Implementation of Treatment Protocols in the Diabetes Control and
16
N A L A R T I C L E Implementation of Treatment Protocols in the Diabetes Control and Complications Trial DIABETES CONTROL AND COMPLICATIONS TRIAL RESEARCH GROUP OBJECTIVE — To describe the methods used to implement intensive and conven- tional therapies in the Diabetes Control and Complications Trial (DCCT) and the metabolic results that occurred with the different treatment regimens. RESEARCH DESIGN AND METHODS— The DCCT was a controlled clin- ical trial that demonstrated the beneficial effect of intensive therapy on the long-term complications of insulin-dependent diabetes mellitus (IDDM). A total of 1,441 volun- teers with IDDM, aged 13-39, from 29 centers in the U.S. and Canada, were randomly assigned to conventional or intensive diabetes therapy. Intensive therapy, which used multiple daily injections (MDI) of insulin (>3 injections/day) or continuous subcuta- neous insulin infusion (CSI1), was implemented by a team that included diabetes nurses, dietitians, behavioral experts, and diabetologists. Volunteers in the intensive treatment group could use MDI or CSII, based on patient and clinic preference, and could switch between therapies over the course of the study. The volunteers were followed for a mean of 6.5 years (range 3-9 years). RESULTS — A detailed analysis of implementation of the two treatments indicates that intensive and conventional treatment subjects adhered to their respective insulin injection regimens >97% of the time. Adherence to other elements of intensive treat- ment was similarly high and resulted in median HbA lc values between 6.7 and 7.2, compared with 8.7-9.2 with conventional therapy, over the course of the study. Severe hypoglycemia occurred three times more often in intensively treated subjects. Al- though subjects on intensive treatment were not randomly assigned to MDI or CSII, we compared those subjects who used either of these methods for >90% of the study time. CSII-treated patients maintained a mean HbA lc of 6.8 vs. 7.0 in MDI-treated subjects during the trial (P < 0.05). The frequency of hypoglycemia with coma and seizure and diabetic ketoacidosis was modestly higher with CSII than with MDI. CONCLUSIONS — Intensive therapy was implemented successfully in the DCCT. The detailed description herein will serve to facilitate translation of the DCCT results to the clinical setting. From the Diabetes Control and Complications Trial (DCCT) Research Group (see APPENDIX). Address correspondence and reprint requests to DCCT Research Group, Box NDIC/DCCT, Bethesda, MD 20893. Received for publication 16 March 1994 and accepted in revised form 6 October 1994. ADA, American Diabetes Association; BMI, body mass index; CSII, continuous subcutaneous insulin infusion; DCCT, Diabetes Control and Complications Trial; DKA, diabetic ketoacidosis; IDDM, insulin-dependent diabetes mellitus; MDI, multiple daily injections. T he Diabetes Control and Complica- tions Trial (DCCT) was designed to examine the effects of intensive management of diabetes on the develop- ment and progression of the microvas- cular and neurological complications of insulin-dependent diabetes mellitus (IDDM) (1,2). Between 1983 and 1989, a total of 1,441 volunteers entered the study. They were randomly assigned to either intensive diabetes treatment or conventional treatment. Intensive ther- apy attempted to achieve glycemic con- trol as close to the nondiabetic range as possible. In contrast, conventional ther- apy attempted to eliminate symptoms of high or low blood glucose and did not have specified blood glucose targets. The DCCT provides a unique database con- sisting of more than 9,000 patient-years of treatment experience in IDDM patients selected for the absence of advanced com- plications at baseline and followed closely under the conditions of a controlled clin- ical trial. The major results of the DCCT were reported recently (2). Based on the uniform, significant delay in onset and re- duction in progression of the microvascu- lar and neurological complications of IDDM, the DCCT Research Group rec- ommended intensive therapy for most patients with IDDM. This report provides a detailed description and analysis of the implementation of the conventional and intensive treatment protocols used in the DCCT. The major components of inten- sive therapy, including insulin adminis- tration, monitoring, and diet, will be pre- sented in detail, and the variations in intensive therapy among clinics and over time will be discussed. RESEARCH DESIGN AND METHODS — The DCCT was a multi- center, randomized, and controlled clini- cal trial (1). The design, eligibility criteria, baseline characteristics, and operating procedures have been published previ- ously (1-7). In brief, the study was de- signed between 1982 and 1983. After the successful completion of a feasibility DIABETES CARE, VOLUME 18, NUMBER 3 , MARCH 1995 361 Downloaded from http://diabetesjournals.org/care/article-pdf/18/3/361/526529/18-3-361.pdf by guest on 14 January 2022
Transcript of Implementation of Treatment Protocols in the Diabetes Control and

N A L A R T I C L E
Implementation ofTreatment Protocols inthe Diabetes Control andComplications TrialDIABETES CONTROL AND COMPLICATIONS TRIAL RESEARCH GROUP
OBJECTIVE — To describe the methods used to implement intensive and conven-tional therapies in the Diabetes Control and Complications Trial (DCCT) and themetabolic results that occurred with the different treatment regimens.
RESEARCH DESIGN AND METHODS— The DCCT was a controlled clin-ical trial that demonstrated the beneficial effect of intensive therapy on the long-termcomplications of insulin-dependent diabetes mellitus (IDDM). A total of 1,441 volun-teers with IDDM, aged 13-39, from 29 centers in the U.S. and Canada, were randomlyassigned to conventional or intensive diabetes therapy. Intensive therapy, which usedmultiple daily injections (MDI) of insulin (>3 injections/day) or continuous subcuta-neous insulin infusion (CSI1), was implemented by a team that included diabetesnurses, dietitians, behavioral experts, and diabetologists. Volunteers in the intensivetreatment group could use MDI or CSII, based on patient and clinic preference, andcould switch between therapies over the course of the study. The volunteers werefollowed for a mean of 6.5 years (range 3-9 years).
RESULTS — A detailed analysis of implementation of the two treatments indicatesthat intensive and conventional treatment subjects adhered to their respective insulininjection regimens >97% of the time. Adherence to other elements of intensive treat-ment was similarly high and resulted in median HbAlc values between 6.7 and 7.2,compared with 8.7-9.2 with conventional therapy, over the course of the study. Severehypoglycemia occurred three times more often in intensively treated subjects. Al-though subjects on intensive treatment were not randomly assigned to MDI or CSII, wecompared those subjects who used either of these methods for >90% of the study time.CSII-treated patients maintained a mean HbAlc of 6.8 vs. 7.0 in MDI-treated subjectsduring the trial (P < 0.05). The frequency of hypoglycemia with coma and seizure anddiabetic ketoacidosis was modestly higher with CSII than with MDI.
CONCLUSIONS — Intensive therapy was implemented successfully in the DCCT.The detailed description herein will serve to facilitate translation of the DCCT results tothe clinical setting.
From the Diabetes Control and Complications Trial (DCCT) Research Group (see APPENDIX).
Address correspondence and reprint requests to DCCT Research Group, Box NDIC/DCCT,Bethesda, MD 20893.
Received for publication 16 March 1994 and accepted in revised form 6 October 1994.ADA, American Diabetes Association; BMI, body mass index; CSII, continuous subcutaneous
insulin infusion; DCCT, Diabetes Control and Complications Trial; DKA, diabetic ketoacidosis;IDDM, insulin-dependent diabetes mellitus; MDI, multiple daily injections.
The Diabetes Control and Complica-tions Trial (DCCT) was designed toexamine the effects of intensive
management of diabetes on the develop-ment and progression of the microvas-cular and neurological complications ofinsulin-dependent diabetes mellitus(IDDM) (1,2). Between 1983 and 1989, atotal of 1,441 volunteers entered thestudy. They were randomly assigned toeither intensive diabetes treatment orconventional treatment. Intensive ther-apy attempted to achieve glycemic con-trol as close to the nondiabetic range aspossible. In contrast, conventional ther-apy attempted to eliminate symptoms ofhigh or low blood glucose and did nothave specified blood glucose targets. TheDCCT provides a unique database con-sisting of more than 9,000 patient-yearsof treatment experience in IDDM patientsselected for the absence of advanced com-plications at baseline and followed closelyunder the conditions of a controlled clin-ical trial. The major results of the DCCTwere reported recently (2). Based on theuniform, significant delay in onset and re-duction in progression of the microvascu-lar and neurological complications ofIDDM, the DCCT Research Group rec-ommended intensive therapy for mostpatients with IDDM. This report providesa detailed description and analysis of theimplementation of the conventional andintensive treatment protocols used in theDCCT. The major components of inten-sive therapy, including insulin adminis-tration, monitoring, and diet, will be pre-sented in detail, and the variations inintensive therapy among clinics and overtime will be discussed.
RESEARCH DESIGN ANDMETHODS — The DCCT was a multi-center, randomized, and controlled clini-cal trial (1). The design, eligibility criteria,baseline characteristics, and operatingprocedures have been published previ-ously (1-7). In brief, the study was de-signed between 1982 and 1983. After thesuccessful completion of a feasibility
DIABETES CARE, VOLUME 18, NUMBER 3 , MARCH 1995 361
Dow
nloaded from http://diabetesjournals.org/care/article-pdf/18/3/361/526529/18-3-361.pdf by guest on 14 January 2022

