Immunoblotting 55 systemicJ Ph MERY,3 AND M F KAHN2 Fromthe 'Laboratoire d'Immuno-Rhumatologie,...
6
Annals of the Rheumatic Diseases 1989; 48: 594-599 Immunoblotting profiles in 55 systemic lupus erythematosus sera lacking precipitating antibodies to extractable nuclear antigens 0 MEYER,1 P BOURGEOIS,2 A AESCHLIMANN,2 T HAIM, J Ph MERY,3 AND M F KAHN2 From the 'Laboratoire d'Immuno-Rhumatologie, H6pital Lariboisiere, 2 rue Ambroise Pare, 75475 Paris Cedex 10; the 2Clinique de Rhumatologie, Universite Paris VII, H6pital Bichat, 46 rue Henri Huchard, 75018 Paris; and the 3Service de Nephrologie, H6pital Bichat, 46 rue Henri Huchard, 75018 Paris SUMMARY Serum samples from 55 patients with systemic lupus erythematosus (SLE) were selected for the absence of anti-extractable nuclear antigen antibodies after routine immunodiffu- sion tests. These sera were immunoblotted for anti-Sm and anti-RNP antibodies on a HeLa cell nuclear extract. Ten (18%) were negative and 45 (82%) produced complex patterns: 10 (18%) suggestive of anti-Sm, three (5%) anti-RNP, and 32 (58%) a combination of anti-Sm and anti- RNP antibodies. These data were very similar to those obtained from sera from a control group of 28 SLE sera selected for positivity of anti-Sm and anti-RNP precipitins with the immunodiffusion test. IgM isotype antibodies to the D peptide were significantly more prevalent than IgG isotype antibodies, whereas antibodies to the 68 kD polypeptide were of both IgM and IgG isotypes. Sera with an anti-Sm/RNP immunoblotting pattern stemmed from a group of patients with SLE with a higher titre of anti-dsDNA antibodies. Among clinical symptoms, the incidence of haemolytic anaemia was higher in the group of patients with the anti-Sm immunoblotting profile. Patients with an anti-RNP immunoblotting profile showed a higher incidence of cutaneous symptoms. It is concluded that immunoblotting for anti-Sm or anti-RNP antibody determination is a very sensitive diagnostic tool in patients with SLE. Key words: antinuclear antibodies, Western blotting, anti-Sm/RNP antibodies. Patients with systemic lupus erythematosus (SLE) produce antibodies which react with various nuclear components: DNA, histones, proteins, and RNA- protein complexes such as Sm and U1RNP antigens. ' The anti-Sm antibodies are considered to be a specific marker of SLE and constitute a major serological American Rheumatism Association criterion for diagnosis.2 Anti-UlRNP antibodies have a strong association with mixed connective tissue disease but are also present in SLE, frequently associated with anti-Sm antibodies.35 Anti-Sm anti- bodies, however, are less frequently present in SLE sera and are found in only 10-30% when immuno- Accepted for publication 26 October 1988. Correspondence to Dr 0 Meyer, H6pital Bichat, 46 rue Henri Huchard, 75018 Paris, France. diffusion and counterimmunoelectrophoresis are used for their detection.1 Sera containing anti-Sm and anti-RNP react with a family of small nuclear RNA-protein complexes.3 Immunoblotting studies have shown that anti-Sm antibodies react preferentially with a set of at least two proteins of the RNP-protein complexes: B/B' (25 kD) and D (14 kD) peptides,4 67 whereas anti-RNP sera react with the 68 kD, A (31 kD), and C (19 kD) peptides.6 The purpose of this study was to analyse the immunoblotting pattern in 55 patients with SLE lacking anti-Sm or anti-RNP precipitins on immuno- diffusion and to investigate whether there were correlations between the blot pattern and distinct clinical and serological findings. 594 copyright. on December 23, 2020 by guest. Protected by http://ard.bmj.com/ Ann Rheum Dis: first published as 10.1136/ard.48.7.594 on 1 July 1989. Downloaded from
Transcript of Immunoblotting 55 systemicJ Ph MERY,3 AND M F KAHN2 Fromthe 'Laboratoire d'Immuno-Rhumatologie,...

