

Improving Transitions of Care, Handoffs and Coordination Across Units Dr. Ayse Gurses & Dr. Mahiyar...
40
Improving Transitions of Care, Handoffs and Coordination Across Units Dr. Ayse Gurses & Dr. Mahiyar Nasarwanji Armstrong Institute for Patient Safety and Quality
-
Upload
angelina-pierce -
Category
Documents
-
view
217 -
download
0
Transcript of Improving Transitions of Care, Handoffs and Coordination Across Units Dr. Ayse Gurses & Dr. Mahiyar...

Improving Transitions of Care, Handoffs and Coordination Across Units
Dr. Ayse Gurses & Dr. Mahiyar Nasarwanji
Armstrong Institute for Patient Safety and Quality

2
Objective
• To highlight the importance of smooth care transitions and handoffs
• To provide a list of good practices during transitions of care

3
Overview
• Background • Define
– Care transitions – Handoffs
• Good practices – For each stage of the transition
• Handoffs• Other pieces of the intervention package
4
Significance of Care Transitions
• 46% to 56% of all medication errors during transitions (Pippins et al 2008, Barnsteiner 2005)
• Hazards (Horwitz 2009)
– Inadequate support for situation awareness
– Inaccurate / inadequate information transfer
– Unstructured / non-standardized handoff
– Responsibility / Role ambiguity– High workload

Communication Breakdowns are frequently the root cause of…undesirable outcomes
Improving Handoff Communications: Meeting National Patient Safety Goal 2E, Joint Comm Perspectives on Patient Safety, 2006.

6
Handoff reports
• Patients are particularly vulnerable during handoffs – Incorrectly communicated information– Information not communicated at all
• Appropriate measures for evaluating effectiveness of handoffs still need to be established and validated1
1. Solet DJ, Norvell JM, Rutan GH, et al., Acad Med, 2005.

7
Part of the larger care process…
Pre transfer care
Prepare patient for transfer at
sending endPhysically transfer patient
Stabilize patient at receiving
end
Handoff
Post transfer care

8
Care transitions
“Set of actions designed to ensure the coordination and continuity of health care as patients transfer (move) between different locations or different levels of care. Care transitions encompass both the sending and the receiving aspects of the transfer”
American Geriatrics Society Health Care Systems Committee. Improving the Quality of Transitional Care for Persons with Complex Care Needs. Journal of the American Geriatrics Society. 2003;51(4):556-557.
Patient
ER
ICU
OR
FloorRehab center
Home
Home care

9
Handoffs
“The transfer of information (along with authority and responsibility) during transitions in care across the continuum for the purpose of ensuring the continuity and safety of the patient’s care.”
Presentation for Standardizing Handoffs for Patient Safety AORN. 2012. Accessed April 8, 2013. Available at: http://www.aorn.org/WorkArea/DownloadAsset.aspx?id=20863

10
Care transitions intervention

11
Evidence
• CSTS project (site visits)– Observations– Interviews– Tool analysis (handoff report
checklists)• Literature• Wisdom of crowds (Clinical
expertise and experiences)

12
Systems Engineering Initiative for Patient Safety (SEIPS) Model
Carayon, P., Hundt, A.S., Karsh, B.-T., Gurses, A.P., Alvarado, C.J., Smith, M. and Brennan, P.F. “Work System Design for Patient Safety: The SEIPS Model”, Quality & Safety in Health Care, 15 (Suppl. 1): i50-i58, 2006.

