Improving Care and Enhancing Patient Safety by Researching...
45
Central CCAC Outstanding care – every person, every day Improving Care and Enhancing Patient Safety by Researching Never Events in the Community June 21 st , 2013
Transcript of Improving Care and Enhancing Patient Safety by Researching...

Central CCAC
Outstanding care – every person, every day
Improving Care and Enhancing Patient Safety by Researching Never
Events in the Community
June 21st, 2013

Central CCAC
Introductions
2
• Cathy Szabo Chief Executive Officer Central Community Care Access Centre
• Dr. Diane Doran Professor Emeritus Lawrence S. Bloomberg Faculty of Nursing University of Toronto
• The Research The Identification of Serious Reportable Events for Home Care (September 2012)

Central CCAC
Objectives
3
• The Concept: Introduce the innovative concept of a Never Event in the community setting and why it is so important
• The Methodology: Share the process and findings of our joint research study
• The Practical Application: Explore how this research can be applied to care and services in the community setting to improve safety for our patients
Through this presentation you will gain an understanding of…

Central CCAC
The Concept
4

Central CCAC
What is a Never Event?
5

Central CCAC 6
Serious
Preventable
Reportable
Applying the Concept to Home Care in the Community….

Central CCAC
Context: Why This, Why Now?
• Central CCAC Quality Framework
• Opportunity to partner with research community and home care experts to
• improve safety for patients
• identify system level solutions
• Aligns with the need for
• clearer accountability through performance measures
• increased transparency through public reporting
• Health Quality Ontario
• Quality Improvement Plans
7

Central CCAC
The Research
8

Central CCAC
Research Overview
• Title: The Identification of Serious Reportable Events for Home Care Delphi Survey
• Research team:
• Dr. Diane Doran, University of Toronto
• Dr. Ross Baker, University of Toronto
• Cathy Szabo, Central CCAC
• Research staff:
• Jennifer Carryer
• Julie McShane
9

Central CCAC
Research Objectives
1. Determine serious reportable events for home care
2. Determine characteristics of systems that have been established to identify serious reportable events
3. Generate recommendations for clinical, administrative and policy strategies
10

Central CCAC
Definitions
• Serious: An event that results in death or loss of a body
part, disability, or loss of body functioning lasting more than seven days or still present at time of discharge from home care, or - when referring to other than an adverse event - an event the occurrence of which is not trivial.
• Preventable: An event that could have been anticipated
and prepared for, but that occurs because of an error or other system failure.
• Reportable: The act of making events that should never
occur in a safe environment known to a higher authority.
11

Central CCAC
Research Methodology
• Literature review related to home care safety incidents and characteristics of successful reporting systems
• Delphi survey - 24 panelists from six provinces/ territories to determine serious reportable events
12

Central CCAC
Delphi Survey Process
• Researchers created an initial list of 30 Never Events
• Panelists
• Reviewed the list and indicated degree to which each was “reportable and preventable”
• Provided comments about the context of events, and suggested other items for inclusion
• Process generated a list of the top four most “reportable and preventable” events
13

Central CCAC
Delphi Survey Results Top Four Events*
14
* Events perceived as reportable and preventable by >90% of panelists
1. Serious injury related to inappropriate patient service plan
2. Adverse reaction requiring emergency department visit/hospitalization due to medication-related event
3. New peritoneal dialysis infection
4. Serious event related to care or services contrary to current professional or other practice standards

Central CCAC
Further Research Discussion
15

Central CCAC
Characteristics of Successful Reporting Systems
Non-punitive
Confidential
Independent
Expert analysis
Timely
Systems oriented
Responsive
16
Sources: Leape (2002), WHO (2005), Karsh et al. (2006)

Central CCAC
Patient Safety Event Learning Systems
1. Identifying events
2. Analyzing their causes
3. Taking corrective action to reduce re-occurrence of similar events
4. Providing timely feedback to those involved in the events.
17
Ginsburg et al. (2009b)

Central CCAC
1. Identifying Events
2. Analyzing Their Causes
3. Taking Corrective Action to Reduce the Re-occurrence of Similar Events
4. Providing Timely Feedback to Those Involved in the Events
18

Central CCAC
Challenges to Measuring Home Care Adverse Events
• Lack of consistent definitions between organizations
• Lack of agreement about what to focus on
• Events are usually a cumulative effect of small errors
• Not all events are caused by error
• Error rates do not measure success of safety efforts
• Concept of prevention is problematic: families participate in care and patients choose to live at risk
• Delivering care in the home is less controlled
• Different perceptions of error based on perspective
• Low rate of reporting
19
Sources: Runciman et al., 2009; Yu Nation & Dooley, 2005; Ginsburg et al., 2009a, Chuang, Ginsburg &
Berta, 2007; Johnson, 2006, Northcott et al., 2008

Central CCAC
1. Identifying Events
2. Analyzing Their Causes
3. Taking Corrective Action to Reduce the Re-occurrence of Similar Events
4. Providing Timely Feedback to Those Involved in the Events
20