Implementation ofDCCT treatment regimens
phase (8), the full-scale trial was initiatedin 1985. Twenty-six clinics across theU.S. and three in Canada entered partici-pants into the trial from 1983 to 1989.Volunteers were randomly assigned to re-ceive either intensive or conventionaltherapy. Virtually all diabetes care wasprovided by the DCCT.
Eligibility and exclusion criteriaThe rigorous clinical and biochemical se-lection criteria for patients participatingin the primary prevention and secondaryintervention studies of the DCCT havebeen described in detail in previous pub-lications (1-4,7). The baseline character-istics of the entire cohort are shown inTable 1.
Details of treatment regimensEach participant was assigned to a treat-ment team consisting of nurse, physician,and dietitian; in most centers, regularmeetings with a mental health profes-sional were incorporated into the treat-ment plan. Mental health professionalsincluded social workers, psychologists,and psychiatrists. All care and suppliesrelated to the DCCT were provided free ofcharge.Conventional treatment. Subjects ran-domly assigned to the conventional treat-ment group were provided with conven-tional diabetes education, nutritioncounseling, and advice on insulin admin-istration, such as site rotation. No singleeducational program was used study-wide; rather, each center instructed thesubjects using locally developed pro-grams and methods. Up to two injectionsper day of any mixture of short-acting,intermediate, or long-acting pork, beef/pork, or human insulin was prescribed.Patients were seen in follow-up by thetreatment team every 3 months.
The primary goals for the conven-tional treatment group included the ab-sence of symptoms attributable to hyper-or hypoglycemia, absence of ketonuria,and the maintenance of normal growthand development. No predefined targetsfor glucose control were set, and insulin
doses were not usually adjusted on thebasis of urine or glucose monitoring re-sults. The investigator and patient weremasked to the quarterly HbAlc results un-less values exceeded 13.1% (1). If this oc-curred, therapy was adjusted, and theHbAlc was measured monthly untilHbAlc was again <13.1%. Pregnancy orplans to become pregnant mandated de-viation to intensive treatment. Patients re-sumed conventional treatment after de-livery. Initially, urine testing was theprimary method of self-monitoring forconventional therapy group patients.With the increased use of capillary bloodglucose monitoring in community prac-tice, this technique was made part of theconventional treatment regimen in 1986.Patients were instructed to perform atleast one capillary blood glucose or oneurine test per day. A urine test for ketoneswas required when the blood glucose was>240 mg/dl. More intensive monitoringwas indicated for sick days or days withunusual exercise or to increase safety.Diet management: Registered dietitians ateach center tailored meal plans and edu-cational strategies to the needs and life-style of each individual, based on a nutri-tion assessment and diet history. The diethistory method has been previously re-ported (9). Calories were prescribed toachieve and maintain 90-120% idealbody weight and/or support normalgrowth and development. Diet composi-tion goals were 10-25% protein (no lessthan 0.8 g/kg for adults, 0.84 g/kg forages 15-18, and 1 g/kg for ages 13-14),30-35% fat with a 0.8-1.0 polyunsatu-rated:saturated fat ratio and <600 mgcholesterol, and 45-55% carbohydratewith <25% of carbohydrate from simplesugars. Consumption of concentratedsweets was generally discouraged. Theuse of snacks in the meal plan was basedon patient preference and the insulin reg-imen. Diet education was provided in astepped approach until all participantsunderstood survival level, home manage-ment, and lifestyle skills (10).
In response to the National Cho-lesterol Education Program (11) and the
prudent low-fat dietary recommenda-tions of the American Diabetes Associa-tion (ADA) and the American Heart Asso-ciation, the study protocol was amendedin 1988 so that all participants receivedcounseling on the step I diet of the Na-tional Cholesterol Education Program.Diet composition goals were <30% fat,^10% saturated fat, and <300 mg/daycholesterol. Further counseling and ad-vice on the step II diet and cholesterol-lowering medication, if necessary, wereprovided to those who did not attain tar-get low-density lipoprotein cholesterollevels despite adherence to the step I diet.Exercise: Specific exercise prescriptionswere not required. Exercise was encour-aged according to the individual's interestand physical fitness. Patients were taughtto adjust insulin doses and diet to accom-modate exercise with emphasis placed onavoidance of hypoglycemia.Intensive treatment. Intensive treatmentwas a comprehensive program compris-ing many elements, including flexible ad-justment of insulin dose, frequent moni-toring of glucose levels and diet, andbehavior change. The aim for the inten-sive treatment group was to achieve andmaintain glycemic control as close to thenondiabetic range as possible while min-imizing severe hypoglycemia. Goals forblood glucose levels, measured at leastfour times daily, were the following: fast-ing and preprandial 70-120 mg/dl; post-prandial <180 mg/dl (90-120 min aftermeal); and 3:00 A.M. >65 mg/dl (mea-sured weekly). The goal for HbAlc, mea-sured monthly, was to maintain a levelwithin 2 SD of the mean for a sample ofpeople without diabetes (<6.05). Pa-tients aimed to have no episodes of hypo-glycemia requiring assistance, no epi-sodes associated with altered mentalstatus, even if this could be managed bythe subject without assistance, and lessthan four easily self-treated episodes perweek without significant mental impair-ment.
Initiation of intensive treatment: Pork,mixed beef/pork, and human insulinswere used. Insulin was administered ei-
362 DIABETES CARE, VOLUME 18, NUMBER 3 , MARCH 1995
Dow
nloaded from http://diabetesjournals.org/care/article-pdf/18/3/361/526529/18-3-361.pdf by guest on 14 January 2022

DCCT Research Group
ther with continuous subcutaneous insu-lin infusion (CSII, pump) or with multi-ple (three or more) daily injections(MDI). The initial choice of CSII or MDIrested with the treatment team and vol-unteer. Patients who used MDI had accessto a variety of convenience devices (peninjectors, button infusion) to facilitatetherapy.
Intensive treatment group pa-tients were hospitalized, generally for 2-4days, to teach the elements of MDI or CSIIand to develop individual treatment algo-rithms. A major goal of the hospitaliza-tion was to incorporate the patient intothe team that would be working togetherto achieve intensive treatment goals. Dur-ing their inpatient hospital stay, patientswere trained to use an insulin pump oradminister insulin via MDI, to measureand record blood glucose levels accu-rately, and to use the monitoring data toalter individual treatment regimens. Pa-tients were also taught the impact of in-jection site on insulin absorption. Patientsand family members were given an indi-vidualized diet prescription and instruc-tions on how to treat hypoglycemia, man-age intercurrent illness and ketosis, andcontact the on-call treatment team.Continuing management: Patients wereseen weekly until they were comfortableand confident with the treatment regi-men. Thereafter, they were seen at leastmonthly. Telephone contact was as oftenas daily for the first few weeks, thenweekly thereafter. The purpose of the vis-its and telephone contacts was to reviewglycemic control, reinforce goals andprinciples of intensive management, andadjust the treatment regimen, which in-cluded insulin scales, diet, exercise, andglucose monitoring to achieve the glyce-mic goals. Clinic staff and volunteers pur-sued the glycemic goals vigorously overtime, and, to that end, changed regimensas often as necessary and often used inno-vative treatment strategies.Protection of subjects: If intensification oftreatment resulted in repeated severe hy-poglycemia that could not be preventedby adjusting insulin dose, diet, or exercise
or with patient reeducation, then clinicstaff were required to raise blood glucoseand HbAlc targets to a level consistentwith patient safety. A clinic monitoringgroup reviewed with the staff of the indi-vidual clinics the records of patients withrecurrent, severe hypoglycemia as well asrecords of those with extremely high(>13.1) HbAlc values. Patients in the in-tensive treatment group who were unableto prevent recurrent severe hypoglycemiadespite manipulations within the inten-sive treatment protocol or who were inac-cessible because of distance, illness, orother reasons could be changed to a regi-men of fewer than three daily injectionsand were considered to have deviatedfrom therapy. An independent group ofphysicians and biostatisticians (Data,Safety, and Quality Review Group) alsoreviewed quarterly adverse event reportsto monitor for unacceptable trends overtime.
Glucose monitoring: Patients in the inten-sive treatment group were instructed toperform blood glucose tests a minimumof four times per day, including three pre-prandial and one bedtime sample. Theyalso were instructed to test a 3:00 A.M.sample once a week with a repeated testthe next night if the value was <65 mg/dl.Clinic staff were to be notified promptly ifthe repeat value was <65 mg/dl. Post-prandial samples (90-120 min after themeal) were obtained as necessary to de-tect glucose excursions outside of the tar-get range and adjust preprandial dosesand timing of injections. HbAlc results,measured monthly, were used to assessprogress and motivate subjects to achieveor approach the goal level of <6.05. Inthe event that glycemic goals were notbeing met, more frequent self-monitoringof postprandial glucose levels was re-quired. A variety of commercially avail-able meters were used during the trial,including meters with memory, as theybecame available.
Diet management: In addition to the con-ventional dietary teaching outlinedabove, intensive treatment group partici-pants received more frequent and de-
tailed instruction on the role of diet inattaining normoglycemia. Considerabletime and attention were given to the de-velopment and implementation of indi-vidualized meal plans. Attaining glycemicgoals took precedence over other dietarygoals, such as macronutrient compositiongoals. Therefore, the importance of dietconsistency, especially carbohydrate con-sistency, and meal regularity (15-45 minafter insulin injection) was emphasizedwith all participants. Dietitians used a va-riety of strategies, based on clinic and par-ticipant preference, to teach diet consis-tency. No particular meal planningapproach was mandated, and a variety ofmethods were used, including the ADAexchange system, carbohydrate counting,total available glucose, and healthy foodchoices (13). Once a framework for dietconsistency was established, intensivelytreated patients learned to use foodrecords in conjunction with blood glu-cose records to observe patterns in bloodglucose control. Dietitians then taughtthem a problem-solving approach to ana-lyze blood glucose response to food, ac-tivity, and insulin (14). Follow-up visitswith the dietitian were scheduled as oftenas necessary (usually at least monthly forthe first 6 months) to facilitate problem-solving, help patients regulate insulin de-livery to food intake, and provide sup-port. Over time, most participants wereable to adjust insulin doses for expectedchanges in food intake or activity andcontinued to adjust their regimen as life-style changes occurred.
Weight gain during intensivetherapy has been described elsewhere indetail (15). Although goals for weight were90-120% ideal body weight, weight-lossintervention programs were emphasized inresponse to the following issues: patientconcern about weight; elevations in bloodpressure or low-density lipoprotein; failureto meet treatment goals because of con-cerns about weight; or adverse effects ontreatment adherence due to weight gain.Exercise: As with conventional therapy,no specific exercise prescription was re-quired; rather, exercise was encouraged
DIABETES CARH, VOLUME 18, NUMBER 3, MARCH 1995 363
Dow
nloaded from http://diabetesjournals.org/care/article-pdf/18/3/361/526529/18-3-361.pdf by guest on 14 January 2022

Implementation ofDCCT treatment regimens
according to patient preference. How-ever, intensive treatment subjects weretaught specific adjustments in their MDIand CSII regimens to maintain glycemicgoals and avoid hypoglycemia.
Adherence activitiesA wide range of activities designed tomaintain as high a level of adherence aspossible to the study protocol in generaland to assigned treatment were con-ducted. Such activities included motiva-tional programs, symbolic rewards forachieving treatment goals, and othergroup activities. Adherence activities var-ied from clinic to clinic.
Outcomes—glycemia, overweight,ketoacidosis, severe hypoglycemia,and catheter infectionHbAlc was the principal outcome mea-sure of glycemic control. The other out-comes reported here were defined and as-certained as follows. Weight and heightmeasurements were obtained as part ofthe annual clinical examination. Mea-sures of weight status for this analysiswere based on the body mass index(BMI), which was calculated by dividingeach subject's weight (in kilograms) bythe square of his or her height (in meters).We used the National Center for HealthStatistics definition of overweight. Menwere considered overweight if their BMIwas ^27.8 kg/m2, and women were con-sidered overweight at a BMI of ^27.3 kg/m2. Ketoacidosis was defined as a constel-lation of typical symptoms in thepresence of ketonuria and acidemia thatrequired treatment within a health carefacility. Severe hypoglycemia was definedas episodes in which the patient experi-enced coma, seizure, or suspected seizureor impairment sufficient to require the as-sistance of another person. Either theblood glucose level was measured andfound to be <50 mg/dl or the clinicalmanifestations were reversed by oral car-bohydrate, subcutaneous glucagon, or in-travenous glucose. Catheter infection wasdefined as any infection at the site of aninsulin infusion catheter that required
systemic antibiotic treatment and/or sur-gical incision or drainage.
CSII users are defined as patientsin the study who used an infusion pumpfor at least 18 of the first 20 quarterly vis-its or for 90% of the time among patientsfollowed for at least 4.5 years. MDI usersare defined as those patients who usedMDI 90% of the time. Intensive treatmentpatients who did not fulfill either of thesecriteria are in a category called mixed. Pa-tients in the mixed cohort were character-ized according to periods of use of MDIduring the first 5 years of follow-up(mixed-MDI) and periods of use of CSII(mixed-CSII).
Statistical analysisAll reported P values are two-tailed. Allcomparisons between treatment groupsare based on randomized treatment as-signment. For comparison of the twotreatment groups at baseline, the Wil-coxon rank-sum test was used for ordinaland numerical variables and the correctedX* test of association in contingency ta-bles for categorical variables. Values arepresented as means ± SD unless other-wise indicated. For these comparisons, allresults significant at P < 0.05 are indi-cated.
Event rates are presented as thenumber per 100 patient-years based onthe ratio of the observed number of eventsto the total patient-years of exposure inany calendar year.
Regression models for longitudi-nal data were used to analyze outcomesover time. Analyses were performed usinga model that allowed for correlated re-peated measurements within the samesubjects (17,18). Analyses were per-formed to assess a linear trend over yearsof calendar time and to perform pairwisecomparisons between calendar years.These methods were used to assesschanges in the quantitative measures dur-ing each calendar year, or the logit of theproportion, log(P/l — P), of subjects witha characteristic during each year, and alsousing the log of the rate of events (per 100patient-years) within each calendar year.
For the pairwise comparisons among cal-endar years, the sequential Bonferroniprocedure of Holm (19) was used. Unad-justed P values for pairwise comparisonswere obtained using indicator variablesfor each calendar year in the regressionmodel and then constructing contrasts forthe j3 coefficients for each calendar year.These unadjusted P values were then re-ferred to the critical P value required forsignificance in the pairwise comparisons.To keep the overall error rate at P ^ 0.05,the P value needed to declare a pairwisecomparison significant was very conser-vative (i.e., very low).
Analyses of treatment group dif-ferences over the calendar year werebased on methods that account for un-balanced and incomplete data. The N-weighted test of stochastic ordering wasused to test for treatment group differ-ences in insulin dosage (20).
Follow-up in 1993 was devoted toend-of-study data collection, and the au-thors did not include this final study yearin describing the treatment implementa-tion.
RESULTS— Participants 'baselinecharacteristics have been presented in de-tail (2,3) (Table 1). Diet at baseline wasmodestly different from the ADA guide-lines, with 38% of calories derived fromfat and 45% from carbohydrates. The twotreatment groups had similar diets whenanalyzed by total calories, nutrient com-position, and intake of alcohol, fiber, andcaffeine (Table 2). The volunteers selectedfor the study were of above-average intel-ligence, with a mean IQ of 113; 73% hadsome schooling after secondary schooland half were married (Table 3).
Conventional treatmentProtocol adherence. No more than 1.0%of conventional treatment patients wereconsidered inactive (i.e., not followingthe protocol and not being seen in theclinic for data collection) for any reason inany one year. Overall, subjects assignedto conventional therapy spent 97% of thestudy time using conventional therapy,
364 DIABETES CARE, VOLUME 18, NUMBER 3, MARCH 1995
Dow
nloaded from http://diabetesjournals.org/care/article-pdf/18/3/361/526529/18-3-361.pdf by guest on 14 January 2022