13
How do we implement it?
• Leverage your CUSP teams• Covered in the face to face meeting
1. Identify executive leadership 2. Identify units involved 3. Identify team 4. Identify current practice and expectations Today
5. Assessment of current system
6. Training program
7. Develop and roll out handoff tool
8. Periodic assessment
9. Continual improvement

14
Good Practices

15
Focus
• Concentrates on transfers from– OR ICU – ICU Floor
• List of good practices are generic – Some many not apply to specific transition

16
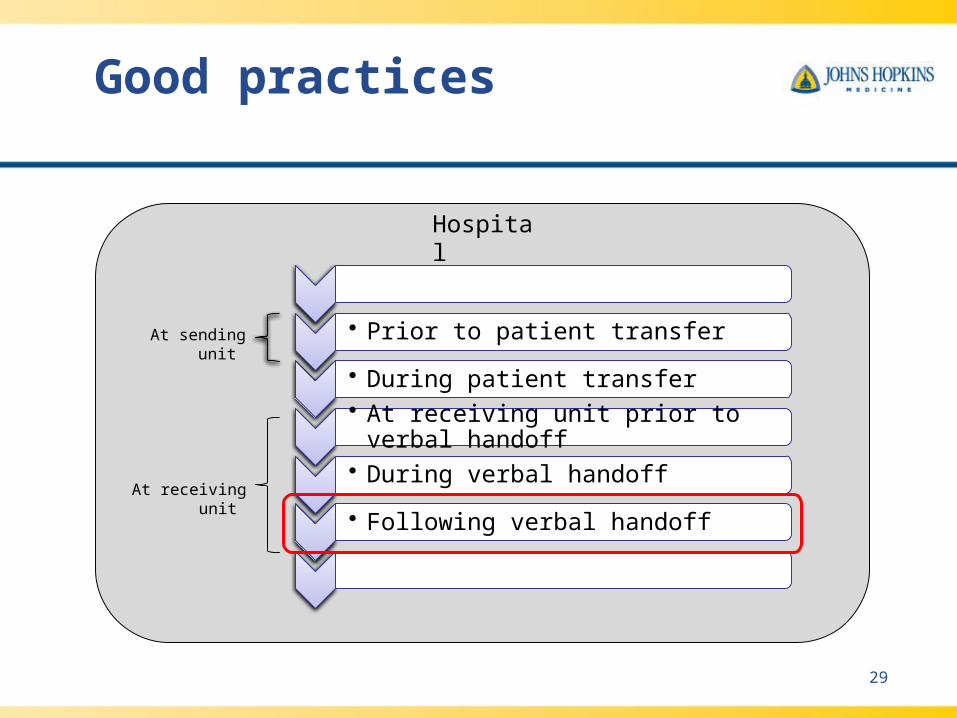
Good practices
• Prior to patient transfer
• During patient transfer
• At receiving unit prior to verbal handoff
• During verbal handoff
• Following verbal handoff
At sending unit
At receiving unit
Hospital
17
At the hospital level
• Handoff policy – That all staff are aware of– Or staff know where to locate
• Adequate and appropriate training on care transitions and handoffs
• Coordination and teamwork between units should be regularly evaluated and improved
• Designated champions at various locations– Can be contacted for questions – Can collect feedback
• Equipment should be functional and ready to use• Consider compatibility of devices across units when making
purchasing decisions

18
• Prior to patient transfer
• During patient transfer
• At receiving unit prior to verbal handoff
• During verbal handoff
• Following verbal handoff
Good practices
At sending unit
At receiving unit
Hospital

19
Prior to patient transfer
• Inform receiving unit of– Patient’s time of arrival– Patient related information (telephone handoff)– Specific equipment needs
• Inform sending unit of patient’s destination• All cables, lines and wires should be
– Clearly labeled – Organized and secured
• Patient should be stable and ready for transfer
20
• Prior to patient transfer
• During patient transfer
• At receiving unit prior to verbal handoff
• During verbal handoff
• Following verbal handoff
Good practices
At sending unit
At receiving unit
Hospital

21
During patient transfer
• Equipment should permit stable movement of the patient– Bed / wheelchairs used for transport should
have adequate and appropriate locations to place and secure all equipment required for transfer
• At least one individual should be aware of the exact destination at the sending unit

