IMPACT OF ECONOMIC
147
IMPACT OF ECONOMIC INCENTIVES ON DIALYSIS PATIENT CARE BRUCE CULLETON, MD CVS KIDNEY CARE
Transcript of IMPACT OF ECONOMIC

Proprietary
IMPACT OF ECONOMIC
INCENTIVES ON
DIALYSIS PATIENT CARE
BRUCE CULLETON, MD
CVS KIDNEY CARE

Proprietary
THREE BASIC
QUESTIONS
¡ Can economic incentives change behavior?
¡ Can economic incentives change behavior within healthcare?
¡ Can economic incentives change behavior within healthcare and improve outcomes? And more specifically within kidney care?

Proprietary
POTENTIAL CONFLICTS OF INTEREST AND DISCLAIMERS
¡ I am an employee of CVH Health
¡ I am not an economist

Proprietary
CAN FINANCIAL INCENTIVES CHANGE HUMAN BEHAVIOR?
¡ Appears to be a very straight forward YES
¡ But, there are considerations and potential complications
¡ Extrinsic incentives (money for example) may ‘crowd out’ intrinsic motivations that are important for long term behavior change (Would you pay your child to read? Would you support paying kids to stay in school?)
¡ Is paying for short-term success enough?
¡ Monetary incentives have two kinds of effects - the standard direct price effect and the indirect psychological effect, which may work in the opposite direction
¡ Communities offered high monetary compensation for a nuclear waste site development (may interpret the high compensation as a signal that the nuclear site will be too high risk)
¡ Research subjects who are offered high compensation to participate in a study

Proprietary
CAN FINANCIAL INCENTIVES CHANGE BEHAVIOR IN HEALTHCARE? PATIENTS / CONSUMERS
¡ Consistent intrinsic and extrinsic paradigms as we just discussed
¡ Higher order cognitions such as beliefs and attitudes may be changed by persuasion and education but less likely by money
¡ Lower order mental processes that trigger a spontaneous response can be changed by economic incentives
¡ For example, it is well established that higher price reduces consumption
¡ Smoking decreases by ~ 5% with every 10% increase in real price of cigarettes (and other ‘sin’ taxes)

Proprietary
Giuffrdia A and Torgerson DJ.
Should we pay the patient? Review of financial incentives to enhance patient compliance. BMJ
1997;315:703-7.

Proprietary
CAN FINANCIAL INCENTIVES CHANGE BEHAVIOR IN HEALTHCARE? PATIENTS / CONSUMERS
¡ In contrast, recent reviews of the evidence of the impact of economic instruments on diet and physical activity and their corollary outcomes (obesity) reveal that the evidence is limited and the results are inconsistent and ambiguous
¡ Consistent themes across the literature:
¡ Opportunity costs of the changed behavior is not the same across income groups, meaning that small incentives may have more of a benefit in low income groups
¡ The context or environment in which choices are provided (or taken) may have more of an impact than large price changes (nudge theory)
¡ Losses loom larger than gains – loss aversion is one of the most robust phenomenon from behavioral economics
¡ Living for today at the expense of tomorrow aka ‘present bias’ – standard (linear) discounting doesn’t apply

Proprietary
THE IMPETUS FOR HEALTH CARE SYSTEM CHANGE
$0
$5
$10
$15
$20
$25
$30
$35
$40
$45
$50
0 1-2 3-4 5+
An
nu
al C
ost
per
Pers
on
(‘1000s)
Number of Chronic Diseases
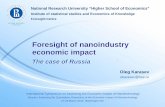
HEALTH CARE COSTS ARE CONCENTRATED AMONG THOSE WITH MULTIPLE CHRONIC DISEASES2
1. Mitchell E. and Machlin S. Concentration of Health Expenditures and Selected Characteristics of High Spenders, U.S. Civilian Noninstitutionalized Population, 2015. Statistical Brief #506. AHRQ, 2017.2. Cohen, SB. The concentration and Persistence in the Level of Health Expenditures for the U.S. Population, 2012-2013. Statistical Brief #481. AHRQ, 2015.
SPENDING ON HEALTH CARE ACCOUNTS FOR ~ 18% OF GDP IN THE U.S.1
FRAGMENTED
EPISODICCOMPLEX
WASTEFUL
HEALTH CARE SYSTEM

Proprietary
CAN FINANCIAL INCENTIVES CHANGE BEHAVIOR IN HEALTHCARE? PHYSICIANS
¡ “That any sane nation, having observed that you could provide for the supply of bread by giving bakers a pecuniary interest in baking for you, should go on to give a surgeon a pecuniary interest in cutting off your leg, is
enough to make one despair…”George Bernard Shaw

Proprietary
CAN FINANCIAL INCENTIVES CHANGE BEHAVIOR IN HEALTHCARE? PHYSICIANS
¡ Accumulating research shows that the effects of financial incentives to physicians improve the delivery of health care are
mixed; where effects are observed, they tend to be modest and short lived.
¡ Barriers to providing better care may lie outside the incentivized physician’s sphere of control.
¡ Small tweaks to payments for physicians are unlikely to fix systemic problems and can cause harm if they mean that other opportunities for change are not addressed.
¡ We need to design payment systems that do not get in the way of better care, and accept that physician payments
alone are not likely to deliver change where it is most needed.
Summary

Proprietary
CAN ACCOUNTABLE CARE ORGANIZATIONS PLAY A ROLE –MOVING RISK TO PHYSICIANS WITHIN A SPHERE OF CONTROL
¡ ACOs are voluntary, primary care–focused alternative payment models that can involve physicians, hospitals, and other health care providers.
¡ The ACO model offers financial incentives for participating entities to invest in care coordination and quality improvement.
¡ Participating providers are eligible to share cost savings when patients incur lower costs than expected.
¡ In two-sided ACOs, providers have the potential to benefit from more shared savings, but must assume financial risk if expenditures exceed expectations.
¡ In 2018, an estimated 10% of the US population was part of an ACO, including roughly 12 million individuals with Medicare.