DCCT Research Group
Table 1—Comparison of selected demographic and clinical characteristics of intensive andconventional treatment groups at baseline
nAge (%)
Adolescent (13-17 years)Young adult (18-25 years)Adult (26-39 years)
Women (%)Duration of 1DDM (years)Daily insulin dose (U/kg)
AdolescentsAdults
History of severe hypoglycemia (%)History of DKA in past year (%)Level of cardiovascular activity (%)
StrenuousVigorousModerateSedentary
Overweight (%)MenWomen
Current smokers (%)
Intensive
711
13276049
5.8 ± 4.23
0.95 ± 0.270.63 ± 0.21
4.96
14105818
59
18
Conventional
730
14295646
5.5 ± 4.09
0.96 ± 0.310.62 ± 0.21
5.35
14125619
97
18
Data are means ± SD. There were no statistically significant differences between treatment groups.
i.e., one or two daily insulin injections.Pregnancy or the desire to become preg-nant accounted for >50% of the conven-tional treatment patients' taking three ormore daily insulin injections. No morethan 0.8% were taking three or more dailyinjections for non-protocol-mandatedreasons, such as the desire to switch to amore intensive form of treatment, duringany one year. Between 74 and 80% re-ported following their diet >55% of thetime.Treatment implementation. Table 4 is adescription of conventional therapy asimplemented in the DCCT. During thecourse of the DCCT, -90% (81-91%) ofconventional treatment patients weretreated with two insulin injections perday at a dose that decreased in adults from0.72 U/kg body wt in 1984 to 0.62 U/kgbody wt in 1992 (P = 0.008). If the co-hort of patients who entered the trial in1983-1984 are followed until 1992, thesame decrease in insulin dose is seen. Inadolescents, doses fell from 0.91 U/kg in
1984 to 0.86 U/kg in 1992 (P = 0.0002).During the 1984-1987 period, 10-16%of patients were treated with only onedaily injection, but this number de-
creased steadily so that in the early 1990sonly 5-6% of patients were treated withone daily insulin injection. Approxi-mately 13-18% of the patients indicatedthat they adjusted insulin doses based ontheir blood glucose monitoring between1987 and 1992.
The two treatment changes mostcommonly seen with conventional treat-ment during the trial were more frequentuse of self-monitoring of blood glucoseand use of human insulin. An increasingfraction of patients used blood glucosemonitoring over the course of the trial(41% in 1987 compared with 73% in1992). Urine glucose monitoring de-clined steadily from 59% in 1987 to 27%in 1992. While some of the shift fromurine to blood glucose monitoring overtime was accounted for by a larger frac-tion of patients entering the trial whowere using blood glucose monitoring,much of the shift was secondary to DCCTpatients switching from urine to bloodglucose monitoring. In 1987, the firstyear in which data were reliably collectedregarding species of insulin, only 17% ofpatients were using human insulin. Use ofhuman insulin increased progressively to57% by the end of 1992. This was due, inpart, to recruitment during the mid-
Table 2—Comparison of dietary intake in intensive and conventional treatment groupsat baseline
Intensive Conventional
Median total calories% of calories from
ProteinFat
Saturated fatMonounsaturated fatPolyunsaturated fat
CarbohydrateSimple sugarsAlcohol
Cholesterol (mg)Caffeine (mg)Total dietary fiber (g)
7112,328
18 ± 3.038 ± 6.913 ±3 .114 ± 3.08 ± 2.4
45 ± 7.216 ± 5.3
0.7 ± 1.7403 ± 278.5341 ± 380.6
26 ± 10.9
7302,327
18 ± 2.938 ± 6.713 ± 3.114 ± 3.08 ±2 .4
45 ± 7.216 ± 5.5
0.78 ± 1.7402 ± 220.4372 ± 489.3
26 ± 10.9Data are means ± SD. There were no statistically significant differences between treatment groups.
DlABEThS CARh, VOLUME 1 8 , NUMBER 3 , MARCH 1 9 9 5 365
Dow
nloaded from http://diabetesjournals.org/care/article-pdf/18/3/361/526529/18-3-361.pdf by guest on 14 January 2022

Implementation ofDCCT treatment regimens
Table 3—Comparison of neuropsychological and social characteristics of intensive andconventional treatment groups at baseline
Intensive
Full scale IQEducation (years)Level of education (%)
Graduate schoolCollege graduateSome college or trade schoolSecondary school graduateSome secondary schoolElementary school
Currently married (%)
Conventional
711113.4 ±9 .7
14 ± 2.2
928361313
148
730113.0 ± 10.2
14 ± 2.4
11263613132
50
Data arc means ± SD. IQ was measured with the Weschler Adult Intelligence Scale. There were no statisti-cally significant differences between treatment groups.
11
1O
Si& B
* 7
e
A
-----i i
27B
225
1 2 5
[3
I"7
L414
i_L1
|
1980s of patients already treated with hu-man insulin but was also due to theswitch to human insulin after entry intothe trial as evidenced by the continuedreduction in the number of patients usinganimal insulins after recruitment wascompleted in 1989.
Total median daily caloric intakeamong conventional treatment patientsranged from a low of 1,922 calories in1986 to a high of 2,318 calories in 1990.The percentage of calories derived fromprotein and carbohydrate remained fairlyconstant at 18 and 44-49%, respectively,during the trial. About 15-16% of calo-ries were derived from simple sugars and22-25% from starch during the trial. In1985, 38 and 14% of calories were fromtotal and saturated fats, respectively;these figures declined to 34 and 12% in1992 after step I diet education of all vol-unteers. Cholesterol intake averaged379-396 mg/day in 1985-1987 and thendeclined to 306 and 292 mg/day in 1991and 1992. Dietary fiber remained con-stant at 10-11 g/1,000 calories through-out the trial. Between 1985 and 1992 thepercentage of patients who met the di-etary goals for cholesterol, fat, and satu-rated fat intake increased by 28, 20, and22%, respectively (Fig. 1). Although thelinear trend is significant (P < 0.0002, P< 0.00001, and P < 0.001, respectively),
Intensive p<0.0001 Conventional p<0.001
B
Intensive p<0.04 Conventional p<0.0002
Intensive p<0.004 Conventional p<0.0001
Figure 1—Proportion of patients who achieved
nutrition goals at annual diet history for intensive
( ^ 0 and conventional ( M ) subjects for choles-
terol goal (A; <300 mg/dl), total fat goal (B;
^30% of calories), and saturated fat goal (C;
<10% of calories).
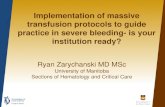
Figure 2—Median HbAlc (A) and median
blood glucose profiles (BGP) (B) obtained at an-
nual visit by calendar year for intensive (*) and
conventional ( • ) treatment subjects. The 25th to
75th percentiles are shown by the bars.
the absolute percentage of patients whoreached dietary goals in 1992 for total fatand saturated fat remained relatively low(24 and 28%, respectively).
Outcomes with conventional therapyGlycemia. Median HbAlc values duringthe feasibility phase (1984-1985) were9.0% in the conventional group and re-mained between 8.9 and 9.0% for allyears except 1986, when a low value of8.7% was recorded, and 1987, when apeak median value of 9.2% was recorded(Fig. 2). A total of 97% of conventionalannual capillary blood glucose profilescontaining five or more samples werecompleted. The mean value for these fiveor more blood samples was calculated foreach patient and used to compare the twotreatment groups. The lowest mean glu-cose values were seen before lunch (197± 7 1 mg/dl) and the highest values afterbreakfast (271 ± 68 mg/dl) in the con-ventional treatment group. The mean ofall blood glucose values calculated fromthe quarterly blood glucose profiles was231 ± 55 mg/dl.
366 DIABETES CARE, VOLUME 18, NUMBER 3, MARCH 1995
Dow
nloaded from http://diabetesjournals.org/care/article-pdf/18/3/361/526529/18-3-361.pdf by guest on 14 January 2022