Annals of the Rheumatic Diseases 1989; 48: 594-599
Immunoblotting profiles in 55 systemic lupuserythematosus sera lacking precipitating antibodiesto extractable nuclear antigens0 MEYER,1 P BOURGEOIS,2 A AESCHLIMANN,2 T HAIM,J Ph MERY,3 AND M F KAHN2
From the 'Laboratoire d'Immuno-Rhumatologie, H6pital Lariboisiere, 2 rue Ambroise Pare, 75475 ParisCedex 10; the 2Clinique de Rhumatologie, Universite Paris VII, H6pital Bichat, 46 rue Henri Huchard, 75018Paris; and the 3Service de Nephrologie, H6pital Bichat, 46 rue Henri Huchard, 75018 Paris
SUMMARY Serum samples from 55 patients with systemic lupus erythematosus (SLE) were
selected for the absence of anti-extractable nuclear antigen antibodies after routine immunodiffu-sion tests. These sera were immunoblotted for anti-Sm and anti-RNP antibodies on a HeLa cellnuclear extract. Ten (18%) were negative and 45 (82%) produced complex patterns: 10 (18%)suggestive of anti-Sm, three (5%) anti-RNP, and 32 (58%) a combination of anti-Sm and anti-RNP antibodies. These data were very similar to those obtained from sera from a control group
of 28 SLE sera selected for positivity of anti-Sm and anti-RNP precipitins with theimmunodiffusion test. IgM isotype antibodies to the D peptide were significantly more prevalentthan IgG isotype antibodies, whereas antibodies to the 68 kD polypeptide were of both IgM andIgG isotypes. Sera with an anti-Sm/RNP immunoblotting pattern stemmed from a group ofpatients with SLE with a higher titre of anti-dsDNA antibodies. Among clinical symptoms, theincidence of haemolytic anaemia was higher in the group of patients with the anti-Smimmunoblotting profile. Patients with an anti-RNP immunoblotting profile showed a higherincidence of cutaneous symptoms. It is concluded that immunoblotting for anti-Sm or anti-RNPantibody determination is a very sensitive diagnostic tool in patients with SLE.
Key words: antinuclear antibodies, Western blotting, anti-Sm/RNP antibodies.
Patients with systemic lupus erythematosus (SLE)produce antibodies which react with various nuclearcomponents: DNA, histones, proteins, and RNA-protein complexes such as Sm and U1RNP antigens. 'The anti-Sm antibodies are considered to be aspecific marker of SLE and constitute a majorserological American Rheumatism Associationcriterion for diagnosis.2 Anti-UlRNP antibodieshave a strong association with mixed connectivetissue disease but are also present in SLE, frequentlyassociated with anti-Sm antibodies.35 Anti-Sm anti-bodies, however, are less frequently present in SLEsera and are found in only 10-30% when immuno-
Accepted for publication 26 October 1988.Correspondence to Dr 0 Meyer, H6pital Bichat, 46 rue HenriHuchard, 75018 Paris, France.
diffusion and counterimmunoelectrophoresis areused for their detection.1
Sera containing anti-Sm and anti-RNP react witha family of small nuclear RNA-protein complexes.3Immunoblotting studies have shown that anti-Smantibodies react preferentially with a set of at leasttwo proteins of the RNP-protein complexes: B/B'(25 kD) and D (14 kD) peptides,4 6 7 whereasanti-RNP sera react with the 68 kD, A (31 kD), andC (19 kD) peptides.6The purpose of this study was to analyse the
immunoblotting pattern in 55 patients with SLElacking anti-Sm or anti-RNP precipitins on immuno-diffusion and to investigate whether there werecorrelations between the blot pattern and distinctclinical and serological findings.
594
copyright. on D
ecember 23, 2020 by guest. P
rotected byhttp://ard.bm
j.com/
Ann R
heum D
is: first published as 10.1136/ard.48.7.594 on 1 July 1989. Dow
nloaded from

Immunoblotting profiles in systemic lupus erythematosus sera 595
Patients and methods
PATIENTS AND SERASerum samples used in this study were obtainedfrom 83 patients who fulfilled the revised AmericanRheumatism Association criteria for SLE.2 Fiftyfive sera found to be devoid of anti-Sm or anti-RNPprecipitating antibodies were drawn from 55patients with SLE (47 female, eight male, 51 white,four black; mean (SD) age: F 34 (12) years, M 31-5(13-3) years) with a mean (SD) duration of diseaseof 7-2 (5.8) years.
