Improving IYCF Through Social and Behavior Change Approach. Yewelsew.pdf · 66.7 72.4 98.1 37.4 6.3...
27
Improving IYCF Through Social and Behavior Change Approach Presenter: Yewelsew Abebe, Alive & Thrive, FHI 360 Addis Ababa Ethiopia
Transcript of Improving IYCF Through Social and Behavior Change Approach. Yewelsew.pdf · 66.7 72.4 98.1 37.4 6.3...

Improving IYCF Through Social and Behavior Change Approach
Presenter: Yewelsew Abebe, Alive & Thrive, FHI 360 Addis Ababa Ethiopia

Content Outline
1. Introduction
2. Objectives
3. Results and discussion
4. Conclusions and recommendations

Introduction
Promotion of appropriate IYCF: Recommended intervention for growth & development A priority agenda of the NNP
Alive &Thrive promoted appropriate IYCF through the HEP: To mothers with under two children With IFHP & other partners: Involving HEWs & volunteers At health posts, home visits, community
Federal and regional level advocacy
Overall aim is supporting the governments NNP especially Strategic Objectives 2

Objectives
Improve IYCF by: Maintaining high rates of exclusive breastfeeding Improving complementary feeding practices
Areas of operation: In four large regions: Amhara, Oromia, SNNPR, Tigray
Impact evaluation involves: 2010 baseline vs 2014 end line ( SNNPR & Tigray) Evaluation by IFPRI evaluation team

A&T’s SBCC Approach to Scaling up IYCF
4
1
3
2

Interpersonal communication
Mothers practicing the 7 key IYCF messages on the child nutrition card

Community mobilization
Strengthening social norms around IYCF practices

Mass communication: Delivering Similar IYCF messages in different language
Radio and television spots
Drama based on agrarian analogy were used

MethodologyImpact evaluation ( community & mass media) involves:
An “ adequacy evaluation design” i.e.,
“ Were the program goals achieved?”
Involving pre-& post interventions / without comparison group
Conducted by IFPRI Evaluation
Data analysis methods : Estimation of changes in :
1. In IYCF practices between baseline & end line
2. Among program impact pathways – exposure to uptake
3. Dose-response analysis between program exposure and IYCF practices
4. In child nutrition outcomes between baseline & end line
5. underlying determinants – child, maternal, and household level factors

Methodology: Study Areas
Random selection of 75 enumeration
areas† from 56 woredas
89 IFHP woredas in 2 regions (Tigray & SNNPR)
Cross-sectional endline survey (2014)
Process evaluation survey on implementation and utilization (2013)
Cross-sectional baseline survey (2010)
Process evaluation (qualitative study) on implementation in 8 woredas (2012)
† 75 enumeration areas from 19 woredas in Tigray and 37 woredas in SNNPR.
Household sample 0-5.9 mos: n=6196-23.0 mos: n=87524-59.9 mos: n=1475oversample 24-35.9 mos: n=727
Household sample 0-5.9 mos: n=6076-23.0 mos: n=88324-59.9 mos: n=1502

Results & Discussion
11
Infant & Young Child Feeding Practices

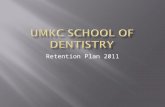
66.7
72.4
98.1
37.4
6.3
45.6
4.6
2.1
81.7
82.8
95.6
59.7
12.4
70.3
10.1
4.1
0 20 40 60 80 100
Early initiation of BF (within 1hour of birth)
Exclusive BF among childrenunder 6 months
Continued BF at 1 year
Introduction of solid, semi-solidor soft food
Minimum diet diversity (≥4 food groups)
Minimum meal frequency
Minimum acceptable diet
Consumption of iron-rich food 2010 2014
IYCF practices( WHO Indicators) increased significantly among children 0-23.9 months
12†Percentage point; adjusted for cluster; *p<0.05, **p<0.01, *** p<0.001
% PP change†
15.0***
10.4***
-2.5
22.3***
6.1***
24.7***
5.5***
2.0*

TIMELY
0
2
4
6
8
10
12
14
16
18
Ch
ild a
ge (
mo
nth
s)
2010 2014
Timely introduction of most liquids and foods improved among children 0-23.9 months
13adjusted for cluster; *p<0.05, **p<0.01, *** p<0.001
*** *** * *** *** *** *** *** *** *** ***

Consumption of most food groups in last 24 hours increased among children 6-23.9 months
14
%
82.9
20.2
32.8
1.5
9.6
20.3
4.1
88.9***
34.9***31.0
3.3*
18.9***
27.0**
4.9
0
20
40
60
80
100
Grains, roots,tubers
Legumes andnuts
Dairy products Flesh foods Eggs Vitamin A-richfruits and
vegetables
Other fruitsand vegetables
%
2010 2014
adjusted for cluster; *p<0.05, **p<0.01, *** p<0.001

Moderate reach of interventions to target households (mothers with <2yrs) achieved
31.5
12.2
30.3
7.2
44.6
31.230.8
11.2
72.5
8.814.1
38.1
11.5
0
20
40
60
80
100
HEW homevisit in last 6
mos
HEW talkedabout IYCF at
last visit
Volunteerhome visit in
last 6 mos
Volunteertalked about
IYCF at last visit
Ever seen CNC Fooddemonstration
in last 6 mos
Villagegathering onIYCF in last 6
mos
Ever heard anyradio spot
Ever seen anyTV spot
%
2010 2014
Interpersonal communication Social mobilizationMass media