DCCT Research Group
•£•
ONON
ooON
uuQ
00ON
vO00ON
roO ON in
H VOON in
o o
ON inoo -*•
ON m00 ro
vo00
O <ON Z
r - oo•—i rN
d d+1 +1rN vovq ood doo ini-i rN
d d+1 +1rN vovq oqd doo •*•—i rN
d d+1 +1ro ovo ON
00 I—<-< rN
d d+1 +1rn rovq ON
d dON N ->—i rN
d d+1 +1
o o
o inrN rN
d d+1 +1VO ON
vq 00
d doo vo--I rN
d d+1 +1m oovo oo
o oorN rN
d d+1 +1ON inVO ON
d dON ^H—i ro
d d+1 +1N - ON
d d
in wo
as C w
o 3 g jso C 3 „ "
!§* § -S 3 "o
^ Q< <
m o vo 00in rN -—1
00 o vo 00+ rN 1—1
o in vorN 1—1
ON rN rN in
z z
z z
z z
o
o
^ T 3 CDO O O
•0 rNr-H 00
+ 1 +1i-H OON' CO
^ vor-H f*^
+1 +11—1 1—1
ON' £j
+ 1 +1i—l ON
« ON
+1 +1rN ^H
vq ,_,
^-i 00
+ 1 +1<-< rN
^3
invqr-! 00
+1 +1n inON (N
N . in
+1 +1
ON ON
»rN
«n rNr-H 00
+ 1 +100 ^)-
00 a
9̂ in--H 00
+1 +1ON in
s8^O u 2
8 •§
r ^
in -^.S ,J
"g 2
3$ •*=H re-' s 6^ DO
S3 -S
a s
§-"8(U O
-S x4) DO
3 Co
J g Sre ui D.« c S<-> u OO ' 3 u
Q § 6
^ 6 S+1 ai &;
S J2 - ^
s s sQ u- ex
1984 1S85 1S86 1S87 1988 1989 1990 1991 1992
Year
1984 1985 1986 1987 1988 1989 1990 1991 1S92
Year
Figure 3—Hypoglycemia requiting assistance
by calendar year for intensive treatment group
(A) and conventional treatment group (B). • , to-
tal events; +, events that occurred while the pa-
tient was asleep; and * , events that occurred
while the patient was awake with no warning
symptoms. Events that occurred before 198b were
not characterized by type of symptoms and sleep
status. In 1986, the study entty cntetia were
changed to exclude patients who had experienced
more than two episodes of severe hypoglycemia
within the prior 2 years or more than one event
without warning symptoms.
Hypoglycemia, weight gain, and dia-betic ketoacidosis (DKA). Conventionally treated subjects had 19 episodes ofsevere hypoglycemia per 100 patient-years during the DCCT (Fig. 3). This in-cluded 257 instances of coma or seizure.The absolute rate of events decreased after1986. As previously reported, about two-thirds of severe hypoglycemic events oc-curred while patients were asleep orawake without warning symptoms (21).In the conventional treatment group,11.8% of patients were considered over-weight in 1984, and this increased to17.5% by 1992 (P = 0.00001) (Fig. 4).
DIABETES CARE, VOLUME 18, NUMBER 3 , MARCH 1995 367
Dow
nloaded from http://diabetesjournals.org/care/article-pdf/18/3/361/526529/18-3-361.pdf by guest on 14 January 2022

Implementation ofDCCT treatment regimens
linn I1984 1985 1986 1987 1988 1989 1990 1991 1992
Year
Figure 4—Point prevalence of DCCT patientswho were overweight at annual visit for intensive(^!) and conventional ( • ) therapy subjects bycalendar year. Overweight is defined as BMl>27.8 in men and >27.3 in women. The preva-lence increased significantly over time within eachtreatment group (P < 0.0001).
DKA occurred in between 1 and 5% ofconventionally treated patients per year.The change in the frequency of DKA from1985 and 1986 to the early 1990s (from 4and 5% to <2%) is not significant (P <0.06).
Intensive treatmentProtocol adherence. No more than 2.2%of the intensive treatment patients wereconsidered inactive in any one year. Morethan 97% of patients assigned to intensivetreatment were taking three or more insu-lin injections daily or using a pump. Inthe majority of patients treated with fewerthan three daily injections, a less intensiveform of treatment was mandated forsafety reasons, usually because of recur-rent severe hypoglycemia.Treatment implementation. Table 5 is adescription of intensive therapy as imple-mented in the DCCT. Intensively treatedsubjects could change between CSII andMDI regimens because of difficulty inreaching glycemic goals or because of per-sonal preference. Insulin pump treatmentwas used by 40% of intensively managedpatients in 1984, dropped to a nadir of29% in 1989, and rose yearly to 42% in1992. The increase in CSII use between1989 and 1992 was entirely due to the
greater number of patients switchingfrom MDI to CSII.
The most common MDI regi-mens, used by 56-60% of all MDI pa-tients between 1988 and 1992, includedpremeal regular insulin and one or moreinjections of NPH or lente insulin. Ultra-lente-based regimens with premeal regu-lar insulin were used by 40-44% of pa-tients treated with MDI during the sametime period. Other combinations of regu-lar, NPH-lente, and ultralente regimenswere used during the study based on in-vestigator preference. The division of in-sulin dose between intermediate or long-acting and rapid-acting insulin was highlyvariable across patients.
Total daily insulin dosage de-creased in adults from mean values of0.73 U/kg body wt in 1984 to 0.67 U/kgin 1991 and 1992 (P = 0.01). In adoles-cents over the same time period, dosagedecreased from mean values of 1.24 to0.95 U/kg (P = 0.0008). The doses forintensely treated adults were 0.01-0.05U/kg greater than those for convention-ally treated adults (P = 0.001). The dosesfor intensively treated adolescents were0.09-0.33 U/kg greater than those forconventionally treated adolescents (P =0.007). As in the conventional treatmentgroup, the use of human insulin increasedsubstantially from 18% of the intensivelymanaged patients in 1987 to 62% in1992.
The majority of intensively treatedpatients (86-92%) reported monitoringblood glucose at least three times per dayduring the study. More than 97% of pa-tients reported at least one blood glucosetest per day each calendar year. The low-est rates of adherence to the treatmentprotocol were to the weekly monitoring at3 A.M. Weekly 3 A.M. testing was per-formed by >90% of patients in the first 2years (1984-1985) of the study but byonly 67-70% during the last 2 years(1991-1992). Adjustment of insulindoses based on results from self-monitor-ing of blood glucose was reported by 94-98% of intensively managed patientsthroughout the trial.
Between 77 and 85% of inten-sively treated patients reported followingtheir diet >55% of the time, and <9%reported that they failed to follow theirdiet at least 45% of the time during anyone year of the study. Total daily caloricintake in the intensively managed pa-tients remained fairly constant between1,957 and 2,128 calories throughout thetrial. The percentage of calories from pro-tein (18%), carbohydrate (43-48%), sim-ple sugars (14-16%), and starch (21-25%) also remained constant and similarto that consumed by the conventionaltreatment group. About 38 and 14% ofcalories were from total and saturatedfats, respectively, in 1985. These figuresdeclined to 35 and 12% in 1992. As in theconventional treatment group, choles-terol intake decreased from a high valueof 397 mg/day in 1985 to 272-293 mg/day during the last 3 years of the trial.Dietary fiber remained constant at 10-11g/1,000 calories throughout the trial.From 1985 to 1992, the proportion of pa-tients who met the dietary goals for cho-lesterol, fat, and saturated fat increased(Fig. 1). Although the linear trend is sig-nificant (P < 0.001, P < 0.04, and P <0.004, respectively), the absolute per-centage of patients achieving dietary goalsfor fat and saturated fat intake remainedrelatively low (24 and 28%, respectively,in 1992), similar to the percentage in theconventional treatment group.
Outcomes of intensive diabetestreatmentGlycemia. With intensive treatment, me-dian HbAlc values were lowest during thefeasibility phase (6.7 and 6.8%) and re-mained between 7.0 and 7.1% for theyears 1986-1992, except for 1987, whenthe median was 7.2 (Fig. 2). Although44% of the patients achieved the targetHbAlc (<6.05) at least once, <5% main-tained a mean HbAlc <6.05% through-out the study. A total of 99% of intensiveannual capillary blood glucose profilescontaining five or more samples werecompleted. As with conventional therapy,the lowest mean values were obtained be-
368 DIABETES CARE, VOLUME 18, NUMBER 3 , MARCH 1995
Dow
nloaded from http://diabetesjournals.org/care/article-pdf/18/3/361/526529/18-3-361.pdf by guest on 14 January 2022

DCCT Research Group
ONvO
ON00VO
mO\vO
rM
OrM
invo
rM vo rM ON rM^ j - 1/̂ 1 1*̂ . ^ j - ^ j -
ON 00 vo
n in oo
m vo o ON ooro vo o oo m
O N O ( N C O Or M !•»• h - ^J- • * •
ON ON CO O inrM vo in ro ro
H 00 (N C Nm v o -^ r M r M
o oo in vo o•̂ t- in rM rM
s| 2
o o+1 +1r nvq ON
d d
d d+1 +1vO OvO O
d d+ 1 +1VO ONVO O NO O
d d+1 +100 rMVO O
.—I 00rM rM
d d+1 +1
O - w
B S d 6Z Z
o o+1 +1o ind .-i
o ONrM rM
d d+ 1 +1ON rMvO O
in mrM ro
d d+ 1 +1
5 <-> <-> . s
vo rMm vo
O O ON•^ vO in
O O VO•3- vo in
O O O Nr t - v o T f -
r O N 0 0•*• m m
0 0 r M 0 0•̂ - m rH
VO <VO Z
vo r-- ooco vo ON
t 00 00 O N00 N (J
ON in vo00 r- ON
in vo ON oo m0 0 N O N
VO O ON inON h- ON
^" m r H H \ ( -ON 00 ON
(N IN i nON ON ON
•5b
-3 ft? <£ «
• o '£in
3 'o o 2
H
IIin <uS D-"2 io§ cS g
c
+ l w + l
^ ON ^+ 1 +1
^ ON ^+ 1 +1
+ 1 -H
+1 -H +1
r i C U
a <
o
S c
o g;
i2 £3 re
re o
s reuC re
.2P <u
5 ? ^
n
Ss22 c
o « 5r- <J O
^J <u c
1 1 aD- > i-
s ii %
fore lunch (130 ± 41 mg/dl) and thehighest after breakfast (195 ± 50 mg/dl).The mean blood glucose level calculatedfrom all of the profiles for all of the inten-sively treated subjects was 155 ± 30 mg/dl.Severe hypoglycemia. We have previ-ously reported that between 1983 and1987 severe hypoglycemia occurred ap-proximately three times more often in in-tensively managed DCCT patients, that adisproportionate number of episodes oc-curred during sleep, and that about one-third of episodes occurred while patientswere awake but without warning symp-toms (21). All of these trends continuedthrough 1992 (Fig. 3). The cumulative in-cidence of at least one episode of severehypoglycemia was approximately twice asgreat in the intensively managed patientsduring the study as in the conventionaltreatment group (72.8 vs. 41.3% at studyend). In the intensive treatment group,459 patients had 2,896 events (62 epi-sodes/100 patient-years), while 255 pa-tients had 892 events in the conventionaltreatment group (19 episodes/100 pa-tient-years).
As with conventional therapy, theabsolute frequency of severe hypoglyce-mia decreased over time. Approximately38-41% of intensive treatment patientsand 15% of conventional treatment pa-tients had at least one episode of severehypoglycemia during one of the years1983-1985. Between 1986 and 1992, thefraction of patients experiencing at leastone episode of severe hypoglycemia inany one year declined, ranging from 21.6to 31.8% in the intensive treatment groupand from 6.5 to 12.0%> in the conven-tional treatment group. Event rates weretwo to five times higher in the intensivelymanaged patients during every year of thetrial.
Weight gain and DKA. We have re-ported that during the early years of theDCCT the intensively managed patientsexperienced greater weight gain than thepatients treated conventionally (15), andthis is confirmed by the final data (Fig. 4).In the intensive treatment group, 18.5%
DIABETES CARE, VOLUME 18, NUMBER 3 , MARCH 1995 369
Dow
nloaded from http://diabetesjournals.org/care/article-pdf/18/3/361/526529/18-3-361.pdf by guest on 14 January 2022

