Improving the interface between home, hospital and aged care Professor Helen Bartlett Australasian...
35
Improving the interface between home, hospital and aged care Professor Helen Bartlett Australasian Centre on Ageing The University of Queensland Presentation to the 2006 Healthcare Providers Conference,11-13 September 2006 Christchurch, New Zealand
-
Upload
griffin-stone -
Category
Documents
-
view
214 -
download
0
Transcript of Improving the interface between home, hospital and aged care Professor Helen Bartlett Australasian...

Improving the interface between home, hospital and aged care
Professor Helen BartlettAustralasian Centre on AgeingThe University of Queensland
Presentation to the 2006 Healthcare Providers Conference,11-13 September 2006
Christchurch, New Zealand

Outline
1. What are the current challenges facing the aged care sector in Australia?
2. What are the issues at the home, hospital and aged care interface?
3. How should the system respond?4. What lessons do recent pilot projects and
innovations offer for future models? 5. What is the evidence base to inform future
directions?

Changing structure of the Australian Population
Source: Productivity Commission 2005

Source: ABS, Population Projections 2004-2101 (Cat 3222.0)
Demographic shifts in the Australian population

The drivers for change• Increasing numbers of older people with high
dependency levels• Rising cost of aged care: $8.3 billion in 2003/4 to $30.6
billion in 2022/23 – dementia greatest cost• Shift towards home care over past decade – formal plus
informal care costs less then institutional care• Shortage of skilled workforce• Decrease in availability of women to provide informal
care • Fragmentation of services - access issues, duplication
of assessment, unmet need• Changing needs and expectations of older people –
greater choice, control, individuality, remaining in own home

Policy context: “Achieving World Class Care”
“For the oldest Australians with multiple complications and co-morbidities, models of care will be required at the local level to ensure quality, integrated care”
“If community care and step-down care, including rehabilitation, were built into an interrelated care system, then following hospitalisation some older people might only need to access high level care on a short term rather permanent basis”.
“Better resourcing and linking of existing care health services such as hospital based geriatric medicine and rehabilitation services, community care services and GP services would be another way of integrating care for older people with chronic conditions who wish to remain in the community”.
“Reform options should look at how existing systems and programs might be better organised or differently funded to support integration of care …at the local level as well as state and national levels”.
Ref: National Strategy for an Ageing Australia (2002)

Policy context
• ‘Ageing in Place’ - policy goal since mid-1980s
• Community Care – A Discussion Paper (2003)
• A New Strategy for Community Care: The Way Forward (Commonwealth DoHA, 2004)
• Australian Local Government Population Ageing Action Plan 2004-2008
• Hogan Review (May 2004)
• AHMAC Care of Older Australian Working Group: From Hospital to Home (July 2004)
• Aged Care Amendment (Transition Care and Assets Testing) Bill 2005

Community Care
Low Care
50 130
ExtendedAged Care at Home
1125
High Care101 780
Community Aged Care Package28 899
Respite Care
48 295
Home and Community
Care537 000
Residential Care
Veterans Home Care – 61600 veterans received a serviceMultipurpose Services - 2093 RAC places & 447 CACPs were available at June 2004
Aged Care Services in Australia 2005

Source: Australia’s Welfare 2005, AIHW
Use of aged care services by the oldest old, Australia 2003-04

Trends in provision
• hospital beds decreased between 1985-2001;
• residential care places increased in number, but relative to population decreased.
• Increase in community care investment, but high care places decreased, low care remained the same.
• Community care aged packages increased
• % of older people in hospital the same as 10 years ago
• Length of stay decreased in very old, not changing in young

Why is the hospital / home interface important in aged care?

70+ in the Community(nil, informal care,
formal care HACC CACPEACH, on PRAC EntryList, on Hospital W ait
List)New Pop 70+(male,female)
70+ in overnightHospital
(acute, sub-and non-acute care)
Hospital ACATAssessment
Die
70+ in overnight Hospital
awaitingPermanent
Residential AgedCare
(high,low )
70+ in
PermanentResidential Aged
Care(high, high in low , low )
Die
Return toPRAC
PRAC toovernightHospital
Die
Die
Return toCommunity
(nil orassistance)
PRACEntry
OvernightAdmits
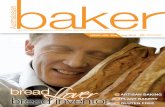
Exploring the acute- aged care interface
(diagram courtesy Geoff McDonnell, Adaptive Care Systems & Len Gray)

Issues at the interface
• Poor coordination and lack of integration at service provider and government levels
• People waiting for permanent care – approx 2,000 waiting in hospital beds for RAC
• Pressure to make transitions from hospital to residential care• Expected to recover more quickly than reasonable• Some hospital admissions are unavoidable• RAC admission may be premature• Poor access to hospitals from residential aged care• Access blocked to hospital for frail older people• Access to rehabilitation and sub-acute care poor• Role of rehab, convalescent and sub-acute care and links with
acute care needs strengthening

Some Australian initiatives

Coordinated Care Trials
First round• 9 trials in 6 states and Territories funded,
including 4 trials among ATSI involving 6600• 10967 intervention and 5571 control participants• Ran from 1997-1999• Intervention varied by trial based on different
models of care coordination, care planning and funds pooling
Second round• 6 trials (3 general, 3 Aboriginal community) • Started in late 2002 for 3 years.

