
Implementation of High Fidelity Post- Partum Hemorrhage ...
20
Implementation of High Fidelity Post- Partum Hemorrhage Simulation for an Acute Care Multisite, Interprofessional Women and Children’s Service Line Improves Patient Care Outcomes Laura Wining MSN, CHSE, CAPA, CHPN Coordinator of Education Programs-Simulation Tracy D. McGuire, MSN, RNC-HROB, C-EFM, FM Clinical Education Nurse-Women’s and Children’s Service Line
Transcript of Implementation of High Fidelity Post- Partum Hemorrhage ...
Implementation of High Fidelity Post-Partum Hemorrhage Simulation for an Acute Care Multisite, InterprofessionalWomen and Children’s Service Line Improves Patient Care Outcomes
Laura Wining MSN, CHSE, CAPA, CHPNCoordinator of Education Programs-Simulation
Tracy D. McGuire, MSN, RNC-HROB, C-EFM, FMClinical Education Nurse-Women’s and Children’s Service Line

ANCC
Continuing Nursing Education
International Nursing Association for Clinical Simulation & Learning is accredited as a provider of continuing nursing education by the
American Nurses Credentialing Center’s Commission on Accreditation.

Disclosures
1. Conflict of Interest
• Laura Wining reports no conflict of interest• Tracy D. McGuire reports no conflict of interest•Julia Greenawalt (INACSL Conference Administrator & Nurse Planner) reports no conflict of interest• Leann Horsley (INACSL Lead Nurse Planner) reports no conflict of interest
2.
Successful Completion
• Attend 100% of session• Complete online evaluation

Learning Outcomes
Upon completion of this educational activity, participants will be able to:
1. Identify at least three ways to successfully develop interprofessional, multisite, in situ, simulation education scenarios.
2. Summarize different opportunities found post education that will contribute to determining the effectiveness of simulation offerings.
3. Give examples of how to begin development of simulation education through a needs assessment that will later assist in measuring qualitative data to determine effectiveness of simulation education offerings.
4Set footer with Insert > Header & Footer
Medical Center of the Rockies Poudre Valley Hospital 187 Patient Beds 262 Patient Beds

Simulation Objectives in 2015-2016
To implement an in situ high fidelity simulation for a multisite multidisciplinary Women and Children’s service line to increase early Crew Resource Management and use of medications for effective treatment in patients with postpartum hemorrhage (PPH), therefore decreasing surgical interventions and blood product replacement.
6Set footer with Insert > Header & Footer

Setting:A large hospital system in Colorado where approximately 3,500 women give birth each year.
Participants:Each simulation included 4 nurses, 1-2 physicians, and 1 technician45 High Fidelity Simulations were completed with a total of: 195 nurses 34 physicians 24 surgical techs
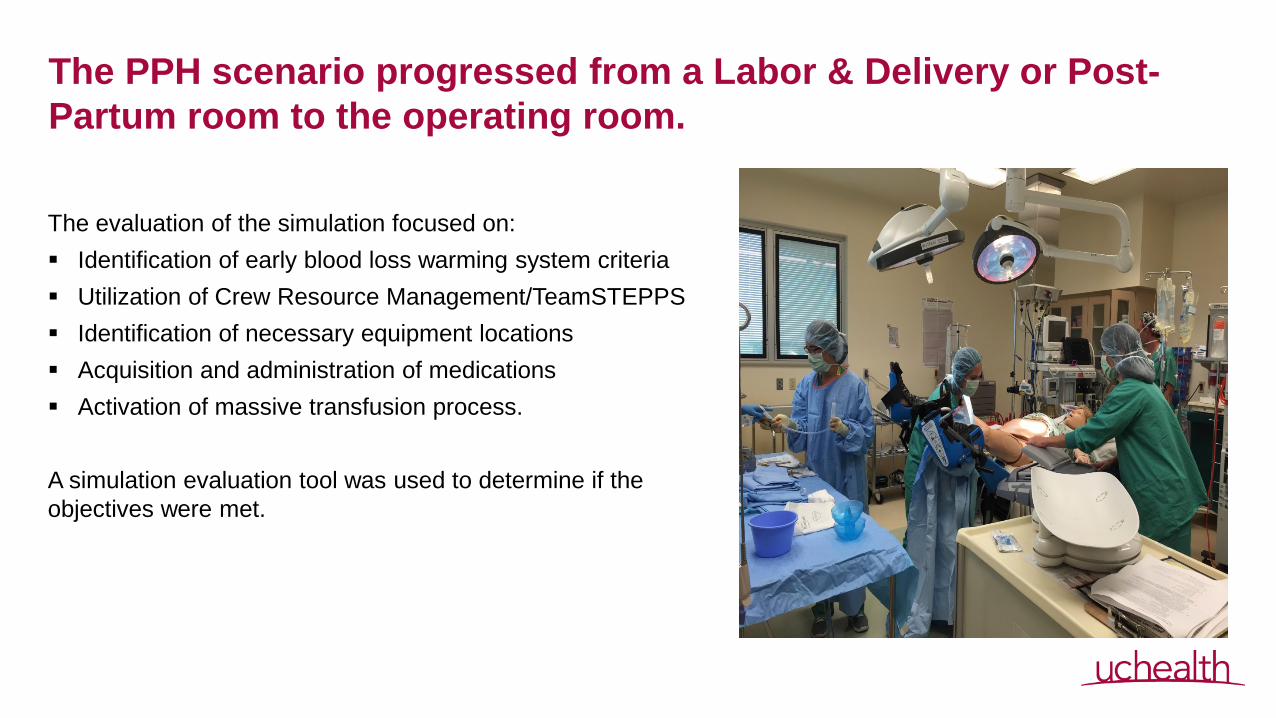
The PPH scenario progressed from a Labor & Delivery or Post-Partum room to the operating room.
The evaluation of the simulation focused on: Identification of early blood loss warming system criteria Utilization of Crew Resource Management/TeamSTEPPS Identification of necessary equipment locations Acquisition and administration of medications Activation of massive transfusion process.
A simulation evaluation tool was used to determine if the objectives were met.

