Improving Delivery of the Direct Enhanced Service in Haringey Dylan Kerr, Alcohol Nurse Manager,...
24
Improving Delivery of the Direct Enhanced Service in Haringey Dylan Kerr, Alcohol Nurse Manager, HAGA Laura Pechey, Brief Interventions Specialist, HAGA
-
Upload
jodie-gilmore -
Category
Documents
-
view
219 -
download
0
Transcript of Improving Delivery of the Direct Enhanced Service in Haringey Dylan Kerr, Alcohol Nurse Manager,...

Improving Delivery of the Direct Enhanced Service in
Haringey
Dylan Kerr, Alcohol Nurse Manager, HAGALaura Pechey, Brief Interventions Specialist, HAGA

What is IBA?
• Identification and Brief Advice• Also known as Screening and Brief Interventions
(SBI)• Identification of risk using a screening tool• Short structured interaction for Increasing and
Higher Risk drinkers• Delivered by Tier 1 practitioners• Extended Brief Interventions for Higher Risk
drinkers• Referral pathway for dependent drinkers

Efficacy of IBA• Extensive evidence base: more than 56 controlled trials
(Moyer et al 2002; Cochrane Review 2007)
• 1 in 8 people who receive simple alcohol advice will reduce their drinking to within Low Risk levels (Moyer et al., 2002)
• Significant reduction in alcohol-related and alcohol-specific hospital admissions across regions
• On-going Screening and Intervention Programme for Sensible Drinking (SIPS) project in primary care, A&E and criminal justice settings

Why IBA in Primary Care Settings?
• Key setting• “Trust transfer”• Alcohol-related GP attendance (i.e. GP
“frequent flyers”)• Removal of stigma• High impact (i.e. patient numbers
reached)
Roadblocks within Primary Care
• Time• Whose responsibility?• Commitment• Skills and training• Varied quality and style • Process• Tools• Lack of clear, up-to-date and concise DES
guidance document
Local Enhanced Service
• Alcohol Harm Reduction Strategy (2004)
• Local package targeted at meeting needs of population
• Screening of existing patients and deliver of Brief Advice
• Payment locally agreed

Direct Enhanced Service
• Introduced in 2008
• Government incentive
• Screening of all new registrations (+16)
• FAST or AUDIT-C tools
• £2.33 payment for screening