Implementation ofDCCT treatment regimens
were considered overweight in 1984, andthis increased to 33.6% by 1992. Theprevalence of overweight conventionaltreatment group patients was 11.8 and17.5% at these two time points. These in-creases over time were statistically signif-icant (P < 0.00001) in each group. DKAoccurred in ~2% of intensively managedpatients in any one year of the trial. Therates of DKA were not different betweentreatment groups.Catheter infections. From 1988 to1992, the annual rate of catheter infec-tion in the 4.5-year cohort of patients(n = 124) consistently receiving CS1Itherapy ranged from 7.3 to 11.3 events/100 years of patient follow-up. There isno evidence of a linear trend, and no yearswere significantly different from eachother.MDI versus CSII. The DCCT study de-sign, which did not randomly assign in-tensive treatment subjects to specificregimens, does not allow definitive com-parison of the relative efficacy and risks ofCSII and MDI. Since patient and clinicpreferences and experiences influencedthe choice of treatment, any comparisonof CSII and MDI will reflect patient,clinic, and treatment team differences, aswell as differences between the treatmentsthemselves. Although the nonrandomstudy design with regard to intensive reg-imens prevents a clear examination of theattributes of CSII versus MDI, a numberof observations can be made.
A total of 555 patients, 78% of theintensive treatment group, were studiedfor at least 4.5 years. The baseline charac-teristics for the three intensive treatmentsubgroups (MDI, CSII, and mixed; seeMETHODS) are shown in Table 6. Therewere only two significant differences inthe baseline characteristics among thethree subgroups. The mixed group had ahigher proportion of women than theother two groups, and the CSII grouptended to have a higher proportion ofmarried individuals than did the othertwo groups.
The HbAlc levels achieved by thepatients with at least 4.5 years of fol-
Table 6—Comparison of selected baseline variables by mode of insulin delivery
nMean eligibility HbAlc (%)Stimulated C-peptide (pmol)
% >0.20 pmolDuration of IDDM (months)Past history of severe hypoglycemia (%)Past history of DKA (%)Overweight (%)Age at baseline (%)
Adolescent (13-18 years)Young adult (18-25 years)Adult (>25 years)
Age (years)Women (%)Attained education (years)Full scale IQMarried at entry (%)Levels of cardiovascular exercise (work
and leisure) (%)StrenuousVigorousModerateSedentary
MDI
2849.07 ± 1.50.10 ±0.11
1776 ± 5 0
647
142660
27.0 ± 7.2946
14 ±2.16113 ± 10
46
18105418
CSII
1249.16 ± 1.650.09 ±0.11
1381 ± 51
666
53065
28.9 ± 6.4144
14 ± 1.74113 ± 9
65t
159
5719
Mixed
1479.07 ± 1.570.10 ± 0.11
1477 ± 54
798
122464
27.3 ± 6.7959*
14 ± 2.12114 ± 9
49
6116518
Data are means ± SD unless otherwise indicated. IQ was measured with the Adult Weschler IntelligenceScale. *P = 0.02, TP = 0.001, compared with other groups.
low-up in these subgroups are shown inFig. 5. The CSII subgroup achieved 0.2-0.4% lower HbAlc levels than the MDIgroup, which in turn had levels 0.1-0.2%
12 18 24 30 36 42 48 54 60
Figure 5—Median HbAlc levels for the three in-
tensive delivery subgroups ( • , CSII; M, MDI; A,
mixed) for patients with at least 4.5 years of fol-
low-up. The 25th to 75th percentiles are shown by
the bars (P < 0.0001).
lower than the mixed group (P < 0.001for test of equality of average HbAlc val-ues; P = 0.010 for test of equality ofslopes over time).
A separate analysis was also con-ducted among all 711 intensively treatedsubjects comparing the HbAlc values ateach annual visit for patients using apump at the time of the visit versus thoseusing MDI, irrespective of pump versusMDI use at other visits. After adjustmentfor the effects of time, patients using apump at an annual visit had a meanHbAlc 0.27% less than that among thoseusing MDI (95% confidence interval0.185-0.35; P < 0.0001).
Bearing in mind the difficulty ininterpreting any differences between theintensive treatment subgroups that wereconstructed retrospectively, we foundsome differences in the adverse effects oftherapy among these three subgroups
370 DIABETES CARE, VOLUME 18, NUMBER 3 , MARCH 1995
Dow
nloaded from http://diabetesjournals.org/care/article-pdf/18/3/361/526529/18-3-361.pdf by guest on 14 January 2022

DCCT Research Group
Table 7—Adverse effects of intensive treatment rates and proportion by mode ofinsulin delivery
nPatient years of follow-up*Hypoglycemic events requiring assistance
No. of events (rate)No. of patients (%)
Hypoglycemic events resulting in coma/seizureNo. of events (rate)No. of patients (%)
DKANo. of events (rate)No. of patients (%)
OverweightNo. of events (rate)No. of patients (%)
MDI
2841,743
774 (44)166 (59)
171 (10)T88 (31)
13 (0.8)*12(4)
100 (7.9)100 (35)
CS1I
124761
408 (54)82 (66)
135 (18)t47 (38)
14(1.8)?10(8)
40 (7.2)40 (32)
Mixed
MDI CS1I
147486
307 (63)71(48)
83 (17)t38 (26)
3 (0.6)*2(1)
32 (9.4)32 (25)
413
225 (55)63 (43)
44(ll)t23 (16)
14 (3.4)?10(7)
24(9.1)24 (20)
Rates are expressed as events/100 patient-years over the first 5 years of follow-up (rate of events or percent-age). Overweight event rate is based on the time to the first occurrence of overweight over the first 5 years offollow-up. "During first 5 years of follow-up. tP = 0.009 MDI vs. CS11; P = 0.032 MDI vs. mixed-MDI.fP = 0.045 MDI vs. CS11; P = 0.002 MDI vs. mixed-CSll; P = 0.036 mixed-MDI vs. mixed-CSII.
Clinical center variation intreatmentThe total number of rehospitalizations,usually in General Clinic Research Cen-ters, for the purpose of improving meta-bolic control was 177 in 89 patients. Thisnumber varied greatly from 0 to 84 hos-pitalizations at the different clinics. Oneclinic reported a single patient admitted20 times for teaching and improvement ofmetabolic control. Mode of insulin deliv-ery also varied among clinics. The pro-portion of patients using CSII among the29 participating clinics ranged from 13 to96% of intensive treatment group pa-tients. The proportion of total patienttime spent receiving CSII therapy duringthe trial ranged from 7 to 89% amongclinics.
The median annual HbAlc con-centration from 1983 through 1992 in in-tensively treated patients varied by clinicfrom 6.6 to 7.4% and from 8.4 to 9.8%among conventionally treated patients
over the 4.5 to 5 years of follow-up (Ta-ble 7). The incidence of total episodesof severe hypoglycemia was not signi-ficantly different between these inten-sive treatment subgroups. The frequencyof episodes resulting in coma or seizurewas higher in the CSII group than inthe MDI group (P < 0.009). How-ever, among patients in the mixedgroup, the rate of such hypoglycemiaduring periods of MDI use (mixed-MDI)was also higher than in the MDI-onlygroup (P = 0.032). The incidence ofDKA was significantly higher in theCSII group and the mixed-CSII groupthan in the corresponding MDI groups.This indicates that CSII may be associatedwith a higher risk of hypoglycemia in-volving coma/seizure among patientswho do not switch modes of inten-sive treatment, and use of CSII is associ-ated with a higher risk of DKA. There wasno difference in the incidence of beingoverweight as a function of MDI or CSII
HypoglycemiaAbsolute RolativoRate Risk
use.
HbAlc (%)Figure 6—Median HbAu levels by DCCT clinic at annual visits from 1984 through 1992 for intensive
(^1) and conventional ( • ) therapy subjects. Absolute rates of severe hypoglycemia (episodes/100
patient-years) in intensive therapy subjects and relative risk of hypoglycemia for intensive compared
with conventional therapy subjects arc presented for each clinic.
DIABETES CARE, VOLUME 18, NUMBER 3 , MARCH 1995 371
Dow
nloaded from http://diabetesjournals.org/care/article-pdf/18/3/361/526529/18-3-361.pdf by guest on 14 January 2022

Implementation ofDCCT treatment regimens
(Fig. 6). The relative risk of severe hypo-glycemia and the absolute risk also variedby clinic. Among the five clinics with thelowest median HbAlc concentrations (all^6.8%), the average rate of severe hypo-glycemia among intensively managedpatients was 52 events/100 patient-years.This was similar to the rates of 51 events/100 patient-years in the five clinics with thehighest HbAlc concentrations (all ^7.3%)and the study group as a whole.
CONCLUSIONS— We have de-scribed in detail the components of con-ventional and intensive therapies in theDCCT. Although aspects of the DCCT in-tensive protocol were designed primarilyfor research purposes, the intensive treat-ment regimen and its benefits and adverseeffects should be relevant to clinical prac-tice.
The DCCT recruited two groupsof volunteers carefully selected to meetthe specific entry criteria. In addition tothe self-selection of the volunteers, the se-lection process involved an intensive ef-fort to inform the volunteers of the natureof the trial. The selection process resultedin a study cohort with above-average in-telligence and education. The study par-ticipants' adherence to the study protocolwas extraordinary, with <0.6% dropoutsand virtually complete adherence to as-signed treatment.
Clinic flexibility and willingnessto anticipate and meet the needs of indi-vidual study participants were probablymajor factors in the success of the trial.Also important were adequate staffing ofclinics to allow weekly telephone con-tacts, special training sessions for nursingand dietary personnel, and monitoring ofall clinics' performance by a central mon-itoring group. The level of adherence inthe clinical setting, with less selected pa-tients, is likely to be lower; on the otherhand, the DCCT results may providestrong motivation to health professionalsand patients alike that was not available toDCCT volunteers.
The remarkably stable levels ofglycemia among the conventionally
treated patients is noteworthy in view ofthe evolution of standard treatment of di-abetes in North America between 1984and 1992. The proportion of patientstreated with two daily injections of insu-lin was 81% in 1985, increased to 89% in1988, and remained at 90% until 1992.Of the conventionally treated volunteers,< 1 % were taking three or more daily in-jections for non-protocol-mandated rea-sons. The mean amount of insulin takenby the conventionally treated patients de-clined by -0.10 U/kg between 1984 and1985 and 1989 and 1992, which may bedue, in part, to the shift from animal spe-cies to human insulin (17% of the partic-ipants used human insulin in 1987 vs.57% in 1992) (22). Comparable decre-ments in mean insulin doses were alsoseen in the intensive treatment group.The number of conventional treatmentpatients performing self-monitoring ofblood glucose during the course of thetrial increased substantially. By 1992,—73% were monitoring their blood glu-cose at least once daily and 18% reportedadjusting their insulin dose based on self-monitoring of blood glucose, which wasnot a design feature of conventional ther-apy. Despite these changes over time,HbAlc levels remained relatively con-stant.
Among intensively treated pa-tients, median levels of glycemia werelowest in 1984 and 1985, during the fea-sibility phase of the DCCT, when —20%of the intensive treatment patients hadHbAlc values below the target value of6.05%. During this period, daily insulindoses and rates of severe hypoglycemiawere highest. After 1985, median levels ofHbAlc ranged between 7.0 and 7.2% un-til the end of the trial. Rates of severe hy-poglycemia and mean insulin dose de-clined between 1985 and 1992. Theproportion of patients annually withHbAlc <6.05% decreased and remainedbetween 7 and 11% between 1987 and1992. These observations suggest that ef-forts to decrease the frequency of hypo-glycemia, including adjustment of glu-cose goals, were partially successful but
may have contributed to a modest in-crease in HbAlc over time. Whether thedecrease in absolute rates of severe hypo-glycemia over time in both treatmentgroups was secondary to a relativelylower fraction of adolescents in the sec-ondary cohort over time, increased expe-rience on the part of the treatment teams,or other factors is unknown. The overallrates of severe hypoglycemia in the inten-sively treated patients were lower thanthose reported recently by the concurrentStockholm Diabetes Intervention Studythat used definitions of severe hypoglyce-mia similar to those used by the DCCT(23).
The fairly constant mean level ofglycemia seen after 1984 among inten-sively managed patients was in the settingof bidirectional switching of patients be-tween MDI and insulin pump treatmentregimens. After 1984, - 9 - 1 5 % of pa-tients switched in each year of the trial.Use of CSII varied substantially amongthe different clinics and was influenced bystaff attitudes and experience and otherfactors, such as the distance of the pa-tients from the various clinics. Among theintensively treated DCCT patients, forwhom all supplies and equipment wereprovided free of charge, —40% weretreated with CSII at the end of the trial.Although subject to multiple interpreta-tions, the comparison of patients whoused CSII or MDI throughout the courseof the study suggests that CSII use is as-sociated with modestly lower HbAlc lev-els and higher rates of DKA and severehypoglycemia resulting in coma or sei-zure. Whether this association is a func-tion of the particular intensive regimen,the patients (or clinics) that chose onemodality over another, or other factors, isunknown.
The relatively low percentage ofpatients who achieved dietary goals forfat, saturated fat, and cholesterol intakemay reflect the relatively less attentionpaid to these goals compared with glyce-mic goals. In the intensive treatmentgroup, nutrition counseling sessions fo-cused on helping patients develop the
372 DIABETES CARE, VOLUME 18, NUMBER 3 , MARCH 1995
Dow
nloaded from http://diabetesjournals.org/care/article-pdf/18/3/361/526529/18-3-361.pdf by guest on 14 January 2022

