Recommendations to Health Care Providers for Responding to ...

Immunization in Healthcare Providers: Recommendations,
Evidence and Controversy
Shelly A. McNeil, MD, FRCPCProfessor of Medicine, Division of Infectious Diseases
Clinician Scientist, Canadian Center for Vaccinology
Dalhousie University, Halifax NS

Disclosures
In the past 2 years I have been an employee of:
In the past 2 years I have been a consultant of:
In the past 2 years I have held investments in the following pharmaceutical organizations, medical devices companies or communications firms:
In the past 2 years I have been a member of the Scientific advisory board of:
Sanofi Pasteur, Roche, Pfizer
In the past 2 years I have been a speaker for:
In the past 2 years I have received research support (grants) from:
GSK, Pfizer, Sanofi Pasteur
In the past 2 years I have received honoraria from:
I agree to disclose approved and non-approved indications for medications in this presentation:
YES
I agree to use generic names of medications in this presentation:
YES

Acknowledgements
Dr. Paul Van Buynder, CMOH Fraser Health, BC
Dr. Allison McGeer,Mount Sinai Hospital

Objectives
� To review current recommendations for immunization of healthcare workers
� To discuss evidence supporting recommendations for influenza immunization of healthcare workers
� To review strengths and limitations of policies requiring influenza vaccination as a condition of employment for healthcare providers

Current immunization recommendations
Vaccine Schedule Indication Notes
Hepatitis B 3 doses; 0, 1, 6 All HCP Serology 1-6mos post dose 3 to confirm immunity
MMR 2 doses; 4 weeks apart
Non-immune HCP regardless of age
Immunity= proof of vaccine X2, lab confirmed infection, serology
Td Q 10 yrs All HCP
Tdap 1 adult dose All HCP Even if vaccinated in school
Varicella 2 doses; 4 weeks apart
Non-immune HCP Immunity= HCP diagnosis of VZV, proof of vaccine X2, serology

Vaccine Schedule Indication Notes
Influenza (TIV/LAIV)
Annually All HCP TIV preferred in HCP of IC pts; TIV if egg allergic, comorbidity, >59y
Quadrivalentconjugate meningococcal
Q 5 years Lab personnel at risk of exposure
Even if prior MenC-C

Vaccine coverage in Canadian HCP
0
10
20
30
40
50
60
70
Influenza Hepatitis B Tetanus Varicella Pertussis
% H
CP
vaccin
ate
d
2006
2008
http://resources.cpha.ca/CCIAP/data/544e.pdf
Innocence vs Ignorance
N. Wong, Dal Med 2006

When should a public health intervention be mandatory ?
� When the burden of disease is significant
� When there is clear medical value of the intervention to the individual
� When there is clear medical value of the intervention to public health
� When there is no other means to obtain the public health benefit
Wynia Am J Bioethics 2007;7:2-6

Mandates for vaccines
� Entry into countries
� Yellow fever vaccine
� Meningococcal vaccine – Saudi Arabia for the Hajj
� School entry
� Childhood vaccines and public schools
� HepB, MMR, Varicella, TdaP - medical and nursing schools
� Occupational licensure
� Paramedics, some physicians

What do we mean by mandatory in public health?
� A mandate requires that
� Opting out requires more than just saying “no”
� There is an enforcement method, and a consequence
Wynia Am J Bioethics 2007;7:2-6

Enforcement of “mandates”
� None
� Moral suasion
� Signed declination
� Stated philosophical or religious objection
� bureaucratic complexity
� requirement for notarization
� restrictions on religion/philosophy
� Medical contraindications only

When should a public health intervention be mandatory ?
� When the burden of disease is significant
� When there is clear medical value of the intervention to the individual
� When there is clear medical value of the intervention to public health
� When there is no other means to obtain the public health benefit
Wynia Am J Bioethics 2007;7:2-6

