
Improvement Associates Ltd. Using Process Mapping to Identify Improvement Opportunities Presented...
39
Improvement Associates Ltd. Using Process Mapping to Identify Using Process Mapping to Identify Improvement Opportunities Improvement Opportunities Presented by: Rosmin Esmail and Tanis Rollefstad
-
Upload
aileen-booker -
Category
Documents
-
view
213 -
download
0
Transcript of Improvement Associates Ltd. Using Process Mapping to Identify Improvement Opportunities Presented...

Improvement Associates Ltd.
Using Process Mapping to Identify Using Process Mapping to Identify Improvement OpportunitiesImprovement Opportunities
Presented by:
Rosmin Esmail and Tanis Rollefstad

June 2007 2Improvement Associates Ltd.
PurposePurpose
• By the end of this session, participants will have:– A better understanding of the tool– Experience in using the tool – Ideas on how to apply process mapping to
clinical processes

June 2007 3Improvement Associates Ltd.
Systems and processesSystems and processes
“Every system is perfectly designed to get the results it gets.
“If we want better outcomes, we must
change something in the system. To do
this, we need to understand our systems.”
Don Berwick

June 2007 4Improvement Associates Ltd.
What is a System?What is a System?
• Collection of parts and processes organised around a purpose
• Health care organisations are – complex - many and varied relationships – adaptive systems - people in the systems can
change in response to new conditions
Source: NHS: www.modern.nhs.uk/improvementguides - Working in Systems Plsek, 2000

June 2007 5Improvement Associates Ltd.
What is a process?What is a process?
• A sequence of repeatable steps that lead to a desired end or output
• All work is a process• Many processes are not designed – they evolve• 40- 60% of activity in a large complex process may
be non – value adding
ProcessInputs Outputs
Source: NHS: Improvement Leaders’ Guide to Process mapping, analysis and redesign

June 2007 6Improvement Associates Ltd.
What is a process map?What is a process map?
• A “picture” of a process, showing the connections and actual sequence of steps

June 2007 7Improvement Associates Ltd.
Source: NHS: www.modern.nhs.uk/improvementguides Managing the Human Dimensions of Change
Feels like an Elephant?Feels like an Elephant?
“The thing that was astounding was the mapping. We all thought we knew how the system worked but none of us had a clue. Many times an hour my mouth was just falling open because I didn’t realize what a mess it was …”
Lead Clinician Cancer Services Collaborative

June 2007 8Improvement Associates Ltd.
Why use process maps?Why use process maps?• Communication and understanding
– make work ‘visible’; common understanding– show how work currently gets done – serves as a training aid for new team members– establish performance measures
• Quality Improvement
– identify risks, inefficiencies and improvement opportunities
– standardize work processes, decrease variation• Process Redesign/Development
– show how you want work to be done e.g. planning
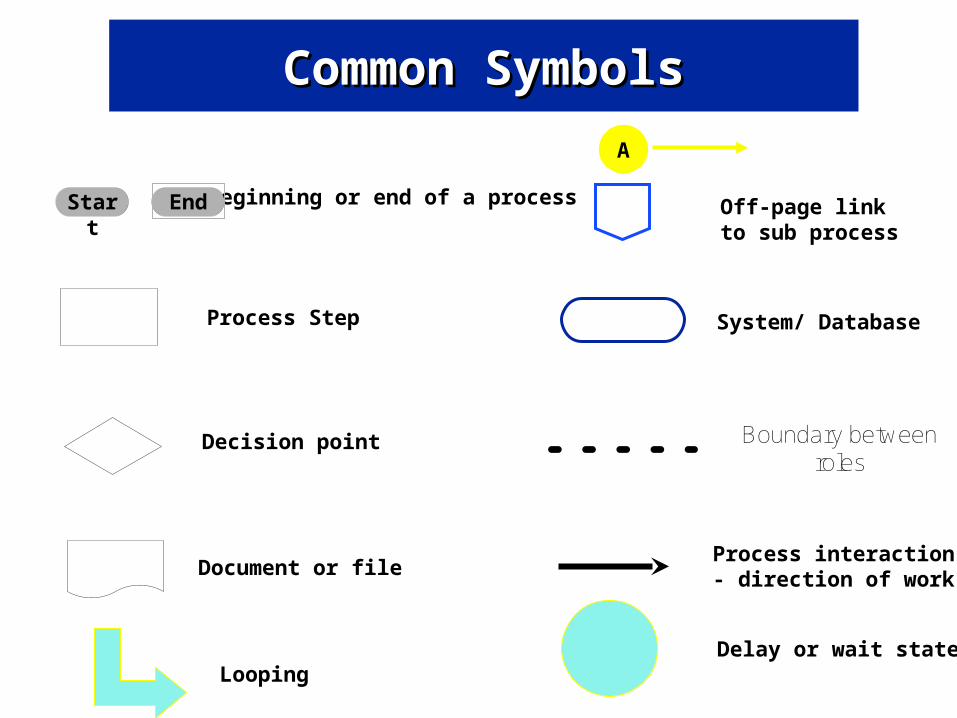
Beginning or end of a process
Process Step
Document or file
Decision point
Process interaction- direction of work
Off-page link to sub process
System/ Database
Start End
Common SymbolsCommon Symbols
Boundary between roles
A
Delay or wait stateLooping