DCCT Research Group
problem-solving skills necessary to man-age the impact of food, insulin, and activ-ity on daily blood glucose goals.
Without careful patient selectionand intensive management by a coordi-nated group of expert personnel, at-tempts to implement intensive treatmentand maintain mean blood glucose in therange attained during the DCCT may re-sult in more frequent severe hypoglyce-mia than that seen in the trial. Severe hy-poglycemia was most common during thenight, and one-third of daytime episodesoccurred without recognized warning(21), stressing the need for frequent mon-itoring of bedtime and early morningblood glucose values and the routine useof frequent blood glucose monitoringduring intensive treatment. Reliance onsymptomatic hypoglycemia as an indica-tor of clinically significant hypoglycemiais not sufficient. Additional blood glucosemonitoring is necessary before driving,during and after strenuous exercise, andin patients with a previous history of hy-poglycemia unawareness or severe hypo-glycemia.
The excess weight gain seenamong intensively managed patients hasbeen reported previously by the DCCT(15) and others (24,25). Three factorsmay have contributed to the excessweight gain. First, caloric loss due to gly-cosuria was less in intensively managedpatients. Second, hypoglycemia may havecaused excessive food intake. Third, thepatient with well-controlled IDDM mayhave a more efficient pattern of energy ex-penditure than the patient with less well-controlled IDDM (26). Attention toweight gain and reduction in calorie in-take among patients with unwanted orexcessive weight gain were an integralcomponent of treatment in most clinics.Unwanted weight gain may be a signifi-cant impediment to successful intensivetherapy.
The DCCT study design does notpermit dissection of the intensive regimento determine which elements of the treat-ment were most critical to successful im-plementation. In the absence of such
data, the DCCT results support the imple-mentation of the intensive regimens usedin the study, including the team approachto therapy with heavy emphasis on theroles of the nurse educator and dietitianas integral members of the treatment team(13,27). Until other treatment methodsare demonstrated to provide superior re-sults to those in the DCCT, the insulin,dietary, and monitoring regimens, patientself-management training, and careful su-pervision described in this report shouldbe considered the standard of care formost patients with IDDM.
Acknowledgments— This study was sup-ported by the Division of Diabetes, Endocri-nology, and Metabolic Diseases of the NationalInstitute of Diabetes and Digestive and KidneyDiseases, National Institutes of Health,through cooperative agreements and a re-search contract. Additional support was re-ceived from the National Heart, Lung, andBlood Institute, the National Eye Institute, andthe National Center for Research Resources.
APPENDIX: DCCTRESEARCH GROUP,1 9 8 2 - 1 9 9 3 — Albert EinsteinCollege of Medicine—H. Shamoon, H.Duffy, N. Fleischer, S. Engel, P. Saenger,M. Strelyzn, M. Litwak, J. Wylie-Rosett,A. Farkash, D. Geiger, H. Engel,J. Fleisch-man, D. Pompi, N. Ginsberg, M. Glover,M. Brisman, E. Walker, A. Thomasunis, J.Gonzalez; Former members: M. Ville-neuve, M. Cypress, R. Portenoy, L.Lieberman, M. Schank, J. Chess, R.Mazze, B. Currie, P. Barry, D. Stasolla, R.Smorgan, P. Demas, D. Buble McGee, A.Wax. Case Western Reserve Universi-ty—S. Genuth, W. Dahms, E. Brown, P.Pugsley, L. Mayer, D. Kerr, B. Landau, L.Singerman, T. Rice, M. Novak, S. Smith-Brewer, J. McConnell, D. Drotar, D.Woods, M. Litvene, B. Katirji, C. Brown;Former members: P. Crawford, K. BehmJ.Rosenzweig, N. Kohlia, C. Woods, L. No-tarian, S. Parker, S. Horwitz, K. Puess, B.McBee; Acknowledgment: M. Lusk. Cor-nell University Medical Center—R.
Campbell, M. Richarson, M. Lackaye, B.Levy, S. Chang, M. Hein-Heinemann, S.Barron, L. Astor, D. LeBeck, D. Brillon, B.Diamond, A. Vasilas-Dwoskin, M. Bris-man, B. Laurenzi, N. Foldi, M. Rubin;Former members: L. Jovanovic, B. Boseo, J.Choppin, P. Farley, R. Herschcopf, H.Katzeff, F. Luckom-Nurnberg, D. Bajournas, R. Wilkins, K. Fong, R. Hanna, S.Rosen, L. Brenner-Gati, P. Tsairis, J. Bosc,
E. Darrell, R. Groce, J. Shovlin. HenryFord Hospital—F. Whitehouse, D. Kah -konen, D. Kruger, J. Fachnie, J. Fisk, J.Carey, M. Cox, B. Ahmad, F. Angus, H.Campbell, D. Fields, M. Croswell, K.Basha, P. Chung, A. Schoenherr, K. Mar-chiori, M. Mobley, J. Francis, J. Kelly;Former members:]. Brunncr, T. Overholt,R. Lesser,K. Adams, K. Dudewicz,J. Red-mond, D. Leach, M. Wisgerhof, J. Gold-man, K. Christopherson, J. Partamian. In-ternational Diabetes Center—D.Etzwiler, P. Hollander, P. Callahan, G.Castle, R. Bergenstal, M. Spencer, J. Nel-son, L. Bezecney, C. Roethke, M. Orban;Former members: J. Gott, N. Rude, B. Ol-son, W. Mestrezat, M. Franz, R. Ramsay,J. Gust, C. Kapsner, K. Bertils, T. Bun-kers-Lawson, D. Wilcox, A. Endy, D.Goetz, J. Sabo, L. McKenzie, D. Rahm, D.Ellis, R. Morris, R. Birk; Acknowledgments:C. Ulrich, L. Gill, K. Morgan, J. Laechelt,
F. Taylor, D. Freking, A. Towey, M. Liepp-man, S. Rakes, J. Magnum, N. Cooper, P.Upham. Joslin Diabetes Center—J. Jacobson, S. Crowell, J. Wolfsdorf, R.Beaser, O. Ganda, J. Rozenswieg, C. Stew-art, B. Halford, E. Friedlander, D. Tarsy,P. Arrigg, G. Sharuk, S. Shah, G. Wu, J.Cavallerano, R. Poole, R. Cavicchi, D.Fleming, J. Marcus, C. Griffiths, N.Capella; Former members: L. Rand, M. Po-mare, A. Kopple, L. Suprcnant, L. Me-Cowan, D. Marthinson, S. Zimmerman,L. Vignati, F. Dunn, S. Brink, N. Fred-holm, G. Cassens, M. Lorantos, J. I .am-bert, E. Reilly, K. Finn, M. Maloberti, P.Spanolo, J. Eisenstein, L. Wolfe, H. Men-dez, N. Mitchell, L. Kinzel, D. Rothstein,L. Poirier, D. Mohsin, A. Bell, K. Bach-man. Massachusetts General Hospi-tal—D. Nathan, M. Larkin, J. Godinc, S.
DIABETES CARE, VOLUME 18, NUMBER 3 , MARCH 1995 373
Dow
nloaded from http://diabetesjournals.org/care/article-pdf/18/3/361/526529/18-3-361.pdf by guest on 14 January 2022