Proprietary
¡ ACO-type contract with BCBS
Massachusetts
¡ Providers receive shared savings if spending is below a risk-adjusted budget and incur
shared losses if spending exceeds the budget. Providers
are evaluated on the quality of care through 64 measures
N Engl J Med 2019; 381:252-263

Proprietary

Proprietary

Proprietary
THE IMPETUS FOR CHANGE IN KIDNEY CARE
*Compared to the general Medicare population, 66 years and older.
Source: United States Renal Data System. 2018 USRDS annual data report: Epidemiology of kidney disease in the United States. National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD, 2018.
>700K cases of ESRD in the U.S.
¡ Up to 10x higher mortality rates*
>500KAmericans on dialysis
$114BMedicare total cost of care for CKD and ESRD
11hospital days per year
1 in 3readmissions within 30 days
Utilization and Cost
Unmet Clinical Needs

Proprietary
MEDICARE FEE FOR SERVICE SPENDING 2009-2018

Proprietary
NEPHROLOGIST PAYMENT REFORM
¡ In July of 2003, the Centers for Medicare and Medicaid Services (CMS) announced a plan to transform
reimbursement to nephrologists for the delivery of outpatient dialysis care.
¡ At the time, nephrologists received a single monthly payment for providing outpatient dialysis care, regardless of how frequently they visited a patient.
¡ Beginning in 2004, CMS implemented a tiered fee-for-service payment system, where reimbursement varied
according to the number of times per month that a physician (or advanced practitioner) saw a patient.
¡ CMS wrote that the goals of the physician payment reform were to “align incentives,” “encourage increased frequency of face-to-face visits for patients who require it,” and, in doing so, to “improve the quality of care
delivered.”
Kevin F. Erickson and Wolfgang C. Winkelmayer JASN 2018, 29 (12) 2777-2779.

Proprietary
MENTARI EK ET AL. AM J KIDNEY DIS 2005;46:621-627

Proprietary
NEPHROLOGIST PAYMENT REFORM
¡ Nephrologist visits increased from 1.52 at baseline to 3.14 visits per month after reimbursement reform
¡ 9.8% increase in the proportion of patients seen 4 or more times per month
¡ No change in all-cause hospitalization, re-admission rates, or mortality
¡ Increased vascular access procedures
¡ No improvement in patient satisfaction
¡ Sicker patient populations, those living in poorer areas, and those in rural areas were less likely to be seen weekly than those who were healthier and less vulnerable socioeconomically
Kevin F. Erickson and Wolfgang C. Winkelmayer JASN 2018, 29 (12) 2777-2779.Mentari EK et al. Am J Kidney Dis 2005;46:621-627

Proprietary
NEPHROLOGIST PAYMENT REFORM
¡ In 2009, after a review from the American Medical Association’s Relative Value Scale Update Committee, the
temporary “G-codes” reforming the nephrology MCP became permanent…
¡ Despite evidence that more frequent visits did not improve patient health, may have led to an unnecessary expense of time and effort, and may create disincentives to placing patients on home dialysis or to spend needed time for the care of patients with advanced CKD.

Proprietary
BUNDLED PAYMENT REFORM FOR DIALYSIS
¡ The Medicare Improvements for Patients and Providers Act of 2008 required CMS to add injectable medications administered during dialysis to the Composite Rate bundle of dialysis services beginning in 2011.
¡ In its final rule released to the public in 2010, CMS summarizes three primary objectives of this policy:
¡ (1) reduce the overuse of profitable separately billable drugs, particularly erythropoietin (EPO);
¡ (2) through flexibility offered, increase desirable outcomes and enhance the quality of care; and
¡ (3) target payment to facilities with more costly patients in order to promote equitable payment and access to services.

Proprietary
Reduced proportion of
patients receiving
epoetin alfa (EPO),
reduced EPO doses,
reduced hemoglobin
concentrations just
preceding and after
regulatory changes,
and subsequent
increase in use of
transfusion.
Glenn M. Chertow et al. JASN 2016;27:3129-3138
©2016 by American Society of Nephrology
% of EPO users
EPO Dose
Hb Level
Transfusion rate

Proprietary
BUNDLED PAYMENT REFORM FOR DIALYSIS
¡ No increase in all-cause mortality, CV mortality or MI
¡ May have been a decrease in stroke, heart failure, and thrombosis
¡ Impact on patient QOL is unknown
Glenn M. Chertow et al. JASN 2016;27:3129-3138

Proprietary
CEC (ESCO MODELS OF CARE)
¡ The CEC Model is designed to create incentives for dialysis facilities and nephrologists to coordinate care for
Medicare beneficiaries with ESRD across settings by making the ESCO responsible – financially and clinically –for care delivered in other inpatient and outpatient settings.

Proprietary
CEC
https://innovation.cms.gov/Files/re
ports/cec-annrpt-py2.pdf

Proprietary
CEC 2-YEAR
RESULTS
https://innovation.cms.gov/Files/r
eports/cec-annrpt-py2.pdf

Proprietary
CEC
¡ Unlike the ESRD PPS, which applies to all Medicare fee-for-service beneficiaries, many of the newer value-based payment initiatives are more limited in scope.
¡ Although early evaluations suggest the CEC model led to fewer hospitalizations in its first 2 years, only 12% of dialysis facilities participated in the model.
¡ Other methods of introducing value-based payment into dialysis care are, therefore, necessary.
https://innovation.cms.gov/Files/reports/cec-annrpt-py2.pdf

Proprietary
Shivani Bakre et al. CJASN 2020;15:1777-1784
©2020 by American Society of Nephrology

Proprietary
https://innovation.cms.gov/Fi
les/reports/cec-annrpt-
py2.pdf

Proprietary
ACCOUNTABLE CARE ORGANIZATIONS
¡ To achieve similar success in long-term dialysis, health care providers participating in ACOs will need to identify
ways to incorporate dialysis care in their broader chronic-care management programs.
¡ Because ACOs care for many patients with advanced CKD, they are uniquely well positioned to reduce dialysis costs by optimizing advanced CKD care.

Proprietary
CMS INITIATIVES TO LOWER COST AND IMPROVE CARE IN KIDNEY DISEASE
¡ In 2004, the Centers for Medicare and Medicaid Services (CMS) changed reimbursement to nephrologists for the delivery of outpatient dialysis care.
¡ In 2011, the ESRD Prospective Payment System (PPS) was expanded to incorporate injectable medications into bundled dialysis payments in an effort to reduce the high costs of these medications.
¡ In 2015, Centers for Medicare and Medicaid Services implemented the Comprehensive ESRD Care (CEC) model to encourage dialysis clinics, nephrologists, and other care providers to deliver high-value, coordinated care, by offering shared savings from judicious use of resources.
¡ In 2019, the Advancing American Kidney Health (AAKH) initiative called for five new nephrology-specific alternative payment models that include incentives to delay the onset of dialysis and encourage home dialysis and kidney transplantation.
¡ In 2021, Medicare beneficiaries with kidney failure requiring dialysis or transplantation will have the option to enroll in Medicare Advantage plans.