June 2007 10Improvement Associates Ltd.
Exercise (work on your own)Exercise (work on your own)
• Choose a process you are familiar with e.g. getting to work in the morning
• What are the steps?• Start=you get up• End=you are at work• What is the sequence? • Time (10 mins)• Report out

June 2007 11Improvement Associates Ltd.
Types of process mapsTypes of process maps
• Detailed flow chart (micro)
• Cross functional map (deployment)
• Relationship map (macro)
Incr
easi
ng
Det
ail

June 2007 12Improvement Associates Ltd.
Relationship Maps (Macro)Relationship Maps (Macro)
• ‘High level’ organizational view of:– functions – what we do– inputs – e.g. where we get clients from– outputs – e.g. where we send clients, services
provided
• Facilitates understanding of the system and how/where one department fits with another

June 2007 13Improvement Associates Ltd.
Day Surgery Relationship MapDay Surgery Relationship Map
Admitting
Day surgery
Operating Room
Recovery Room
Client in the Community
Surgeon’s Office
FP Office

June 2007 14Improvement Associates Ltd.
Cross-functional mapsCross-functional maps
Illustrate: • How work gets done in an organization
across departments • Departments, functions, or roles that
perform each step- people: process interface
• Inefficiencies e.g. hand-offs

Cross Functional Process MapCross Functional Process Map
Portable / Mobile X-Ray Process
DI G
ener
al
Dut
y T
echn
olog
ist
PC
U C
lerk
PC
U N
urse
Phy
sici
an
No
Yes
Place order
receipt in bin
Page DI for
portable exam
Enter order in order entry
system
Portable Order?
Start
Check in with
pt’s nurse
2
Pick up mobile X-ray equip.
Complete exam
Pick up order
receipt from bin
Phone PCU for
more info
Assist with
exam
Phone PCU to alert of arrival
Change in Patient Condition or Routine Assessment
Assess patient condition, X-ray
required
Use STAT
standard page if STAT
request
If not right after original page

June 2007 16Improvement Associates Ltd.
Creating a Cross Functional MapCreating a Cross Functional Map
• Identify start/end points• Draw table on flip chart• Label columns with all departments/roles
involved in process• List process steps on ‘Post-it Notes™’• Place Post-it’s in order in first row of table • For each process step, place check mark in
column of person/department responsible

June 2007 17Improvement Associates Ltd.
StartStart – client enters service
Assess client
New Client?
Start new chart or pull chart
Follow-up required? Arrange for f/u
Existing services required?
Provide services
Send Chart to Clerk
Document in chart
Enter into database
EndEnd – File Chart
Send back to program
Client PHN Clerk
X
X
X
X
X
XX
XX
X

June 2007 18Improvement Associates Ltd.
Then……..Then……..
• Draw swim lanes on another piece of flip-chart paper
• Label swim lanes with roles/departments• Place each Post-it Note in the appropriate
swim lane• Draw arrows to indicate process flow

June 2007 19Improvement Associates Ltd.
Sample Cross Functional MapSample Cross Functional Map
start
end
Client entersservice
Enter into database
New client?
Services provided
Start new chart
Pull chart
Existing services required?
Follow-up req’d?
Arrange for f/u
Document in chart
Send chart to clerk
Clerk
Client
PHN/Outreach worker
Pro
gra
m X
Syst
em
Com
munit
y
XYZ databaseSystem
no
no
no
yes
yes
yes
Assess client
Send back to program
File chart
June 2007 20Improvement Associates Ltd.
Flow ChartFlow Chart
• Document sequence of events e.g. investigating sentinel event
• Most detailed map – shows process detail
• Useful for process steps of single individual