Central CCAC
Classifying and Analyzing Adverse Events
• Attributing root cause is difficult due to
• Patients and families managing own care
• Patients choose to live at risk
• Events can represent larger system problems
• Lack of institutional control for care delivered in the home (vs. care delivered in hospital setting)
• Difficult for users to translate long narratives into analyzable data and track true nature of event
21
Sources: Sears, 2008; Hoffman et al., 2008

Central CCAC
1. Identifying Events
2. Analyzing Their Causes
3. Taking Corrective Action to Reduce the Re-occurrence of Similar Events
4. Providing Timely Feedback to Those Involved in the Events
22

Central CCAC
System Feedback and Change
“Learning from adverse events does not stop with the collection of data. To successfully improve patient safety, organizations must improve on the process that contributed to the adverse event”
23
Source: Doran, Baker & Szabo, 2012

Central CCAC
System Feedback and Change
• Characteristics of event, group involved and organization all impact whether learning will occur
• Keep staff informed on
• Status of the report they submitted
• What happened/ changed as a result
• Four learning responses
• Systematic - what occurred, why, how it happened
• Procedural changes resulting from event are followed up
• Individuals involved contributed to understanding/ analysis
• Individuals involved contributed to solution-generation
24
Sources: Chuang et al., 2007; Ginsburg, 2009a

Central CCAC
Researcher Recommendations
25

Central CCAC
Recommendations: Identifying Events
1. Develop a list of reportable events using Delphi list as a starting point
2. Select highest frequency/most severe events; use focused approach for specific education and improvement
3. Use positive terminology for reporting
4. Create strong incentives to report and remove disincentives and barriers
5. Encourage reporting; report “analyst” to determine required follow-up; voluntary and mandatory approaches
26

Central CCAC
Recommendations: Analysis
6. Policies and procedures that support a foundation for safety; senior managers and safety champions highly visible and engaged in process
7. Flexible, easy to access system that is used by professionals and non-professionals and supports multiple methods of reporting
8. Guiding framework or matrix for separating events related to quality and events that are a threat to patient safety
9. System to support meaningful analysis
10. Share information in meaningful ways/different formats
27

Central CCAC
Recommendations: Timely Feedback and Change
11. Give reporters immediate feedback on their report and close the loop once event is followed up on
12. Examine events in a systematic, multidisciplinary way (no blame)
13. Offer support and counseling to those involved
14. Conduct organizational learning (i.e. focus groups, newsletters, safety walkabouts etc.)
15. Continue to support best practice and standardization of home care-specific guidelines
28

Central CCAC
The Practical Application
29

Central CCAC
Central CCAC’s Quality and Safety Framework
30

Central CCAC
Quality Through
Accreditation
Initiatives Supporting Quality
31
Patient Safety
Culture Tool
Patient Safety Play
Quality Reporting
System (QRS)
Patient Satisfaction
Safety at Home
Research Study
Never Events
Research Study
LEAN/ Process Improvements

Central CCAC
Application at Central CCAC
• In alignment with our Quality Framework:
• Raise awareness among staff about the concept of a Never Event in the community and why it is important
• Identify and prioritize our own Never Events through stakeholder engagement
• Help staff connect the concept to their role
• Develop systems to track and reduce Never Events to improve patient safety
• Continue to build a patient safety culture by building on Quality and Safety framework engagement already done. (e.g., Patient Safety Play: Seeing the Forest)
32

Central CCAC
Identifying our Never Events
• Communicated about the concept of Never Events
• Conducted data analysis to assess current state
• Engaged stakeholders in focus groups
• Patients
• Quality and Safety Steering Committee
• Front-line staff
• Service providers
• Used information gathered from staff, current state analysis and selection criteria to determine primary area of focus
33

Central CCAC
Our Criteria
Serious
Measurable
Relevant (i.e. occurs or can occur)
Impact on provincially driven measures/ indicators publicly reported measures
Matches researcher findings
Everyone can relate
Affects CCAC, service providers and referral source
Within control/influence of CCAC and service provider
34

Central CCAC
Our Focus: Medication-Related Event
35
Event Type Examples
Serious injury related to
inappropriate client service plan
Incomplete, inaccurate
assessment, care plan design or
implementation
Adverse reaction requiring ER visit
or hospitalization related to a
medication related event
Wrong drug, dose, time, rate,
preparation, route of
administration
New peritoneal dialysis infection Site infection, peritonitis
Any serious event related to care
or services that are contrary to
current professional or other
practice standards
Incorrect treatment, theft, lack of
hand washing, retention of a
foreign object, individual
practicing outside scope of
competence

Central CCAC
Roles and Responsibilities Event
• Service providers and CCAC front-line staff/managers
• Goals
• Increase awareness on research and application
• Help staff connect their role to med error prevention
• Identify top drivers preventing med errors
• Inform CCAC staff/service provider education materials
• Education on Never Events and med error rates
• Root cause analysis with real cases
• Outlined roles and responsibilities to reduce errors
• ‘Parking lot’ for potential improvement initiatives
36