Twenty eight control sera, selected for a positiveanti-Sm (23 sera) or anti-Sm and anti-RNP (fivesera) precipitation test, were drawn from 28 patientswith SLE (23 female, five male; 19 white, sevenblack, two oriental) matched for the same mean
duration of disease as the 55 patients with SLEwithout anti-Sm or RNP antibodies. All sera werestored at -20°C and complement inactivated at 56°Cfor 30 minutes before use.
IMMUNOBLOTTING FOR THE DETECTION OF
ANTINUCLEAR ANTIBODIESThe technique described by Habets et al was usedwith only slight modifications.8 HeLa cell nuclearextract was dissolved in sodium dodecyl sulphate gelsample buffer and then suibjected to 12% sodiumdodecyl sulphate-polyacrylamide gel electro-phoresis according to Laemmli9 for 18 hours at 50V/0-3 A. After separation the nuclear proteins weretransferred to transblot nitrocellulose sheets byelectroblotting according to Towbin et allo for fourhours at 70 V/0-4 A. To probe for the presence ofantigenic nuclear peptides the nitrocellulose stripswere incubated with patient sera diluted 1:100 inphosphate buffered saline containing 0-1% Tween.Binding ofthe antibodies was detected by horseradishperoxidase conjugated rabbit antihuman IgG or IgMantibodies (Cappel, Flobio France, 3201-0121) withdiaminobenzidine as the substrate. Standard serawere applied on each blot as positive controls and asreference samples to allow identification of anti-RNP (68 kD band, A band, C band) and anti-Sm(B/B' doublet and D band) specificities.6
ASSAY FOR PRECIPITATING ANTIBODIESAGAINST EXTRACTABLE NUCLEARANTIGENSExtractable nuclear antigens were prepared by themethod of Mattioli and Reichlin11 from fresh calfthymus, or using an extract of rabbit thymus powder(Pel Freez, Rogers, Arkansas). The extractablenuclear antigen preparations were used at a finalconcentration of 40 mg/ml for calf thymus and 100mg/ml for rabbit thymus in phosphate buffered
saline pH 7-4. Antibodies were detected by im-munoprecipitation with 0-8% agarose in phosphatebuffered saline. Patients' sera were tested undiluted,and diffusion was carried out at room temperaturein a humidified chamber for 48 hours.
Precipitins were identified by comparison withreference anti-RNP and anti-Sm sera from theCenter For Disease Control, Atlanta, Georgia,USA12 and by searching for lines of completeidentity with the patient's precipitin(s). Antibodiesdetected against Ro (SSA) antigen were also testedby immunodiffusion with a human splenic solubleextract13 and identified with a reference anti-SSA(Ro) serum.12
OTHER LABORATORY PROCEDURESThe following laboratory procedures were per-formed routinely: assay for antinuclear antibodiesby indirect immunofluorescence on rat liver sec-tions,14 and for anti-dsDNA antibodies by indirectimmunofluorescence on Crithidia luciliae as describedby Aarden et al. 15
STATISTICSStatistical comparisons between groups were madeby the x2 method, with Yates's continuity correction,or Fisher's exact test ifthe number ofpatients was low.A value of p<0-05 was considered significant.
