
Implementing a Remote Emergency Blood Supply
53
Implementing a Remote Emergency Blood Supply Kate Chipperfield MD FRCPC Vancouver Coastal Health University of British Columbia 3 November 2010 The 2010 Olympic Experience
Transcript of Implementing a Remote Emergency Blood Supply

Implementing a Remote Emergency Blood Supply
Kate Chipperfield MD FRCPCVancouver Coastal HealthUniversity of British Columbia
3 November 2010
The 2010 Olympic Experience

AndPlanning for Blood Contingencies; Ethical considerations
Learning Objectives
1. Describe unique circumstances of Whistler’s Olympic venues dictating supply needs
2. Review the planning process and the role of the Transfusion Medicine Service (TMS), including challenges and lessons learned
3. Discuss an approach to blood contingency planning
4. Describe importance of clinical priorities and an ethical framework in blood contingency

The Bigger Blood picture
• Concurrent NAC and BC Blood Contingency plan development
• Canadian Blood Services: Efforts to ensure adequate supply and delivery– Transportation– Donor participation– Potential Human Resources impacts minimized– Weather – Pandemic Influenza– Vendors, Network, Security
• Precedence: Contacts through CBS to past games hosts

Many Venues
• Pacific Coliseum / Hastings Park• Vancouver Olympic/Paralympic Centre (Hillcrest)• Canada Hockey Place (GM Place)• UBC Thunderbird Arena• Cypress Mountain• Richmond Oval
• Whistler Creekside• Whistler Sliding Centre• Whistler Olympic Park

• Pacific Coliseum / Hastings Park• Vancouver Olympic/Paralympic Centre (Hillcrest)• Canada Hockey Place (GM Place)• UBC Thunderbird Arena• Cypress Mountain• Richmond Oval
• Whistler Creekside• Whistler Sliding Centre• Whistler Olympic Park
VGH
Olympic and Paralympic Family Hospital
SPH
Designated Facility for Spectators /Public
PolyClinic / MMU*-Olympic and Paralympic Family
WHCC - Spectators
Vancouver Polyclinic

Unique to 2010: Whistler & MMU
• Whistler Site
• The Athlete's Village Polyclinic and Mobile Medical Unit (MMU)
• MMU:– Life Limb Threatened Organ from Whistler Venue (Alpine, Sliding Centre)
– Emergency Surgery in the event of transportation blockage– Mass casualty situation





PC/MMU Team Members
• 5 Teams (deployed for range of 9‐14 days)
• General Trauma Surgeon(s)
• Orthopedic Trauma Surgeon(s)
• Trauma Anesthesiologist(s)
• Emergency Physician(s)
• Emergency/Critical Care/ OR RNs
• Respiratory Therapist(s)
• Lab tech (not TMS)
Recruited from
VCH but also from across Canada

MMU: List of Potential Procedures
• Neuro ‐ Burr Holes
• Thoracic ‐Tracheotomy/Tracheostomy
• CardioThoracic ‐ Thoracotomy
• General –Trauma Laparotomy
• Ortho – ORIF
• Vascular –Repairs and Shunts
• They want BLOOD

• O neg RBC only stocked at MMU (plus crystalloid, colloid)
• WHCC – expanded O neg inventory• Training ( on line) and procedures for inventory/equipment management, issue, administration, packing/transport, restocking and TR follow up
• October 2009 ‐ Training day
Plan A –WHCC and MMU

Plan B – MMU Stock•10 units - O neg packed red blood cells (RBC)
•Monitored blood fridge
•20 units – Frozen AB plasma (FP)•Monitored plasma freezer
•Plasma thawing bath
•6 (500 IU) vials - Octaplex (PCC)•2 (2.4mg) vials – Niastase (recombinant fVIIa)
WHCC – resource and re-stocking site for MMU 18 units O neg at WHCC, no plasma. Restock from Vancouver will
take time.No platelets, cryo, or other factors or derivatives in Whistler area