Central CCAC
Participant Feedback
“Great to have service providers in the room”
“Use of real cases/scenarios”
“Learning different roles and responsibilities/handoffs”
“Such a diverse group was very helpful”
• Key themes
• Ask questions – don’t assume someone else is doing this
• We all have to think big picture, not in our silos
• Challenges with transitions require extra focus/care
37

Central CCAC
Measuring Our Never Event
• Conducted data analysis to assess current state
• Established measures to track progress
• Quality Reporting System – Med Errors Category
• MSAA measures and QIP alignment
• Business plan measure around med errors
• Measurement by service provider with analysis of themes
38
Central CCAC
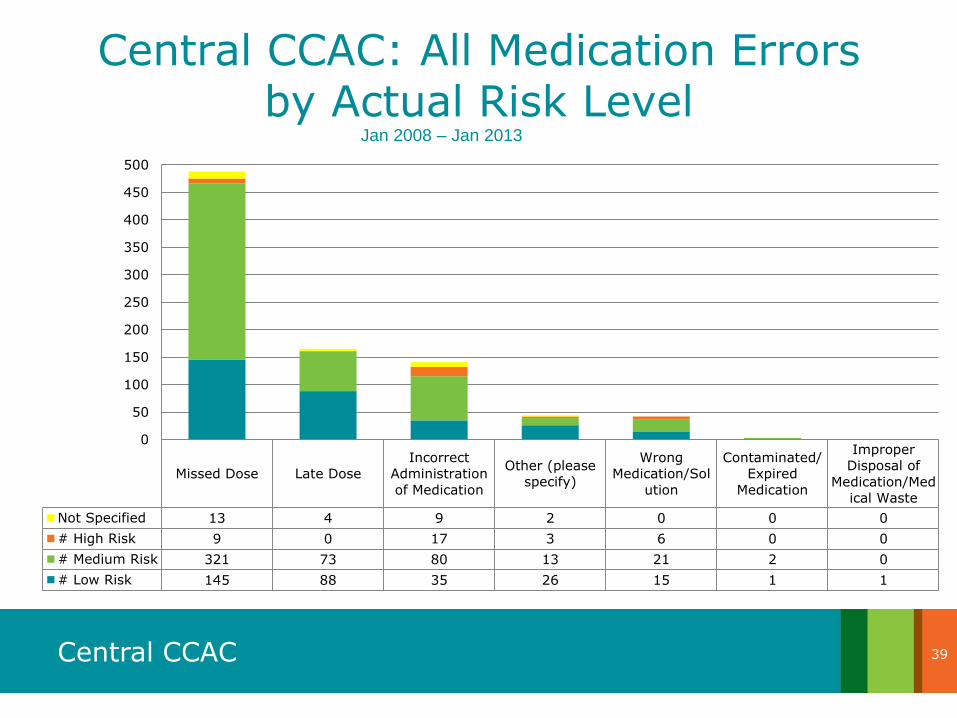
Central CCAC: All Medication Errors by Actual Risk Level
(Jan. 2008 - Jan. 31, 2013
39
Missed Dose Late Dose
Incorrect
Administration
of Medication
Other (please
specify)
Wrong
Medication/Sol
ution
Contaminated/
Expired
Medication
Improper
Disposal of
Medication/Med
ical Waste
Not Specified 13 4 9 2 0 0 0
# High Risk 9 0 17 3 6 0 0
# Medium Risk 321 73 80 13 21 2 0
# Low Risk 145 88 35 26 15 1 1
0
50
100
150
200
250
300
350
400
450
500
Jan 2008 – Jan 2013

Central CCAC
Measuring Medication Errors
40

Central CCAC
Measuring Med Error Never Events
41
# D
ays
Be
twe
en
Ne
ve
r E
ve
nts
Date
As of May
1st, 2013 it
has been
591 days
since our
last Never
Event!
Good

Central CCAC
Next Steps for Central CCAC
• Cross-functional education for staff and service providers
• Raise awareness of research and application
• Help connect their role to reduction of Never Events
• Provide a clear sense of next steps and how they can support Safety, Science, Service
• Continue measuring/tracking Never Events
• Expected a spike in # reported following education
• Use data to target process improvements and reduce medication errors
• Complete process improvement initiatives to support the reduction in medication errors
• Continue to apply the 15 recommendations
42

Central CCAC
Conclusion
43
The Concept: Introduced the innovative concept of a Never Event in the community setting and why it is important
The Research: Shared the process and findings of our joint research study
The Practical Application: Explored how this research can be applied to health care and services in the community setting to improve safety for our patients and shared our progress so far

Central CCAC
For More Information…
44
The Research Study: Diane Doran at [email protected]
Central CCAC: Deb Gollob (Improvement Advisor, Project Lead) at [email protected]

Central CCAC
Questions?
45