Flowchart of Process of Obtaining Antibiotics Flowchart of Process of Obtaining Antibiotics from Pharmacy at FMC- May 28 2004from Pharmacy at FMC- May 28 2004
Flow Chart of Process for Obtaining Antibiotics from Pharmacy at FMC-May 28, 2004
Order Acyclovir (Antibiotic)on TDS in the ICU
START
Order is printed inpharmacy and oncomputer in ICU
immediately
Order printed onprinter in ICU and
pharmacy.Pharmacy
technician checksprinter every 2 to
10 minutes
NO
YES
Pharmacist sticksa red flag for STATon order and puts
in grey box atentering pharmacytechnician’s desk
Entering pharmacytechnician entersorder in pharmacy
system BDM
Fillingpharmacy
technician picks upthe order if it’s
STATDELAY in picking
up order
DELAY in pickingup order bypharmacytechnician
*Order statesdrug, dose, howto administer, itis a STAT, any
allergies*STAT is
highlighted onthe bottom of
page
Need to phonedoctor?
Pharmacist triesto find entering
pharmacytechnician to do
this right away forSTAT
Need to makedrug?
NO
Pharmacistchecks drug and
signs order.Order filed in
pharmacy
STAT red flagremoved and
pharmacyassistant takes
drug to ICU rightaway
Filling pharmacytechnician bringsdrug to front tableand signs order
*The hospital isdivided up into 2
sides (ICU isside #2).
Pharmacist checksthe order on TDSto make sure it isright i.e profile,check allergies,
not interacting withanything, look up
microbiology ifresistant
Pharmacist signsthe order
Pharmacist callsthe doctor and
clarifies-this cantake up to 20
minutes to 1 hourDELAY
Order is taken topharmacist to
review and checkPharmacist may
not be thereDELAY
DELAY if enteringpharmacy
technician notthere
*Patient islooked up,
patient bed, ID#,doctors name,drug selected,
dose, labels areprinted.
Enteringpharmacy
technician signsorder and puts it
on the desk
Filling pharmacytechnician checks
cupboard forAcyclovir
*Pharmacy assistantis paged bypharmacy
technician. Arriveswithin 15 minutes
END
Mixing pharmacytechnician writes
up order at table atback
Mixing pharmacytechnician entersinformation in thecomputer in Wordfor labels, order
filled in
Mixing Pharmacytechnician makes
drugs in hood
Mixing pharmacytechnician making
2 to 3 drugsDELAY
Mixing pharmacytechnician takes to
filling pharmacytechnician at front
table
Filling pharmacytechnician labelsdrug and signs
order
Filling pharmacytechnician picks up
the labels
*Wash up = 10mins
*Clean hood=10mins
*Takes 5 to 10minutes to make
drug
Mixing pharmacytechnician checksorder, order filed
YES
Notes:1. Process for a STAT drug if it does not need to be made= ½ hour.2. Process for a STAT drug if it does needs to be made=1 to 1½ hour.3. Process for ASAP drug-deliveries made on the ½ hour every hour exceptmornings (730, 8, 830, 9, 930).3. Night cupboard-code phoned in, porter gets print out, porter gets drug fromcupboard (approximately 12 to 14 orders on average a night), and delivers drugto unit. Pharmacist on call (called in once per week).4. Days-five pharmacists until 11am, 4 pharmacists until 330, 3 pharmacistsuntil 1030pm. Weekends-5 pharmacists until 11am, 4 pharmacists until 330, 2pharmacists unitl 1030pm.5. Six pharmacy techs during day (2 entering, 2 filling and 2 mixing techs, 6pharmacy assistants). All can be different for each drug order. Number of techsvaries at night and on weekends.6. Most antibiotics in fridge or desk A, B in ICU.7. Dispensary extremely noisy, chaotic, lots of people, inadequate room to fill,store, too many distractions, located in basement.
Pharmacyassistant puts
STAT drug in bluebox at desk A and
tells unit clerk
DELAY in unitclerk telling
nurse or take tobedside and no
nurse there
Nurse administers drug topatient
*Labels for IVand pills areprinted onseparateprinters.