Both HEWs and volunteers are needed to optimize reach to target households
HEW25%
Volunteer
11%HEW&Vol20%
Neither44%
N=1494
Implication: Build the capacity of HDAs to deliver appropriate health messages!
Exposure to home visits in last 6 months among mothers with <2-y-o, 2014

IYCF knowledge among HEWs increased over time
17
2010 2014
WHO IYCF Indicators Tigray(n=25)
SNNPR(n=48)
All(n=73)
Tigray(n=48)
SNNPR(n=90)
All(n=138)
Breast feeding Put the baby on breast immediately (<1 hr after birth) 100.0 100.0 100.0 95.8 98.9 97.8***
Give colostrum to baby 88.0 89.6 89.0 77.1 96.7 89.9*
Water should not be given even in hot weather 92.0 89.6 90.4 95.8 98.9 97.8***
Mothers can give expressed milk if she needs to leave the baby <6 mos 44.0 33.3 37.0 70.8 96.7 87.7***
Complementary feedingAt 6 mos babies should first start to receive foods 96.0 97.9 97.3 97.9 100.0 99.3***
Special food to complement BF: Enriched porridge with egg 20.0 14.6 16.4 64.6 53.3 57.2***
A 6–9-mo-old child should eat at least 3 times per day 88.0 95.8 93.2 97.9 97.8 97.8***
A 12–23-mo-old child should eat at least 3 times per day 96.0 93.8 94.5 100.0 100.0 100.0***
*p<0.05, **p<0.01, *** p<0.001

What were the key exposure indicators of A&T interventions?
Type of intervention Exposureindicator (Y/N)
Intensityindicator (varied)
Interpersonalcounseling
1- Received home visit by HEW to discuss about IYCF in last 6 mos
Number of home visits in last 6 months
2- Received home visit by community volunteer to discuss IYCF in last 6 mos
Number of home visits in last 6 months
3- Ever seen Child Nutrition Card (CNC) with 7 IYCF actions (BF: 1-2, CF: 3-7)
Number of CNC messages recalled
Group education/ social mobilization
4- Attended in village gatheringdiscussing about IYCF in last 6 mos
---
Mass media 5- Ever heard radio spot (BF spots 1-2, CF spots 3-6)
No. of radio spots heard No. of radio spot messages
recalled
= Overall program intensity score (0-5)

Higher intensity of BF radio spot exposure and program intensity score associated with early initiation of BF
80.5 82.695.5
0
20
40
60
80
100
None 1 message 2 messages
%
BF radio messages recalled**
76.3 81.4 82.1 91.7
0
20
40
60
80
100
None Low(1 exposure)
Medium(2-3 exposures)
High(4-5 exposures)
%
Program intensity score**
Indicator Odds ratio1
Intensity of BF radio spot exposure:
None ref
1 BF message recalled 1.17
2 BF messages recalled 4.91**
Program exposure intensity:
None ref
Low (1 exposure) 1.3
Medium (2-3 exposures) 1.21
High (4-5 exposures) 2.60**p<0.05, **p<0.01, ***p<0.0011Fully adjusted model
(n=193) (n=480) (n=100)(n=445)
(n=1044) (n=90)(n=84)

Higher intensity of volunteer home visits, CNC exposure, CF radio spot exposure, and program intensity score
associated with minimum diet diversity
Indicator OR1
Intensity of CF radio spot exposure:
None ref
1-2 CF spots heard 2.47*
3-4 CF spots heard 3.37**
None Ref
1-2 CF messages recalled 2.94**
3-4 CF messages recalled 2.04
Program exposure intensity:
None ref
Low (1 exposure) 2.28
Medium (2-3 exposures) 3.45*
High (4-5 exposures) 11.81**
Indicator Odds ratio1
Intensity of volunteer home visits:
None ref
1-2 visits in last 6 mos 1.41
3+ visits in last 6 mos 2.15*
Intensity of CNC exposure:
None ref
1-2 CF messages recalled 1.54
3-5 CF messages recalled 4.16**
*p<0.05, **p<0.01, ***p<0.0011Fully adjusted model
Similar patterns for minimum acceptable diet

Small but significant change in stunting only among children 24-59.9 months
55.9
30.2
4.4
51.5
28.4
3.8
0
20
40
60
80
100
Stunting Underweight Wasting
%
2010 2014
-1.7 pp, p=0.31
-0.6 pp, p=0.47
*p<0.05
-4.4 pp, p=0.04
*

Conclusion & Recommendations
22
“ Our children are not getting sick any more, children are not dying these days as before”.

Conclusion
IYCF practices improved significantly over time in intervention areas.
EBF increased, MDD doubled,
Gaps remain in consumption of >4 food groups & iron-rich foods
Higher intensities of program exposures i.e., radio spots, volunteer home visits , CNC exposure are associated with
Early initiation of breast feeding
Minimum diet diversity
Minimum meal frequency
Minimum acceptable diet

Recommendations
1. Ensure higher intensity of contacts for long term change in IYCF
practices
2. Target multiple actors- particularly household influentials
3. Use multiple SBCC approaches and channels than using one
4. Use community friendly tools & job aids for increased knowledge &
quality of contact

Building on Lessons Learned in Phase 2
25
In collaboration with the RHB refined IPC tools to improve coverage at community level
Planned to Increase the intensity of contacts by working through health and agriculture systems
Intensifying the learning around
the community component

Acknowledgements
• IFPRI MLE team
• Tigray and SNNPR: Regional health bureaus, woreda health
offices, and study participants
• Data collection by Addis Continental Institute of Public Health
• Funded by Bill & Melinda Gates Foundation, through A&T,
managed by FHI360; and by the CGIAR A4NH, led by IFPRI.

Thank you