National Program of Cancer Registries Cancer Surveillance ...
Upload
isabella-richardsonCategory
view
217download
1
Immunotherapy and CancerMauricio Burotto MD
National Cancer Institute
National Institutes of Health
DISCLOSURE
• Nothing to disclose

Nature 2001

Nature 2008
Applied Biosystems 3730xl
Illumina (Solexa) sequencing
Ion Proton Machine


OMICS
GENOMICS
TRANSCIPTOMICS
PROTEOMICS
METABOLOMICS
IMMUNOMICS
MICROBIOMICS
EPIGENOMICS

The Hot topic…
Genomics Deep sequencing
Stem Cells
Cancer Metabolism
EpigenomicsInmunotherapy
Clonal evoution
Target Therapy


Cancer ImmunotherapyType Specific Tumor Stage FDA
Interleuquines IL-2IL-15
Melanoma IV yesNo
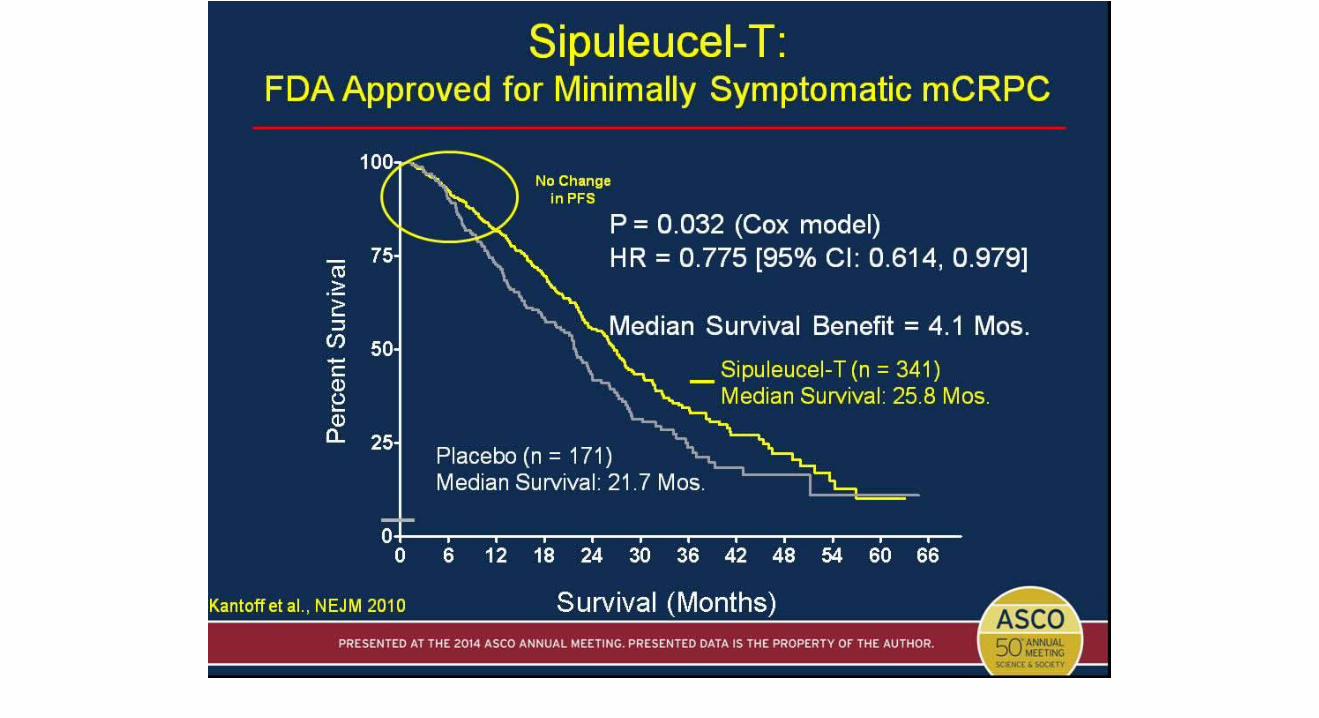
Vaccines Sipileucel-TProsvac
Prostate IV yesNo
Check point inhibitors
Anti-CTLA4Anti-PD1Anti-PDL1
MelanomaNSCLC
IV yesyesyes
Adoptive Cell Therapy
CARsTILs
ALL NHL IV No
Target therapy in Cancer
• Bevacizumab Antiangiogenic therapy
• FDA approved for – RCC– NSCLC– CRC– Ovarian Cancer– Cervical Cancer– Gliobastoma