June 2007 22Improvement Associates Ltd.
How to start mapping…How to start mapping…
• Determine intended use of process map– e.g. measurement, quality improvement, process
re-design
• Decide how to collect information– e.g. self generate,1 on 1 interviews, team
interview
• Select an appropriate team • Decide the level of map • Identify boundaries – start & end points
June 2007 23Improvement Associates Ltd.
StepsSteps
• Agree to start & end points, customers, and measures
• Agree to appropriate levels of detail.• Brainstorm process participants (if using
cross-functional flowchart)• Brainstorm all possible activities, inputs,
outputs and decisions using appropriate symbols
• Sequence the steps

June 2007 24Improvement Associates Ltd.
StepsSteps
• Use “swim lanes” to distinguish departments (if using a cross-functional flowchart)
• Add arrows and symbols• Test for completeness by
– comparing it with what is actually happening– asking content experts
• Finalize the chart

June 2007 25Improvement Associates Ltd.
Using Process Maps Using Process Maps
• Bottlenecks• Delay• Errors and work-arounds• Rework loops – to fix errors• Role ambiguity - don’t know who…• Cycle time – too long, variation• Duplication - of data entry, work steps• Unnecessary steps – non-value added for staff or client• Inappropriate decision steps – too many steps or too many
people making similar decisions
Smith, M.L. BOLO (Be On Look Out) List for Analyzing Process Mapping. No date www.isixsigma.com/library/content/c040301a.asp
Remember our Quality definition:right service for the right patient at the right time by theright provider with a minimum of waste and rework

June 2007 26Improvement Associates Ltd.
Analysis of Flowchart / Process Analysis of Flowchart / Process RedesignRedesign
• Can it be standardized?
• Does every step or activity add value?
• Is there duplication of work?
• Are there invalid assumptions?
• Is it possible to simplify?

June 2007 27Source: The Improvement Guide. Langley et al. 1996
Example of improvement – blood donationDonor arrives
Donor is interviewed and fills out
form
Donor’s veins are checked in waiting room
Doctorevaluation
occurs
Donor goes to donor room
Veins OK ?
Yes
No
RejectedHealthOK ?
Rejected
Yes
No
Phlebotomist checks veins
Veins OK ?
Rejected
No
Yes
Plasma drawn
Redesigned
Donor arrives
Donor is interviewed and fills out
form
Doctorevaluation occurs and phlebotomist
checks veins
Donor goes to donor room
Plasma drawn
Healthand veins
OK ?No
Yes
Rejected

June 2007 28Source: The Improvement Guide. Langley et al. 1996
Example of improvement – blood donationDonor arrives
Donor is interviewed and fills out
form
Donor’s veins are checked in waiting room
Doctorevaluation
occurs
Donor goes to donor room
Veins OK ?
Yes
No
RejectedHealthOK ?
Rejected
Yes
No
Phlebotomist checks veins
Veins OK ?
Rejected
No
Yes
Plasma drawn
Redesigned
Donor arrives
Donor is interviewed and fills out
form
Doctorevaluation occurs and phlebotomist
checks veins
Donor goes to donor room
Plasma drawn
Healthand veins
OK ?No
Yes
Rejected

June 2007 29
Example of improvement – ovarian cancer clinic
Source: NHS: Improvement Leaders’ Guide to Process mapping, analysis and redesign
Clinic Clinic ClinicHospital for ultrasound
Hospital for blood test
Hospital to see physician
Hospital for chest x ray
Simplication
Hospital for blood test, ultrasound, chest x - ray
ClinicHospital to see
physician

June 2007 30
Example of improvement – ovarian cancer clinic
Source: NHS: Improvement Leaders’ Guide to Process mapping, analysis and redesign
Clinic Clinic ClinicHospital for ultrasound
Hospital for blood test
Hospital to see physician
Hospital for chest x ray
Simplification
Hospital for blood test, ultrasound, chest x - ray
ClinicHospital to see
physician

June 2007 31Improvement Associates Ltd.
TipsTips• Use a group knowledgeable about the process and interested in
improvement
• Use a facilitator
• Don’t focus on solutions - keep a ‘parking lot’ for issues, solutions
• Adopt ‘rough draft’ principle – get it down, then get it good
• To clarify steps: go to the program and observe the process, consult with clients/staff