Each Simulation Included:
20 Minute Scenarios
Per INACSL Standards of Simulation Education ractices
9Set footer with Insert > Header & Footer

Developing a Successful Simulation Education ScenarioWith consideration of Interprofessional, Multisite, and In Situ components
10Set footer with Insert > Header & Footer
1. Include all stakeholders from different disciplines in the planning phases.
2. Begin with a needs assessment that incorporates all interprofessionalneeds. Quality/Safety Intelligence Reports (SI) New Early Blood Loss Intervention (EBI) Policy Hardwiring Team Response and Delineation of Roles
3. Self Scheduling through an electronic learning management system with stakeholders involvement in date/time/site selection.
UCHealth North Simulation Center
Unit/Area- Mother and Children Service Line RN/Tech/Physician Simulation Name- Lucy Heart-Post-Partum Hemorrhage Purpose of Simulation- Annual competency for staff Anticipated Participants per Simulations- 7 Participants per scenario Content to be included- Utilization of the EBI policy with recognition of the EBI trigger criteria, Medication administration for obstetrical hemorrhage, Initiation of massive transfusion protocol, Practice emergent SBAR communication/hand-off, Perform mechanical hemorrhage interventions. Objectives:
1. The participants will appropriately administer uterotonics in the post-partum hemorrhaging patient.
2. The participants will demonstrate knowledge of policy and procedures for hemorrhage management.
3. The participants will apply SBAR communication and closed loop communication appropriately within the simulation.
4. The participants will demonstrate appropriate documentation for the actively hemorrhaging patient.
5. The participants identify additional needs and seek additional resources appropriately.
Supplies-Noelle simulator with boggie uterus, Name band with blood lock code, glasses, BP cuff, D & C/Hyst Tray-Totes, Bakri Balloon, hemabate, methergen, Pitocin, cytotec, foley, LR to gravity, NS, Blood draw tubes, Blood/tubing, IV start pack, Vacutainers, pressure bag, med syringes,
Developing a Successful Simulation Education Scenario (Continued)
With consideration of Interprofessional, Multisite, and In Situ components
11Set footer with Insert > Header & Footer
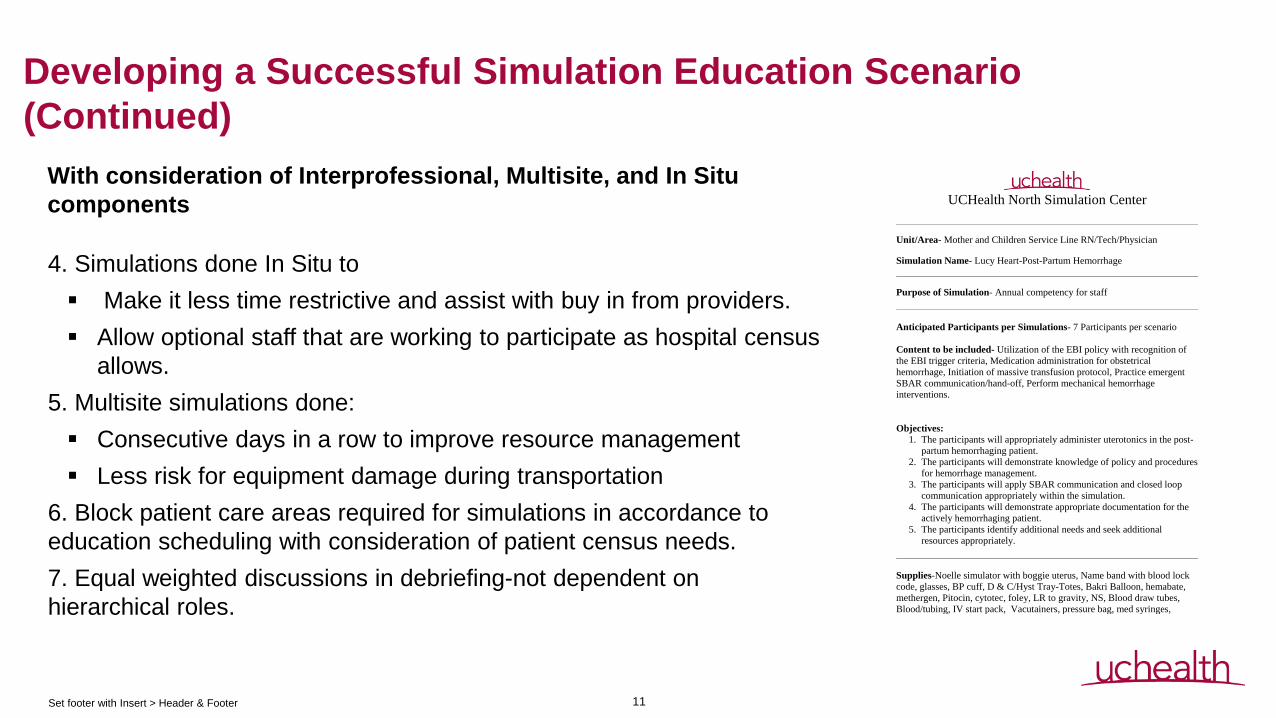
4. Simulations done In Situ to Make it less time restrictive and assist with buy in from providers. Allow optional staff that are working to participate as hospital census
