had caused brain damage. She drove her father to and from an experimental drug trial, and sat with him and other patients several times a week. “I was in the midst of watching my own father go through research and was ex-periencing the hopes that can come from sci-ence, but also the frustration and fear. It was a frightening time. The research didn’t help him, and in the end, the study was dissolved without fulfilling promises it made to the pa-tients about access to treatment. The experi-ence really taught me about the wonder and hope of science, but also the complicated and sometimes painful ways it can affect people’s lives.”
While the publication of her book has im-proved public awareness of the importance of informed consent, she points out that as-pects of tissue research ethics still have not been addressed: “Should people have [the] right to control what’s done with their tis-sues once they’re removed from their bod-ies? And who, if anyone, should profit from those tissues?” Each of the billions of sam-ples stored in tissue banks and research labs around the world come from a human being. At present, as long as the patient’s identity is removed from the sample, consent isn’t re-quired to use the leftover tissue for research. “No one wants that research to stop,” Skloot points out, “but it’s pretty clear that many people want to know when their tissues are being used in research, and when there’s a potential for the results of such research to be used commercially.”
Finally, Skloot leaves us with some advice as researchers: “At its core, [the Lacks family story] is about the importance of communi-cating scientific information to the general public, and the problems that can arise when that doesn’t happen. It’s important for clini-cians and researchers to keep that in mind as they try to get consent and explain research projects; patients are often scared in the mo-ment, and don’t read the forms or under-stand exactly what doctors say. One thing clinicians don’t often do after explaining re-search or a procedure is stop to ask patients to explain what they believe is happening to make sure they’ve actually understood it. If scientists had done that with the Lacks chil-dren before doing research on them 25 years after Henrietta’s death, a lot of confusion and trauma could have been avoided.”
Skloot is working on her next book, inspired by her experiences as a veterinary techni-cian, exploring the human-animal bond.
I
Worth missing a day at the lab Try to squeeze in between experiments Wait for the weekend Wait until degree is completeExcellent Very Good Good Average
Column by Jennifer Rilstone

28IMS MAGAZINE WINTER 2012 SPORTS-RELATED INJURIES |
What are you reading?Tetyana Pekar, year 2 MSc student, recom-mends two classic popular science books: Natural Obssessions: Striving to Unlock the Deepest Secrets of the Cancer Cell by Natalie Angier (1988, 1st ed), and The First Three Minutes: A Modern View of the Ori-gins of the Universe by Steven L. Weinberg (1977, 1st ed)
“Natural Obsessions reads like a mystery-thriller novel and indeed, it is much, much more than a typical fact-filled science book. Award-winning science writer Natalie Angier accu-rately depicts the drama and dynam-ics of a high-power lab, the intra and inter-lab competition, and the highs and lows of basic science research. The bonus: Finding what the real-life characters are up-to, 20 years later.”
“In The First Three Minutes, Nobel Laureate Steven Weinberg takes us on a journey to the birth of the Uni-verse. Written over 30 years ago, many details are surely out-dated, but that shouldn’t deter the reader: Weinberg’s masterfully addictive and cogent sto-rytelling draws you in from the start and more than makes up for it. The bo-nus: A mathematics appendix.”
Melanie Dawn Guenette, year 2 MSc student, recommends the satirical novel House of God by Samuel Shem.
“House of God is an absolutely hilari-ous parody of life as an intern. I cer-tainly couldn’t put it down and found myself literally laughing out loud imagining the scenarios depicted by Shem. An old classic and great read for those considering a career in medi-cine or working in health care.”
ost texts on women’s mental health work their way systemati-cally through the various psychi-
atric categories of illness. This book does have a small section on disorder categories, but contains much more. There are chapters about interesting topics such as racial, eth-nic, and social class disparities, parental sta-tus, information technology, the workplace, and other knowledge domains pertinent to women’s mental health.
Each chapter is written by a different au-thor or group. Such variety often makes for uneven collections, but this book shows evidence of tight editing, with each chapter following a similar structure and written in similar style. This is good news for students, for whom this book is primarily intended, but may make reading a bit tedious for the casual reader.
Edited by public health authority Bruce Lubotsky Levin and women’s health expert Marion Ann Becker, this volume is intended for students in the social and behavioural sciences, mental health professionals, policy makers, advocates and consumers of mental health services - i.e., pretty much everybody.
The hope is that it will influence public pol-icy, improve services, and aid in the task of primary and secondary prevention of mental health problems in women.
The book is, unfortunately, written by Ameri-cans for Americans. Although many chapters pay homage to the influence of background and culture on psychological symptoms and on the provision of services, the editors stayed very much within the U.S. context.
Quibbles aside, this is a valuable book, as the foreword by former U.S. First Lady, Rosalynn Carter, affirms. My favourite chapter is the one by Alicia Dugan and Vicki Magley on services in the workplace. The chapter points out that, apart from sleeping, most of us spend more time at work than anywhere else. Also, up to 40% of the population reports stresses at work, which may have to do with allocated tasks, the roles we are assigned, the physical environment, and, importantly, in-terpersonal relationships. The same can be said for graduate student workplaces. The authors show that distress is caused not so much by the stressors themselves, but by in-dividuals’ perception of what they mean and by their responses.
Expectations of women are different in the workplace than they are for men. Opportuni-ties for advancement are often limited. Glass ceilings, tokenism, and sexual harassment are all facts of life. In addition, women work a second shift after they get home, as they are primarily responsible forthe household, their children, and aging kin. The work-family conflict is a potent stressor that progressive workplaces are only now be-ginning to address. The authors discuss child-care services, flexible hour arrangements and other strategies to relieve the double work-load. This chapter is somewhat longer than most of the others, and well worth carefully reading.
There are many critically important chapters in this book, which all, I hope, will find a wide audience.
Levin BL and Becker MA. (eds) A Public Health Perspective of Women’s
Mental HealthSpringer, New York, 2010l; 406 pages
M
If you are an IMS faculty member or student and would like to have your book recommendation published in a future issue of the IMS Magazine, please send a 50-word review to [email protected]
Column by Mary V. Seeman MD, Graduate Coordinator IMS
BOOK REVIEWS