June 2007 32Improvement Associates Ltd.
TipsTips• Use post-it notes for ease of mobility
• Keep the flowchart simple using basic symbols
• Be consistent with levels of detail
• Ensure flowchart represents process as it really is, not how it ought to be
• Use “verb noun” structure for activities
June 2007 33Improvement Associates Ltd.
Software Software
• Low Tech Stickies
• Visio

June 2007 34Improvement Associates Ltd.
Some Examples Some Examples
June 2007 35Improvement Associates Ltd.
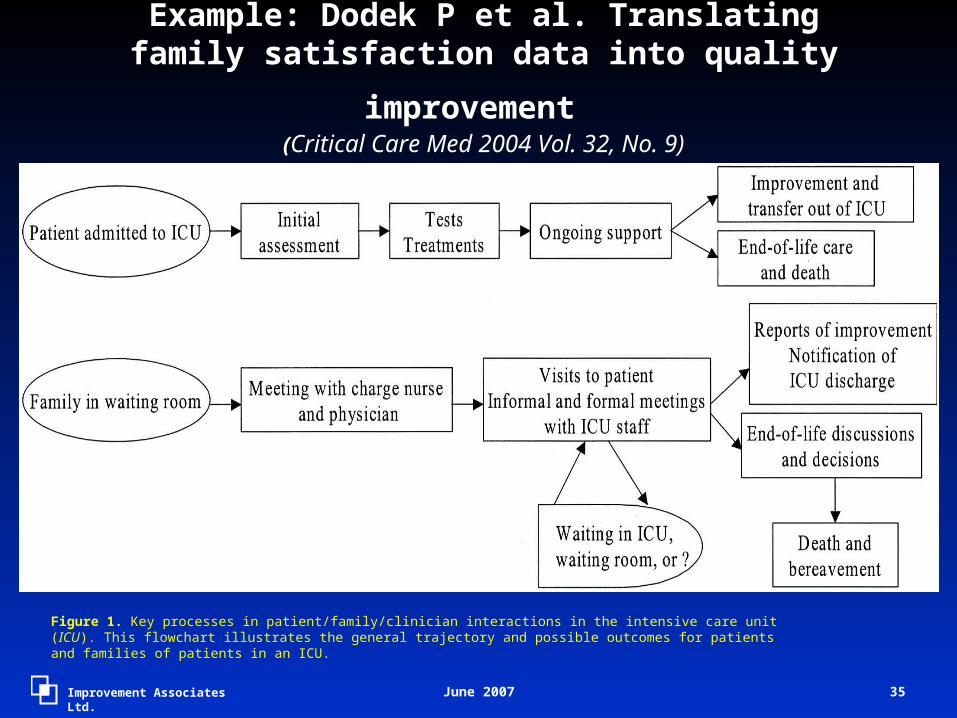
Example: Dodek P et al. Translating family
satisfaction data into quality improvement ((Critical Care Med 2004 Vol. 32, No. 9)
Figure 1. Key processes in patient/family/clinician interactions in the intensive care unit (ICU). This flowchart illustrates the general trajectory and possible outcomes for patients and families of patients in an ICU.
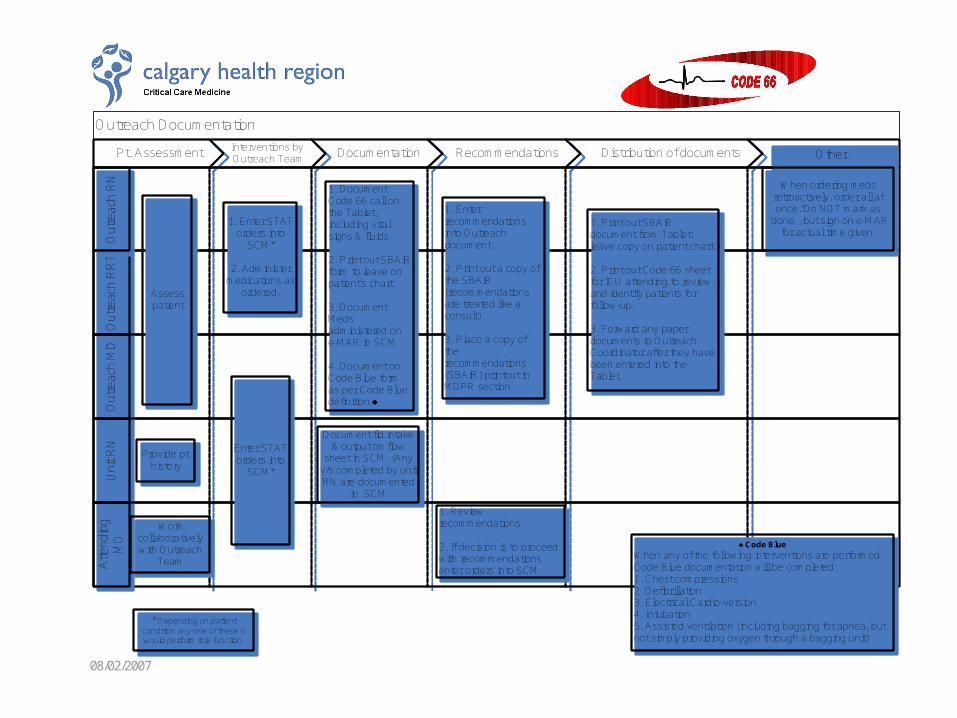
Outreach Documentation
Pt. Assessment Interventions by Outreach Team Documentation Recommendations Distribution of documents
Out
reac
h R
RT
Out
reac
h R
RT
Out
reac
h M
DO
utre
ach
MD
Uni
t RN
Uni
t RN
Atte
ndin
g M
D
Atte
ndin
g M
DO
utre
ach
RN
Out
reac
h R
N
Assess patient
Provide pt. history
Work collaboratively with Outreach
Team
1. Enter STAT orders into
SCM*
2. Administer medications as
ordered.
Enter STAT orders into
SCM*
1. Document Code 66 call on the Tablet, including vital signs & fluids
2. Print out SBAiR form to leave on patient’s chart.
3. Document Meds administered on e-MAR in SCM
4. Document on Code Blue form as per Code Blue definition ♦
1. Enter recommendations into Outreach document.
2. Print out a copy of the SBAiR (recommendations are treated like a consult).
3. Place a copy of the recommendations (SBAiR) printout in MDPR section
1. Review recommendations
2. If decision is to proceed with recommendations enter orders into SCM
Document fld intake & output on flow
sheet in SCM. (Any v/s completed by unit RN are documented
in SCM
1. Print out SBAiR document from Tablet: leave copy on patient chart.
2. Print out Code 66 sheet for ICU attending to review, and identify patients for follow-up.
3. Forward any paper documents to Outreach Coordinator after they have been entered into the Tablet.
Other
When ordering meds retroactively, order all at once. Do NOT mark as
“done”, but sign on e-MAR for actual time given.
* Depending on patient condition any one of these 5 would perform this function.
♦ Code Blue
When any of the following interventions are performed Code Blue documentation will be completed:1. Chest compressions2. Defibrillation3. Electrical Cardio-version4. Intubation5. Assisted ventilation (including bagging for apnea, but not simply providing oxygen through a bagging unit)
08/02/2007