allows.5. Multisite simulations done: Consecutive days in a row to improve resource management Less risk for equipment damage during transportation
6. Block patient care areas required for simulations in accordance to education scheduling with consideration of patient census needs. 7. Equal weighted discussions in debriefing-not dependent on hierarchical roles.
UCHealth North Simulation Center
Unit/Area- Mother and Children Service Line RN/Tech/Physician Simulation Name- Lucy Heart-Post-Partum Hemorrhage Purpose of Simulation- Annual competency for staff Anticipated Participants per Simulations- 7 Participants per scenario Content to be included- Utilization of the EBI policy with recognition of the EBI trigger criteria, Medication administration for obstetrical hemorrhage, Initiation of massive transfusion protocol, Practice emergent SBAR communication/hand-off, Perform mechanical hemorrhage interventions. Objectives:
1. The participants will appropriately administer uterotonics in the post-partum hemorrhaging patient.
2. The participants will demonstrate knowledge of policy and procedures for hemorrhage management.
3. The participants will apply SBAR communication and closed loop communication appropriately within the simulation.
4. The participants will demonstrate appropriate documentation for the actively hemorrhaging patient.
5. The participants identify additional needs and seek additional resources appropriately.
Supplies-Noelle simulator with boggie uterus, Name band with blood lock code, glasses, BP cuff, D & C/Hyst Tray-Totes, Bakri Balloon, hemabate, methergen, Pitocin, cytotec, foley, LR to gravity, NS, Blood draw tubes, Blood/tubing, IV start pack, Vacutainers, pressure bag, med syringes,

Opportunities Actualized Post Simulation to Improve patient Care
Identified Opportunities
1. RN’s unsure about their roles in OR as Primary and Secondary nurses.
2. Identified different processes between sites for how each activates a resource response for a massive transfusion protocol (MTP).
3. Knowledge deficits with utilization and allocation of Level 1 Rapid Infuser.
4. Knowledge deficits with providing assistance to Anesthesia with rapid sequence intubation (RSI).
Implemented Interventions
1. Signage hung in all OR’s with role delineation.
2. Implemented a standardized process for activating MTP.3. Follow up education provided to staff with hands on remediation validated.
4. Follow up education that included individual check offs with charge RN’s and every primary RN.
12Set footer with Insert > Header & Footer