Proprietary
TODAY’S CARE MODEL
¡ Value-based models become slightly more common, but economic value is predominantly created by FFS
model which continues to drive provider, payor, and patient behavior.
¡ Patient experience still falls short because of a lack of focus on the patient as the user and lack of reimbursement around VAS.
¡ The industry focuses on reducing costs and enabling providers to deliver better care by working to aggregate and segment large patient populations, redistributing tasks to social workers/care techs., introducing new technology to streamline administrative tasks, and scaling telehealth. Some new innovations emerge, but there is a lack of massive disruption in the form of scalable, integrated solutions.
VBC
FFS
PatientProvider

Proprietary
TOMORROW’S CARE MODEL
¡ Economic value is predominantly created through risk-based models due to new regulation around
reimbursement that incentivizes prevention and proactive disease management.
¡ Nephrologists are more likely to recommend and support alternative sites for of care because of better outcomes and lower costs.
¡ Nephrologists are increasingly working in interdisciplinary care teams to deliver better outcomes.
Innovation in delivering advanced, cost-effective diagnostics for screening purposes, precision medicine is advancing, and new entrants are delivering data sharing and technology products and services to enable providers to make better, faster decisions and minimize time spend on administrative tasks.
VBC
FFS
PatientProvider

Proprietary
ALTHOUGH TODAY’S WORLD IS LARGELY FOCUSED IN THE BOTTOM LEFT
QUADRANT, INCENTIVES WILL SHIFT CARE UP AND TO THE RIGHT
Predominantly
Value-based Care
Predominantly
Fee-for-Service
Patient as
Prioritized End
User
Provider as
Prioritized
End User
Represents most of the current state
moves in the industry
Value-based care models focused on
provider engagement
Concierge care through premium services designed
for the patient as the prioritized user
Equitable consumer based holistic care

Proprietary
THREE BASIC
QUESTIONS
(ANSWERED, I HOPE)
¡ Can economic incentives change behavior?
¡ Can economic incentives change behavior within healthcare?
¡ Can economic incentives change behavior within healthcare and improve outcomes? And more specifically within kidney care?

Lester Health Law PLLC1
Lester
Health
Law PLLC
The Homer Building
Eleventh Floor South
601 Thirteenth Street NW
Washington, DC 20005
202-903-6627
Economic Evaluation of Dialysis
Therapies: Real and Hidden Costs
Kathy Lester, JD, MPH
Lester Health Law, PLLC

Lester Health Law PLLC2
Understanding the Cost of Services Requires
Understanding the Medicare ESRD PPS
Source: MedPAC, “Payment Basics: Outpatient Dialysis Services Payment System (2020)
Medicare coverage
~395,000 patients
under the ESRD PPS
Labor costs remain
a substantial part of
the cost of providing
services

Lester Health Law PLLC3
Under the ESRD PPS, Medicare Rates Have
Not Covered the Cost of Providing Care
-1.10%
0.40%
-0.40%
2.40%**
-1.10%
-2.00%*
0.50%*
-2.50%
-2.00%
-1.50%
-1.00%
-0.50%
0.00%
0.50%
1.00%
1.50%
2.00%
2.50%
3.00%
Projected Margin Actual Margin
2017 2018 2019 2020
Source: MedPAC, Report to the Congress (2015-2020).
* Without TDAPA included
** After new dollars added
for calcimimetics

Lester Health Law PLLC4
Most ESRD Patients Are < 64 Years Old and Lost
Kidney Function because of Diabetes or Hypertension
1%
14%
43%
25%
17% 0-21
22-44
45-64
65-74
75+
Percentage of Incident Patients
by Age (2017)
38%
26%
15%
5%
2%
9%
3%
2%
Diabetes
Hypertension
Glomerulonephritis
Cystic kidney
Other urologic
Other cause
Unknown cause
Missing cause
Percentage of Incident Patients by
Cause of Kidney Failure (2017)
Lack of CKD management prior to kidney failure leaves patients unprepared,
forcing them often into in-center dialysis, and reducing transplant options;
also increase the cost of the initial period of dialysis treatment.
Source: USRDS, Annual Data Report (2019).

Lester Health Law PLLC5
TDAPA Provides Temporary Dollars;
Adjustment Needed for Long-Term Sustainability
Functional Categories:
• Access Management,
• Anemia Management,
• Bone and Mineral Metabolism,
• Cellular Management,
• Antiemetic,
• Anti-infective,
• Antipruritic,
• Anxiolytic,
• Excess Fluid Management,
• Fluid and Electrolyte Management
Including Volume Expanders, and
• Pain Management
• Based on CMS data the
functional categories, other
than anemia management,
only ~$3.00 of the base rate
is linked to the cost of
providing drugs/biologicals
• The cost of any new
product, especially a break-
through or truly innovative
product, cannot be
absorbed into the system
Likely to experience similar problem with
truly innovative devices

Lester Health Law PLLC6
ESRD PPS and Other Regulations Do Not Support Care Coordination, Where Savings Lie
• According to a Lewin Report published by CMS, the CEC Model produced a statistically significant savings of $114 per beneficiary per month.
• Given the $45 treatments billed to Medicare in 2016, Medicare may be able to save nearly $400M per year through better coordination of care for dialysis patients
6
A variety of fraud and abuse rules severely limit or prohibit the ability of providers to
communicate and coordinate care.
The Lewin Group, “Comprehensive End-Stage Renal Disease Care (CEC)
Model: Performance Year 2 Evaluation (Sept. 2019)

Lester Health Law PLLC7
Reason to Hope
• Both political parties recognize that patients with kidney disease deserve better
• Need to translate this sentiment into concrete reforms– Address kidney disease earlier to slow onset of kidney
failure
– Establish a sustainable PPS that rewards innovation and correctly reimburses the cost of care
– Eliminate regulatory and organizational silos that block coordination
– Implement policies that truly reward Part B care when it reduces Part A expenditures

Medicare Payment Changes to
Support Increased Home Dialysis
Eugene Lin, MD, MS, FASN
Assistant Professor of Medicine and of Health Policy & Management
@eugelin06
3/7/2021

Disclosures
NIH / NIDDK
Acumen, LLC
ASN Quality Committee
NKF Scientific Advisory Board

Objectives
Pre-2021 Payment for Home Dialysis
End-Stage Renal Disease Treatment Choices Model (ETC)
Voluntary Kidney Models
Opportunities for Providers