Implementation ofDCCT treatment regimens
Brink, D. Norman, C. McKitrick, L. Dela-hanty, E. Anderson, P. Lou, C. Taylor, D.Cros, J. Lynch, D. Meinkes, K. Folino, R.Lyon; Former members: C. Kelley, C. Hag-gen, K. Hansen, L. Selter, M. Grinvalsky,D. Kawahara, H. Bode, B. Shahani, D.Seeley, H. Leahy, P. Chong, S. Gominak,L. Coleman, M. Hayes; Acknowledgments:K. Abbott, K. Sicotte, S. Morton, R. Pro-tasowicki. Mayo Foundation—F. Ser-vice, A. Schmidt, R. Rizza, B. Zimmer-man, W. Schwenk II, J. Mortensen, G.Ziegler, A. Lucas, N. Hanson, J. Pach, R.Woodwick, R. Tackmann, G. Suarez, K.LeBarron, M. Shumann, M. Lien; Formermembers:]. Novak, M. Haymond, J. Gres-eth, B. Klein, K. Burns, T. McPhee, L.Schafer; Acknowledgments: J. Trautmann,J. King, J. Rostvold, T. Link, P. Dyck, J.Daube, R. Colligan, A. Windebank, D.Jensen, A. Oeltjen, G. Bartley. MedicalUniversity of South Carolina—J. Col-well, R. Mayfield, J. Pickett, D. Wood, M.Chitwood, D. Billings, Y. Dabney, J. Buse,L. King, S. Vale, T. Thompson, B. Bohm,T. Lyons, K. Hermayer, A. Rice; Formermembers: C. Saylor, J. Parker, M. Boehm,V. Sanford, M. Oxemann, E. Jenkinson,E. Chandler, H. Wohltmann, I. Hansen,K. Boggess, J. Chambers, N. Clair, J. Ca-sat, E. Sturgis, M. Hughes, K. Zarzar, T.Catoe; Acknowledgments: G. Reid, J. Hop-kins, M. Lane, Y. Rosen. NorthwesternUniversity—M. Molitch, B. Schaefer, C.Johnson, J. Lyons, B. Metzger, B. Cohen,T. Nishida, K. Parque, V. Yusim, M.Moore, K. Dineen, J. Stahl, L. Richine, D.Weinberg, I. Loose, M. Kushner, L. Jam-pol; Former members: L. Hirsch, O. Green,A. Campbell, M. Powers, J. Puklin, R. Se-gura, M. Orzech, E. Basian, N. Bezino-vich, B. Tallman, N. Freinkel, B. Silver-man, S. Heller, C. Bouska, J. Gerty, M.Giese. University of British Colum-bia—A. Morrison, H. Tildesley, A. Jal-bert, S. Leung, I. Begg, D. Johnson, T.Kennedy, G. Meadows; Former members:J. Hunt, S. Brunsdon. University of Cal-ifornia, San Diego—O. Kolterman, G.Lorenzi, K.Jones, M. Goldbaum, I. Grant,M. Swenson, R. Reed, K. Kadlec, M. Giot-ta, R. Lyon, L. Kirsch; Former members: G.
Friedenberg, M. Prince, L. Fish, J. Gross,J. Crapotta, R. Garcia, A. Listhous; Ac-knowledgments: T. Clark, J. Grant, R.Ochabski, R. Gloria, J. Goodman, G.Birchler, R. Abram, S. Cahill, L. Sayner, B.Grasse, L. Christie; B. Abreu. Universityof Iowa—R. Zietler, W. Sivitz, H. Schrott,R. Hoffman, J. Maclndoe, J. Kramer, M.Bayless, N. Olson, B. Tindal, L. Snetse-laar, D. Mueller, J. Swartzendruber;Former members: A. Dudler, K. Smith, R.Thompson, J. Brown, C. Read, A. Packer,J. Baron, B. Ekdom, R. Dreyer, J. Tracy, B.Ginsberg, J. Kimura, L. Metcalf, K. Reiset-ter, M.Jones, C. Blodi, P. Bosch, D. Mey-erson, J. LeGrand, C. Hansen, B. Vino-grade, E. Whitmore, G. Mitchell, J.Pulido; Acknowledgments: T. Weingeist, A.Kimura, E. Stone, T. Grout, C. Fountain,S. Karakas, C. Vogel, P. Montague, D.Keyser, S. Mennan, C. Doggett, G. Rose,K. DeVet, P. Muhle. University of Mary-land School of Medicine—A. Kowarski,P. Levin, D. Ostrowski, D. Young-Hy-man, S. Chalew, M. Barlow, J. Hylton, V.Lakhanpal, M. Elman, W. Buie, Jr., S.Blum, B. Weiner, B. Mace, M. Millar. Uni-versity of Michigan—D. Greene, J.Floyd, C. Martin, S. Bennett, A. Lasichak,A. Vine, J. Albers, T. Sandford, J. Loftin,M. Stevens, S. Elner, F. Dunn, D. Henry;Former members: B. Anderson, N.Burkhart, N. White, W. Herman, S.Sneed; Acknowledgments: C. Martonyi, F.Mclver, S. Stanley, J. Willis, S. Nalepa, K.Ryan, T. Spiegelberg, B. Glasgow, E.Chan, P. Dotimas, A. Burke, J. Bocszar,M. Thomas, L. Bardack, J. Peters, C. 01-szewski, D. Spica. University of Minne-sota—J. Bantle, M. Balles, W. Kennedy,M. Khan, M. Mech, J. Olson, C. Kwong, L.McKenzie, R. Ramsay, R. Warhol, W.Robiner, W. Knoblock; Former members:J. Barbosa, H. Hoberman, B. Hoogwerf, L.Schmidt, C. Boehnert, F. Goetz, D. Klein,E. Ryan, Jr., T. Strand, H. Cantrill, M.Popkin, A. Moran, D. Brown, D. Trence,B. Jackson; Acknowledgments: K. Johnson,B. Cherryhomes, C. Roiger, J. Stein, R.Sahinen, G. McDonough, A. Genia, M.Monahan, J. Haynes, N. Oestreich, D.Philiph, B. McMichael, L. Fimreite, E.
Stinson, L. Ponwith, P. Straus, J. Verness.University of Missouri—D. Goldstein,M. Hall, T. Burns, D. Klachko, J. Giangi-acomo, S. Rawlings, L. Aston, J. England,H. Wiedmeyer, M. Daugherty, M. Light-foot, R. Wilson, R. Wilson, K. Blinder, L.Gash, D. Gardner, G. Griffing, M. Brown-lee-Duffeck, N. Rebecca Palmer, R. Con-way; Former members: C. Ide,J. Simonds,R. Wertheimer, J. Pickens, S. Hanson, K.Smarr, C. Mihalevich, J. Grasela, T. Per-rigo, C. Meier. University of New Mex-ico School of Medicine—D. Schade, C.Johannes, R. Reidy, J. Bicknell, A. Vogel,D. Drumm, N.Jones, P. Boyle,J. Canady,D. Nickell, F. Crofton; Former members:G. Argoud, J. Rich, V. Brittain, G. Sieja, J.Morris, R. Eaton, L. Johnson, L. Atler, P.Shaw. University of Pennsylvania-Chil-dren's Hospital of Pennsylvania—L.Baker, P. Ilves-Corressel, S. Schwartz, S.Braunstein, J. McBride, A. Brucker, L.Rendle, M. Brown, J. Sladky, B. Masack-Carey, D. Lawley, W. Nyberg, L. Weeney,E. Sanburg, S. Byrd, E. Aguado, N. Mul-holland, D. Cahn, M. Suscavage; Formermembers: K. Wong, W. Williamson, C.Stanley, R. Kaye, K. Schlichter; Acknowl-edgments: J. Egler, M. Vaughan-Norton,C. Collins-Burke, H. Mameniskis. Uni-versity of Pittsburgh—A. Drash, J.Wesche, M. Bratkowski, D. Becker, S. Ar-slanian, B. Doft, D. Finegold, L. Lobes, J.Rinkoff, J. Wamicki, D. Curtin, D. Stein-berg, G. Vagstad, C. Ryan, F. Harris, L.Steranchak, J. Arch, K. Kelly, K. Olsen, P.Ostroska, M. Guiliani, M. Good, T. Wil-liams, A. Campbell, C. Shipe, P. Flavia, R.Conwit; Former members: D. Greene, J.Ulbrecht, P. Carroll, J. Johnston, R.Salata, T. Yeager, C. Longstreet, S. Baser,R. Sabo, N. Fisher, W. Evron, K. Mel-linger, L. Morrow, R. Wing, V. Kamp-Nielsen, M. Kiok, J. Moore, J. Gerich, A.Peterson, W. Smith, P. Kendrick, M.McHugh. Acknowledgments: M. Zaucha,C. Priore, L. Henry, S. Braden. Univer-sity of South Florida—J. Malone, D. Mc-Millian, N. Grove, L. Babione, T. DeClue,P. Pavan, J. Korthals, H. Sole, A. Man-gione; Former members: A. Morrison, B.Kranendonk, J. Kaenzig. University of
374 DIABETES CARE, VOLUME 18, NUMBER 3, MARCH 1995
Dow
nloaded from http://diabetesjournals.org/care/article-pdf/18/3/361/526529/18-3-361.pdf by guest on 14 January 2022