29 | IMS MAGAZINE WINTER 2012 SPORTS-RELATED INJURIES
ichael Corrin, an enthusias-tic Biomedical Communications lecturer and recent IMS appoin-
tee, is driven by his passion to communicate scientific knowledge effectively, accurately and broadly. This is reflected most noticeably in his advocacy for mentorship and personal research pursuits.
Corrin received a Bachelor of Fine Arts from Concordia University, as well as a Bachelor of Arts in History and an Honours Bachelor of Science in Biology from the University of Winnipeg. Following his undergraduate education, he completed a Master of Science in Biomedical Communications (MScBMC) from the University of Toronto, where he now teaches.
As one of only five accredited programs in North America, the MScBMC program bridges art, science, medicine and commu-nication: students learn scientific concepts,
M
Science explained visually By Nina BahlBiomedical Communications lecturer Michael Corrin relays his passion for precise and meaningful visual communication of scientific concepts.
Phot
o by
Pau
lina
Rzec
zkow
ska
CLOSE UP
such as anatomy and pathology, while they simultaneously learn to visualize and depict these concepts in an understandable and ac-curate way. Corrin is determined to teach and apply visual communication methods to enhance scientific understanding as best he can.
Q What prompted your own involvement with BMC as a student?
A It was a very natural fit for me. Every year, we ask our first-year students to write a brief paragraph about how they ended up at BMC, and you can almost predict their re-sponses: “I love both art and science.” I fol-lowed the same route and found a place to explore my passions.
I realized during my undergraduate educa-tion that while I loved the fine arts, I really wanted to be involved in science too—if not pursuing my own scientific endeavours, then
finding a way to communicate the work of others. There is room to investigate how we can communicate best within the scientific community, and that’s really what motivated me to enter into this field.
Q Describe some of your teaching respon-sibilities. What do the courses entail and what do you hope students are able to learn?
A I started out providing technical assis-tance and teaching media tools, which I still do, but my role as a teacher has expanded to explain visual communication more wholly. The first course I was involved with pertained to medical legal visualization, a sub-disci-pline that creates visuals for the courtroom. For instance, if a doctor delivers a baby and the infant is injured, there might be a medical malpractice case where the doctor’s defense attorney wants to create visual support for the physician’s methods. We teach our stu-dents some of the Canadian and American

30IMS MAGAZINE WINTER 2012 SPORTS-RELATED INJURIES |
Imag
e co
urte
sy o
f Mic
hael
Cor
rin
To learn more about the PIE group and their available medical tools, please visit: pie.med.utoronto.ca.
CLOSE UP
legal framework, and then focus on the cre-ation of appropriate visuals.
I also teach a course on surgical illustration, which can be challenging but very rewarding for students. It teaches them to communi-cate a sequence of events in an accurate and understandable manner. Students attend a few live surgeries—ranging from cardiac to orthopedic procedures—and bring sketch-books with them to conceptualize the sur-gery. Initially, the focus is on gathering per-tinent information as swiftly as possible and becoming familiar enough with the proce-dure to pick out fine details and personalized surgical techniques. Ultimately, they consoli-date the information and create a sequence of images that depict the surgery clearly and with precision.
Q Outside of the classroom, how have you been able to apply components of visual communication theory in a practical way?
A I work with the Perioperative Interac-tive Education (PIE) group, housed within the Department of Anesthesiology at To-ronto General Hospital. We are comprised of a small group of biomedical multimedia developers and clinicians, and our aim is to develop useful medical education tools to be disseminated on the web, largely free of cost.
The essential idea is to get a group of clinical educators to think about what they are hav-ing a hard time communicating, as well as to think of new ways to get those ideas and concepts across. This is all done with the idea that we are not just serving a local group—by having these tools freely accessible, we’re po-tentially serving the world.
In an ideal scenario, educators come to us and say, “I’m having trouble teaching this concept. I think students would really benefit from some sort of supportive visual tool.” We collaborate with them, and the projects in-volve a lot of back-and-forth discussion. Our group works hard to develop communication solutions that really address the overall goal of the educator, but are also pertinent to any-one else accessing the information.
Q What would you consider your most sig-nificant accomplishment?
A With the PIE group, I developed tools to
help teach transesophageal echocardiography (TEE). Briefly, this technique is used in the operating room to monitor the heart in real-time by inserting an ultrasound probe down the esophagus. It can be difficult to visualize how the two-dimensional image onscreen re-lates to the three-dimensional aspects of the heart; we’ve been building a myriad of tools to help with this problem, including software simulations.
One of the multilingual TEE applications has garnered a great deal of positive feedback. We’ve had responses from people all over the world—including from places as far away as China and India—who say the tool has made it possible for them to visualize this challeng-ing concept. It’s extremely gratifying to know that people have found this tool useful.
Q How do you hope to continue your work in this field?
A I think teaching and mentorship are re-ally important, especially in our program. It would be difficult to imagine biomedical communication students sequestered to text-books—there’s a lot more guidance and in-struction required. I foresee myself continu-ing to do a lot of that, including some more one-on-one time, because I think and hope it really helps them.
In terms of research interests, I’m really in-terested in how we use digital tools to learn the structure of and relationships between objects in three-dimensional space, and how those tools help us construct corresponding mental representations. I hope that this re-search can generate principles to guide the design of digital tools that will ultimately help physicians and surgeons build more meaningful mental models of three-dimen-sional structures.
I am also very interested in the development of domain-specific toolkits to help visual communicators create explanatory imagery more efficiently and precisely. I would love for there to be shared repositories of some basic building blocks of our work—for in-stance, simple and accurate three-dimen-sional models—so anyone in our field can access these basic components for use in their projects. The art for me is not solely in creating those building blocks; the art is in telling the story well—it’s in interpreting information in an accurate way and helping others to understand.