Hardware and Facility Challenges

Hardware and Facility Challenges
• Equipment– Borrowed fridge
– New plasma freezer; but no circular recording chart (!)
• Space– Workflow
– Access, and monitoring of audible alarms
• Power
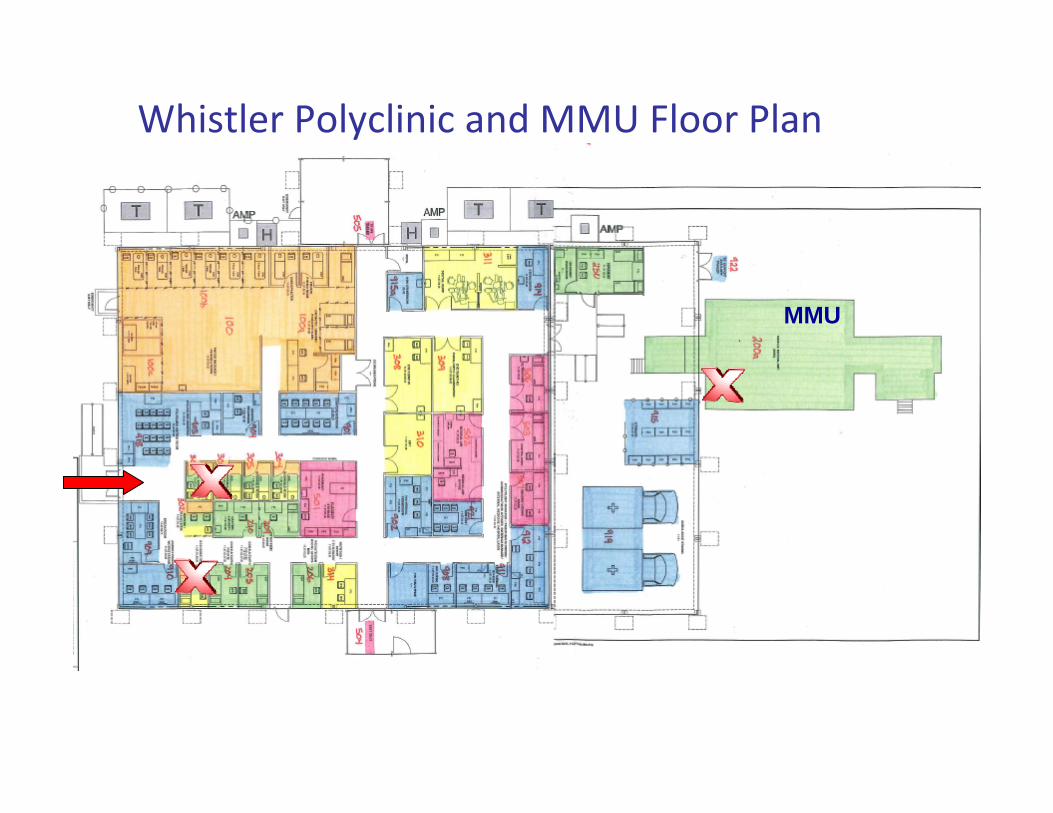
MMU
Whistler Polyclinic and MMU Floor Plan

Training Challenges

Other Challenges
• Security• Accreditation • WHCC Technologist’s experience• Staffing – audible alarms!
– Plasma freezer: q4h documentation– RBC fridge 2400 to 0700h: q1 hourly check
• External laboratory contracted to PolyClinic– No perceived need for INR when lab menu set early in 2009– Disconnect from TMS– Octaplex: need for INR

CTAS‐1 Injury
• Single athlete
• Severe upper body trauma
• CPR at scene
• Further attempted resuscitation at MMU
• 5 units RBC
• 2 units AB plasma thawed

Lessons Learned
• Supply underpins all plans – CBS– Squeaky wheel phenomenon
• DETAILS– Facility, electrical, equipment– Written procedures– Understanding of roles and responsibilities– Brief and Achievable Training with Tracking/Doc’n
• Web‐based less effective than hands‐on
– Clinical and Laboratory Champions
• Gail MacDonald and WHCC Lab staff
• Heather Mah
• Shelley Feenstra
• Dr Ross Brown
• Leanne Appleton
• Canadian Blood Services – Haleh Bahrami
• Shannon Selin, PBCO and BC EBMC
Acknowledgements

What is a contingency?
• An event – often an emergency – that may, but is not certain to, occur.
• blood contingency = an event that results in a blood shortage.
• We work to avoid contingency every day – Best transfusion practice– Conservation strategies

Blood Contingencies
Reduced supply Surge Demand
• National or Prov shortage – CBS issues
• Natural disaster
• Man-made hazards
• Pandemic
• Inventory stockpiling
• Weather Isolation or Local storage failure (remote site)
• Multiple casualties, Natural or Man-made disasters
• Massive transfusion of single patient
• Seasonal increase in traumas

Key stakeholders – BC example
• National, provincial/territorial, health authority, facility specific
• BC Contingency planning working group: PBCO, MoH, CBS medical and operations, HA TM medical and technical, Nursing
• Your facility:– Blood Supplier– TMS – MD, Tech, RN, Operations– Disaster planners/ EOC command– Clinical representation, BTC!– ? Ethicist

Key Data
• What information do you need to know to handle a shortage?

Key data
• Information specific to the shortage – impact, how long, which products or groups, length of recovery phase
• Personnel impacts• Facility impacts; electrical, communications etc• Your inventory: current levels, daily issues (mean and variation), RSL from supplier, delivery interval
• Inventory of Supplier and Others in your geographic area
• Urgency of demand in your facility




Phases are linked to: 1. Product Guidelines 2. Clinical Urgency
Green, Amber and Red Phases
• Green phase actions reflect adherence to published product guidelines
• Increased scrutiny in Amber
• Further patient prioritization in Red

Phases by Product and Day’s on hand

Prioritizing Orders and Needs
• A fundamental switch in physician thinking; your patient may no longer be the most important consideration
• Now that we are in Amber or Red phase; How do we prioritize the product orders as they come in?