DCCT Research Group
Tennessee-Memphis—A. Kitabchi, L.Taylor, T. Bertorini, G. Burghen, J. Fisher,T. Hughes, J. Linn, D. Meyer, W. Mur-phy, M. Justice, A. Sherman, L. Wright, L.Murphy, H. Ricks; Former members: L.Amis, M. Briggs, L.Jones, M. Murphy, M.Orlick, S. Sundbye, J. Stanfield, K. Pitts, J.Bittle; Acknowledgments: D. Adkins, A.Crisler, H. Lambeth, J. Runyan. Univer-sity of Texas Southwestern MedicalCenter—P. Raskin, S. Strowig, M. Basco,S. Cercone, L. Ramirez, R. Anand, C. Wil-son, R. Greenlee; Former members: J.Marks, L. Sullivan, G. Sanborn, T. Fri-berg, D. Giles, J. Halter, G. Pesicka, J.Rosenstock, R. Fish; Acknowledgments: W.Anderson, M. Biggs, E. Mendelson, J.Moore, B. Newton, L. Pels, K. Sherrill, P.Vanachek, J. Howard, C. Ousley, B. Yates,D. Conger, K. Beaudet, B. Maguire. Uni-versity of Toronto—B. Zinman, A.Barnie, R. Ehrlich, D. Daneman, K. Perl-man, L. Leiter, R. Devenyi, C. Mortimer,A. Gordon, R. Ferguson, K. Camelon, S.Simkin, C. Littlefield, G. Rodin, K. Hart-ley, J. Kwan, D. Gnanapandithen, S. Rog-ers, S. McLean, L. MacKeen, C. Miller, M.Mandelcorn, P. Nellis, L. Ruttan, D. Wil-son-Smith; Former members: I. Gottes-man, S. McClure, L.Johnston, C. Worth-ington, D. Buchanan, L. Bauer, V.Kozousek, S. Mendlowitz, P. Defeudis, V.Gilbert, E. Chew, S. Craven, C. McCul-loch, M. Pickard, B. Rich, K. Moffat, L.Haye, J. Rosen, S. Mezei, E. Bailey, A.Walker, O. Plain, S. Walker, S. Hope-Williams, A. Lazosky, J. Vasarhelyi, B.Dibkin, M. Fischer. University of Wash-ington—J. Palmer, J. Ginsberg, J. Kin-youn, H. Doerr, R. Mauseth, K. Sweeney,L. Ottingham, L. Thomson, C. Green-baum, L. Sameshima, I. Hirsch, R. Far-kas-Hirsch, G. Rosenbaum, N. Rubner, T.Brown, G. Kraft, J. Broeckel, M. Karlsen,D. Khakpour, M. Ramirez; Former mem-bers: M. Gordon, H. Hayashi, L. Klaff, D.Frankel, D. McCullough, V. Cook, R.Cox, D. Bedford, M. Bordeaux, M. Mc-Masters, J. Woodward, K. Parker, A. Ul-richson, S. Schoenfleld, S. Rattray, L.White, D. Kanter; Acknowledgments: B.Clifton, R.Jones, B. Lawrence, P. Ernst, T.
Erickson, N. Mettert, L. Stout, B. Smit, L.Mix. University of Western Ontario—J.Dupre, N. Rodger, P. Colby, I. Hramiak,M. Jenner, C. Canny, W. Brown, T.Smith, J. Harth, S. Bondy, S. Beath, S. Mc-Cabe, C. Gouchie; Former members: J.Galbraith, J. McDonald, J. Adair, P. Hei-denheim, G. O'Hanley, C. Schwartz, V.Kozousek, R. Garcia, M. Brent, S. Ru-scher, S. Kosar, D. Vollick, J. Mahon, H.Burton, J. Evans, R. Duncan; Acknowledg-ments: K. Blanchard, J. McCallum, S.Jung, C. Walter, P. Williamson, A. Sue-Tang. Vanderbilt University—R.Lorenz, J. Lipps, J. McRae, J. May, M.May, P. Campbell, S. Feman, A. Kilroy, C.Pulliam, D. Schlundt, K. Jannasch, D.Davis; Former members: J. Diekhoff, A.Samowich, N. Christensen, 1. Burr, I. Tur-kat, R. Jamison, R. Scruggs, T. Kelly; Ac-knowledgments: N. Cullen, C. Leslie, K.Hoover, M. Snell, C. Premeau, T.Sbrocco, T. Adkins, B. Lacy, K. Virts, L.Quesenberry. Washington University,St. Louis—J. Santiago, N. White, L.Levandoski, J. McGill, J. Bubb, R. Oik, M.Noetzel, I. Boniuk, M. Grand, R. Kacizak,E. Ort, G. Nobel, J. Bodner, J. Dahl, P.Bilyeu, M. Thomas, J. Blank, L. Schmidt,Y. Strassburg, C. Walters, D. Williams, P.Rodriguez, M. Erickson, S. Hedrick, L.Breeding, G. Hoffmeyer; Former members:N.Janes, B. Talent, M. Casso, M. Paige, L.Miller, R. Escoffery, J. Marnett, P. Am-brose, M. Howard, R. Shalwitz, R. Bouri-saw, D. Kroll. Yale University School ofMedicine—W. Tamborlane, J. Ahern, R.Sherwin, P. Gatcomb, K. Stoessel, N.Held, J. Ebersole, I. Scanlon; Formermembers: J. Puklin, N. Tiglio-Ruches, W.Petit, J. Rolland, R. Louard; Acknowledg-ments: C. Wildstein, D. Bilodeau, K. Fong,D. Ottaviano, C. Larson.
Office of the Chairman, Vander-bilt University—O. Crofford. Data Co-ordinating Center, George WashingtonUniversity—J. Lachin, P. Cleary, D.Thompson, D. Kenny, S. Lan, G. Lan, A.Brenneman, W. Owen, J. Backlund, K.Adams, D. Arnold, R. Campanell, N. Lor-ing, P. Scheirer, D. Becker, N. Janifer, D.Lamas, C. Dunegan, H. Atluri, C. Wil-
liams, S. Abdul-Baaqiy, S. Pakalapati, V.Yalamanchili, S. Ho, R. Friedman, B. Me •Naney,J. Givens,Y. Colaco, M.Jenifer, R.Osborne, V. Zell, J. Young; Fonncr mem-bers: P. Gilbert, J. Knoke, A. Zbikowski, S.Sorlie, F. Eliopoulos, M. Foulkes, M.Tanenberg, M. Halperin, D. Kruger, R.Tanenberg, Q. Barros, J. Dunbar, W.Watson, H. Hollander, E. White, D. l e v -eling. Consultants—A. Kassoff, K. Ad-ams, I. Grant, R. Heaton, J. Dorman, R.Spielman, R. Klein. National Institute ofDiabetes and Digestive and KidneyDiseases Program Office—C. Siebert, D.Beverly, S. Shores, L. Stecklein, T. Pike;Former members: R. Silverman, S. Heyse,D. Belcher, K. Newlin, R. Sherwin, L.Zalc, J. Schlechter. Central Units: Cen-tral Autonomic Coding Unit (SouthernIllinois University)—M. Pfeiffer, M.Schumer, M. Moran, J. Farquhar; Fonncrmembers: K. Hoskins, R. Hand. BackupHbAlc Laboratory (University of Mis-souri)—J. England, H. Wiedmeyer; Ac-knowledgment: C. Rohlfing. Central Fun-dus Photograph Reading Center(University of Wisconsin)—M. Davis,L. Hubbard, Y. Magli, S. Thomas,J. Ono-frey, K. Jensen, R. Brothers, S. Ansay, J.Armstrong, D. Badal, M. Vanderhoof-Young, B. Esser, P. Gelthman, D. Hurl-burt, J. Reimers, K. Kewley, K. Miner;Former members: M. Harding, G. Boone,S. Meuer, V. Wipperfurth, P. Segal, A.Ganguly, P. Chinn-Sloan, L. Dold, A.Temple. Central Biochemistry Labora-tory (University of Minnesota)—M.Steffes, J. Bucksa; Former HbAh. Labora-tory, Joslin Diabetes Center: S. Soeldner, M.Tanenberg. Central NeurobehavioralCoding Unit (Western Psychiatric In-stitute and Clinic)—C. Ryan, K. Adams;Acknowledgments: R. Catanzaro, A. Lukes,G. Bagovich, T. Woodnll. Central ECGReading Unit (University of Minneso-ta)—R. Crow, C. Johnson, B. Carlson;Former members: R. Prineas, M. Mac-Donald. Central Nutrition Coding Unit(University of Minnesota)—I. Buzzard,M. Stevens, B. Sielaff, B. Pickering, S.Schakel; Former members: J. Wenz, Y. Sic-vert. Economic Evaluation Unit•—W.
DIABETES CARE, VOLUME 18, NUMBER 3, MARCH 1995 375
Dow
nloaded from http://diabetesjournals.org/care/article-pdf/18/3/361/526529/18-3-361.pdf by guest on 14 January 2022

Implementation ofDCCT treatment regimens
Herman (chairman), E. Dasbach, T.Songer, G.Janes, P. Smith. Mortality andMorbidity Committee—L. Deeb, R.Ewart, T. Orchard. Data, Safety, andQuality Review Group—C. Clark(chairman), G. Cutter, M. Davis, D.DeMets, F. Ferris, C. Furberg, E. Horton,J. Keen, D. Lockwood, P. Palmberg, B.Rourke, T. Tsiatis. Policy AdvisoryGroup—R. Levy (chairman), R. Frank, J.Grizzle, A. Rubenstein, J. Schneider, J.Skyler. Industrial support (organiza-tions providing goods, services, and/ordiscounts to the DCCT. This listing doesnot reflect endorsements of these compa-nies; it simply recognizes their generoussupport of the trial)— Abbott Industries;Acme United Corporation; Alladin Indus-tries; Ames Division, Miles Laboratories;Auto-Syringe and Flint Divisions, Trave-nol Laboratories and Travenol Canada;Beckman Instruments, Becton-Dickin-son; Belmont Springs; Bio Dynamics Di-vision, Boehringer Mannheim Diagnos-tics; Bio-Rad Laboratories; CardiacPacemaker; Costar; Derata Corporation;Eli Lilly and Company; Federal Express;General Foods Corporation; Hewlett-Packard; Laboratory Data Control Divi-sion, Milton Roy Company; Lifescan;Med-Tec Gases; Micromeritics; MonroeStationers; Nordick USA; Polyfoam Pack-ers Corporation; The Purdue FrederickCompany; Rainin Instrument Company;Smith, Kline and French Laboratories;Squibb-Novo; Teledyne Avionics; TerumoMedical Corporation; 3M; Thermo-Serv;Ulster Scientific; Union Carbide Corpora-tion; Vanguard International; and WelderSupply Company.
References1. DCCT Research Group: The Diabetes
Control and Complications Trial (DCCT):design and methodologic considerationsfor the feasibility phase. Diabetes 35:530-545,1986
2. DCCT Research Group: The effect of inten-sive treatment of diabetes on the develop-ment and progression of long-term compli-cations in insulin-dependent diabetesmellitus. N Engl J Med 329:977-986,1993
3. DCCT Research Group: Diabetes controland complications trial (DCCT): update.Diabetes Care 13:427-433, 1990
4. DCCT Research Group: Implementationof a multicomponent process to obtain in-formed consent in the diabetes controland complications trial. Controlled ClinTrials 10:83-96, 1989
5. DCCT Research Group: Feasibility of cen-tralized measurements of glycated hemo-globin in the Diabetes Control and Com-plications Trial: a multicenter study. ClinChem 33:2267-2271, 1987
6. DCCT Research Group: DCCT Protocol.Springfield, VA, Dept. of Commerce, Na-tional Technical Information Service,1988 (publ. no. 88-116462-AS)
7. DCCT Research Group: DCCT Manual ofOperations. Springfield, VA, Dept. ofCommerce, National Technical Informa-tion Service, 1993 (publ. no. PB-93-82282)
8. DCCT Research Group: Diabetes Controland Complications Trial (DCCT): resultsof feasibility study. Diabetes Care 10:1—19,1987
9. Burke BS: The dietary history as a tool inresearch. J Am Diet Assoc 23:1041-1046,1947
10. Franz M, Krosnick A, Maschak-Carey BJ,Parker T, Wheeler F: Coals jor DiabetesEducation. Alexandria, VA, American Dia-betes Association, 1989
11. Cholesterol Adult Treatment Panel Re-port: Report of the National CholesterolEducation Program Expert Panel on de-tection, evaluation, and treatment of highblood cholesterol in adults. Arch InternMed 148:36-69, 1988
12. Siebert C, Clark DM Jr: Operational andpolicy considerations of data monitoringin clinical trials: the Diabetes Control andComplications Trial experience. Con-trolled Clin Trials 14:30-44, 1993
13. DCCT Research Group: Expanded role ofthe dietitian in the Diabetes Control andComplications Trial: implications forclinical practice. J Am Diet Assoc 93:758-767,1993
14. DCCT Research Group: Nutrition inter-ventions for intensive therapy in the Dia-betes Control and Complications Trial. JAm Diet Assoc 93:768-772, 1993
15. DCCT Research Group: Weight gain as-
sociated with intensive therapy in the Di-abetes Control and Complications Trial.Diabetes Care 11:567-573, 1988
16. Williamson DF, Kahn HS, Remington PL,Anda RF: The 10-year incidence of over-weight and major weight gain in US adults.Arch Intern Med 150:665-672,1990
17. Liang KY, Zeger SL: Longitudinal dataanalysis using generalized linear models.Biometrika 73:13-22, 1986
18. Zeger SL, Liang KY: Longitudinal dataanalysis for discrete and continuous out-comes. Biometrics 42:121-130, 1986
19. Holm S: A simple sequentially rejectivemultiple test procedure. Scand J Stat6:65-70, 1979
20. Wei LJ, Lachin JM: Two-sample asymp-tomatically distribution-free tests for in-complete multivariate observation. J AmStat Assoc 79:653-661, 1984
21. The DCCT Research Group: Epidemiol-ogy of severe hypoglycemia in the Diabe-tes Control and Complications Trial. AmJMed 90:450-459, 1991
22. Gulan N, Gottesman IS, Zinman B: Bio-synthetic human insulin improves post-prandial glucose excursions in type I dia-betes. Ann Intern Med 107:506-509,1987
23. Reichard P, Nilsson BY, Rosenqvist U:The effect of long-term intensified insulintreatment on the development of micro-vascular complications of diabetes melli-tus. NEnglJ Med 329:304-309, 1993
24. Wing RR, Klein R, Moss SE: Weight gainassociated with improved glycemic con-trol in population-based sample of sub-jects with type I diabetes. Diabetes Care13:1106-1109, 1990
25. Reichard P, Berglund B, Britz A, Cars I,Nilsson BY, Rosenqvist U: Intensifiedconventional insulin treatment retardsthe microvascular complications of insu-lin-dependent diabetes mellitus (IDDM):the Stockholm Diabetes InterventionStudy (SDIS) after 5 years. J Intern Med230:101-108
26. Carlson M, Campbell P: Intensive insulintherapy and weight gain in IDDM. Diabe-tes 42:1700-1707,1993
27. The DCCT Research Group: The role ofthe trial coordinator in the Diabetes Con-trol and Complications Trial. DiabetesEduc 19:509-512, 1993
376 DIABETES CARE, VOLUME 18, NUMBER 3 , MARCH 1995
Dow
nloaded from http://diabetesjournals.org/care/article-pdf/18/3/361/526529/18-3-361.pdf by guest on 14 January 2022