31 | IMS MAGAZINE WINTER 2012 SPORTS-RELATED INJURIES
istorically, women were confined to the domestic roles of wife and mother, and were often
depicted as innately emotional and incapable of objective reasoning. Among other human rights advancements, the Women’s Rights movement helped women redefine their role in society and achieve greater equality. The unseen and unbreakable glass ceiling that kept qualified and accomplished women from rising to the upper echelons of the pro-verbial career ladder has seemingly shattered. However, the overt obstacles to women’s suc-cess are now replaced with a complex mosaic of subtle obstacles to career advancement,
with scientific career advancement being no exception.
While the trends are favourable—with an increase in female associate professors from 20% in 1990 to 33% in 2003 in Canada1—the leaky pipeline phenomenon persists: at suc-cessively higher ranks, women hold a de-creasing proportion of academic posts. The percentage of female full professors in Can-ada was only 8% in 1990 and 17% in 20031, which demonstrates the lower fraction of fe-males achieving full versus associate profes-sorship. Although an increasing number of women earn undergraduate degrees in tech-
nical fields, there is no increase in the pro-portion of female faculty. The leaky pipeline phenomenon was investigated by Wennerås and Wold in 1997; they identified pervasive sexism in the peer-review system as one fac-tor explaining why women are being awarded significant percentages of PhDs but a smaller proportion of postdoctoral research posi-tions, and a smaller still proportion of full faculty positions2.
Despite efforts to promote gender equality, the research sector is plagued by persistent inequalities between men and women, with a deficit of women in senior positions. Hav-
H
Scientist by day,Mother by night
How the mommy track runs covertly parallel to the tenure trackBy S. Amanda Ali
Phot
o b
y M
inya
n W
ang.
VIEWPOINT

32IMS MAGAZINE WINTER 2012 SPORTS-RELATED INJURIES |
ing made overt sexism socially unacceptable, women now face a labyrinth of subtle bar-riers, the top five of which include the bal-ance of work with family responsibilities, time management of work responsibilities, isolation and a lack of mentoring, the gain of credibility and recognition from peers, and the balance of one’s career with a spouse’s career3. In her book on the science glass ceil-ing, Rosser identifies other challenges facing today’s female scientists as they plan their careers: discomfort with self-promotion, funding instability, job restrictions (e.g. loca-tion, salary), networking, affirmative action backlash, negative social images, harassment, competition, and stereotypes3.
Societal pressures cause female scientists to develop carefully crafted public personae to keep their public and private selves separate, because, “If they disclose their private do-mains – as wives, as mothers, or as sexual human beings – they can jeopardize their status as professionals”4. In her report in the Yale Journal of Biology and Medicine, Wasserman describes how many successful women “make deliberate efforts to fit into the prevailing scientific culture by keeping their personal lives hidden.” Several of the scien-tists she interviewed for her article withheld permission to have comments concerning their domestic lives published4.
One might be tempted to assume that Was-serman is referring to a minority of female scientists, but I offer my experience as fur-ther evidence: successful female scientists at the University of Toronto can be reluctant to discuss their personal lives for fear of “ridi-cule” [Anonymous female faculty member]. One female researcher rationalizes, “I think the issue of work/life balance for women in medicine/research is very complex and per-haps it’s best … to present examples of some of us who have been able to make this work without getting into personal detail or com-ment that may run the risk of being misinter-preted by some and potentially undermine what we’re trying to achieve” [Anonymous].
1. Statistics Canada., The rising profile of women aca-demics, in Perspectives on labour and income. 2005, Statistics Canada = Statistique Canada: [Ottawa]. p. v.6.2. Wenneras, C. and A. Wold, Nepotism and sexism in peer-review. Nature, 1997. 387(6631): p. 341-3.3. Rosser, S.V., The science glass ceiling : academic women scientists and the struggle to succeed. 2004, New York: Routledge. xxv, 165 p.4. Wasserman, E., The Public and Private Personae of Women in Science Yale Journal of Biology and Medi-cine, 2003. 76: p. 163-165.5. Kolata, G. (2011) Women Atop Their Fields Dissect the Scientific Life. The New York Times.
References
Understandably, female scientists may choose to minimize their domesticity to maintain privacy and professionalism. Some may be convinced that the sexes are equal and feel that dwelling on the issue only sanctions so-cial norms regarding perceived gender-based disadvantages. Regardless of their underlying motivation, when female scientists strategi-cally refrain from mentioning their personal lives in public forums, they are depicted as one-dimensional, single-minded individuals. These skewed accounts are likely to contrib-ute to the leakiness of the pipeline by dis-couraging talented young women to pursue scientific careers. Another female researcher at U of T explains, “We work in the academic world of the University and we feel strongly that the way to make a case for being an effec-tive academic scientist/working mother is to talk about the work and achievements only - and let others make the inferences they wish to about inherent challenges and strategies needed to get to this place” [Anonymous]. Recall that isolation and a lack of mentoring were among the top five challenges experi-enced by female scientists3.
Generally speaking, professors at the Univer-sity of Toronto take their mentorship respon-sibilities seriously and speak frankly with stu-dents in private settings. Although the topics would never be breached in public forums, several female professors spoke candidly with me about the advantages and disadvan-tages of being a scientist and having a family. They freely offered advice for female students considering a career in science, but were op-posed to having that advice published. One female faculty member was happy to advise young women in “an informal sit-down chat regarding a career in science,” but felt her comments would “look unprofessional in press.” The inherent challenge to this is the logistics required to privately mentor the thousands of female students at U of T.
The intention of this article is not to berate female scientists for behaviour precipitated by societal pressures, nor to resurrect the Women’s Rights movement. Rather, the in-tention is to highlight a problem that must be addressed at an institutional level. Dr. Joy Hirsch, a professor of neuroscience at Colombia University, endorses the need for institutional procedure and commitment to raise the visibility and numbers of women in science. She describes doing exactly this,
without compromising quality, during her time at Yale University as the chairperson of the Status of Women Committee5. Dr. Hirsch emphasizes the need for diversity in the field of science, and contends that women’s ability to collaborate and think differently is impor-tant for the trajectory of the field5.
Initially setting out to document the career paths of female scientists, I was genuinely intrigued to learn how I too could be both an accomplished scientist and caring mother. The goal was to use the success stories of fe-male scientists who truly “have it all” to in-spire young female scholars and convince them that it was achievable. In order to en-courage females to pursue careers in science and effectively fix the “leaky pipeline,” strong leaders and role models need to emerge. Beginning with changes at the institutional level, we need to readjust societal norms to recognize, commend, and support female sci-entists in their career and family endeavours. Either one of these pursuits is sufficiently intimidating, so for future generations to be-lieve that both can be done, and done well, successful Dr. Mom’s need to speak up.
VIEWPOINT
Disclaimer: The opinions expressed by the author are in no way affiliated with the Institute of Medi-cal Science or the University of Toronto. Com-ments are welcome at [email protected].
In an effort to protect their scientific reputation, many female scientists refrain from speaking openly and honestly about their lives outside of work.
Needless to say, I was thoroughly disappointed by the resistance and censorship I encountered.