The ”Real’” Target therapy
• Cancer therapy pardigm in 2000
• CML Philadelphia cromosome 9/22
• NSCLC and history of EGFR
• Melanoma and the BRAF


Science 2002




Evolucion clonal
Heterogeneidad molecular

Gerlinger NEJM 2012

Immune system
• Innate immune system– Neutrophiles– Complement – NK
• Adaptive immune system– B cell– T cell– Antibodies
Immune system
• Innate immune system– Neutrophiles– Complement – NK
• Adaptive immune system– B cell
– T cell– Antibodies
Therapeutic Cancer Vaccines
• Designed to generate a targeted anti-tumor immune response
• Associated with minimal toxicities
• May have delayed effects relative to standard cytotoxic chemotherapy
• May have an impact beyond the period of administration
Slide 4

Sipuleucel-T: Activates Immune Cells Ex Vivo

Prostvac: Off the Shelf Vaccine

Phase II Trial: Prostvac <br />Extended Overall Survival in mCRPC
Presented By Ravi Madan at 2014 ASCO Annual Meeting

Immune Checkpoint Inhibitors
• Checkpoint molecules are the immune system ‘s way to auto-regulate
• Blocking these molecules can enhance T-cell activity
• Immune Checkpoint Targets– CTLA-4 (activated T cells)
– PD-1 (activated T and B cells)
– PDL-1 ( can be expressed on tumor cells)

CTLA-4 Checkpoint Inhibition

CTLA-4 Checkpoint Inhibition

Slide 14

Slide 35

Impressive Activity for Anti-PD-1 in RCC
• 57-year-old patient had developed progressive disease after receiving sunitinib, temsirolimus, sorafenib, and pazopanib
• Rx with Nivolumab (anti-PD-1) at 1 mg/kg q 2 wks x 2 years
• Completed 12 cycles – now with PET Complete Response
Pretreatment 6 months
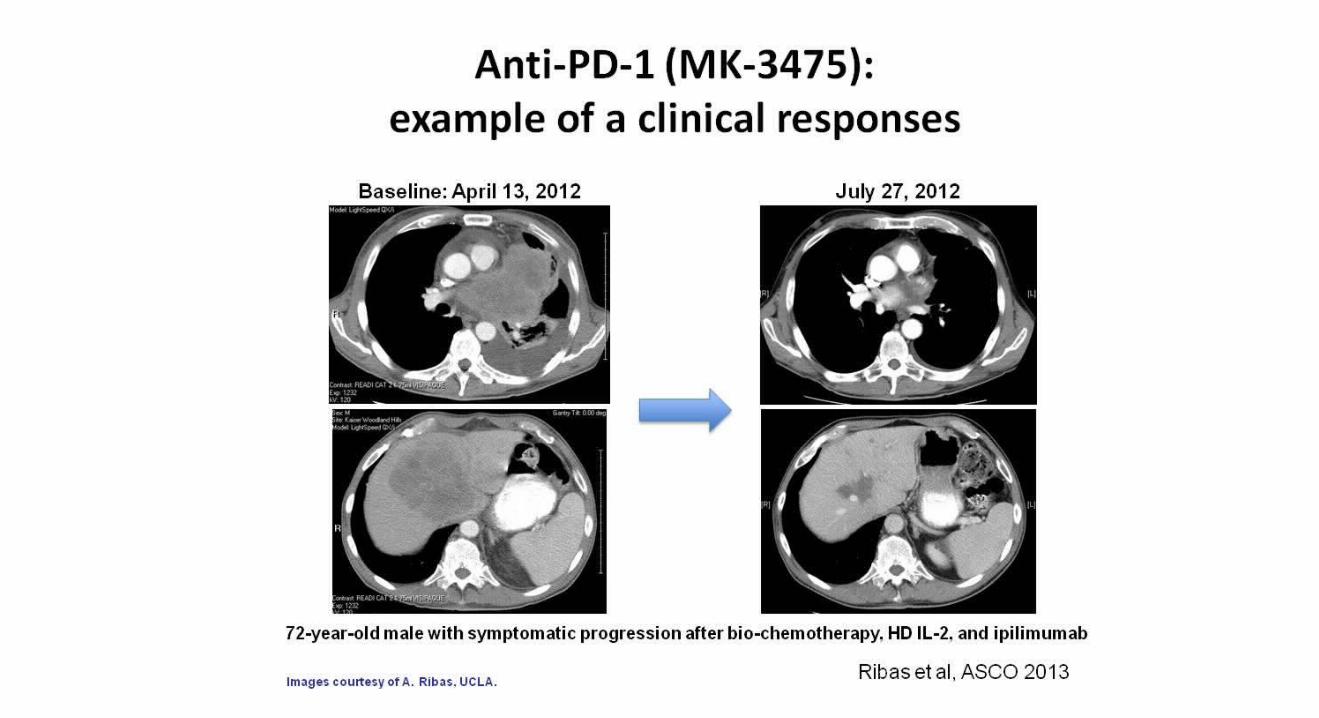
Anti-PD-1 (MK-3475): <br />example of a clinical responses

