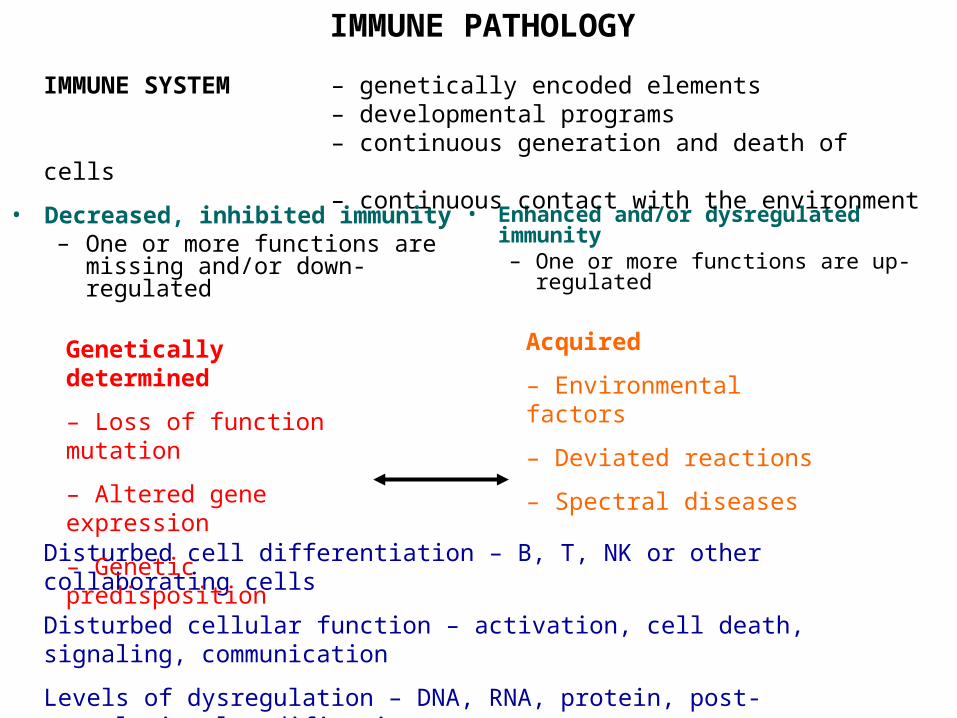
IMMUNE PATHOLOGY Decreased, inhibited immunity –One or more functions are missing and/or...
15
IMMUNE PATHOLOGY • Decreased, inhibited immunity – One or more functions are missing and/or down- regulated • Enhanced and/or dysregulated immunity – One or more functions are up- regulated Disturbed cell differentiation – B, T, NK or other collaborating cells Disturbed cellular function – activation, cell death, signaling, communication Levels of dysregulation – DNA, RNA, protein, post- translational modification, IMMUNE SYSTEM – genetically encoded elements – developmental programs – continuous generation and death of cells – continuous contact with the environment Genetically determined – Loss of function mutation – Altered gene expression – Genetic predisposition Acquired – Environmental factors – Deviated reactions – Spectral diseases
-
Upload
madeleine-moore -
Category
Documents
-
view
218 -
download
0
Transcript of IMMUNE PATHOLOGY Decreased, inhibited immunity –One or more functions are missing and/or...
IMMUNE PATHOLOGY
• Decreased, inhibited immunity– One or more functions are missing
and/or down-regulated
• Enhanced and/or dysregulated immunity– One or more functions are up-regulated
Disturbed cell differentiation – B, T, NK or other collaborating cells
Disturbed cellular function – activation, cell death, signaling, communication
Levels of dysregulation – DNA, RNA, protein, post-translational modification, secretory function etc.