Estimates of Canadian influenza mortality burden
Mortality rate/
100,000 pop/yr
# Deaths/y, Canada
Methods
CDC – P&I1976-2007
2.4 700Serfling model, adjusted for influenza and other viral activity
CDC – all1976-2007
9.0 2600Serfling model, adjusted for influenza and other viral activity
Canada1990-1999
13 4000Poisson regression, adjusting for season, viral activity
ONBOIDS2006
2.2 700Epidemiologic studies to estimate contribution of influenza to respiratory infection syndromes
TIBDN2005-2011
1.1 370Laboratory confirmed, hospitalized cases; in-hospital mortality
Thompson MMWR 2010;59:1058; Schanzer Epidemiol Infect 2007;135:1109-16Kwong J www.ices.on.ca/file/ONBOIDS_FullReport_intra.pdf; TIBDN, unpublished

Ontario Burden of Infectious Diseases Study
0 1,000 2,000 3,000 4,000 5,000 6,000 7,000 8,000 9,000 10,000
Gonorrhea
Adenovirus
Chlamydia
Legionella
Tuberculosis
Haemophilus influenzae
Group A streptococcus
Group B streptococcus
Parainfluenza virus
Respiratory syncytial virus
Rhinovirus
Clostridium difficile
Influenza
Staphylococcus aureus
HIV/AIDS
Escherichia coli
Hepatitis B virus
Human papillomavirus
Streptococcus pneumoniae
Hepatitis C virus
HALYs
YLL
YERF
http://www.oahpp.ca/resources/documents/reports/onboid/ONBoID_ICES_Report_ma18.pdf

Traditional measures of influenza BOD
Glezen WP, Keitel WA, Taber LH, et al.
Am J Epidemiol. 1991 Copyright Elsevier

Catastrophic disability
� Defined as a loss of independence in ≥ 3 ADL
� 72% who experience catastrophic disability have been hospitalized
� Leading causes of catastrophic disability
1. Stroke
2. CHF
3. Pneumonia and influenza
4. Ischemic heart disease
5. Cancer
6. Hip fracture
Ferrucci et al. JAMA 277:728, 1997Barker et al. Arch Int Med 158:645, 1998Falsey et al. N Engl J Med. 2005;352:1749
Vaccine Preventable Disability

Impact of influenza on Frailty McNeil, SOS Network, CIC 2012
Influenza Cases
Mean (SD)
Controls
Mean (SD)P value
Baseline 0.24 (.15) 0.24 (.14) 0.98
On admission
0.29 (.16) 0.31 (.16) 0.39
30d post discharge
0.30 (.15) 0.26 (.14) 0.06
Change from baseline
0.06 0.02
- Cases (flu) are left more frail at 30d than controls (increase of .06 or 2.3 new deficits vs 0.02 or 0.8 new deficits)

Acute care hospital-acquired influenza
Incidence3 / 1000 admissions8 / 1000 admissions6 / 1000 admissions
California, 1987Virginia, 1988-94Houston, 1988
Case fatality rate
7 % (0-60%)
Cost/ case$7,545$ 4,050$ 3,622
US, 1990US, 1993US, 2000
Weingarten AIM1988;148:113; Glezen CJIC 1991;6:65; Adal ICHE 1996;17:641; Serwint PIDJ 1993;12:200; Evans AJIC 1997;25:357; Salgado LancetID 2002;2:145

Passive surveillance in TIBDN for acute care hospital-acquired, lab-confirmed influenza, 2005-2011
0
1
2
3
4
5
6
7
8
9
10
2004/5 2005/6 2006/7 2007/8 2008/9 2009/10 2010/11
no
so
co
mia
l L
CI
per
1000 a
dm
issio
ns (
No
v-A
pr)
Season
307 cases & 52 deaths / 7 years~ 30% associated with outbreaks
TPH: 17 ACH outbreaks in 5 years

When should a public health intervention be mandatory ?
� When the burden of disease is significant
� When there is clear medical value of the intervention to the individual
� When there is clear medical value of the intervention to public health
� When there is no other means to obtain the public health benefit
Wynia Am J Bioethics 2007;7:2-6