22
During transfer of patient
• Remove all barriers – Provide an assigned or limited access
elevator for transfers – Path of travel should be a barrier free zone
• No equipment in the corridors• No movement past family waiting areas

23
• Prior to patient transfer
• During patient transfer
• At receiving unit prior to verbal handoff
• During verbal handoff
• Following verbal handoff
Good practices
At sending unit
At receiving unit
Hospital

24
At receiving unit prior to verbal handoff
• At least one nurse in addition to the primary nurse should be present to receive the patient (dependent on patients condition)
• The cables and monitors in from the sending unit should be compatible with those in the receiving unit
• When transferring cables and lines– Cables and lines should be transferred sequentially– Warning should be provided prior to disconnecting– No more than a 30s disruption
• Patient should be stable and comfortable

25
• Prior to patient transfer
• During patient transfer
• At receiving unit prior to verbal handoff
• During verbal handoff
• Following verbal handoff
Good practices
At sending unit
At receiving unit
Hospital

26
Verbal handoff (1 of 3)
• At least the primary nurse and/or the provider from the receiving unit (e.g., intensivist) should be present
• The environment should– Be free of noise– Provide adequate space for all the key players– Not interfere with other clinical workflow
• Adequate time should be provided to complete the handoff
27
Verbal handoff (2 of 3)
• There should be an identified leader that initiates and directs the verbal handoff
• The primary nurse or provider should be asked and explicitly acknowledge readiness for the handoff
• There should be no distractions and interruptions other than for– Clarifications– Questions – To take care of critical patient related issues in the unit
• Nurses and providers should be able to pause the handoff • Everyone should feel comfortable asking questions

28
Verbal handoff (3 of 3)
• A standardized handoff checklist or tool – Should be consistently used – Kept as a temporary record
• Primary nurse and provider should make notes of what is being discussed
• The primary nurse or practitioner at the receiving unit should explicitly acknowledge assumption of care
• Principles of good teamwork should be followed– Empowerment– No role or responsibility ambiguity– Appropriate conflict resolution – Clear, complete, brief and timely communication
29
• Prior to patient transfer
• During patient transfer
• At receiving unit prior to verbal handoff
• During verbal handoff
• Following verbal handoff
Good practices
At sending unit
At receiving unit
Hospital
30
Following verbal handoff
• The nurses and physicians at the receiving units – Should be aware of the short-term and long-term
goals for the patient– Know who to contact after the handoff for questions
and concerns• How to contact them
– Should verify critical information communicated during the handoff
• Should be a mechanism to provide immediate informal feedback

31
Lets concentrate a little more on the verbal handoffs …

32
Handoffs
Why?
When?
Where?
Who?
How?
What?
• Successful transfer of information
• Dedicated time• Sufficient length
• Close to work area• Large enough
space• Free from
distractions• Access to required
information and technology
• Key personnel / players• Active involvement of
senior physicians
• Clear leadership • Good
communication• Team involvement • Avoid interruptions • Discussion and
questions• With the aid of
checklists, tools and technology
• Provider information • Patient information• Plan of care • Discussion and
questions
Adapted from: AMA Clinical Handover Guide - Safe Handover: Safe Patients: https://ama.com.au/ama-clinical-handover-guide-safe-handover-safe-patients

33
Primary objective of handoffs
• “The primary objective of a “hand off ” is to provide accurate information about a [patient’s] care, treatment, and services, current condition and any recent or anticipated changes.”
Meeting the Joint Commission 2008 National Patient Safety Goals, Joint Commission, 2007.