© 2007, BC Children’s Hospital, C&W
Wound Care (DRAFT)Physician Registered Nurse Wound Care Clinician Allied Health (OT, PT, RT)
Wound identified Wound identified
Complete wound assessment and initiate Wound
Care Flowsheet
Does the wound appear
infected?
Notify physicianutilizing SBAR
framework
Assess wound
Swab wound for C&S
yes
no
Order appropriate antibiotics
Do I have the competencies to
determine appropriate wound care?
yes
Consult wound care clinician using SBAR framework
no
Assist with identifying appropriate
dressing choices and in
individualizing patient care plan
Wound pressure related?
Develop care plan and
reassess as indicated
yes
Wound pressure related?
No
Consult OT/PT/RT
Yes
Has wound resolved?
Discontinue wound care
yes
No
Complete wound assessment
Yes
Apply appropriate dressing and initiate
individualized careplan
Reassess wound. Contact Physician and wound care
clinician
No
Consult RN
Culture positive?
Advanced wound management required?
Yes No
Implement VAC
dressing protocol
Consult others as needed
Follow-up as appropriate
No

Improvement Associates Ltd.
““How can you possibly improve How can you possibly improve something unless you know how it something unless you know how it
works”works”

June 2007 39Improvement Associates Ltd.
Application (working in teams)Application (working in teams)
• Identify a clinical process affected by the changes you are trying to introduce
• What is the starting point? End point? • What are key activities (verb, noun)?• What is the sequence? • Create a flow chart of the process
– Use a post-it note for each step– Find a large space on which to work– Leave symbols off until your steps are complete
• Time: 20 mins• Report out-what worked well, what were challenges?


