Results
Sera from the 55 patients with SLE without anti-Smor anti-RNP precipitins showed a variety of im-munoblot patterns of peptide reactivity (Table 1).Thirty three sera (60%) reacted against the Dpeptide and 28 (51%) against the B/B' doublet.Twenty sera (36%) reacted against the 68 kDpolypeptide; 14 (25%) and 17 (31%) sera reactedagainst the A and C peptide respectively. Ten sera
Table 1 Immunoblot results of sera from 55 patients withsystemic lupus erythematosus without Sm or SmIRNPprecipitins. Values show the number of sera binding tospecific polypeptides and detected with antisera specific forimmunoglobulin isotype
Polypeptide IgG 1gM lgG and IgG or IgMIgM
No %
68 kD 5 3 12 20 36A (31 kD) 4 5 5 14 25B/B' (25 kD) 6 7 15 28 51C (19 kD) 5 5 7 17 31D (14 kD) 3 10 20 33 60Blank 10 18
copyright. on D
ecember 23, 2020 by guest. P
rotected byhttp://ard.bm
j.com/
Ann R
heum D
is: first published as 10.1136/ard.48.7.594 on 1 July 1989. Dow
nloaded from

596 Meyer, Bourgeois, Aeschlimann, Haim, Mery, Kahn
(18%) showed a negative Sm or RNP immunoblotreactivity on two different runs.Table 1 also shows the patterns of IgG and IgM
reactivities with the U1RNP and Sm polypeptides.Both antibody isotypes were present against eachpolypeptide in approximately 50% of the sera.IgM was the dominant isotype of anti-D (14 kD)
polypeptide positive sera (x2=4*7; p<005), where-as IgG was the dominant isotype of anti-68 kDpolypeptide positive sera.Most sera produced a complex pattern suggestive
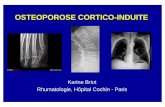
of anti-Sm, anti-RNP, or anti-Sm and anti-RNPantibodies (Table 2). Ten sera (18%) recognisedeither the B/B' doublet or the D protein and wereidentified as anti-Sm sera. Three sera (5%) recog-nised the 68 kD polypeptide, alone or in conjunctionwith the A or C peptide, or both, and were calledanti-RNP positive sera. Finally, 32 sera (58%)recognised simultaneously the 68 kD, B/B' doublet,and D peptides as well as either the A or C peptidesand were identified as anti-Sm/RNP positive sera(Fig. 1). The control group of 28 SLE sera with Smor Sm/RNP precipitins produced very similar im-munoblot patterns of peptide reactivity (Table 2).At the time of sampling 47 patients (85%) were
positive in the indirect immunofluorescent test onCrithidia luciliae for anti-dsDNA antibodies: 21patients had an anti-dsDNA antibody titre over 40.Among these 21 patients, 14 (67%) produced ananti-Sm/RNP pattern on immunoblots. One third ofsera with an anti-RNP or anti-Sm pattern and 20%of sera with a negative reactivity produced asimilarly high titre of anti-dsDNA antibody(p=NS). Sera from patients with anti-Sm/RNPantibodies had a low anti-dsDNA antibody titre lessfrequently than all the other groups of sera (p<003)(Table 3).
Table 2 Comparison ofthe immunoblot results of55 SLEsera without Sm or SmIRNP precipitins and 28 SLEsera with Sm or SmIRNP precipitins
Immunoblot Ouchterlony result for anti-Sm orantibody SmIRNP precipitinsspecificity
Negative Positive
No % No %
Sm* 10 18 5 18RNPt 3 5 3 11Sm/RNPt 32 58 18 64Blank 10 18 2 7
*Sm=B/B'+D or D alone or B/B' alone.tRNP=68 kD, alone or associated with either A or C polypeptides.tSm/RNP=any combination of RNP polypeptides with Smpolypeptides.
.. r E ~~MW. ( Kda
F 4~~~69
445
2f 3; 4 'I(J 7 92
Fig. 1 Immunoblotting ofseven sera from patients withsystemic lupus erythematosus lacking anti-Sm or RNPprecipitins. Lane 1, 2, 3: reference sera for anti-La (SS-B),anti-RNP, and anti-Sm specificities; lane 4:68 kD+A+C;lane 5: 68 kD+A; lane 6: B/B'+C; lane 7 B/B'+C+ E;lane8: BIB';lane9: B/B'+ ?+D;lanelO:histone+BIB'++D.Extra lines are also present.
Table 3 Relation between anti-dsDNA antibody titres andimmunoblot antibody specificities of 55 systemic lupuserythematosus sera without Sm or SmIRNP precipitins
Immunoblot antibody specificity
Sm SmIRNP RNP blank(n=1O) (n=32) (n=3) (n=1O)
Anti-dsDNA titreS 10 (n=17) 6 6* 0 5> 20 (n=38) 4 26 3 5
*X2=5-3; p<003.
