IMPROVING ACCESS TO EMERGENCY OBSTETRIC AND PERINATAL CARE IN GHANA
34
E. Y Kwawukume Professor and Chair, K.K. Bentsi- Enchill Chair, University of Ghana Medical School, College of Health Sciences, Dept of Obst and Gynae, Korle Bu
description
IMPROVING ACCESS TO EMERGENCY OBSTETRIC AND PERINATAL CARE IN GHANA. E. Y Kwawukume Professor and Chair, K.K. Bentsi-Enchill Chair, University of Ghana Medical School, College of Health Sciences, Dept of Obst and Gynae, Korle Bu. INTRODUCTION. - PowerPoint PPT Presentation
Transcript of IMPROVING ACCESS TO EMERGENCY OBSTETRIC AND PERINATAL CARE IN GHANA

E. Y KwawukumeProfessor and Chair, K.K. Bentsi-Enchill Chair,
University of Ghana Medical School, College of Health Sciences, Dept of Obst and Gynae,
Korle Bu

The main indices of quality obstetric and perinatal care in a given geographical location are maternal and perinatal mortality.
WHO estimates that at least 1,600 women die every day associated with pregnancy and child birth.
90% of these deaths occur in sub-Saharan Africa and Asia.
Annual del KBTH is between 10,000 to 12,000 women.
About 36% of the pregnant women with complications reach the hospital in a moribund state

40% or more of pregnant women may experience acute obstetric problems during pregnancy, child birth and puerperium.
Of this number an estimated15% of the pregnant women develop life-threatening complications.
Significant percentage of the maternal deaths is therefore due to emergency complications of pregnancy.
This is a descriptive study. Data was collected from published articles
including studies from 1984 to 1994 and 1995 to 2002,
records were retrieved from the depart of Obs/Gynae and Child Health, KBTH
Ghana Statistical Service, Ministry of Health Human resource Division
University of Ghana Medical School.

Year Total deliveries Live births Still Births SB/Live
births% 2002 11,798 11,122 676 5.7
2003 10,528 9,901 627 6.3
2004 11,099 10, 392 707 6.8
2005 11,175 10, 443 732 7.0
2006 7,229 7,624 395 5.2
2007 7,378 6,993 385 5.5
2008 10,310 9,785 525 5.4

Year Live births Maternal deaths MMR
2005 10,443 95 909 2006 7,624 62 813 2007 6,993 72
1,029 2008 9,785 77 786 2005-2008 - - 884
MMR/100,000Most of the cases are referrals from the district

Year Rate 1984-1994 734.4 1995-2002 777.2 2003-2008 884.2

Causes 1984-1994. 2005-2008 Hemorrhage 17.7% 30.0%
Hypertensive disorders 17.5% 25.8%
Abortions 13.5% 10.7% Genital infections 9.5% 3.5% Obstructed labour 5.5% 0.3% Others 36.3% 29.4%Causes of MM remain the same but there is
significant increase in the major causes, ie hypert and haemorrage

Year Rates .
1991 99.1 1992 99.8
2008 80.7 The perinatal mortality rate showed 18.4%
decrease as compared to the year 1991.

Causes Number
Prematurity 145 Birth Asphyxia 121 Bacteria Sepsis 6

Causes year
1990 1992 1991/1902 2008
Prematurity 52.1% 55.3% 58.8% 53.3%
Birth asphyxia 26.7% 19.1% 23% 44.4%
Bacteria sepsis 11.6% 14.6% 13% 2.2%

Languages Women Men
English/other languages 45.7% 62.9% English/one Ghanaian language 27.2%
41.6% More than half of the population in Ghana is
illiterate. The literacy rate of women is lower than that
of men.

Sex Number Women 11,816,192 Men 11,600,326 Total 23,416,518 The population of women and men is almost
equal with the women having a slight edge over the men

Staff Number % Population Ratio . Nurses 14,297 0.1 1 to 1,000
women Doctors 2,334 0.02 1 to 5,000
women There is a geographical there are regional
variation from the North to the South

Year enrolled No Year graduated No
graduated
1999 83 2005 77 2000 89 2006 87 2001 90 2007 83 2002 89 2008 88 2003 111 2009 105 An average of 88 doctors is produced annually
since 1999.