33 | IMS MAGAZINE WINTER 2012 SPORTS-RELATED INJURIES
umerous surveys report that there is a greater proportion of athe-ists in the scientific community
compared to the overall population. Roughly 40% of scientists are atheists, while 45% believe (in some capacity) in a god1. This is in stark contrast with the overall popula-tion where approximately 75% of American citizens believe in a god2. Yet in this author’s opinion, the number of believers in the sci-entific community is too high, since science is in direct irreconcilable conflict with reli-gion.
Instead of formulating an epistemological argument in favor of religious or scientific beliefs as representing the truth, I will pursue a more methodological analysis. Thus, I will speak from the perspective of a scientist, who already thinks scientifically. As a scientist, one makes the basic assumption that theo-ries regarding the material world must, at the very least, have independently testable, falsi-fiable predictions. Of course, the underlying philosophies that lead one to support these scientific criteria may be varied, but the basic assumption that a scientist upholds these cri-teria still stands.
Philosopher John Worrall posits that the ex-istence of believers among scientists can be
attributed to three things: 1) failure to fully think about the compatibility between sci-ence and religion, 2) failure to be truly sci-entific, and 3) adopting an assumption that science and religion cannot conflict because their jurisdictions are fundamentally differ-ent3.
Biologist Stephen Jay Gould named the third possibility ‘NOMA’ (non-overlapping mag-isteria). As he describes it, “Science tries to document the factual character of the natural world, and to develop theories that coordi-nate and explain these facts. Religion, on the other hand, operates in the equally impor-tant, but utterly different, realm of human purposes, meanings and values – subjects that the factual domain of science might il-luminate, but can never resolve.”4
There are many ways one can interpret the NOMA position. The first is to assume that science and religion have inherently different mechanisms for assessing non-intersecting claims: science is concerned with descrip-tions of the natural world (descriptive, or material claims), whereas religion should answer questions within the purely super-natural, metaphysical realm (non-material claims). By separating the two disciplines as such, it must be mandated that religion can-
not make any factual assertions about the material world, and science cannot make any assertions about the metaphysical. Thus, de-scriptive claims necessitate scientific testing (because they are in the realm, or jurisdic-tion of science) to ensure validity, while reli-gious claims must be assessed by completely separate, non-scientific standards3. To accept this idea is to accept the plurality of the word “standards”; that is, “if we allow different standards for explanations in religion, why not also in the study of the paranormal, or voodoo, or scientology, or... and the list goes on.”3 It is clear that there is no single stan-dard with which non-material claims can be assessed. There is only one way of doing science, but there are many religions, each denying the standards set out by others, and claiming their own as true.
Furthermore, restricting religion to non-material assertions opposes the vast majority of the prevailing theistic religions in society. There are countless religious intrusions into the natural world: prayer, miracles, resurrec-tion, virgin birth, reincarnation, etc. Each of these dogmas is a claim about the natural world, or about the interaction between the natural and supernatural. Thus, if one is to restrict religious claims to the purely meta-physical realm, then religious assertions that
By Adam Santoro
N
Imag
e: G
od c
reat
es A
dam
; Sis
tine
Chap
el, M
iche
lang
elo
Buon
arro
ti.15
10.
VIEWPOINT
An Irreconcilable Conflict

34IMS MAGAZINE WINTER 2012 SPORTS-RELATED INJURIES |
involve the material world must be inter-preted as entirely metaphorical3 (a difficult position, as religions claim non-metaphorical material truths) or must be simply declared false due to the confinement of religious as-sertions to the non-material.
Thus, the number of possible religions that a scientist could adhere to is extremely lim-ited under this interpretation of NOMA. The religion must contain no descriptive claims about the natural world, or must admit that any such claims are entirely metaphorical3. Since there is no standardized method for evaluating non-material assertions3, a scien-tist would have to choose a priori to follow a religion that meets these criteria. Such a deci-sion is completely arbitrary.
The second interpretation of NOMA sug-gests that religion can indeed make descrip-tive claims about the material world, but it may only do so when science fails. This “God of the Gaps” argument is pervasive in history, and is a fundamentally flawed perspective for scientifically minded individuals. It forces scientists to become unscientific (Worrall’s reason #2) by encouraging non-scientific an-swers to scientific questions. There are two claims that a religion may make: 1) actual explanations of natural phenomena when science does not have a sufficient explana-tion, or 2) “why” explanations about natural phenomena, which some claim fall beyond the realm of science. If history serves as any lesson, then the first type of claim should be quickly dismissed. Science is a continu-
ous discovery process; questions that were once deemed impossible to answer may be common knowledge in the future (such as the earth being round or the earth revolving around the sun).
The second type of claim is more interest-ing. Are there certain things that cannot be answered by science? Must the answers to “deep” questions be captured by religion? Worrall explains: “...the scientific cosmolo-gist cannot explain why it was that the so-called escape velocity of matter at ‘Planck time’ shortly before the big bang had the value it did - she must just take it as brute fact...The religious person can, as always, ‘explain’ that value by invoking a creator and his wishes...Although the structure of sci-ence inevitably leaves religion free to claim it can give ‘deeper’ explanations, what could warrant such claims? ... A religious explana-tion in terms of a creator and his intentions is just another (attempted) explanation...why did the creator choose an inverse square law rather than, say, and inverse cube one? ... The idea that religion can do what science cannot by “explaining everything” is an illusion.”3
Aside from being an attempt at understand-ing with a lack of evidence, illusory claims force scientists to become unscientific. Truly scientific questions are given non-scientific answers and are supposed to be taken as fact because religious presuppositions - not ra-tional thought - deem it so. Of course, there are indeed non-scientific questions that sci-ence cannot answer. But, as described above, if there is no definitive standard for answer-ing such questions, then any such answer is arbitrary.
Besides the NOMA hypothesis, under which science and religion must be entirely separate in order to live in harmony, some contend that science and religion can step on each other’s toes. This would imply that religion can make claims about the natural world. My only comment on this matter is that a truly scientific individual should demand the same quality of evidence for religious claims as for scientific claims. There is to date no religious assertion about the material world that has overcome scientific rigor; for example, there is no scientific proof of miracles, the soul, or the efficacy of prayer. One common criticism of this analysis is
that there may be an underlying assumption that all that exists is the material world. This is not the case. If we assume that a religious claim about the material world must be sub-ject to scientific rigor (as any scientist should assume), then many things can persuade a scientist that religion and science can coin-cide, like the proven existence of angels or evidence of intelligent design. However, no examples currently exist, so the current con-flict between science and religion stands.
Readers might note the irony in the article’s title; if reconciliation is theoretically possible, then why describe the conflict between reli-gion and science as “irreconcilable?” To bor-row from Bertrand Russell, this reconcilia-tion is theoretically possible - much like how it is theoretically possible for there to be a mi-croscopic teapot orbiting Saturn; or for there to be a flying spaghetti monster. For scientists who uphold a certain standard of rigor, there is no rational reason to be religious.
1) Larson, Edward J., and Larry Witham. “Scientists Are Still Keeping the Faith.” Nature 386.6624 (1997): 435-36. 2) Barry A. Kosmin and Ariela Keysar. “American Religious Identification Survery 2008.” Hartford, Con-necticut, USA: Trinity College (2008). 3) Peterson, Michael L., and Raymond J. VanArragon. Contemporary Debates in the Philosophy of Religion. Malden, MA: Blackwell, 2004. 4) Gould, Stephen Jay. Rocks of Ages: Science and Religion in the Fullness of Life. New York: Ballantine Pub. Group, 1999.
References
Disclaimer: The opinions expressed by the author are in no way affiliated with the Institute of Medi-cal Science or the University of Toronto. Com-ments are welcome at [email protected].
VIEWPOINT