To investigate a possible relation between im-munoblotting results and clinicoserological findingsin SLE the 55 patients were divided into four groupsaccording to their immunoblotting patterns and
copyright. on D
ecember 23, 2020 by guest. P
rotected byhttp://ard.bm
j.com/
Ann R
heum D
is: first published as 10.1136/ard.48.7.594 on 1 July 1989. Dow
nloaded from

Immunoblotting profiles in systemic lupus erythematosus sera 597
Table 4 Relation between immunoblotting antibody specificities and disease symptoms in the group of 55 patients withsystemic lupus erythematosus
Disease feature No (%) of patients No (%) of sera positive for antibody specificity studied bywith the disease feature immunoblotting
Sm SmlRNP RNP Blank(n=1O) (n=32) (n=3) (n=10)
Malar erythema 41 (75) 5 (50) 26 (81) 3 (100) 7 (70)Discoid lupus 2 (4) 0 (0) 2 (6) 0 (0) 0 (0)Photosensitivity 26 (47) 4 (40) 16 (50) 2 (66) 4 (40)Oral ulcers 8 (15) 2 (20) 5 (16) 0 (0) 1 (10)Alopecia 13 (24) 3 (30) 7 (22) 1 (33) 2 (20)Raynaud's syndrome 16 (29) 6 (60) 6 (19) 2 (66) 2 (20)Swollen fingers 7/53 (13) 1 (10) 4 (13) 0 (0) 2 (20)Vasculitis 14 (25) 4 (40) 8 (25) 0 (0) 2 (20)Arthritis 38 (69) 8 (80) 20 (63) 3 (100) 7 (70)Pleuritis/pericarditis 24 (44) 5 (50) 12 (38) 1 (33) 6 (60)Renal involvement 33 (60) 6 (60) 21 (66) 2 (66) 4 (40)Central nervous system involvement 11 (20) 4 (40) 5 (16) 1 (33) 1 (10)Haemolytic anaemia 10 (18) 4 (40) 6 (19) 0 (0) 0 (0)Leucopenia 28 (51) 5 (50) 17 (53) 1 (33) 5 (50)Thrombopenia 5 (9) 2 (20) 2 (6) 0 (0) 1 (10)Lupus erythematosus cells 26151 (51) 6 (60) 15 (48) 2 (66) 4 (40)FBTS* 8/54 (15) 2 (20) 5 (16) 1 (33) 0 (0)Anti-dsDNA antibodies 48 (87) 10 (100) 30 (94) 3 (100) 5 (50)Antinuclear antibodies 55 (100) 10 (100) 32 (100) 3 (100) 10 (100)
*FBTlS=false biological test for syphilis.
listed according to the symptoms they displayedduring the course of the disease (Table 4). Patientswith anti-Sm/RNP antibodies showed a decreasedincidence of Raynaud's syndrome (p<005); patientswith anti-Sm antibodies had an increased incidenceof haemolytic anaemia (p<0-05). Patients with anti-RNP antibodies showed a higher incidence ofcutaneous involvement (p<0-05). The incidence ofother American Rheumatism Association criteria,such as renal or central nervous system involvementas well as vasculitis, was not statistically different inthe anti-Sm group as compared with the anti-Sm/RNP and anti-RNP antibody positive groups.
Discussion
The aim of this study was to investigate thesensitivity of the immunoblotting technique for thedetection of anti-Sm and anti-RNP nuclear anti-bodies in sera from patients with SLE lackingprecipitins against these nuclear antigens. For thispurpose we selected a group of 55 patients withSLE, comprising 35 from the rheumatology unit and20 from the nephrology unit. All sera were repeatedlynegative for anti-Sm and anti-RNP precipitins withthe double diffusion technique against rabbit andcalf soluble nuclear extracts. Several studies haveshown that Sm and RNP antigens contain a series ofsmall nuclear RNA species associated with at least
eight polypeptides, which consist of a 68 kDpolypeptide and others of lower molecular weightdesignated A to G, according to Lemer and Steitznomenclature.3 4 6 7 The RNP antigenic determi-nants are present mainly on the 68 kD, A (31 kD),and C (19 kD) proteins; Sm determinants are foundmainly on polypeptides B/B' (25 kD) and D (14kD).6The B/B' polypeptides are sometimes faintly
recognised by anti-RNP positive sera, however.6 Inline with these previously published data we decidedto designate anti-Sm as those antibodies whichrecognised either of the B/B' and D polypeptides,anti-RNP as those antibodies which recognised the68 kD polypeptide or either of the A and Cpolypeptides, and anti-Sm/RNP as those antibodieswhich recognised simultaneously any of the RNPpolypeptides and either of the D or B/B' poly-peptides. According to Pettersson et aP4 and VanVenrooij6 it seems that anti-RNP specificities inpatients with SLE are primarily composed of re-actions with A and C polypeptides.Using the immunoblotting technique in conjunc-
tion with this nomenclature, we found that 45 (82%)of the 55 SLE sera contained non-precipitatingantibodies against the polypeptide components ofthe Sm and RNP particles: Sm polypeptides wererecognised by 10 (18%) of the sera, RNP poly-peptides by 3 (5%), and Sm plus RNP polypeptidesby 32 (58%) of the sera.