Efficacy of influenza vaccinehealthy adults
� 59% reduction in PCR confirmed, symptomatic influenza infection
� “breakthrough” illness less severe
Osterholm Lancet ID 2012;12:36

Reduction in illness associated with influenza vaccination, healthy adults� Episodes of ILI: 3-10 per 100 vaccinated
� Sick days: 21-52 per 100 vaccinated
� Antibiotic scripts: ~0.7 per 100 vaccinated
� (with associated adverse events, allergies, CDAD)
� Hospitalization: 1 per 100,000
� ICU admission: 1.2 per 1,00,000
� Death due to influenza: 1 per 3 M annually
� Guillian-Barré syndrome: Nichol NEJM 1995;333: 889-93; Saxen PIDJ 1999;18:779; Wilde JAMA
1999;281:908; Nichol JAMA 1999;282:137;

Influenza, vaccination and GBS
� Sivadon (GBS registry)
� GBS without known etiology occurs predominantly in winter, and preceded by ILI
� 14/234 documented influenza
� Risk GBS post vaccine and ILI, GPRD
Sivadon EID 2006;12:188; Sivadon CID 2009;48:48; Stowe Am J Epi 2009;169:382; Tam PlosOne 2009;e344
Study Odds ratio (95% CI) for GBS
After vaccine After ILI After ARI
Stowes 0.76 (0.41, 1.4) 18.6 (7.5, 46) -
Tam 0.16 (0.02, 1.3) 7.4 (4.4, 13) 5.2 (3.5, 7.6)

Risks of influenza vaccine:healthy adults
� Common
� Sore arm (40%): in 2 missed work days/100 vaccinees
� Less common
� ORS (~1/10,000): ~15% with a MD visit
� Allergic reaction (~1/20,000)
� Uncommon
� Anaphylaxis (1/500,000)
� Guillain Barré Syndrome (1/1,000,000)Nichol NEJM 1995;333: 889-93; Saxen PIDJ 1999;18:779; Wilde JAMA 1999;281:908; Nichol JAMA 1999;282:137; Smith Cochrane 2004, CD000245; Aroll,Keally Cochrane 2005, CD000247; De Serres, personal communication; Skowronski CID 2003;36:705; Price BMJ 2009;339:b3577

Comparison of risks
Vaccine� 9 minutes missed work
� 40% chance of sore arm
� 1 in 5000 chance of allergic reaction
� 1 in 1,000,000 risk of hospitalization (allergy/GBS)
� 1 in 50 million risk of death
No vaccine� 135 minutes missed work
� 33% chance of ARI
� 2 in 100 chance of illness needing antibiotics
� 1 in 100,000 risk of hospitalization due to influenza
� 1 in 3 million risk of death
Nichol et al. JAMA 1999;282:137; Smith et al. Cochrane 2004, CD000245;
Aroll,Keally Cochrane 2005, CD000247; McGeer CID 2007; TIBDN unpublished
information
Neuzil JAMA 1999;281:907

When should a public health intervention be mandatory ?
� When the burden of disease is significant
� When there is clear medical value of the intervention to the individual
� When there is clear medical value of the intervention to public health
� When there is no other means to obtain the public health benefit
Wynia Am J Bioethics 2007;7:2-6

Rates of symptomatic influenza in unvaccinated HCWs
0 5 10 15 20
Keitel
Wakdman
Kumplainen
Feery
Sirivichayakul
Coleman
Total infection rate (ILI, ARI + asymptomatic) : 8-26%

Proportion of LTCF reporting an influenza outbreak by percentage of residents/staff vaccinated
0
20
40
60
<70% 70-90% >90%
Per
cen
t o
f L
TC
Fs
rep
ort
ing i
nfl
uen
za
ou
tbre
ak
Percent of residents vaccinated
P=0.11, Chi-sq for trend
Stevenson CG, et al. CMAJ 2001;164:1413-9
0
10
20
30
40
50
<25% 25-50% 50-75% >75%
Per
cen
t o
f L
TC
Fs
rep
ort
ing
infl
uen
za o
utb
rea
k
Percent of staff vaccinated