35 | IMS MAGAZINE WINTER 2012 SPORTS-RELATED INJURIES
Behind the Scenes:Dr. Brenda Toner Moving women’s health research forward through multidisciplinary & interprofessional approaches
By Zeynep Yilmaz Phot
o by
Pau
lina
Rzec
zkow
ska
BEHIND THE SCENES

36IMS MAGAZINE WINTER 2012 SPORTS-RELATED INJURIES |
A s of October 2011, the IMS is welcoming Dr. Brenda Toner as new Graduate Coordinator, filling
the position vacated by Dr. Mary Seeman. An IMS faculty member since 1992, Toner is no stranger to the IMS or to leadership positions; she has led many collaborative initiatives among fields such as psychology, psychiatry, gastroenterology, family practice, education, public health, and policy. She is currently the Director of the Fellowship Pro-gram at the Department of Psychiatry and was the Head of the Women’s Mental Health Program from 1997 to the fall of 2011. Her research focuses on disorders that are dis-proportionately represented among women, including—but not limited to—functional gastrointestinal disorders, eating disorders, chronic fatigue, depression, and anxiety. She has used various theoretical frameworks for the study of these disorders, ranging from neuroscience to social determinants of health. She is particularly interested in inves-tigating constructs that cut across diagnosis, including violence, gender role socialization, sexism, and body dissatisfaction.
Toner’s journey in research is a true testa-ment to multidisciplinary approaches and collaborative work. After completing her undergraduate studies in Psychology at Queen’s University, Toner spent one year at Simon Fraser University as a Master’s stu-dent before accepting a research assistant position in Dr. Harvey Moldofsky’s lab at the Clarke Institute (today’s Centre for Addic-tion and Mental Health). During this period, she worked on studies exploring the neu-roscience of sleep apnea, fibromyalgia, and chronic fatigue. She then transferred to the PhD program in the Department of Psychol-ogy at the University of Toronto, studying the psychophysiology of test anxiety. Funded by the Ontario Mental Health Foundation, her postdoctoral fellowship took place in the Eating Disorders Program at Toronto Gen-eral Hospital (TGH), supervised by Dr. Paul Garfinkel. During this time, she and Dr. Al-lan Kaplan, a psychiatry fellow at the time, worked side by side; Toner is very happy to be working with Dr. Kaplan again, this time in a different role within the IMS.
As a fellow at TGH, Toner was presented with an opportunity to expand her research to the area of functional gastrointestinal disorders. She started working on cogni-
tive behavioural models and interventions for chronic gastrointestinal disorders, espe-cially in women. At the time, there was little research being done on the psychosocial is-sues surrounding gastrointestinal disorders in women, and the field suffered from the stigma of these so-called unexplained func-tional medical illnesses. Considering that up to 90% of sufferers of these conditions in tertiary care are women, Toner dedicated her career to exploring and empirically test-ing interventions that improved symptoms and wellbeing in individuals suffering from these chronic and painful disorders. In her fruitful career, Toner has received funding from prestigious organizations such as the National Institutes of Health and the Cana-dian Institutes of Health Research, in addi-tion to publishing numerous high-impact journal articles and supervising more than 50 students. Her book, entitled “Cognitive-Behavioral Treatment of IBS—The Brain-Gut Connection,” aims to deconstruct and destigmatize IBS using a biopsychosocial ap-proach. Her research has received extensive international recognition, and her book has been added to physician training curricula to promote a multidisciplinary approach; it has also recently been translated to Japanese, resulting in critical acclaim.
Having watched the IMS grow from an insti-tute that focused on physicians into a centre for translational and multidisciplinary re-search, Toner is looking forward to being a part of the IMS’s bright future. She has led numerous scholarly and educational initia-tives at the University of Toronto through-out her career, and she states that she really enjoys interacting with students and fellows. Since her fellowship with Dr. Garfinkel, the most inspirational and meaningful activity for her has been mentoring, facilitating for, and interacting with students, trainees, and other researchers. “When I was invited to consider serving as a graduate coordinator at IMS, it was exceptional timing,” she says, and adds that she is very excited to have the opportunity to take the IMS to the next level, particularly in terms of emphasizing transla-tional, collaborative, and multidisciplinary research.
Toner, who has supervised many male and female graduate students over the years, is dedicated to making academia friendlier to young scientists, especially women. She
truly believes in the importance of embrac-ing students and serving as a role model for them. She is devoted to encouraging young researchers to pursue academic positions and providing a safe and creative opportunity for them within academia. When asked about being a female academic, she states that she had a wonderful experience within the af-filiated hospitals and various departments of the University of Toronto. Toner is especially excited about the future, as more women en-ter health care and medicine, and she urges young scientists—men and women alike—to actively seek leadership positions. She hopes to continue her role as a mentor, as well as empower and share her experience with stu-dents under the roof of IMS.
Acknowledging that graduate school can be stressful at times, Toner advises students to choose a research area about which they are passionate. “Since research can be demand-ing, students should ensure that they are truly interested in their line of research,” she adds. She also emphasizes the importance of a good scientific and interpersonal fit with supervisor and PAC members, so that the student’s creativity and ideas are properly embraced. Toner also advises IMS students to be assertive, ask questions and seek help when needed, take part in student life, have a career plan, and develop professional as well as support networks. A firm believer in work-life balance, she reminds students of the importance of having personal passions, spending time with family and friends, and leading a healthy lifestyle. Finally, Toner re-iterates that the most productive activities come when a person feels empowered in a positive and welcoming environment, and she concludes:
“Be mindful, stay open to new ideas, and remember to take a deep breath.”
BEHIND THE SCENES