copyright. on D
ecember 23, 2020 by guest. P
rotected byhttp://ard.bm
j.com/
Ann R
heum D
is: first published as 10.1136/ard.48.7.594 on 1 July 1989. Dow
nloaded from

598 Meyer, Bourgeois, Aeschlimann, Haim, Mery, Kahn
These data are very similar to those obtained withour control group of 28 SLE sera selected forpositive immunodiffusion precipitins against Sm orSm/RNP antigens.Our results suggest either that immunoblotting is
a highly sensitive technique for detection of anti-Smand anti-RNP antibodies or that the sensitivity ofdouble immunodiffusion, in our hands, is poor.Recent data reported from our unit estimated theprevalence of anti-Sm precipitins in patients withSLE as 6% in 40 European Caucasians, 22% in 20Arab North African patients, and 13% in 20Caribbean black patients.16 The prevalence of anti-Ro antibodies was estimated to be 27% in a group ofpatients with SLE.17 These data are very similar tothose published concerning Caucasian patients withSLE.1 16 18 Very few published reports have com-pared immunodiffusion and immunoblotting forthe detection of anti-Sm/RNP antibodies in SLEsera: Williams et al reported that four of the 13anti-Sm sera detected by immunoblotting were notdetected by counterimmunoelectrophoresis andimmunodiffusion.19 20 These sera were all IgMantibodies. They also observed four anti-RNP serathat were not detected by counterimmunoelectro-phoresis and immunodiffusion. These sera con-tained specific antibodies of the IgG and IgMclasses. Our data on antibody isotypes are in goodagreement with published work. 021 Only onestudy has previously reported differential positivityof counterimmunoelectrophoresis and immuno-blotting.22 Of 66 SLE sera without anti-RNPprecipitins as indicated by counterimmunoelectro-phoresis, none was positive for anti-UlRNP poly-peptide antibodies on immunoblotting, whereas 20out of 71 sera without anti-Sm precipitins as indi-cated by counterimmunoelectrophoresis were posi-tive for anti-Sm polypeptide antibodies on immuno-blotting. The prevalence of anti-Sm and anti-RNPwhich we found by immunoblotting is rather highcompared with these studies. Moreover, discrepanciesbetween immunoblotting and immunodiffusionappear to occur in both directions as we found 5/28sera in the control group with anti-Sm precipitins onimmunodiffusion who had a negative immunoblotpattern. Such discrepancies have been reportedpreviously20 22 and can be explained partly by thedifferent species origin of the nuclear extract (calfand rabbit thymus for immunodiffusion, humanHeLa cells for immunoblotting) or by the antibodyisotype not being detected by our immunoblottingtechnique. As reported by previous studies anenzyme linked immunosorbent assay (ELISA) ismore sensitive than counterimmunoelectrophoresisfor the detection of anti-Sm and anti-RNP anti-bodies,23 24 but there is no published comparison of
ELISAs and immunoblotting assays. Evans et al,however, were able to detect anti-UlRNP/Sm anti-bodies in some sera from patients with SLE thatwere negative for precipitin and ELISA assays.24These data suggest but do not prove that immuno-blotting may have a higher sensitivity than ELISAfor the detection of anti-Sm and anti-UlRNPantibodies.