Coordinated Care Trials:success or failure?
RESULTS• mixed success in implementing key strategies • Stakeholders did not fully endorse the trial's key goals and
strategies • general practitioners were unable to become effective purchasers• increased gatekeeping was never fully realised• cost-saving strategies were not taken up• improvements in continuity of care were impeded by limited provider
networks and GP reluctance to collaborate with other providers
CONCLUSIONS • uncovered need and patients liked them• not operationalised• use of market mechanisms insufficient for motivating behaviour
change

Hospital in the Home (HITH)
• Provision of hospital care in own home• Remain as inpatients under care of treating hospital
doctor• Seen by nurse or doctor at least once a day• May have access to staff at nights and weekends• Receive the same treatment as in hospital• May be all or part of treatment• Voluntary• No additional charges• Started in Victoria in 1994 as pilot project

Total HITH patient days for private & public hospitals and as % of total
hospital days
NSW 325,544 (4.2%)
Vic 14,328 (0.23%)
Qld 12,977 (0.28%)
WA 44,499 (2.16%)
Source: Aust Hosp Stats 2004-2005, AIHW

Benefits of HITH
Patients prefer home based treatment than hospital
Better management of hospital resourcesCheaper than hospital care in many cases

Future directions

National Action Plan for Older People
1. Older people have access to an appropriate level of health and aged care services
2. Services are shaped around their diverse needs3. Admissions to hospital or residential care are prevented
where avoidable4. Access to transition care services within acute-aged
care continuum5. Integrated suite of services across acute-aged care
continuum6. Skilled responsive, sufficient workforce7. Informal and family carers well equipped to provide
support and care
Ref: AHMAC 2004

Key initiatives proposed
• Emergency room interventions to target older people• Strengthening discharge planning and post-acute care• Strengthening community care and respite services• Data linkage to include acute, sub-acute, aged care and
community care datasets – e.g. WA• National minimum datasets• Best Practice Assessment Guide for the Care of Older
People in Health Services Settings• Care pathways for stroke and delirium• Extended ACAT model and link with general practice
Ref: AHMAC 2004

Models for the hospital/home interface
Wide range of potential ‘hospital outreach’ programs proposed to fully integrate hospitals with other elements of the health system:
• GP emergency clinics for older patients• Hospital based ambulatory are unit connecting
patients to full range of community heath/wellness services
• Post acute care services outside hospital• Hospital in the home or residential care• Rapid outreach programs
Ref: National Care Alliance May 2006

Transition Care in the Australian Context
“short term support and active management for older people at the interface of the acute/sub-acute and residential aged care sectors…the program also includes transition care provided in a community based setting…”
Australian Department of Health and Ageing 2005 - The Australian Government Transition Care Program

Definitional confusion
intermediate care step-down care convalescent rehabilitation interim care transitional care

The Transition Care Program
2,000 new transition care places over 3 years for people who have been in hospital
Federal and State/Territory Government partnership
Focus on recovery & maintaining function & facilitating long-term care arrangements
Smooth transition from acute/sub-acute services to aged care services - RAC or community
Assessment by Aged Care Assessment Team (ACAT)
8-12 week program
Interdisciplinary input (nursing, therapy, medical, personal) coordinated by care manager
Delivered in residential aged care or community setting
Funded to enable flexible packages of services during transition

The Australian evidence on Transition care
• Post-acute transition care program in Victoria reduced subsequent utilisation of hospital beds (Lim 2003)
• Nursing home-based interim care service in SA reduced length of stay in referring acute hospital (Crotty 2005)
• Home Rehab Support services in SA (ATA-HRSS) reduced admission to long-term care (Kroemer et al 2004)

The evidence gap
• Uncertainty about the impact of transition style programs
• No formal costing analysis
• Limited evidence about clinical outcomes
• Little insight into satisfaction and quality of life from client’s and carer’s perspective
• Impact of social factors on transition to residential care not known

Other questions
• What are the perspectives of transition care users?
• Can it meet the needs of people with dementia and mental health problems?
• Doe its reach people who are homeless?• How is the model applied in rural and
remote areas?• Is the model sufficient for frail older
people?

Is transitional care the answer?
“…as a long term goal the need for transitional beds should remain modest. If there are adequate places in residential aged care facilities and enough community support packages, coupled with good rehabilitation and post acute services in the community or in residential aged care facilities, there should not be a large number of transitional care places”.
Ref: National Aged Care Alliance (May 2006) AHMAC and Beyond – A Strategic Framework for Health Care for Older People

Lessons from intermediate care in UK
Many success factors, e.g. reduction in hospital bed usage BUT:
• Diversity of schemes managed at local level• Led to confusion and fragmentation• Duplication of effort• Reduced cost-effectiveness• No decrease in hospital bed admissions• Weak primary care engagement• Limited evaluation of personal outcomes for patents and
carers• Patients with cognitive impairment excluded
Ref: Joseph Rowntree Foundation 2003

Integration of transition services?
Source: Howe et al, 2002

Expanding the evidence base
Transition Care: Innovation and Excellence
NHMRC Health Services Program Grant: 2006-2011
- University of Sydney (Cameron)
- Flinders University (Crotty)
- University of Qld (Grey, Bartlett)

Objectives of Transition Care Research Program
1. Evaluate the impact of transition care and service integration models on older people and their carers, as well as the use of resources and costs of the services in three states
2. Evaluate the implementation and operation of transition care and service integration models by determining conditions that would assist/inhibit implementation from the viewpoint of older people, their carers and formal caregivers
3. Develop and validate quality, cost and continuity of service indicators for transition care and service integration models in different settings

• Stage 1: development of a classification of models of transition care- review of literature- Mapping programs in each state and demand/unmet need- cost analysis- journey mapping: client/patient outcomes, perceptions and experiences
• Stage 2: Evaluation of models of transition care
• Stage 3: Changing policy and practice