37 | IMS MAGAZINE WINTER 2012 SPORTS-RELATED INJURIES
o say that Dr. Catharine Whiteside is a busy person would be a colossal understatement. Now entering her second term as Dean of the Faculty of Medicine, Whiteside is responsible for professional MD programs, post-graduate MD programs,
and graduate departments including the IMS. She also holds various positions on boards and committees: she recently finished her term as president of the Canadian Academy of Health Sciences, an organization she helped to establish; is currently Co-Chair of the Council of On-tario Faculty of Medicine and the council of Deans of Medicine in Ontario; and is also on the executive of the Association of Faculties of Medicine in Canada. “I sit on seven hospital boards, and when the board [is discussing a topic and] turns to me and asks, ‘What does the univer-
TPh
oto
by P
aulin
a Rz
eczk
owsk
a
A Powerful WomanA peek into the prolific career of
IMS Graduate and Dean of Medi-cine, Dr. Catharine Whiteside
By Allison Rosen
FUTURE DIRECTIONS

38IMS MAGAZINE WINTER 2012 SPORTS-RELATED INJURIES |
sity think?’ it’s very clear that people look to you as the face of the Faculty of Medicine and even the university,” she shares, demonstrat-ing the amount of responsibility inherent to her position.
In addition to the laundry list of prestigious organizations of which Whiteside is a part, her long history with the University of To-ronto tells an exciting story of success. Ob-taining her MD from the University of To-ronto in 1975, Whiteside began her specialty training in internal medicine and nephrol-ogy, after which she entered research train-ing supervised by Dr. Mel Silverman. Being new to basic science research, Whiteside was surprised by how much she enjoyed it. While attempting to find a job in Toronto, she be-came aware of an opening as a clinician-sci-entist. She recalls her conversation with the divisional director of nephrology at Toronto Western Hospital. “I asked, ‘If I do a PhD, will you hire me?’ and he said sure,” White-side laughs. She began her Master’s degree and later transferred to a doctorate program in the Institute of Medical Science. Even then she was a pioneer, being one of the first PhD graduates to become a clinician-scientist.
Whiteside describes her choice to complete her PhD with the IMS: “It was the train-ing ground, even then, for physicians to do graduate work. It was a great experience.” The lab also offered different challenges than her clinical work. “In the lab, you can design a good experiment; that was the most fun about being a PhD student. Even if the re-sults were negative, you’ve been able to test a hypothesis. And then when you finish your PhD, you are probably the most knowledge-able person in the world in that area—at least for a few days,” she remarks, chuckling at the memory.
Heading a laboratory came easily to Whi-teside. After becoming a clinician-scientist
in the Department of Medicine in 1985, she became a full Professor of Medicine in 1996. Her career also rapidly shifted to increasingly administrative leadership positions. From 1993 to 1999, Whiteside served as Graduate Coordinator for the IMS. Due to close inter-actions with students and faculty, Whiteside attests, “If somebody asked what was the best job [I ever had], I would say that.” She became Associate Dean of Graduate and In-ter-Faculty Affairs in the Faculty of Medicine in 2000, and from 2001 to 2005 she chaired the Inter-Professional Education Curricu-lum Planning Committee. After serving as Interim Dean of Medicine, she became Dean of Medicine in 2006. Whiteside officially shut down her lab in 2008. “I miss it, but you can’t do everything,” she remarks wisely.
Whiteside shares that her position as Dean is “like being the CEO of a big company. It’s about building relationships with major part-ners, like the hospitals and research insti-tutes, and overseeing many departments and a lot of people. And it’s fun… most days,” she smiles. Her skills as a clinician and scientist have also been transferrable to her adminis-trative responsibilities. “You have to have a vision, you have to see where you want to go, and really develop your leadership to make it work. Being a successful leader and manager takes a lot of creativity, and to be a scientist you also have to be rigorous and you have to be creative in how you think.”
When asked about the future, Whiteside jokingly admits that throughout her career, she “never knew what [she] was going to do 5 years down the road.” Reflecting on this, she adds, “For as long as I can remember, I always knew I wanted to be a doctor. But I never would have guessed that I’d go into academic medicine.” She hopes to be able to lead the medical school and residency pro-grams through major accreditations in 2012 and 2013, respectively, and also implement the Faculty of Medicine’s Strategic Planning initiative. Whiteside shares her vision for the future of IMS: “We’re heading into an era of interdisciplinary research, and there’s no place that is more interdisciplinary than [this department].”
The IMS Magazine asked Whiteside to elabo-rate on the focus of Strategic Planning, which she did using a personal example. “I was trained as a basic scientist, but I was never
trained to translate that into human research. And if you’re trained in population health or clinical epidemiology, you’re not trained to apply it at a fundamental level. Translation is about being able to take a team approach, where you’ve got a basic scientist, a clinician, and other individuals who can take funda-mental discoveries and apply them for the di-agnosis and treatment of disease, and address questions that any individual group can’t address. We want to develop a true curricu-lum for training individuals in translational research—I think we’ll be able to step for-ward and be leaders in this area.” Whiteside shares an example of a research project with a successful translational aspect. Excitingly described as “the largest single-group cohort study in the world,” a project on human devel-opment based at Mount Sinai Hospital is cur-rently underway. The study links world-class experts from various disciplines, including physiology, epigenetics, fetal development, cognitive psychology, and early childhood development. Without such a multi-centre, interdisciplinary team, the project would “never realize its full potential.”
Whiteside provides some words of advice for IMS students. “Figure out what you like doing the best, because if you’re not passion-ate about it, you’ll never do it well and you’ll never be satisfied. And always be open to new opportunities. You never know where people are going to end up,” she remarks.
Despite her busy career, family remains a pri-ority to her. As we sit in her office, she proud-ly gestures towards a photograph displayed prominently on her wall, in which a smiling girl stands on the stairs of a yellow school bus—it is a picture of her granddaughter on her first day of school. Whiteside has two grandchildren, and she travels to Seattle frequently to visit them. She also enjoys the opera and painting, although she admits that lately she has had little time for her artistic hobby; she jokes that she may resume paint-ing once she finally has the chance to retire. Given the breakneck pace of her career, one can only imagine Whiteside’s retirement to be anything but quiet.
“You have to have a vision, you have to see where you want to go, and really develop your leadership to make it work. Being a successful leader and manager takes a lot of creativity, and to be a scientist you also have to be rigorous and you have to be creative in how you think.”
“Figure out what you like doing the best, because if you’re not passionate about it, you’ll never do it well and you’ll never be satisfied.“
FUTURE DIRECTIONS