Dialysis Reimbursement pre-2021
• Facility Payments
• Bundled (Prospective Payment System)
• $239 / HD treatment * Multipliers
• HD and PD are equivalent / week
• Limited to 3 HD treatments / week
• Nephrologist Payments
• In-center: $205-363 / month
• Home: $300 / month

Prior to 2008, home dialysis was declining
Lin E, et al. J Am Soc Nephrol. 2017; 28(10): 2993-3004

Home dialysis increased after PPS announced
Lin E, et al. J Am Soc Nephrol. 2017; 28(10): 2993-3004

But nephrologists are still rewarded for center-based dialysis• Home Dialysis
• $243 per month
• Patients seen one at a time
• Joint ventures / Medical directorships
• Harder to scale
• In-center dialysis
• $205-363 per month…
• … most providers make $363
• Patients seen in a shift
• Joint ventures / Medical directorships
• Easier to run a large center-based facility at scale

Center-based dialysis margins are still highest
US GAO, 2015. https://www.gao.gov/products/gao-16-125


• CMS mandatory model for 30% of Hospital Referral Regions (HRRs)
• Participants:
• Outpatient dialysis facilities
• Nephrologists billing a monthly capitation payment
ESRD Treatment Choices Model
ETC Final Rule

All HRRs

HRRs Participating in the ETC

• Performance is aggregated at the HRR level:
• Facilities owned by the same chain within an HRR
• Practices with multiple nephrologists within an HRR
• Preserves the ability for chains / practices to specialize
Providers within an HRR are aggregated

• A Home Dialysis Payment Adjustment will include bonuses for all home dialysis claims (facility and physician)
• 2021: 3%
• 2022: 2%
• 2023: 1%
CMS has provided a short “runway”
MCP Pre-2021 2021 2022 2023
Home Dialysis $300 $309 $306 $303
iHD: 4x/month $363 $363 $363 $363
iHD: 2-3x/month $300 $300 $300 $300
iHD: 1x/month $206 $206 $206 $206

Margins Pre-2021 2021 2022 2023
iHD 15% 15% 15% 15%
PD 8% 11% 10% 9%
Home HD -4% -1% -2% -3%
The runway might be relevant for facilities?
(Extrapolated from GAO data)

• 4 points for “home dialysis”
•!"#$#"%&'()
!
"∗+,-./.&0 ($/+ -,1$ #"%&'(
&"&,/ 2.,/0(.( #"%&'(
• NO risk adjustment
• 2 points for “kidney transplant”
•3,.&/.(& #"%&'()/.4.%5 2"%"1 &1,%(6/,%& #"%&'(
&"&,/ 2.,/0(.( #"%&'(
• Adjusted for age-bands (18-55, 56-70, 71-74 years)
The real financial motivation behind the ETC

Payment adjustments are large
Score Performance Payment Adjustment Period
Jul ‘22–Jun ‘23 Jul ‘23–Jun ‘24 Jul ‘24–Jun ‘25 Jul ‘25–Jun ‘26 Jul ‘26–Jun ‘27
5.5 - 6 +4% +5% +6% +7% +8%
4 - 5 +2% +2.5% +3% +3.5% +4%
2.5 - 3.5 0% 0% 0% 0% 0%
1 - 2 -2.5% -3% -3.5% -4.5 / -4% -5 / -4.5%
0 - .5 -5% -6% -7% -9 / -8% -10 / -9%

ETC Benchmarks
# of Points Received 1 2 3 4
Total Points 0-0.5 1-2 2.5-3.5 4-5 5.5-6
Adjustment -5% -2.5% 0% +2% +4%

• Let’s show some counterfactual scenarios
• In all scenarios, assume that the transplant rate is fixed, and this facility / nephrologist is getting 1 point (50th percentile)
To make this more concrete
Home Dialysis Uptake Home Points Percentile Total Points Adjustment
3% 0 < 30% 1 -5%
7% 1 30-50% 2 -2.5%
12% 2 50-75% 3 0%
20% 3 75-90% 4 +2%
30% 4 > 90% 5 +4%

• Assumptions:
• All home dialysis uptake is PD
• Margins calculated using GAO estimates
Change in Facility Margins
Home
Dialysis
Uptake
Adjustment Cost
3% -5% $208
7% -3% $209
12% 0% $209
20% 2% $211
30% 4% $212

• Assumptions:
• All home dialysis uptake is PD
• Margins calculated using GAO estimates
Change in Facility Margins (per treatment)
Home
Dialysis
Uptake
Adjustment Cost
Revenue
without
ETC
Margin
without
ETC
3% -5% $208 $239 15%
7% -3% $209 $239 14%
12% 0% $209 $239 14%
20% 2% $211 $239 14%
30% 4% $212 $239 13%

• Assumptions:
• All home dialysis uptake is PD
• Margins calculated using GAO estimates
Change in Facility Margins
Home
Dialysis
Uptake
Adjustment Cost
Revenue
without
ETC
Margin
without
ETC
Revenue
with ETC
Margin
with ETC
3% -5% $208 $239 15% $227 9%
7% -3% $209 $239 14% $233 12%
12% 0% $209 $239 14% $239 14%
20% 2% $211 $239 14% $244 16%
30% 4% $212 $239 13% $249 17%

• Assume all home dialysis uptake is PD
Change in Nephrologist Revenue (per tx)
Home
Dialysis
Uptake
Adjustment 100% of iHD is 4x/month
Without ETC With ETC
3% -5% $361 $343
7% -3% $359 $350
12% 0% $355 $355
20% 2% $350 $357
30% 4% $344 $358

• Assume all home dialysis uptake is PD
Change in Nephrologist Revenue (per tx)
Home
Dialysis
Uptake
Adjustment 100% of iHD is 4x/month 50% of iHD is 4x/month
Without ETC With ETC Without ETC With ETC
3% -5% $361 $343 $331 $314
7% -3% $359 $350 $329 $321
12% 0% $355 $355 $328 $328
20% 2% $350 $357 $325 $332
30% 4% $344 $358 $322 $335

• I’m going to give a high-level summary here because the economics are not as clear
• In general, these models reward:
• High-quality care
• Low-cost care
• Emphasis on CKD 4, CKD 5, and ESRD
Voluntary Models (Kidney Care Choices)