IMMUNE SYSTEM – genetically encoded elements– developmental programs– continuous generation and death of cells – continuous contact with the environment
Genetically determined
– Loss of function mutation
– Altered gene expression
– Genetic predisposition
Acquired
– Environmental factors
– Deviated reactions
– Spectral diseases
THE IMMUNE RESPONSE TO PATHOGENS

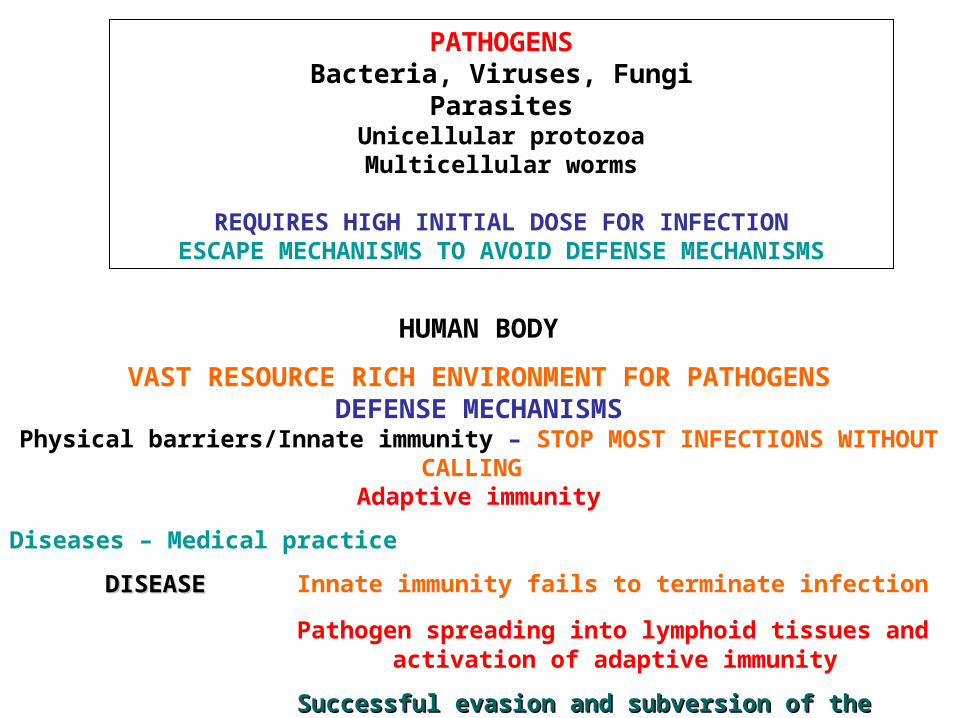
PATHOGENSBacteria, Viruses, Fungi
ParasitesUnicellular protozoaMulticellular worms
REQUIRES HIGH INITIAL DOSE FOR INFECTIONESCAPE MECHANISMS TO AVOID DEFENSE MECHANISMS
HUMAN BODY
VAST RESOURCE RICH ENVIRONMENT FOR PATHOGENSDEFENSE MECHANISMS
Physical barriers/Innate immunity – STOP MOST INFECTIONS WITHOUT CALLING Adaptive immunity
Diseases – Medical practice