39 | IMS MAGAZINE WINTER 2012 SPORTS-RELATED INJURIES
FUNDING
anada faces an innovation imper-ative,” says a report released in No-vember by the Institute for Competi-
tiveness and Prosperity. It finds that in the last decade, “poor productivity and lagging innovation have persisted in the Ontario economy,” leading to a so-called “prosperity gap” despite the fact that Canadians actually lead other developed nations in the number of hours individuals work (also termed ‘work effort’). This suggests that businesses “need to step up their investments in technology – from R&D, to patents (another area where Canada lags behind), to adapting existing technology.”1
In response to this long-standing “prosper-ity gap,” the MaRS Discovery District was founded in 2000. Its goal is to bring govern-ments, businesses and science together to better “capture the commercial potential of Toronto’s $1 billion in annual science and technology research spending.”2
A public-private partnership, MaRS aims to promote innovation to help entrepreneurs secure funding, and to develop success-ful business models that create and retain wealth, knowledge and skills generated in Canada. They seek to accomplish their goals through consulting, market research and venture capital.2
But is MaRS achieving its mission? Are the goals of its founders being realized? Unfor-tunately, the answer is, well, unclear at best. And in the last few years, several concerns have been raised.3
Despite being classified as a charitable orga-nization, MaRS does not release a publically available annual report that documents its public and private sources of revenue and the proportion of funds allocated to programs, services, salaries and other business necessi-ties. The only mention of money allocation is on a webpage titled “Where Your Money Goes,” which contains vague and broad state-ments such as: “MaRS has helped more than 1,300 companies and produced more than 2,400 hours of market research analysis, and roughly the same helping companies with their businesses.”4
A critic named Greg Boutin, who is a for-mer Consultant with the Boston Consulting Group and current Managing Director at Growth Route, calculates on his blog, “That’s a whopping 5 days a year per advisor assum-ing an average of 15 advisors over the past 4 years (generous assumptions since they likely count time spent since MaRS’s inception), or 1.45h per company helped (2,400h divided by 1,300 entrepreneurs).”3
Outside of testimonials, there is no measure of the effectiveness and utility of the services offered, and no quantitative evidence show-ing how client companies have benefited from the services offered at MaRS. Did their clients raise profits? Expand their business? Create more jobs?
The only publically available information I have been able to find is from the Ontario Public Salary Disclosure and the Registered Charity Information of Return on the Cana-da Revenue Agency webpage.5,6
The former depicts an upward salary trend, where despite the absence of any perfor-mance assessments (and accounting for the economic recession), the CEO’s salary rose from $427,500 in 2007 to $532,500.99 in 2010.5 As Boutin points out, in 2010 the CEO’s salary was increased by 22% from the previous year, a month before the McGuinty wage freeze went into effect.7,8 The CEO is the third-highest paid public service employ-ee in the “Other” section of the Public Sector Salary Disclosure list for Ontario.
Although MaRS is touted as a public-private partnership, the true partnership seems highly skewed towards the “public.” The Reg-istered Charity Information of Return shows that MaRS received $130 million in subsidies between 2002 and 2008. Boutin writes, “Al-most all of the revenue (over 90% in 2008) comes from government grants and rental/meeting room income from buildings pur-chased with public dollars.” Why is MaRS—a publically subsidized non-profit organiza-tion—generating revenue by renting govern-ment-funded buildings to, for example, gov-ernment-funded laboratories?
I am not opposed to government-supported initiatives aimed at promoting innovation and commercialization. But I do believe that when large sums of taxpayers’ dollars are spent, there should be full accountability and transparency to the public as to how, for what purpose, and toward what result the money is being spent. Perhaps MaRS is just afraid of people like ‘don242’—a previous employee of a company that was a MaRS client—who voiced his opinion with his online moniker: “…I didn’t get the impression that (MaRS) was helping (clients) develop a relationship with other researchers. Perhaps if they were there a few years longer, something might have developed.”9
It is curious that MaRS relies heavily on gov-ernment funding while providing tradition-ally private-sector services. And as Boutin writes, “After all, the essence of commercial-ization is about making people pay for a so-lution to their need: if hubs can’t do that for themselves, they should not be in the busi-ness of teaching it to others.”3
COpinion: Occupy MaRS By Tetyana Pekar
Phot
o cr
edit
to Ip
Kan
g, e
n.w
ikip
edia
.org
/wik
i/File
:Met
allic
_MaR
S.jp
g.
Kang
is n
ot a
ffilia
ted
with
the
IMS
Mag
azin
e an
d do
es n
ot e
ndor
se a
ny c
onte
nt a
ssoc
iate
d w
ith th
e pu
blic
atio
n.
Disclaimer: The opinions expressed by the author are in no way affiliated with the Institute of Medi-cal Science or the University of Toronto. Com-ments are welcome at [email protected].
References1. http://www.competeprosper.ca/index.php/media/press_re-leases/institute_releases_report_on_canada_2011_canadas_in-novation_imperative/2. http://www.marsdd.com/ 3. http://www.growthtimes.com/2010/04/troubling-facts-about-mars-discovery-district-part-1-of-4/4. www.marsdd.com/donate/where5. http://www.fin.gov.on.ca/en/publications/salarydisclo-sure/2011/otherp11.html6. http://www.cra-arc.gc.ca/7. http://www.growthtimes.com/2011/08/ceo-of-mars-got-22-raise-one-month-before-ontario-wage-freeze-made-533k-in-2010/8. http://ottawa.ctv.ca/servlet/an/local/CTVNews/20100407/OTT_McGuinty_Wages_100407/20100407/?hub=OttawaHome9. http://forums.redflagdeals.com/opinions-mars-1082143/