Two main options for participation
Risk Track Eligible Participants Upside Risk Downside Risk
Kidney Care First (KCF) Nephrologists only Up to 30% bonus Up to 20% penalty
Comprehensive Kidney Care Contracting Models (CKCC)
Graduated Level 1 *Nephrologists †
Transplant †
Dialysis Organizations §
Other Providers
40% -
Graduated Level 2 * 50% 30%
Professional 50% 50%
Global 100% 100%
https://innovation.cms.gov/Files/x/kcc-rfa.pdf

KCF Option
* Red text denotes bottom 50% of KCF Practices
Performance Level Adjustment
Top 25% of KCF Practices +10%
25-50% of KCF Practices +2%
Top 50% of NATIONAL Practices 0%
51-75% of NATIONAL Practices -6%
Bottom 25% of NATIONAL Practices -20%
Did not pass quality gateway -20%

CKCC Option
Shared Losses
Benchmark based on historical expenditures
$
Performance year
expenditures
$
Shared Savings
Benchmark based on historical expenditures
$
Performance year
expenditures
$KCE and CMS share in savings
KCE and CMS share in losses

Does home dialysis save money?
USRDS ADR, 2020

Does home dialysis save money?
Outcome HD PD Difference
Mortality (12 month) 8.1% 7.2% -0.9%
(7.8%, 8.4%) (5.2%, 8.8%) (-3.3%, 0.8%)
# Hospitalizations /
Patient (Months 7-12)0.71 0.66 -0.05
(0.69, 0.72) (0.52, 0.77) (-0.20, 0.07)
Total Spending ($) /
Patient (Months 7-12)$14,208 $13,506 -$702
($13,838, $14,932) ($10,987, $16,906) (-$4,004, $2,909)
Analysis of USRDS data, manuscript under review

• Determine how many patients must transition to home dialysis to move up a performance tier (and whether this is realistic)
• Aggressively identify opportunities to graduate into home dialysis
• Age out in-center HD capital equipment faster
• Identify space that can be converted into a home dialysis space
• Recognize that the ETC is a PRE-ESRD program
Strategies for Success (if in the ETC)

Early Education is Key
0%
5%
10%
15%
1 2 3 4 5 6 7 8 9 10 11 12
Pro
babili
ty o
f S
witchin
g f
rom
HD
to P
D
Month of Dialysis
Uninsured Medicaid
B
Lin E, et al. 2021. Med Care. 2020;58(7):632-642.

• PD may be easier to scale initially, given larger margins.
• Successful home HD programs often require economies of scale
• However, some evidence suggests it is easier to transition patients on in-center HD to home HD rather than PD
Strategies for Success (if in the ETC), cont’d

Questions?

• 1. Lin E, Cheng XS, Chin K-K, et al. Home Dialysis in the Prospective Payment System Era. Journal of the American Society of Nephrology. 2017;28(10):2993-3004. doi:10.1681/ASN.2017010041• 2. United States Government Accountability Office. End-Stage Renal Disease: Medicare Payment Refinements Could Promote Increased Use of Home Dialysis. Report to the Subcommittee on Health, Committee on Ways and Means, House of Representatives. GAO-16-125. Published October 2015. Accessed June 19, 2019. https://www.gao.gov/assets/680/673140.pdf• 3. Centers for Medicare and Medicaid Services (CMS), HHS. Medicare Program; Specialty Care Models To Improve Quality of Care and Reduce Expenditures. CMS-5527-F. Federal Register. 2020;85(189):61114-61381.• 4. Centers for Medicare & Medicaid Services. Kidney Care Choices (KCC) Model: Request for Applications (RFA). Published October 10, 2019. Accessed February 7, 2020. https://innovation.cms.gov/Files/x/kcc-rfa.pdf• 5. United States Renal Data System. 2020 USRDS Annual Data Report: Epidemiology of Kidney Disease in the United States. National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases; 2020. Accessed February 3, 2021. https://adr.usrds.org/2020• 6. Lin E, Chertow GM, Bhattacharya J, Lakdawalla D. Early Delays in Insurance Coverage and Long-term Use of Home-based Peritoneal Dialysis. Med Care. 2020;58(7):632-642. doi:10.1097/MLR.0000000000001350
References

Medicare Payment Changes to
Support Increased Home Dialysis
Eugene Lin, MD, MS, FASN
Assistant Professor of Medicine and of Health Policy & Management
@eugelin06
3/7/2021

Disclosures
NIH / NIDDK
Acumen, LLC
ASN Quality Committee
NKF Scientific Advisory Board

Objectives
Pre-2021 Payment for Home Dialysis
End-Stage Renal Disease Treatment Choices Model (ETC)
Voluntary Kidney Models
Opportunities for Providers

Dialysis Reimbursement pre-2021
• Facility Payments
• Bundled (Prospective Payment System)
• $239 / HD treatment * Multipliers
• HD and PD are equivalent / week
• Limited to 3 HD treatments / week
• Nephrologist Payments
• In-center: $205-363 / month
• Home: $300 / month

Prior to 2008, home dialysis was declining
Lin E, et al. J Am Soc Nephrol. 2017; 28(10): 2993-3004

Home dialysis increased after PPS announced
Lin E, et al. J Am Soc Nephrol. 2017; 28(10): 2993-3004

But nephrologists are still rewarded for center-based dialysis• Home Dialysis
• $243 per month
• Patients seen one at a time
• Joint ventures / Medical directorships
• Harder to scale
• In-center dialysis
• $205-363 per month…
• … most providers make $363
• Patients seen in a shift
• Joint ventures / Medical directorships
• Easier to run a large center-based facility at scale

Center-based dialysis margins are still highest
US GAO, 2015. https://www.gao.gov/products/gao-16-125


• CMS mandatory model for 30% of Hospital Referral Regions (HRRs)
• Participants:
• Outpatient dialysis facilities
• Nephrologists billing a monthly capitation payment
ESRD Treatment Choices Model
ETC Final Rule

All HRRs

HRRs Participating in the ETC

• Performance is aggregated at the HRR level:
• Facilities owned by the same chain within an HRR
• Practices with multiple nephrologists within an HRR
• Preserves the ability for chains / practices to specialize
Providers within an HRR are aggregated

• A Home Dialysis Payment Adjustment will include bonuses for all home dialysis claims (facility and physician)
• 2021: 3%
• 2022: 2%
• 2023: 1%
CMS has provided a short “runway”
MCP Pre-2021 2021 2022 2023
Home Dialysis $300 $309 $306 $303
iHD: 4x/month $363 $363 $363 $363
iHD: 2-3x/month $300 $300 $300 $300
iHD: 1x/month $206 $206 $206 $206