Year No. Obstetricians No. Pediatricians 2006 3 6 2007 - 1 2008 2 1
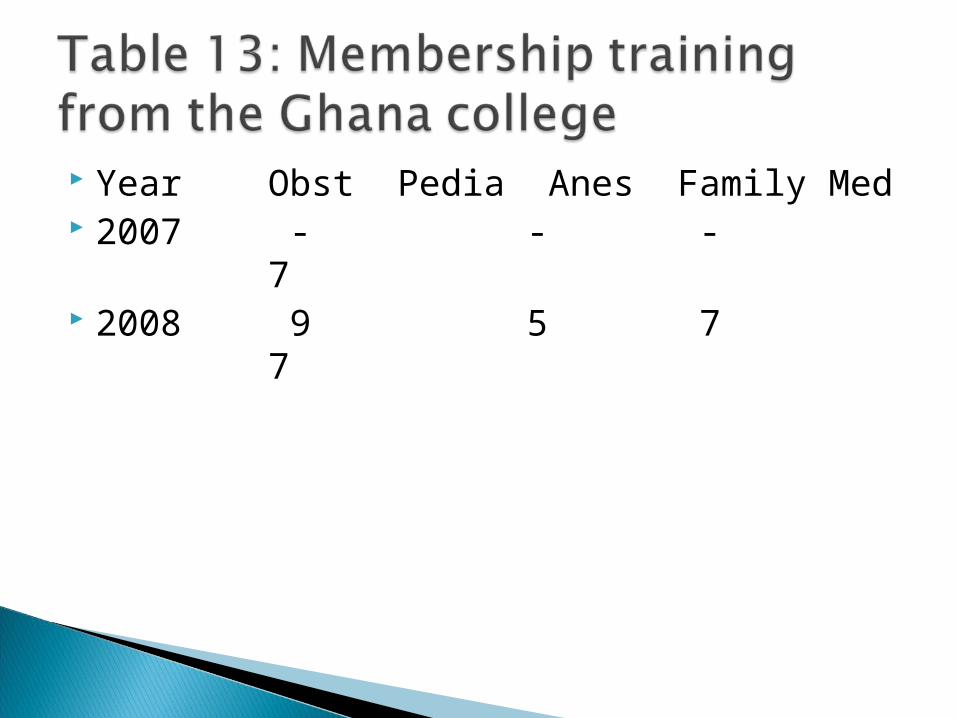
Year Obst Pedia Anes Family Med 2007 - - - 7 2008 9 5 7 7

MMR of 884.2 per 100,000 live births and the perinatal mortality rate of 80.7 per1,000 births are high compared to that obtained in the developed countries.
The causes of maternal and perinatal mortality have remained the same
the major causes of maternal mortality, hemorrhage and hypertensive disorders of pregnancy, showed a significant percentage increase.
These causes are emergency obstetric and perinatal conditions.

More than half of the population of Ghana are illiterate .
The illiterate population is less likely to lead a healthy life style.
They are also less likely to make use of available health services.
Clinical features of complications of pregnancy may not be recognized and as such may be misinterpreted and report late for treatment.

Poverty is a high risk factor It is associated with illiteracy and impedes
access to health care. The global economic situation is not in favor of
the developing countries. This situation has been worsened by bad
governance; bad developmental policies and corruption
The majority of the population is therefore poor. When complications arise there may be no
money to finance transportation and medical bills.
The patient may not be taken to a health care facility.

Due to physical distance, Poor road networks, Inadequate ambulance services.

lack of medical supplies and equipment, non functioning theaters shortage of medical staff. From the study the ratio of a nurse to the
women population is 1:1000 doctor to the women population 1:5000. This is woefully inadequate leading to
MM/PNM.

Measures presently taken to address the situation are also woefully inadequate.
On the average 88 doctors are trained annually from KBTH
Much more worse is the number of Specialist doctors
inadequate number of midwives, lack of functioning theatres frequent shortages of blood and blood
products as against a high annual delivery rate.

To increase the literacy rate at all the levels of education including informal education.
To reach out to the populace on health issues both in English and the local languages.
The transportation network should be improved.
The National Ambulance Service should be resourced and expanded to reach a large number of communities.
Helicopter services should be established to airlift emergency cases to health facilities.

mobile phone services to compliment the services in the transport sector
Governments to tackle the problems of corruption, show good governance and formulate policies when dealing with multinational coorperations in order to get better deals for their countries
National Health Insurance Scheme to be encouraged. The challenges in the NHIS affecting the finances of
the health providers should be quickly addressed. Health personnel should have continuous heath
education including ethics. This is currently being done - Continuous Professional Development Programs for doctors.

Efforts must be made to decongest the hospitals
Polyclinics should be fully functional

La polyclinic now a hospital. The burden on KBTH has reduced. Delivery from
12,000 to 9,931 babies annually. Many standard Private hospitals are springing up Private organizations are helping government
facilities eg MTN refurbishing KBTH labour ward and thaetres.
Private institutions should train more health personnel
They should be encouraged to grow to effectively supplement the efforts of government

Major causes are Prematurity and asphyxia Supervised delivery should be encouraged Adequate ambu-bags in labour wards and
NICU Availabilty of Maternal and neonatal
ventilators Oxygen cylinders to be at all delivery units Management protocols should be
established.

Maternal mortality is a Human Rights issue and should be recognized as such
Doctors and nurses- Are we doing enough! What about Hospital Administrators! What about Parliamentarians!-do you know
the needs of pregnant women in your constituency?
And our Ministers- are we visiting health institutions including maternity homes!
What about ourselves who are hearing this presentation