Immunotherapies combination




Cellular therapies
• TMO– Allogeneic – DLI
• T Cell adoptive therapy
– TILs– CARS ( Chimeric antigen receptor)

Adoptive cell transfer immunotherapy

CARs

Perspective on how treatments in cancer are built
Industry
FDA EMA
NCCNASCO ESMO CCO
Academiccenters NCI
More than 90% of cancer drugs approved since 2004 cost more than $20000 for 12 weeks of treatment.

Latin America and the Caribbean

•By 2020, it is estimated that more than 100 million people older than 60 years will be living in S.A
•1.7 million new cases of cancer will be diagnosed by 2020
•6% of the Latin American population is covered by national cancer registries, by contrast with 96% in the USA and 32% in Europe
•In three years, up to 65% of FDA-regulated clinical trials will be conducted outside the U.S.

Incidence of cancer is lower in Latin America 163 per 100 000 (rate) than in Europe 264 or the USA 300
Cancer mortality-to-incidenceratio for Latin America is 0.59, compared with 0.43 for the Europe and 0.35 in the USA [HIGH LETHALITY]
Ferlay et al , GLOBOCAN 2008http://globocan.iarc.fr (2012)
But
Goss et al. Lancet Oncol. 2013 ;14:391

Challenges to Conducting Clinical Trials in Latin America
• Longer regulatory activities– Regulatory authorization and ethics committee approval– Different local requirements between countries
• Lack of infrastructure – The need for electronic data collection systems.– Better training for the research team (radiologist, pathologist, nurses
etc.)
Outlook 2008. Tufts Center for the Study of Drug Development

Potential advantages to Conducting Clinical Trials in Latin America
• Patient enrollment– Shorter enrollment time
– Fewer or non competing studies in the region
– Most patients are treatment and trial naïve
– Up to 80% of the population is concentrated in big cities.
• Latin America is one of the most diverse regions in the world– Diversity in ethnicity
– However there are regions with very homogenous population (indigenous)
– Example: Chile has the highest incidence of gastric and gallbladder cancer in the world
Outlook 2008. Tufts Center for the Study of Drug Development

Cancer Research in Latin America and the Caribbean
Accrual opportunities
Novel designs and concepts
Pharmacogenomics studies

Tito FojoMaureen Edgerly
Giuseppe GiacconeArun Rajan
Wilfred SteinKrastan BlagoevJohn Marshall
Eva SzaboMaureen Edgerly
James GulleyRobert Motzer
Agradecimientos

Clinical Research Center Staff