Margins Pre-2021 2021 2022 2023
iHD 15% 15% 15% 15%
PD 8% 11% 10% 9%
Home HD -4% -1% -2% -3%
The runway might be relevant for facilities?
(Extrapolated from GAO data)

• 4 points for “home dialysis”
•!"#$#"%&'()
!
"∗+,-./.&0 ($/+ -,1$ #"%&'(
&"&,/ 2.,/0(.( #"%&'(
• NO risk adjustment
• 2 points for “kidney transplant”
•3,.&/.(& #"%&'()/.4.%5 2"%"1 &1,%(6/,%& #"%&'(
&"&,/ 2.,/0(.( #"%&'(
• Adjusted for age-bands (18-55, 56-70, 71-74 years)
The real financial motivation behind the ETC

Payment adjustments are large
Score Performance Payment Adjustment Period
Jul ‘22–Jun ‘23 Jul ‘23–Jun ‘24 Jul ‘24–Jun ‘25 Jul ‘25–Jun ‘26 Jul ‘26–Jun ‘27
5.5 - 6 +4% +5% +6% +7% +8%
4 - 5 +2% +2.5% +3% +3.5% +4%
2.5 - 3.5 0% 0% 0% 0% 0%
1 - 2 -2.5% -3% -3.5% -4.5 / -4% -5 / -4.5%
0 - .5 -5% -6% -7% -9 / -8% -10 / -9%

ETC Benchmarks
# of Points Received 1 2 3 4
Total Points 0-0.5 1-2 2.5-3.5 4-5 5.5-6
Adjustment -5% -2.5% 0% +2% +4%

• Let’s show some counterfactual scenarios
• In all scenarios, assume that the transplant rate is fixed, and this facility / nephrologist is getting 1 point (50th percentile)
To make this more concrete
Home Dialysis Uptake Home Points Percentile Total Points Adjustment
3% 0 < 30% 1 -5%
7% 1 30-50% 2 -2.5%
12% 2 50-75% 3 0%
20% 3 75-90% 4 +2%
30% 4 > 90% 5 +4%

• Assumptions:
• All home dialysis uptake is PD
• Margins calculated using GAO estimates
Change in Facility Margins
Home
Dialysis
Uptake
Adjustment Cost
3% -5% $208
7% -3% $209
12% 0% $209
20% 2% $211
30% 4% $212

• Assumptions:
• All home dialysis uptake is PD
• Margins calculated using GAO estimates
Change in Facility Margins (per treatment)
Home
Dialysis
Uptake
Adjustment Cost
Revenue
without
ETC
Margin
without
ETC
3% -5% $208 $239 15%
7% -3% $209 $239 14%
12% 0% $209 $239 14%
20% 2% $211 $239 14%
30% 4% $212 $239 13%

• Assumptions:
• All home dialysis uptake is PD
• Margins calculated using GAO estimates
Change in Facility Margins
Home
Dialysis
Uptake
Adjustment Cost
Revenue
without
ETC
Margin
without
ETC
Revenue
with ETC
Margin
with ETC
3% -5% $208 $239 15% $227 9%
7% -3% $209 $239 14% $233 12%
12% 0% $209 $239 14% $239 14%
20% 2% $211 $239 14% $244 16%
30% 4% $212 $239 13% $249 17%

• Assume all home dialysis uptake is PD
Change in Nephrologist Revenue (per tx)
Home
Dialysis
Uptake
Adjustment 100% of iHD is 4x/month
Without ETC With ETC
3% -5% $361 $343
7% -3% $359 $350
12% 0% $355 $355
20% 2% $350 $357
30% 4% $344 $358

• Assume all home dialysis uptake is PD
Change in Nephrologist Revenue (per tx)
Home
Dialysis
Uptake
Adjustment 100% of iHD is 4x/month 50% of iHD is 4x/month
Without ETC With ETC Without ETC With ETC
3% -5% $361 $343 $331 $314
7% -3% $359 $350 $329 $321
12% 0% $355 $355 $328 $328
20% 2% $350 $357 $325 $332
30% 4% $344 $358 $322 $335

• I’m going to give a high-level summary here because the economics are not as clear
• In general, these models reward:
• High-quality care
• Low-cost care
• Emphasis on CKD 4, CKD 5, and ESRD
Voluntary Models (Kidney Care Choices)

Two main options for participation
Risk Track Eligible Participants Upside Risk Downside Risk
Kidney Care First (KCF) Nephrologists only Up to 30% bonus Up to 20% penalty
Comprehensive Kidney Care Contracting Models (CKCC)
Graduated Level 1 *Nephrologists †
Transplant †
Dialysis Organizations §
Other Providers
40% -
Graduated Level 2 * 50% 30%
Professional 50% 50%
Global 100% 100%
https://innovation.cms.gov/Files/x/kcc-rfa.pdf

KCF Option
* Red text denotes bottom 50% of KCF Practices
Performance Level Adjustment
Top 25% of KCF Practices +10%
25-50% of KCF Practices +2%
Top 50% of NATIONAL Practices 0%
51-75% of NATIONAL Practices -6%
Bottom 25% of NATIONAL Practices -20%
Did not pass quality gateway -20%

CKCC Option
Shared Losses
Benchmark based on historical expenditures
$
Performance year
expenditures
$
Shared Savings
Benchmark based on historical expenditures
$
Performance year
expenditures
$KCE and CMS share in savings
KCE and CMS share in losses

Does home dialysis save money?
USRDS ADR, 2020

Does home dialysis save money?
Outcome HD PD Difference
Mortality (12 month) 8.1% 7.2% -0.9%
(7.8%, 8.4%) (5.2%, 8.8%) (-3.3%, 0.8%)
# Hospitalizations /
Patient (Months 7-12)0.71 0.66 -0.05
(0.69, 0.72) (0.52, 0.77) (-0.20, 0.07)
Total Spending ($) /
Patient (Months 7-12)$14,208 $13,506 -$702
($13,838, $14,932) ($10,987, $16,906) (-$4,004, $2,909)
Analysis of USRDS data, manuscript under review

• Determine how many patients must transition to home dialysis to move up a performance tier (and whether this is realistic)
• Aggressively identify opportunities to graduate into home dialysis
• Age out in-center HD capital equipment faster
• Identify space that can be converted into a home dialysis space
• Recognize that the ETC is a PRE-ESRD program
Strategies for Success (if in the ETC)

Early Education is Key
0%
5%
10%
15%
1 2 3 4 5 6 7 8 9 10 11 12
Pro
babili
ty o
f S
witchin
g f
rom
HD
to P
D
Month of Dialysis
Uninsured Medicaid
B
Lin E, et al. 2021. Med Care. 2020;58(7):632-642.