DISEASEDISEASE Innate immunity fails to terminate infection
Pathogen spreading into lymphoid tissues and activation of adaptive immunity
Successful evasion and subversion of the immune Successful evasion and subversion of the immune system by pathogenssystem by pathogens
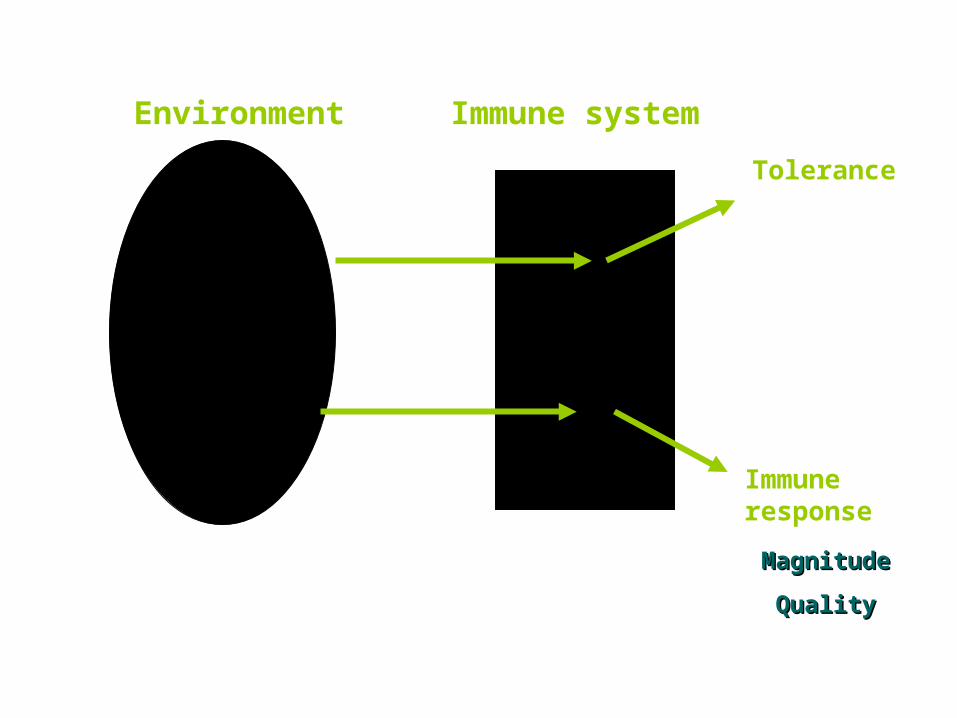
Environment
SELF
NON-SELF
Destructive SELF
Immune system
Tolerance
Immune response
MagnitudeMagnitude
QualityQuality
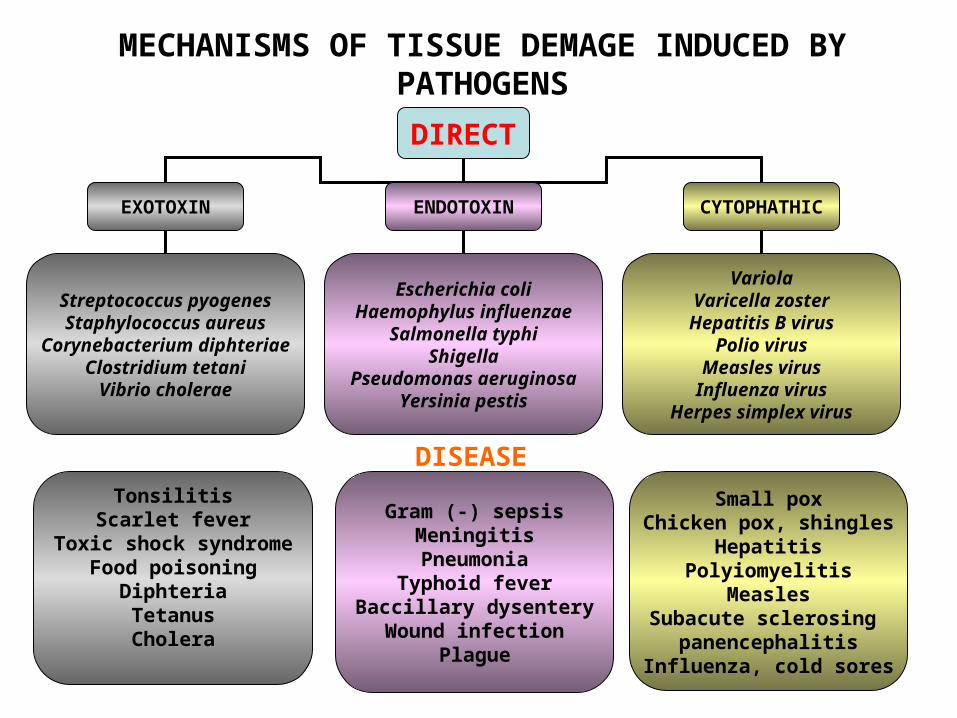
DIRECT
EXOTOXIN ENDOTOXIN CYTOPHATHIC
Streptococcus pyogenesStaphylococcus aureus
Corynebacterium diphteriaeClostridium tetani
Vibrio cholerae
Escherichia coliHaemophylus influenzae
Salmonella typhiShigella
Pseudomonas aeruginosaYersinia pestis
VariolaVaricella zosterHepatitis B virus