Impact of HCP vaccination on patient outcomes (LTCF)� 4 RCTs in long term care facilities
� Potter. J Infect Dis 1997
� 44% ↓ mortality (p<.01)
� Carman. Lancet 2000
� 42% ↓ mortality (p<.01)
� Hayward. BMJ 2006
� 27% ↓ mortality (p<.001)
� Lemaitre. J Am Geriatr Soc 2009
� 20% ↓ mortality (p=.02)

Results, Cochrane review of impact of HCW vaccination on resident outcomes Thomas, Cochrane Database Syst Rev. 2010;(2):CD005187
Outcome Pooled OR (95% CI)
All cause mortality 0.68 (0.55, 0.84)*
ILI 0.71 (0.58, 0.98)*
GP consultation for ILI 0.48 (0.33, 0.69)*
Influenza 0.87 (0.38, 1.99)
*Pneumonia 0.71 (0.29, 1.71)
Hospital admission 0.90 (0.66, 1.21)
Death due to ILI 0.72 (0.31, 1.70)
*Death due to pneumonia
0.87 (0.47, 1.64)Pooled data…found no effect on the outcomes of direct interest. We conclude that there is no evidence from this research that vaccinating healthcare workers against influenza protects elderly people in their care.
*See Dolan et al EID, Aug 2012

What about acute care?

Risk of ILI in ACH during seasonal influenza epidemics, Edouard Herriot Hospital, 2004/5-2006/7 Arch Intern Med 2011; Jan 24