34
What information?
• Customized to hospital and setting • Use pre-existing format and Mnemonics• Some guidelines
– Introduction of all care providers and their roles– Identifiable patient information– Past medical history/ comorbidities of the patient – Current situation / state of patient – Current assessment and diagnosis– Plan of care – Anticipated problems and contingency plans– Read-back and / or synthesis by receiver– Questions– A genuine invitation to call for additional clarifications

35
Standards of effective communication
Brief
Clear
Complete Timely
Verify & validate

36
Teamwork

37
Toolkit
• New material – Assessment of Care Transitions (ACT) Upcoming– Participatory user centered design approach Upcoming
to tool / checklist development
• Reinforcement– Teamwork across unit tool Upcoming– Barrier identification and mitigation tool
• Currently implemented– Transitions of care survey – Part of HSPOS – Relational Coordination

38
You will need to ACT soon… Assessment of Care Transitions
Yes No N/aPre verbal handoff assessment
Was there at least one nurse present in addition to the primary nurse when the patient arrived at the receiving unit to help stabilize the patient?
Were the monitors and or cables, sent with the patient compatible with the monitors and / or cables at the receiving unit?
Was equipment (e.g. monitors) needed for the patient at the receiving unit
a. Available
a. Functional
a. Appropriate / adequate
If lines, tubes and cables were transferred to a new monitor,
a. Were all key parameters visible throughout, with less than a 30s disruption?
a. Was a verbal warning provided prior to disconnecting the key line, tube, wire or cable?
How long did take to stabilize the patient (from the time the patient first arrived at the receiving unit to the time the verbal handoff started)?
min
Did a patient related issue increase the overall time stabilize the patient?
Was the patient situated, stable and comfortable at the receiving unit prior to the verbal handoff?
39
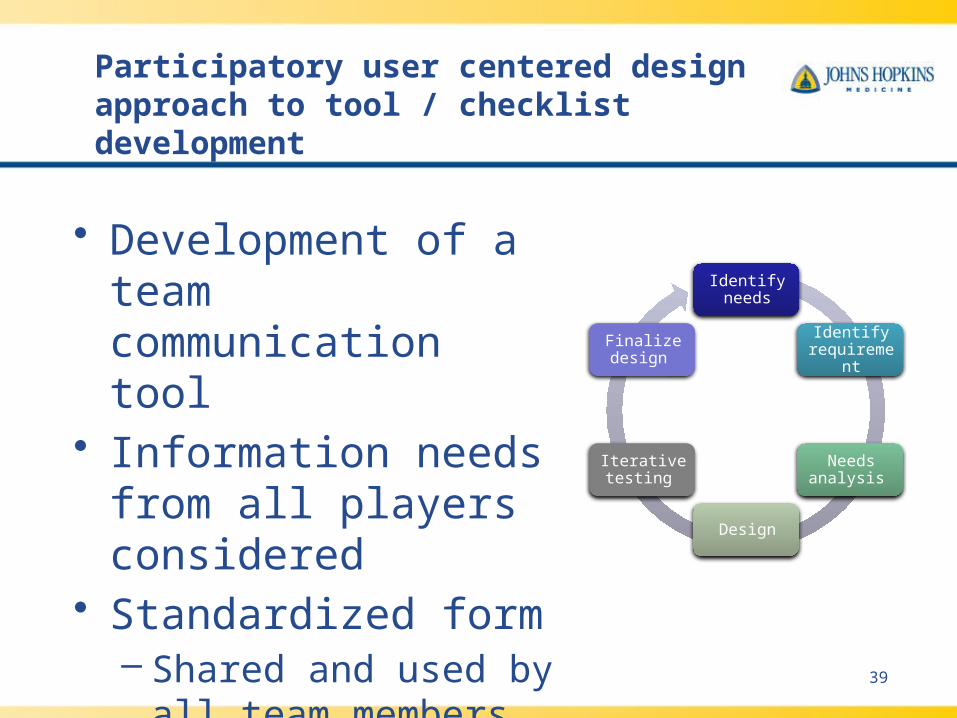
Participatory user centered design approach to tool / checklist development
Identify needs
Identify requirement
Needs analysis
Design
Iterative testing
Finalize design
• Development of a team communication tool
• Information needs from all players considered
• Standardized form– Shared and used by all
team members


