Opportunities Actualized Post Simulation to Improve patient Care
Identified Opportunities
5 . Difficulty setting up OR table stir-ups for correct patient placement that delayed emergency care with one participant injury during education.6. Personal protective equipment (PPE) for OR entry not available at one entrance to OR that delayed movement of patient to OR.7. Inconsistent utilization of Post Partum Hemorrhage (PPH) cart for patient care needs.
Implemented Interventions
5. Follow up education that included individual check offs with charge RN’s and every primary RN.
6. All labor rooms now have PPE available at the exit to the room to expedite emergency departure to OR.
7. Process change to include the PPH cart with all OR set ups.
13Set footer with Insert > Header & Footer

Developing Simulations through a Needs Assessment to assist in Qualitative Measurement
1. Identify your current standard quality chart review process and preexisting quality matrix.
2. Based on current quality data analysis develop objectives/outcomes for the simulation education.
A. To decrease rate of hemorrhages within the service line.
B. To utilize simulation to hardwire a new Early Blood Loss Intervention (EBI) Policy: Validating RN
understanding and implementation into practice.
C. Utilization of a standardized evaluation tool: Scenario specific to monitor simulation stages to determine
remediation needs as well as for debriefing facilitation priorities.
14Set footer with Insert > Header & Footer

Data Collection Methods
1. Chart review was done pre simulation education on 78 women with PPH January – June 2015 and
compared to 82 women February – August 2016 post simulation education.
2. Patient outcomes pre and post education were compared using data abstracted from the electronic
medical record for objective data collection.
3. Individual paper/electronic post simulation surveys were completed by each participant anonymously for
subjective data collection.

16Set footer with Insert > Header & Footer
Conclusions/Implications to Practice
Multidisciplinary in situ simulation education is an effective tool to identify process improvement opportunities, hardwire early intervention for PPH complication and improve patient outcomes.
17Set footer with Insert > Header & Footer

Discussion/Questions
18Set footer with Insert > Header & Footer
ReferencesDadiz, R., Winschreider, J., Schriefer, J., Arnold, C., Greves, C., Crosby, E., Wang, H., Pressman, E.,
& Guillet, R. (2013). Interdisciplary simulation-based training to improve delivery roomcommunication. Simulation in Healthcare, 8(5) 279-291.
Fialkow, M., Adams, C., Carranza, L., Golden, S., Beneditti, T., & Fernandez, R. (2014). An in situ standardized patient-based simulation to train postpartum hemorrhage and team skillson a labor and delivery unit. Simulation in Healthcare, 9(1) 65-71.
Hansen, S., & Arafeh, J. (2012). Implementing and sustaining in situ drills to improve mulitidisciplinaryhealth care training. Journal of Obstetric Gynecologic and Neonatal Nursing 41, 559-571.
Harvey, E., Wright, A., Taylor, D., Bath, J., & Collier, B. (2013). TeamSTEPPSsimulation-based training: An evidenced –based strategy to improve traumateam performance. The Journal of Continuing Education in Nursing, 44 (11)
484-485.International Nursing Association for Clinical Simulation and Learning. (2013) Standards of best
practice: Simulation Standards I-VII, Clinical Simulation in nursing, 9 (65), S3-S32.Retrieved from http://dx.doi.org/10.1016/j.ecns.2013.04.001
Institute of Medicine. (2003). The future of the public health in the 21st century. NationalAcademics Press, Washington, DC.
19Set footer with Insert > Header & Footer

References (Continued)Marzano, D., Frankel, J., Smith, S., & Andreatta, P. (2011). A simulation-based scenario to help prepare
learners in management of obstetric emergencies. Simulation in Healthcare, 6(6) 364-369.
Rutherford-Hemming, T., Kelsey, N., Grenig, D., Feliciano, M., Simko, L, & Henrich, C. (2016). Multisitesingle-blinded randomized control study of transfer and retention of knowledge and skill between nurses using simulation and online self-study module. Simulation in Healthcare, 11(4) 264-270.
Truijens, S., Banga, F., Fransen, A., Pop, V., Van Runnard Heimel, P. (2015). The effect of multiprofessional simulation-based obstetric team training on patient-reported quality of care.Simulation in Healthcare, 10(4) 210-216.
Walker, D., Cohen, S., Fritz, J., Olvera-Garcia, M., Zelek, S., Fahey, J., Romero-Martinez, M., Montoya-Rodriguez, A., Lamadrid-Frgueroa, H. (2016). Impact evaluation of pronto mexico: A simulation-based program in obstetric and neonatal emergencies and team training. Simulation in healthcare 11(1) 1-9.
20Set footer with Insert > Header & Footer


