Salgado ICHE 2005;11:923

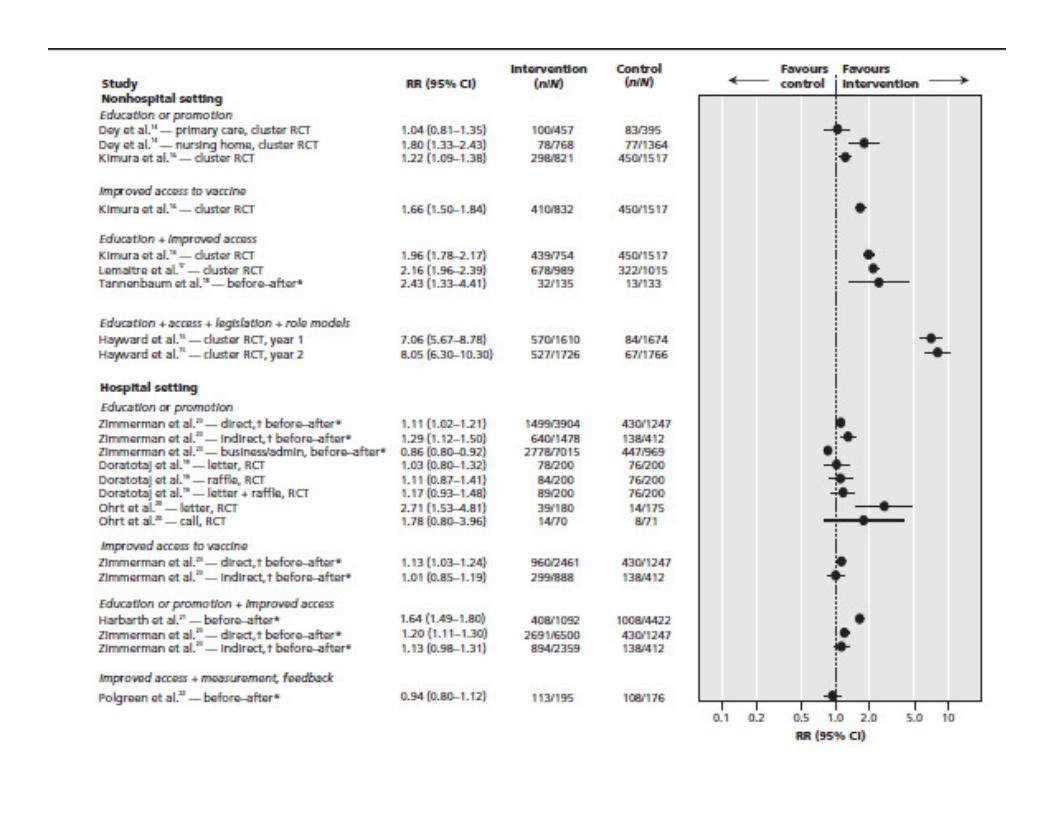
Influenza vaccination of healthcare workers in acute-care hospitals: effect on hospital-acquired influenza among patients
� Nested case-control study
� Cases: patients with laboratory confirmed influenza with onset ≥72 hours after admission
� Controls: patients with HA-ILI, negative for influenza
� 4 controls: case, matched by season
Benet BMCID 2012;12:30
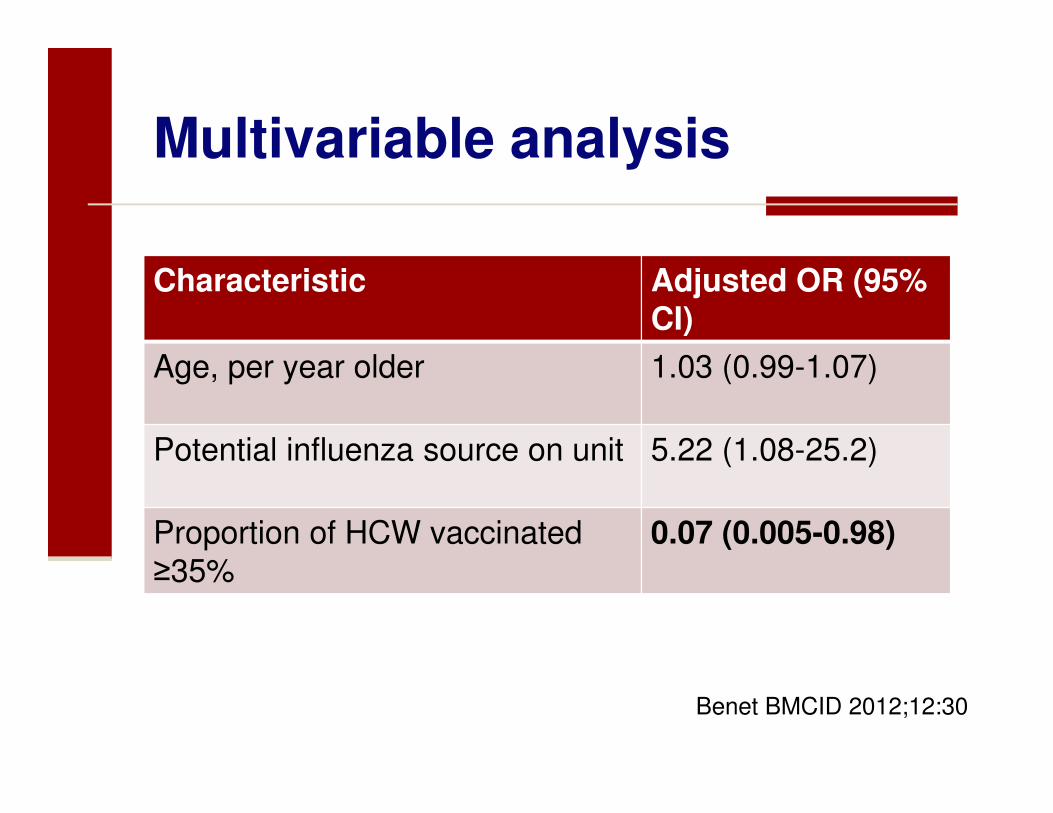
Multivariable analysis
Characteristic Adjusted OR (95% CI)
Age, per year older 1.03 (0.99-1.07)
Potential influenza source on unit 5.22 (1.08-25.2)
Proportion of HCW vaccinated ≥35%
0.07 (0.005-0.98)
Benet BMCID 2012;12:30

