Impact and celebration event - supporting quality improvement in primary care by Somerset CCG
16
Supporting Quality Improvement in Primary Care Clinical Leadership to Improve Health
-
Upload
nhs-improving-quality -
Category
Healthcare
-
view
477 -
download
0
Transcript of Impact and celebration event - supporting quality improvement in primary care by Somerset CCG

Supporting Quality Improvement
in Primary Care
Clinical Leadership to Improve Health

Primary Care Improvement Plan (PCIP)• Multiple work streams directed toward improving safety
and quality
NHS Improving Quality (NHSIQ)• Leading Improvement of Quality and Safety in Primary
Care (LISQ)
Somerset Quality Practice Scheme (SPQS) • Alternative to QOF
• Motivating primary care to examine and change an established model of practice
Clinical Leadership to Improve Health
LISQ – Launch Event, August 2013• Joint Governing Body and COG development session
Making the case for change• challenging assumptions about safety in primary care• time to think and reflect• enhancing and distributing leadership• Empowering patients
NHS Change Model
Clinical Leadership to Improve Health

1
10
100
1,000
10,000
100,000
1 10 100 1,000 10,000 100,000 1million 10million
Number of encounters for each fatality
To
tal l
ives
lost
per
yea
r
REGULATEDHAZARDOUS(>1/1000)
ULTRA-SAFE(<1/100K)
Health Care
Himalayan Climbing
Driving
Chemical Manufacturing
Chartered Flights
Scheduled Airlines
European Railroads
Nuclear Power
What do we know?
Amalberti, R., Y. Auroy, et al. (2005). Ann Intern Med 142(9): 756-764
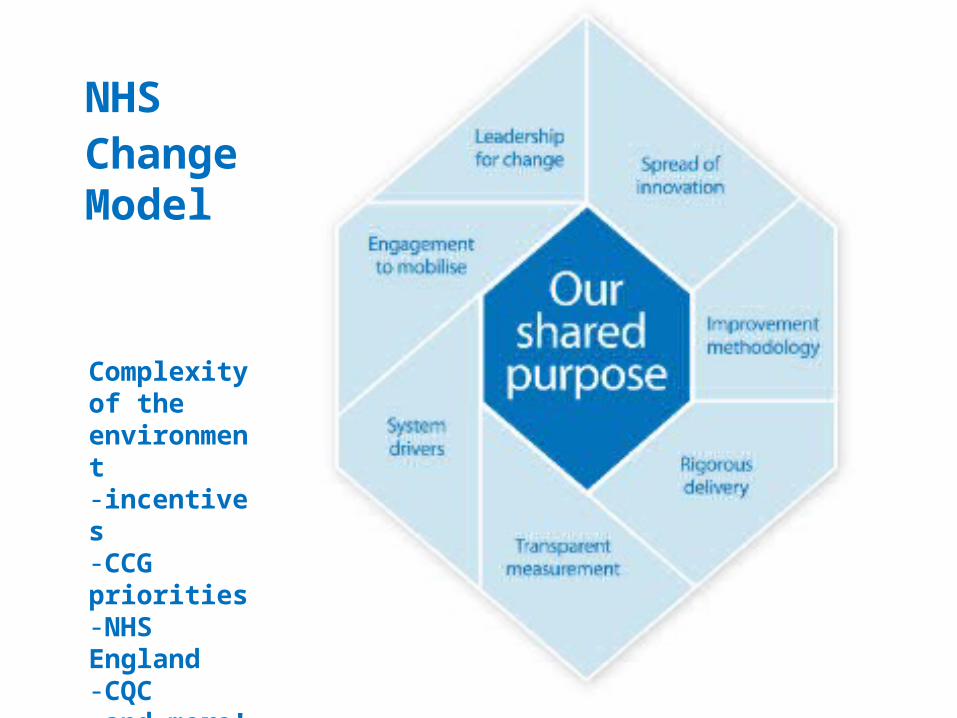
NHSChange Model
Clinical Leadership to Improve Health
Complexity of the environment-incentives-CCG priorities-NHS England-CQC -and more!

Leaders to be a visible presence as COG leaders PPG Involvement Agreement to change – rather than imposition Identify other leaders Federation leadership and support Measure the baseline Identify resources and drivers Safety risks – vulnerable patients who trust their drs! Time to think and reflect
Clinical Leadership to Improve Health
LISQ Launch Event outputs

14 practices across 6 federations 5 workshop days November 2013 – May 2014 Financial incentives to participate – backfill costs Learning
• the case for change• improvement tools and techniques
Improvement testing back at practices between workshops
Clinical Leadership to Improve Health

Established greater insights into patient safety issues Less fear about mistakes – look at the system people
are working in A range of tools and techniques to support making
change and improvement A foundation to build networks for sharing and learning
together collaboratively Medication reporting in primary care Skills and competencies are transferable to other
aspects of work
Clinical Leadership to Improve Health

Build upon the learning• Federation sharing and learning• Access to tools and techniques• identify local issues at federation level for collaborative learning
Medication reporting as a model for sharing and networking
Links to SPQS• increasing primary care adaptive capacity• use the model, tools and techniques for exploring variation• time and space to review systems and processes• enable primary care to rise to the challenges ahead
Clinical Leadership to Improve Health

An initial approach to the Area Team by the LMC and CCG, proposing an alternative approach to QOF
Strong support from the Area Team for innovation
National concern about allowing local variation, especially from the GPC and from some senior leaders in NHS England
Despite the tight timescale, a thorough process of engagement with GPs and other stakeholders
Clinical Leadership to Improve Health

Deep wish to focus on integration, including information sharing
A strong sense that QOF is not facilitating the best quality care (overly medical, insufficiently person-centred)
Strong support for more person-centred care
Education campaigns to influence use of services
Freedom to innovate, but also clarity over what is expected
Clinical Leadership to Improve Health

Not a detailed set of clinical specifications like QOF. Instead GPs commit to three things:
1.Continuing to deliver good quality care
2.Working together with other practices and providers to develop local integration plans
3.Working together with other practices to improve sustainability
Clinical Leadership to Improve Health
Project management support available to practices from the CCG
Funding is based on what practices would have earned from QOF with 70% guaranteed and 30% dependent on satisfactory update reports
South West Academic Health Science Network is leading the evaluation, which focuses on clinical quality and the role of GPs in integrated care systems
Clinical Leadership to Improve Health

Some examples of innovations undertaken as part of SPQS:
Shared nursing staff across groups of practices
Enhanced end of life care in a very rural community
Voluntary sector clinics in general practice
Person-centred care planning and peer support
Clinical Leadership to Improve Health

AHSN evaluation due July 2015
Outcome based
• patient activation and experience
• selected QOF measures - CQRS remains active
Measuring and acting on variation
Practice ownership of measurement
Clinical Leadership to Improve Health

• The relationship between the CCG, LMC and Area Team was crucial.
• There are multiple definitions of quality in general practice.
• The time needed to design an alternative cannot be underestimated.
• The acceptability of measures to clinicians is an important success factor in quality improvement projects.
• Our approach to incentives tends to focus on financial incentives. We found that a strong incentive for general practitioners is a satisfying working day. Consideration of incentives in a broad sense is therefore important.
Clinical Leadership to Improve Health