Studies concerning the clinical and serologicalsignificance of anti-Sm and anti-RNP antibodiesdetected by immunoblotting have shown differentcorrelations: patients with SLE with anti-Sm/RNPantibodies have a higher titre of anti-dsDNA anti-bodies, a low incidence of Raynaud's syndrome, anda high incidence of haemolytic anaemia; patientswith SLE with anti-RNP antibodies have a higherincidence of cutaneous manifestations. In contrastwith previously published reports of the clinicalsignificance of anti-Sm and anti-RNP precipitatingantibodies in SLE,2530 we found no correlationbetween anti-Sm antibodies and vasculitis, renaldisease, or central nervous system symptoms. Re-cent data using immunoblot suggested that patientswith anti-Sm antibodies might have a higher inci-dence of renal disease.31 Our findings do not confirmthis claim. Patients with anti-RNP antibodies hadthe same incidence of renal disease as patients withor without anti-Sm antibodies.The reason for such discrepancies is still unclear,
and further studies with more patients will benecessary to understand the prognostic value of anti-Sm and anti-RNP antibodies detected by immuno-blotting.Our present data suggest, however, that immuno-
blotting is a very sensitive method for the detectionof anti-Sm and anti-RNP antibodies in SLE andcould be very useful for diagnosis of forms of SLEwith little symptomatology.
References
1 Tan E M. Antibodies to nuclear antigens (ANA); theirimmunobiology and medicine. In: Kunkel H G, Dixon F J, eds.Advances in immunology. Vol 33. New York: Academic Press,1982: 167-233.
2 Tan E M, Cohen A S, Fries J F, et al. The 1982 revised criteriafor the classification of SLE. Arthritis Rheum 1982; 25: 1271-5.
3 Lerner M R, Steitz J A. Antibodies to small nuclear RNAscomplexed with proteins are produced by patients with SLE.Proc Nad Acad Sci USA 1979; 76: 5495-9.
4 Pettersson I, Wang G, Smith E J, et al The use of immunoblot-ting and immunoprecipitation of (U) small nuclear ribonuc-leoproteins in the analysis of sera of patients with mixedconnective tissue disease and systemic lupus erythematosus. Across-sectional, longitudinal study. Arthritis Rheum 1986; 29:986-96.
5 Tsay G J, Chan E K L, Peebles C L, Pollard K M, Tan E M. Animmunoassay differentiating sera with antibodies to Sm alone,antibodies to Sm/RNP complex and antibodies to RNP alone.Arthritis Rheum 1987; 30: 389-96.
copyright. on D
ecember 23, 2020 by guest. P
rotected byhttp://ard.bm
j.com/
Ann R
heum D
is: first published as 10.1136/ard.48.7.594 on 1 July 1989. Dow
nloaded from

Immunoblotiing profiles in systemic lupus erythematosus sera 599
6 Van Venrooij W J. Autoantibodies against small nuclear to La, Jo-1, nRNP and Sm detected by multi-track immunoblot-ribonucleoprotein components. J Rheumatol 1987; 14 (suppl ting using a novel filter holder: a comparative study with13): 78-82. counter immunoelectrophoresis and immunodiffusion using
7 Homma M, Mimori T, Takeda Y, et al. Autoantibodies to the sera from patients with systemic lupus erythematosus andSm antigen: immunological approach to clinical aspects of Sj6gren's syndrome. J Immunol Methods 1986; 91: 65-73.systemic lupus erythematosus. J Rheumatol 1987; 14 (suppi 20 Williams D G, Stocks M R, Charles P J, Maini R N. Antibody13): 188-93. class differences are detected in anti-nRNP and anti-Sm
8 Habets W J, de Rooij D J, Salden M H, et al. Antibodies antibodies directed against distinct antigen subunits. Rheumatolagainst distinct nuclear matrix proteins are characteristic for Int 1986; 6: 189-92.mixed connective tissue disease. Clin Exp Immunol 1983; 54: 21 Guldner H H, Lakomek H J, Bautz F A. Anti-Ul RNP and265-76. anti-Sm autoantibody profiles in patients with systemic rheu-
9 Laemmli U. Cleavage of structural proteins during the assembly matic diseases: differential detection of immunoglobulin G andof the head of bacteriophage T4. Nature 1970; 227: 680-5. M by immunoblotting. Clin Immunol Immunopathol 1986; 40:
10 Towbin H, Staehelin T, Gordon J. Electrophoretic transfer of 532-8.proteins from polyacrylamide gels to nitrocellulose sheets: 22 Westgeest A A A, van den Brink H G, Dejong J, Swaak A J G,procedure and some applications. Proc Natl Acad Sci USA Smeenk R J T. Antinuclear antibodies in patients with systemic1979; 76: 4350-4. lupus erythematosus: a comparison of counter immunoelec-
11 Mattioli M, Reichlin M. Characterisation of a soluble nuclear trophoresis and immunoblotting. Rheumatol Int 1987; 7: 77-82.ribonucleoprotein antigen reactive with SLE sera. J Immunol 23 Maddison P J, Skinner R P, Vlachoyrinnopoulos D, Brennand1971; 107: 1281-90. D M, Hough D. Antibodies to nRNP, Sm, Ro (SS-A) and La
12 Tan E M, Fritzler M J, McDouglas J S, et al. Reference sera for (SS-B) detected by ELISA: their specificity and inter-relationsANA. I. Antibodies to native DNA, Sm nuclear RNP and SSB. in connective tissue disease sera. Clin Exp Immunol 1985; 62:Arthritis Rheum 1982; 25: 1003-5. 337-45.