Vaccine 2009;27:6261

When should a public health intervention be mandatory ?
� When the burden of disease is significant
� When there is clear medical value of the intervention to the individual
� When there is clear medical value of the intervention to public health
� When there is no other means to obtain the public health benefit
Wynia Am J Bioethics 2007;7:2-6

Improving HCW vaccination ratesHospital Program % vaccinated
Pre Post
Cadena, 2011, 1 hospital
QI methodology: PDSA cycle, with weekly meetings, force-field analysis, cause and effect diagrams, process flow charts, Gantt charts
59 77
Ribner, 20081 hospital
task force, senior management visible support, weekly feedback to managers, T-shirt given out to vaccinees, declination form required
43 67
Rakita, 20111 hospital
Task force, education, on-line modules, champions, incentives
38 54
Ajenjo, 2010Multiple
Education, communication, incentives, feedback, leadership involvement, prizes, competitions, declination forms
45 72
Zimmerman, 2009multiple
Education, communication, incentives, accessibility
32 39
Lopes, 20081 hospital
Education, communication, incentives, accessibility, leadership involvement
6 49

Influenza vaccination rates in participating members of the UHC benchmarking project, 2007

Immunization program elements associated with higher uptake
Component
No. (%) of facilities
with component
(n = 47)
Vaccination rate, mean ± SD, %
P
At facilities with
component
At facilities without
component
Weekend avail 37 (79) 58.8 ± 12.0 43.9 ± 14.9 .01
Train‐the‐trainer programs 33 (70) 59.5 ± 12.5 46.5 ± 13.2 .005
Feedback of vaccination rates provided to administration 10 (21) 63.9 ± 9.7 53.4 ± 14.1 .01
Letter from administration emphasizing importance 33 (70) 59.3 ± 11.9 47.0 ± 15.0 .01
How do you increase staff vaccination rates?

So… does “mandatory” immunization work?

Virginia Mason Medical Center
Rakita ICHE 2010;31:881

VMMC program (cont’d)
� 5 employees resigned, 2 terminated (2005/6)
� 2007-2010: 2 additional employees have left
� Sick leave 7.1 hrs/HCW v. 6.6 hrs/HCW (P=.43)
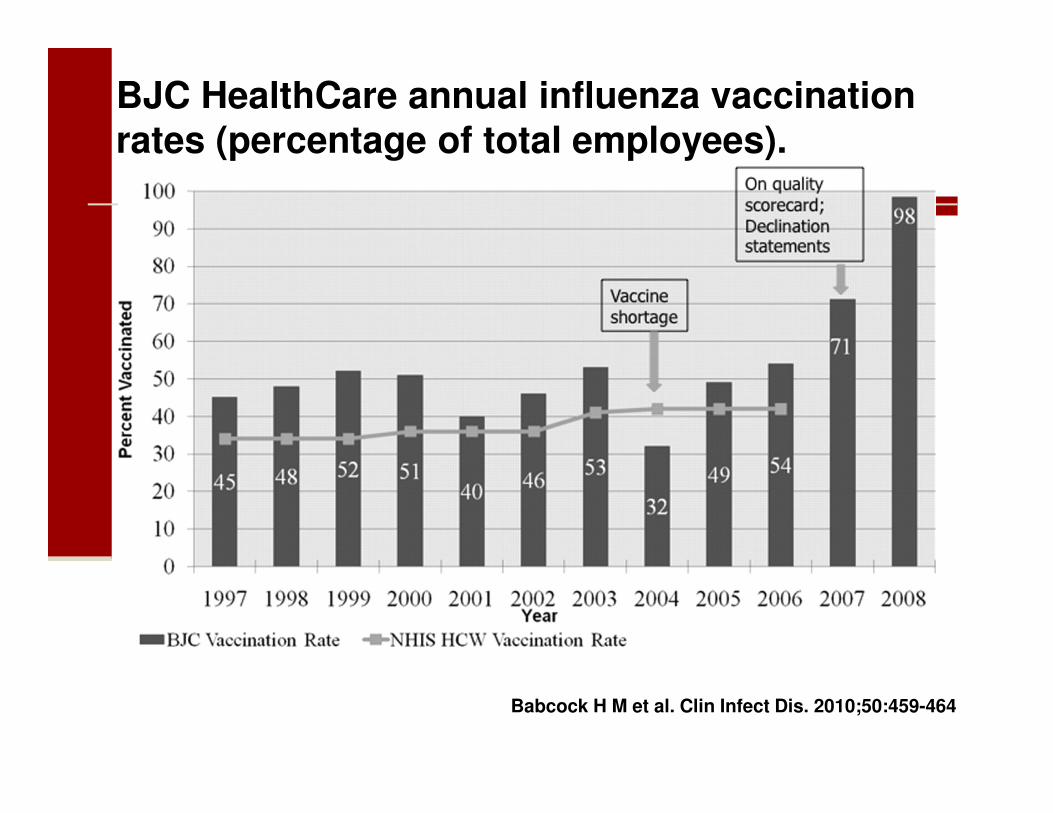
BJC HealthCare annual influenza vaccination rates (percentage of total employees).
Babcock H M et al. Clin Infect Dis. 2010;50:459-464