• PD may be easier to scale initially, given larger margins.
• Successful home HD programs often require economies of scale
• However, some evidence suggests it is easier to transition patients on in-center HD to home HD rather than PD
Strategies for Success (if in the ETC), cont’d

Questions?

• 1. Lin E, Cheng XS, Chin K-K, et al. Home Dialysis in the Prospective Payment System Era. Journal of the American Society of Nephrology. 2017;28(10):2993-3004. doi:10.1681/ASN.2017010041• 2. United States Government Accountability Office. End-Stage Renal Disease: Medicare Payment Refinements Could Promote Increased Use of Home Dialysis. Report to the Subcommittee on Health, Committee on Ways and Means, House of Representatives. GAO-16-125. Published October 2015. Accessed June 19, 2019. https://www.gao.gov/assets/680/673140.pdf• 3. Centers for Medicare and Medicaid Services (CMS), HHS. Medicare Program; Specialty Care Models To Improve Quality of Care and Reduce Expenditures. CMS-5527-F. Federal Register. 2020;85(189):61114-61381.• 4. Centers for Medicare & Medicaid Services. Kidney Care Choices (KCC) Model: Request for Applications (RFA). Published October 10, 2019. Accessed February 7, 2020. https://innovation.cms.gov/Files/x/kcc-rfa.pdf• 5. United States Renal Data System. 2020 USRDS Annual Data Report: Epidemiology of Kidney Disease in the United States. National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases; 2020. Accessed February 3, 2021. https://adr.usrds.org/2020• 6. Lin E, Chertow GM, Bhattacharya J, Lakdawalla D. Early Delays in Insurance Coverage and Long-term Use of Home-based Peritoneal Dialysis. Med Care. 2020;58(7):632-642. doi:10.1097/MLR.0000000000001350
References

Medicare Payment Changes to
Support Increased Home Dialysis
Eugene Lin, MD, MS, FASN
Assistant Professor of Medicine and of Health Policy & Management
@eugelin06
3/7/2021

Disclosures
NIH / NIDDK
Acumen, LLC
ASN Quality Committee
NKF Scientific Advisory Board

Objectives
Pre-2021 Payment for Home Dialysis
End-Stage Renal Disease Treatment Choices Model (ETC)
Voluntary Kidney Models
Opportunities for Providers

Dialysis Reimbursement pre-2021
• Facility Payments
• Bundled (Prospective Payment System)
• $239 / HD treatment * Multipliers
• HD and PD are equivalent / week
• Limited to 3 HD treatments / week
• Nephrologist Payments
• In-center: $205-363 / month
• Home: $300 / month

Prior to 2008, home dialysis was declining
Lin E, et al. J Am Soc Nephrol. 2017; 28(10): 2993-3004

Home dialysis increased after PPS announced
Lin E, et al. J Am Soc Nephrol. 2017; 28(10): 2993-3004

But nephrologists are still rewarded for center-based dialysis• Home Dialysis
• $243 per month
• Patients seen one at a time
• Joint ventures / Medical directorships
• Harder to scale
• In-center dialysis
• $205-363 per month…
• … most providers make $363
• Patients seen in a shift
• Joint ventures / Medical directorships
• Easier to run a large center-based facility at scale

Center-based dialysis margins are still highest
US GAO, 2015. https://www.gao.gov/products/gao-16-125


• CMS mandatory model for 30% of Hospital Referral Regions (HRRs)
• Participants:
• Outpatient dialysis facilities
• Nephrologists billing a monthly capitation payment
ESRD Treatment Choices Model
ETC Final Rule

All HRRs

HRRs Participating in the ETC

• Performance is aggregated at the HRR level:
• Facilities owned by the same chain within an HRR
• Practices with multiple nephrologists within an HRR
• Preserves the ability for chains / practices to specialize
Providers within an HRR are aggregated

• A Home Dialysis Payment Adjustment will include bonuses for all home dialysis claims (facility and physician)
• 2021: 3%
• 2022: 2%
• 2023: 1%
CMS has provided a short “runway”
MCP Pre-2021 2021 2022 2023
Home Dialysis $300 $309 $306 $303
iHD: 4x/month $363 $363 $363 $363
iHD: 2-3x/month $300 $300 $300 $300
iHD: 1x/month $206 $206 $206 $206

Margins Pre-2021 2021 2022 2023
iHD 15% 15% 15% 15%
PD 8% 11% 10% 9%
Home HD -4% -1% -2% -3%
The runway might be relevant for facilities?
(Extrapolated from GAO data)

• 4 points for “home dialysis”
•!"#$#"%&'()
!
"∗+,-./.&0 ($/+ -,1$ #"%&'(
&"&,/ 2.,/0(.( #"%&'(
• NO risk adjustment
• 2 points for “kidney transplant”
•3,.&/.(& #"%&'()/.4.%5 2"%"1 &1,%(6/,%& #"%&'(
&"&,/ 2.,/0(.( #"%&'(
• Adjusted for age-bands (18-55, 56-70, 71-74 years)
The real financial motivation behind the ETC

Payment adjustments are large
Score Performance Payment Adjustment Period
Jul ‘22–Jun ‘23 Jul ‘23–Jun ‘24 Jul ‘24–Jun ‘25 Jul ‘25–Jun ‘26 Jul ‘26–Jun ‘27
5.5 - 6 +4% +5% +6% +7% +8%
4 - 5 +2% +2.5% +3% +3.5% +4%
2.5 - 3.5 0% 0% 0% 0% 0%
1 - 2 -2.5% -3% -3.5% -4.5 / -4% -5 / -4.5%
0 - .5 -5% -6% -7% -9 / -8% -10 / -9%

ETC Benchmarks
# of Points Received 1 2 3 4
Total Points 0-0.5 1-2 2.5-3.5 4-5 5.5-6
Adjustment -5% -2.5% 0% +2% +4%

• Let’s show some counterfactual scenarios
• In all scenarios, assume that the transplant rate is fixed, and this facility / nephrologist is getting 1 point (50th percentile)
To make this more concrete
Home Dialysis Uptake Home Points Percentile Total Points Adjustment
3% 0 < 30% 1 -5%
7% 1 30-50% 2 -2.5%
12% 2 50-75% 3 0%
20% 3 75-90% 4 +2%
30% 4 > 90% 5 +4%