Blood Access Priority 1‐2‐3
Resuscitation of life‐threatening hemorrhage
Surgery and Obs:
Semi urgent surgery, symptomatic but not life threatening post op or post partum anemia
Surgical: Elective surgery likely to require 2 U
Support of Emergent or urgent surgery
Other non‐urgent medical indications for transfusion
Non‐surgical: Life threatening anemia, where delay cannot be tolerated
Symptomatic but not life‐threatening anemia that cannot be managed by non‐Tx means



Ethical Considerations:

Ethical Considerations:
Four Principles of Bioethics:
• Autonomy• Benificence• Non‐malificence• Justice
Substantive Values:• Equity• Solidarity• Trust • StewardshipProcedural Values:o Reasonableo Transparento Inclusiveo Responsiveo Accountable
Blood Allocation in Shortage
• that point where the good of the individual must be weighed against the good of the community (the one versus the many)
• Apparent Cross‐purposes of autonomy/beneficence/non‐malificence and Justice
• Stopping Principles: at the extreme end of the spectrum of allocation decisions. When do you withdraw product support from an individual patient?

Applying the thick veil of Ignorance
• John Rawls, John Harsanyi, Donald Dworkin
• An important construct in philosophical theory; a tool to achieve impartiality
• Rational Parties are deprived of all knowledge of their personal characteristics and social and historical circumstances = the original position
• Given choices, most will choose two principles of justice 1. equal basic rights and liberties, 2. fair equality of education and employment opportunities (and therefore a guaranteed minimum of the all‐purpose means)

....a MultiPrinciple Allocation system*
• A suggested ethical construct within which decisions are made regarding scarce resource allocation in extreme situations
• Extrapolated from example of Influenza Epidemic/Allocation of Ventilators
• Keep all patients eligible who would receive treatment in normal circumstances: – Violate laws of ethical justice if we exclude patient groups from eligibility
– despite clinical distinctions, various groups are similar in ethically relevant ways
• Do not rely solely on: sickest first, first come/first serve. Do not consider Broad Social Value *
White et al Annals Int Med 2009: 150: 132-138




Ventilators ≠ Blood
• Many more clinicians “triaging”; role of TM director/medical designate as coordinator
• No SOFA score for transfusion• ? Duty to the “next patient through the door”– Comparing patient to patient versus comparing patient to theoretical next patient
• What is the point of no return, or the stopping point in massive transfusion in scenario of limited blood resources?

Stopping Principles…..Important Considerations
• Pre‐defined situations, guidelines, roles• Multidisciplinary decision: MD caring for patient, TM/Lab
MD, others• Inclusive and Transparent – open discussion between
clinical, lab, patient representatives• Reasonable – diminishing hopes for single patient, critical
inventory issues, timeline for re‐stocking• Responsive – revisiting decision with change in patient
status/ short and longterm prognosis, and change in product inventory
• Accountable• Document: Who requested, Patient, Reason, Counts (Hb, Plt,
INR), ?Released, Inventory at time of discussion.

Multi‐principle allocation strategies…
• Not a operational plan,
• But a starting point for framework
• Any guidelines should be prepared in advance, vetted by BTC, MD executive, risk management or legal counsel, input of ethicist if at all possible
• Give strong consideration to public review & incorporation of public feedback
• Pending NAC subcommittee recommendations!

Summary
• Successful handling of blood contingency requires planning and testing of plan
• There are many potential causes of blood contingency
• Important tenets of a hospital TMS blood contingency plan: knowledge of your inventory/ average use, close communication with clinicians, and pre‐set ethical and clinical guidelines within which allocation decisions are made.


References
1. Callum et al. Bloody Easy 2 Blood Transfusions, Blood Alternatives, and Transfusion Reactions: A guide to transfusion medicine, 2nd ed. 2005
2. Physician’s Guide 2004 (physicians guide for blood and blood product utilization) BC PBCO
3. Kleinman et al. Toward an understanding of Transfusion Related Acute Lung Injury; statement of a consensus panel. Transfusion 2004; 44: 1777-1789.
4. Mintz et al, ed. Transfusion Therapy; Clinical principles and Practice. AABB press, 2nd ed, 2005.
5. Y. Lin and L. Foltz for TMAG. Guidelines for Platelet Transfusion BC PBCO Nov 2004.
6. BC Transfusion Medicine Advisory Group. Guidelines for Red Blood cell transfusion. BC PBCO Nov 2003.

References
7. National Plan for the Management of Shortages of Labile Blood components. National advisory ctte on blood and blood products and CBS. 2009-09-28.
8. British Columbia blood Contingency Plan. BC Transfusion Medicine Advisory group and PBCO. 2010 2 11 v 3
9. White et al. Who should receive Life Support During a Public Health Emergency? Using Ethical Principles to Improve Allocation Decisions. Ann Int Med. 2009;150: 132-138.


