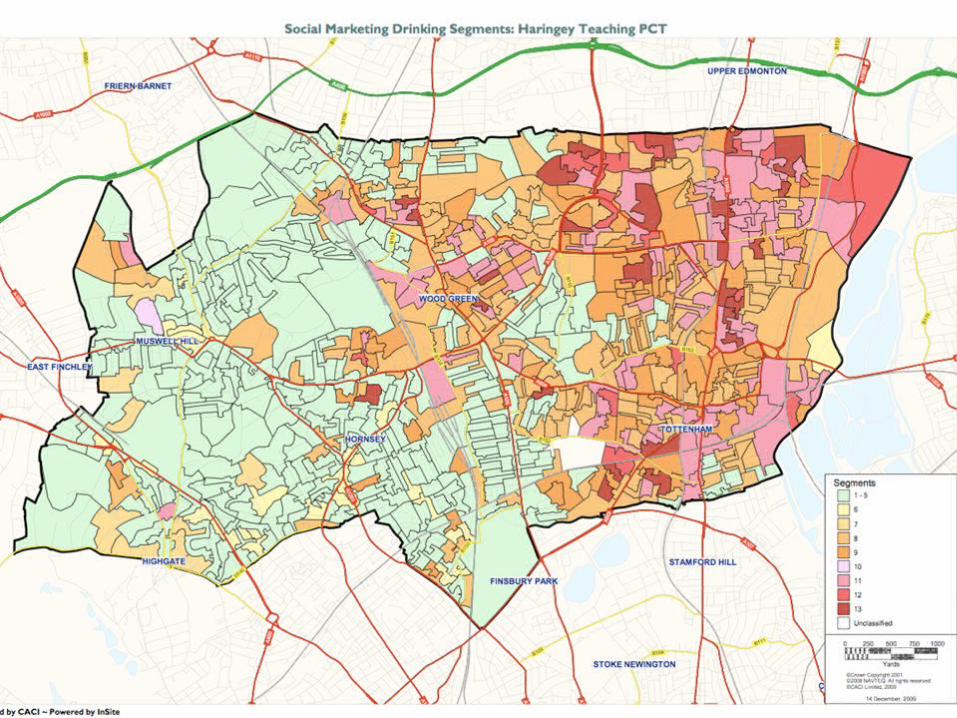
Haringey: The Local Picture

Local Alcohol Profiles
• Highest male mortality rate in London from alcohol-attributable causes (NWPHO 2008)
• 2nd worse liver disease mortality rate in London (NWPHO 2008)
• Patients at North Middlesex A&E (2007 ten-day review)– 52% of male patients drink at Increasing Risk levels– 21% of female patients drink at Increasing Risk levels– 13% of patients dependent drinkers
• Dept of Health drinking estimates (2010): – 37,153 adults Increasing Risk drinkers (16.5% of
Haringey pop)– 11,379 adults Higher Risk drinkers (5%) – 6,132 dependent drinkers (2.3%)– 26,923 binge drinkers (12%)
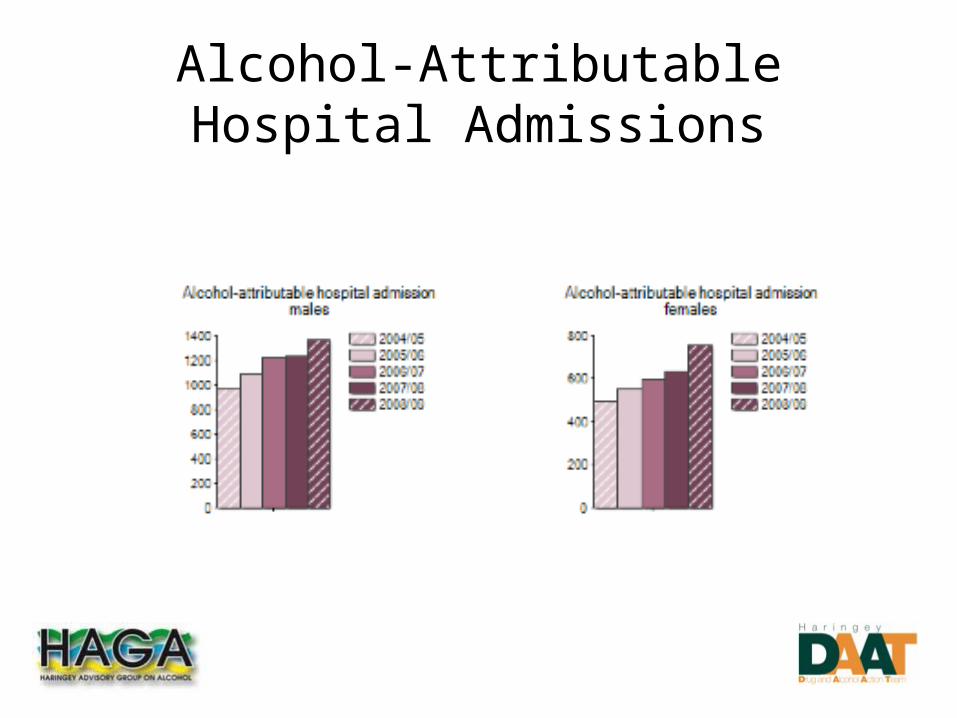
Alcohol-Attributable Hospital Admissions

DES Review
09-10 DES Returns• 29 practices in Haringey provided the Alcohol DES
during 2009-10 • % of new registrations screened under DES varies
considerably • Only 2% of the newly registrations screened
positive and required a brief intervention (347 patients)
• 1/2 identified zero patients requiring a brief intervention
• We would expect 25% of patients to be drinking at Increasing or Higher Risk levels (around 5,038 newly registered patients)

AUDIT-C Screening 2009-2010

Screening Relative to Intervention
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
8 10 12 14 15 16 17 21 24 22 27 29 19 9 7 13 6 2 11 3 1 18 23 28 26 25 4 20 5
practice
% p
atie
nts
scr
een
ed
% screened given brief intervention % screened 'positive' so given full AUDIT % screened negative
Purpose of Review
• To understand the reasons for wide variation in outcomes reported by Haringey practices
• To identify the areas where practices need additional support and training

Practice Selection
• Practices who provided a particularly high or low no. of brief interventions
• Practices who reported 20-40% positive scores as expected
• Practices with particularly unusual results or which appear to be taking a different approach to the DES and may have learning to share with others

Key Findings
1. Incorrect screening process
2. Re-registrations
3. Interventions and referral pathways widely lacking or inadequate
4. Coding

Improvements Made So Far
• Review new registration forms • Standardised local IBA tools in use• Rolling programme of IBA training• IBA Pathways agreed with practices• Training HCAs & nurses in Extended Brief
Interventions• Flagging 8+ scores to GPs• Uniform appointment booking for scores 20+• Reviewing coding with Practice Managers

Best Practice Guidance
• Review cited as example of best practice in J. Currie Intensive Support in Reducing Hospital Admissions (2010)
• We hope that the learning from the review will improve practice nationally

Local Primary Care IBA Initiatives

Social Marketing Project
• Stalls in 12 locations over 12 months
• Alcohol Social Marketing
• Identification & Brief Advice delivered
• Extended Brief Interventions appts
• Training in IBA for primary care
Extended IBA Project
• Two GP practices participating
• Patients on identified disease registers
• Identification & Brief Advice delivered by HCA/GP/nurse
• Extended Brief Interventions clinics run by HAGA
• Training in IBA and EBI

References
• Cabinet Office. (2004) Alcohol Harm Reduction Strategy for England.
• Currie, J. (2010) Intensive Support in Reducing Hospital Admissions: A Report Describing Intensive Support Provided to Ten London Primary Care Trusts (pct)/Drug and Alcohol Action Team (DAAT) Partnerships, London Regional Alcohol Group.
• Kaner E, Beyer F, Dickinson H, Pienaar E, Campbell F, Schlesinger C, Heather N, Saunders J, Bernand B. “Brief interventions for excessive drinkers in primary health care settings.” Cochrane Database of Systematic Reviews 2007, Issue 2. Art No.: CD004148 DOI: 10.1002/14651858.CD004148.pub3.
• Moyer, A., Finney, J., Swearingen, C. and Vergun, P. (2002) “Brief Interventions for alcohol problems: a meta-analytic review of controlled investigations in treatment -seeking and non-treatment seeking populations,” Addiction, 97, 279-292.