• Assumptions:
• All home dialysis uptake is PD
• Margins calculated using GAO estimates
Change in Facility Margins
Home
Dialysis
Uptake
Adjustment Cost
3% -5% $208
7% -3% $209
12% 0% $209
20% 2% $211
30% 4% $212

• Assumptions:
• All home dialysis uptake is PD
• Margins calculated using GAO estimates
Change in Facility Margins (per treatment)
Home
Dialysis
Uptake
Adjustment Cost
Revenue
without
ETC
Margin
without
ETC
3% -5% $208 $239 15%
7% -3% $209 $239 14%
12% 0% $209 $239 14%
20% 2% $211 $239 14%
30% 4% $212 $239 13%

• Assumptions:
• All home dialysis uptake is PD
• Margins calculated using GAO estimates
Change in Facility Margins
Home
Dialysis
Uptake
Adjustment Cost
Revenue
without
ETC
Margin
without
ETC
Revenue
with ETC
Margin
with ETC
3% -5% $208 $239 15% $227 9%
7% -3% $209 $239 14% $233 12%
12% 0% $209 $239 14% $239 14%
20% 2% $211 $239 14% $244 16%
30% 4% $212 $239 13% $249 17%

• Assume all home dialysis uptake is PD
Change in Nephrologist Revenue (per tx)
Home
Dialysis
Uptake
Adjustment 100% of iHD is 4x/month
Without ETC With ETC
3% -5% $361 $343
7% -3% $359 $350
12% 0% $355 $355
20% 2% $350 $357
30% 4% $344 $358

• Assume all home dialysis uptake is PD
Change in Nephrologist Revenue (per tx)
Home
Dialysis
Uptake
Adjustment 100% of iHD is 4x/month 50% of iHD is 4x/month
Without ETC With ETC Without ETC With ETC
3% -5% $361 $343 $331 $314
7% -3% $359 $350 $329 $321
12% 0% $355 $355 $328 $328
20% 2% $350 $357 $325 $332
30% 4% $344 $358 $322 $335

• I’m going to give a high-level summary here because the economics are not as clear
• In general, these models reward:
• High-quality care
• Low-cost care
• Emphasis on CKD 4, CKD 5, and ESRD
Voluntary Models (Kidney Care Choices)

Two main options for participation
Risk Track Eligible Participants Upside Risk Downside Risk
Kidney Care First (KCF) Nephrologists only Up to 30% bonus Up to 20% penalty
Comprehensive Kidney Care Contracting Models (CKCC)
Graduated Level 1 *Nephrologists †
Transplant †
Dialysis Organizations §
Other Providers
40% -
Graduated Level 2 * 50% 30%
Professional 50% 50%
Global 100% 100%
https://innovation.cms.gov/Files/x/kcc-rfa.pdf

Performance Level Adjustment
Top 10% of KCF Practices +20%
11-20% of KCF Practices +16%
21-30% of KCF Practices +12%
31-40% of KCF Practices +8%
41-50% of KCF Practices 2%
Top 50% of NATIONAL Practices 0%
51-75% of NATIONAL Practices -6%
Bottom 25% of NATIONAL Practices -20%
Did not pass quality gateway -20%
KCF Option
* Red text denotes bottom 50% of KCF Practices

CKCC Option
Shared Losses
Benchmark based on historical expenditures
$
Performance year
expenditures
$
Shared Savings
Benchmark based on historical expenditures
$
Performance year
expenditures
$KCE and CMS share in savings
KCE and CMS share in losses

Does home dialysis save money?
USRDS ADR, 2020

Does home dialysis save money?
Outcome HD PD Difference
Mortality (12 month) 8.1% 7.2% -0.9%
(7.8%, 8.4%) (5.2%, 8.8%) (-3.3%, 0.8%)
# Hospitalizations /
Patient (Months 7-12)0.71 0.66 -0.05
(0.69, 0.72) (0.52, 0.77) (-0.20, 0.07)
Total Spending ($) /
Patient (Months 7-12)$14,208 $13,506 -$702
($13,838, $14,932) ($10,987, $16,906) (-$4,004, $2,909)
Analysis of USRDS data, manuscript under review

• Determine how many patients must transition to home dialysis to move up a performance tier (and whether this is realistic)
• Aggressively identify opportunities to graduate into home dialysis
• Age out in-center HD capital equipment faster
• Identify space that can be converted into a home dialysis space
• Recognize that the ETC is a PRE-ESRD program
Strategies for Success (if in the ETC)

Early Education is Key
0%
5%
10%
15%
1 2 3 4 5 6 7 8 9 10 11 12
Pro
babili
ty o
f S
witchin
g f
rom
HD
to P
D
Month of Dialysis
Uninsured Medicaid
B
Lin E, et al. 2021. Med Care. 2020;58(7):632-642.

• PD may be easier to scale initially, given larger margins.
• Successful home HD programs often require economies of scale
• However, some evidence suggests it is easier to transition patients on in-center HD to home HD rather than PD
Strategies for Success (if in the ETC), cont’d

Questions?

• 1. Lin E, Cheng XS, Chin K-K, et al. Home Dialysis in the Prospective Payment System Era. Journal of the American Society of Nephrology. 2017;28(10):2993-3004. doi:10.1681/ASN.2017010041• 2. United States Government Accountability Office. End-Stage Renal Disease: Medicare Payment Refinements Could Promote Increased Use of Home Dialysis. Report to the Subcommittee on Health, Committee on Ways and Means, House of Representatives. GAO-16-125. Published October 2015. Accessed June 19, 2019. https://www.gao.gov/assets/680/673140.pdf• 3. Centers for Medicare and Medicaid Services (CMS), HHS. Medicare Program; Specialty Care Models To Improve Quality of Care and Reduce Expenditures. CMS-5527-F. Federal Register. 2020;85(189):61114-61381.• 4. Centers for Medicare & Medicaid Services. Kidney Care Choices (KCC) Model: Request for Applications (RFA). Published October 10, 2019. Accessed February 7, 2020. https://innovation.cms.gov/Files/x/kcc-rfa.pdf• 5. United States Renal Data System. 2020 USRDS Annual Data Report: Epidemiology of Kidney Disease in the United States. National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases; 2020. Accessed February 3, 2021. https://adr.usrds.org/2020• 6. Lin E, Chertow GM, Bhattacharya J, Lakdawalla D. Early Delays in Insurance Coverage and Long-term Use of Home-based Peritoneal Dialysis. Med Care. 2020;58(7):632-642. doi:10.1097/MLR.0000000000001350
References