13 Clark G, Reichlin M, Tomas T B. Characterisation of a 24 Evans J, Arguelles E, Harley J, Reichlin M, Craft J. Antibodiessoluble cytoplasmic antigen reactive with sera from patients to ribonucleoproteins in SLE [Abstract]. Arthrtis Rheum 1988;with systemic lupus erythematosus. J Immunol 1968; 102: 31(suppl): A101.117-22. 25 Barada F A, Andrews B S, Davis IV J S, Taylor R P.
14 Peltier A P, Strejcek J. Determination de la classe immuno- Antibodies to Sm in patients with SLE. Arthritis Rheum 1981;globulinique des facteurs antinucleaires fixant et ne fixant pas le 24: 1236-44.compIlment. Revue Francaise d'Etudes Cliniques et Biologiques 26 Beaufils M, Nouki F, Mignon F, et al. Clinical significance of1969; 14: 787-95. anti-Sm antibodies in systemic lupus erythematosus. Am J Med
15 Aarden L A, de Groot E R, Feltkamp T E W. Immunology of 1983; 74: 201-5.DNA. III. Crithidia luciliae, a simple substrate for the deter- 27 Reyes P A, Lavalle C. Clinical subset of systemic lupusmination of anti-dsDNA with the immunofluorescence tech- erythematosus. Arthritis Rheum 1980; 23: 1064-5.nique. Ann NY Acad Sci 1975; 254: 505-15. 28 Winn D M, Wolfe J F, Lindberg D A, Fristoe F H, Kingsland
16 Gioud Paquet M, Chamot A M, Bourgeois P, Meyer 0, Kahn L, Sharp G C. Identification of a clinical subset of systemicM F. Differences symptomatiques et pronostiques selon la lupus erythematosus by antibodies to the Sm antigen. Arthritiscommunaute ethnique dans le lupus erythemateux systemique. Rheum 1979; 22: 1334-6.Etude controlee sur 3 populations. Presse Med 1988; 17: 103-6. 29 Munves E F, Schur P H. Antibodies to Sm and RNP
17 Meyer 0, Haim T, Ryckewaert A. Signification des anticorps prognostication of disease involvement. Arthritis Rheum 1983;specifiques d'antigenes nucldaires solubles analogues a SSA et 26: 848-53.SSB au cours du LED. A propos de 35 observations. La 30 Winfield J B, Brunner C M, Koffler D. Serologic studies inNouvelle Presse Medicale 1981; 10: 2179-84. patients with systemic lupus erythematosus and central nervous
18 Hochberg M C, Dorsch C A, Feinglass E J, Stevens M B. system dysfunction. Arthritis Rheum 1978; 21: 289-94.Survivorship in systemic lupus erythematosus. Effect of anti- 31 Combe B, Lussiez V, Graafland H, Rucheton M, Sany J. Anti-body to extractable nuclear antigen. Arthritis Rheum 1981; 24: Sm, anti-RNP and anti-SSB antibodies detected by immuno-54-9. blotting in systemic lupus erythematosus. Clin Rheumatol 1988;
19 Williams D G, Stocks M R, Charles P J, Maini R N. Antibodies 7: 127.
copyright. on D
ecember 23, 2020 by guest. P
rotected byhttp://ard.bm
j.com/
Ann R
heum D
is: first published as 10.1136/ard.48.7.594 on 1 July 1989. Dow
nloaded from