Other published experience
� HCA Inc (163 hospitals)
� Septimus JAMA 2011;305:999
� MedStar (9 hospitals)
� Karanfil ICHE 2011;32:375
� GHS (2 hospitals)
� Esolen ICHE 2011;32:703
� CHOP (1 hospital)
� Feemster Vaccine 2011;29:1762

Broad endorsement of immunization as a condition of employment

Distribution of institutional requirements for influenza vaccination, US hospitals, 2010/11 season
359, 46%
246, 32%
29, 4%
143, 18%
0, 0%
Vaccination not required
Vaccination required, noconsequences
Vaccination required(termination
Vaccination required,mask
Vaccination required,other
Proportion of hospitals with requirements and consequences for vaccine refusal increased from 5% (N=37) in 2007/8 to 25% (N=183) in 2010/11
Miller CID 2011;53:1051; Miller Vaccine2011;29:9398

Change in vaccination rate associated with institutional requirement, by consequences associated with refusal, US hospitals, 2007-11
0
10
20
30
40
50
60
70
80
90
100
Termination Other consequence No consequence
Percent HCW vaccinated
Pre
Post

What is happening in Canada?

Mandatory Influenza Immunization of HCWPosition paper 2012
Annual influenza immunization should be required as a condition of new and on-
going employment or appointment for all workers who spend time in areas where patient care is provided and/or patients
are present.


Annual influenza vaccination should be a condition of continued employment in, or appointment to, health care organizations.
HCW with medical contraindications should be accommodated by
reassignment, or other methods used to protect patients and staff (eg masks)
during influenza season.
Best Practices for Infection Prevention and Control Programs in Ontario, Third Revision, May 2012

British Columbia
� Fall 2012 HCW in BC must be vaccinated
against influenza as a condition of service
� If unable/unwilling must wear a mask
� throughout influenza season
� while in facilities where patient care is given
� includes physicians, RNs, students, volunteers
and contracted workers
� regardless of reason for not immunizing

BC so far….
� Policy implemented Fall 2012
� Nov. 30, 2012 MOH announced that no discipline would be enforced this year to allow further consultation
� Despite this, coverage of 73% of FT staff achieved by Nov. 30

Words of wisdom…..
“The American experience with mandatory (flu vaccination) is that it is not a hill you die on. It's a hill
that actually vanishes when you
start climbing it.”
-A. McGeer, Canadian Press 3/25/13
“There are risks and costs to a program of action. But they are far less than the long-range risks and costs of
comfortable inaction.”- John F. Kennedy

Why vaccinate healthcare providers?