IMS MAGAZINE WINTER 2012 SPORTS-RELATED INJURIES | 40
ExpertsAskthe
Dear Experts, I am in my final year of undergraduate stud-ies. I am interested in pursuing a medical degree and have applied to medical school. Would it be worthwhile to apply to complete a Master’s degree with the IMS, just in case I don’t get accepted to medical school? Will a Master’s degree with the IMS increase my chances of getting into medical school?
-Doctorly DilemmasDear D.D.,Unless you are 100% sure of getting into medical school (and no one really can be), it is safest to also apply to graduate school. If you are genuinely interested in research, it may be beneficial to pursue a graduate de-gree, as some medical schools (but not all) prefer candidates with graduate degrees.
Dear Experts, My first PAC meeting is soon approaching. Unfortunately, I have not been able to gener-ate any data. Is it required to provide data at each meeting? What should go into my pre-sentation?
-Committee ConcernsDear C.C.,You are not expected to have data at your first PAC. What you present is your tentative idea for your project and the reading you have done around it. You should also talk about the courses you intend to take, a time-line that makes sense to you, and whether or not you are thinking of transferring from a MSc to a PhD. If you have a clinical proj-ect, you may want to present your clinical research ethics application. Come prepared to discuss sample sizes and how to estimate them. If you experience problems in the laboratory, don’t hesitate to bring them up.
Dear Experts, I made a mistake during an experiment. Should I speak up? What if I get in trouble?
-Experimental ErrorsDear E.E.,Making mistakes are part of the graduate stu-dent learning process. Be proud of them and make sure everyone knows about them.
Dear Experts, I don’t have a designated workspace in my lab. Is this normal? Is every student entitled to one?
-Deskless and CuriousDear D.C.,If your work requires workspace in the lab, then you need to have it. If there’s no space in your lab, ask your supervisor to organize a space for you close by. Some kinds of re-search do not require workspace. Many students work in libraries. Some work from home. If space continues to be an issue, con-sult the grad coordinators.
Dear Experts,I’m hoping to start a Master’s program next year with the IMS. I’ve noticed that I am eli-gible to apply to some external awards (e.g. OGS). Is it beneficial to apply for funding prior to commencing my Master’s program?
-Ambitious for AwardsDear A.A.,Absolutely. Coming into the program with your own funding means you have a better chance to work with your preferred supervi-sor. Also, each external grant is a stepping-stone to the next one. Even if your applica-tion is not successful, it proves to the world that you are serious about graduate studies.
Mistakes are a normal part of gradu-ate school experience. Don’t be dis-couraged if things don’t work out ex-actly as planned.
Do you have a question for the experts? Please send it to [email protected] (ATTN: Experts).
EXPERT TIP
Dear Experts, I was recently appointed as a faculty member with the IMS. I plan to recruit a few graduate students. Does the IMS of-fer specific guidelines or instructions for supervisors to supervise IMS graduate students? Are there faculty workshops I can attend to bring me up to speed with the program requirements?
-Puzzled ProfessorDear P.P.,Yes to both questions. If you have trouble locating the guidelines or finding out when the next faculty workshop is taking place, please contact one of the graduate coordinators.

41 | IMS MAGAZINE WINTER 2012 SPORTS-RELATED INJURIES
PAST EVENTS
Mo’ support for Mo-vember! IMS students and faculty show off their impressive Mo-vember moustaches at St. Mike’s Hospital’s site-specific event.
All p
hoto
s co
urte
sy o
f IM
SSA
repr
esen
tativ
es
Sunnybrook Hospital’s IMS students warmed themselves up with some delicious hot chocolate at their an-nual site-specific gath-ering.
IMS Students from Toronto West-ern Hospital enjoy pizza, drinks, and chatting with other TWH members at their site-specific IMSSA event.
IMS students enjoy IMSSA’s Amazing Race event by deciphering clues and exploring the streets of Toronto. This event is held annually and gives IMS students an opportunity to become familiar with the city’s hotspots.
PAST EVENTS

42IMS MAGAZINE WINTER 2012 SPORTS-RELATED INJURIES |
Messy Desk Competition!Do you have a difficult time finding a spot to put your papers? Have your fellow lab mates complained about the state of your workspace?If you feel like you have the messiest workspace at the IMS, please send your name and photo of your messy workspace to [email protected] (ATTN: Messy Desk Competition) by March 1, 2012. If you are voted to have the messiest workspace, we will publish a photo of your messy desk in the next issue of the IMS Magazine!
CROSSWORD
Solution to Sudoku from Fall 2011 issue of the IMS Magazine
“Piled Higher and Deeper” by Jorge Cham http://www.phdcomics.com
DIVERSIONS
Mo-rvelous Moustaches! Movember Contest Winners
Left: Artur Jakubowski, IMS StudentRight: John Soleas, 2nd year IMS Student
Across:1. Largest human organ.3. Endocrine disorder of insulin resistance.4. Twins sharing same DNA.7. To take away.8. Addictive component of cigarettes.9. Molecules sitting on cells that receive signals.10. Bone that connects the spine to the legs.11. Treatment centre.14. To soil, dirty.17. Easy to set on fire.
Down:2. Device making small objects bigger.3. Sugar found in DNA.5. Back tooth.6. Last stage of mitosis.7. Germ-free.12. Element number six.13. Hunger stimulating hormone.15. Liquid component of blood.16. Roof of the mouth.18. Instrument used to transfer measured volumes of liquid.