Polio virusMeasles virusInfluenza virus
Herpes simplex virus
TonsilitisScarlet fever
Toxic shock syndromeFood poisoning
DiphteriaTetanusCholera
Gram (-) sepsisMeningitisPneumonia
Typhoid feverBaccillary dysentery
Wound infectionPlague
Small poxChicken pox, shingles
HepatitisPolyiomyelitis
MeaslesSubacute sclerosing
panencephalitisInfluenza, cold sores
MECHANISMS OF TISSUE DEMAGE INDUCED BY PATHOGENS
DISEASE
CYTOPATHIC – CYTO-PROLIFERATIVE INFLAMMATIONAcute and chronic inflammation
Death of individual cells
No or weak host – mediated inflammation
Virus inclusion bodies – CMV, adenovirus, Ebola
Fused multinucleated cells
Modification and proliferation of epithelial cells
Epithelial and lymphoid dysplasia – tumorigenic viruses
INFLAMMATORY RESPONSES TO INFECTIOUS AGENTS
NECROTIZING INFLAMMATION Toxin – mediated lesions
Clostridium, HBV-infected hepatocytes, HHV neurons
CHRONIC INFLAMMATION HBV cirrhosis in liver Schistosoma – fibrosis in liver
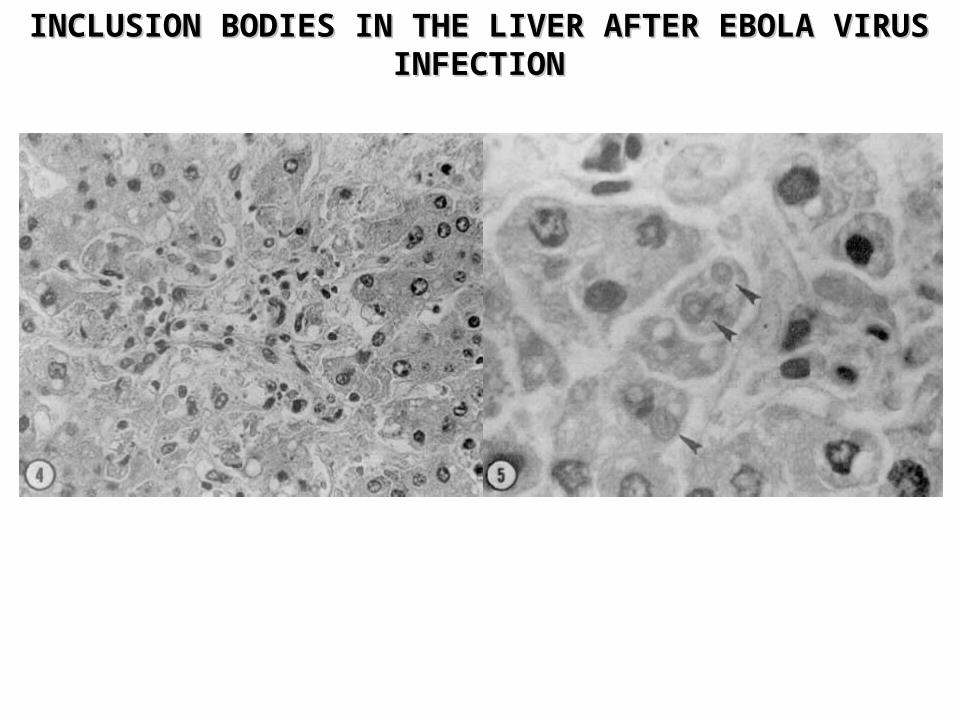
INCLUSION BODIES IN THE LIVER AFTER EBOLA VIRUS INCLUSION BODIES IN THE LIVER AFTER EBOLA VIRUS INFECTIONINFECTION
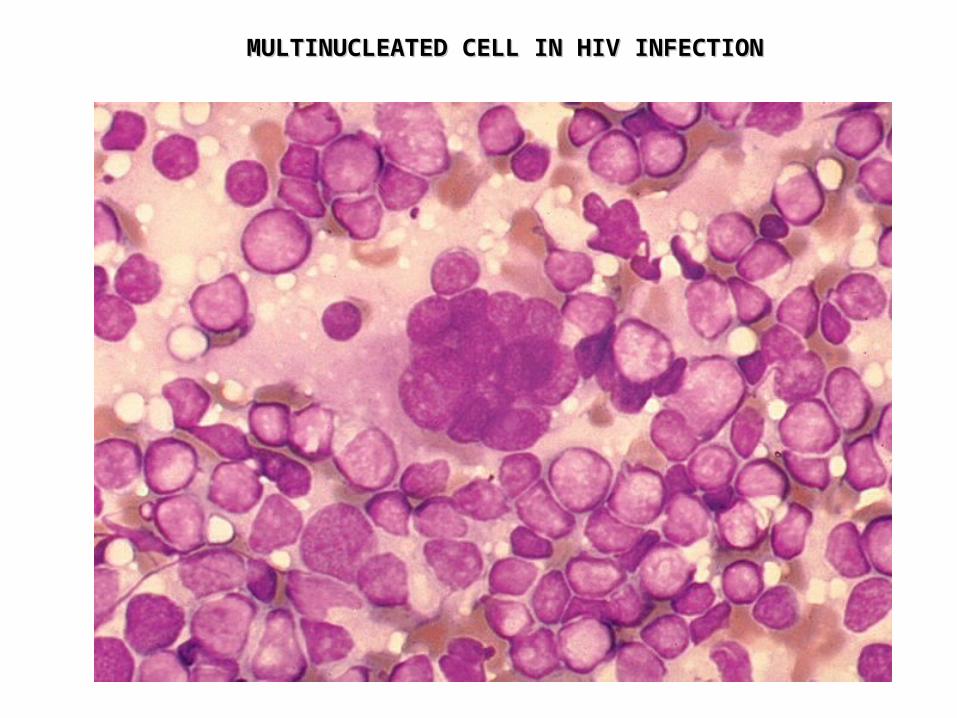
MULTINUCLEATED CELL IN HIV INFECTIONMULTINUCLEATED CELL IN HIV INFECTION
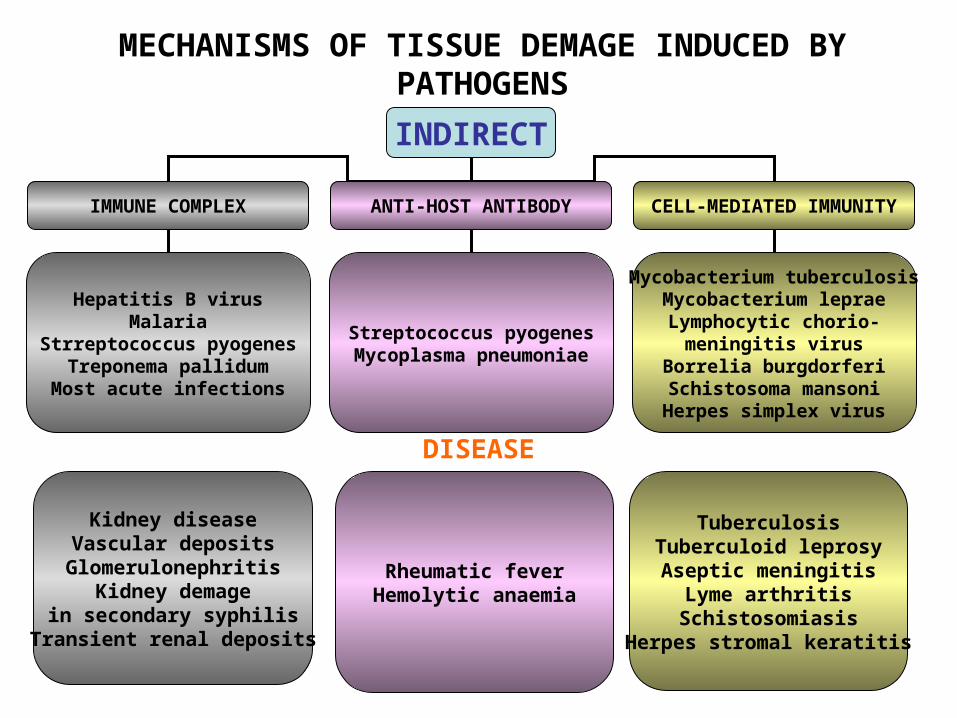
INDIRECT
IMMUNE COMPLEX ANTI-HOST ANTIBODY CELL-MEDIATED IMMUNITY
Hepatitis B virusMalaria
Strreptococcus pyogenesTreponema pallidumMost acute infections
Streptococcus pyogenesMycoplasma pneumoniae
Mycobacterium tuberculosisMycobacterium lepraeLymphocytic chorio-
meningitis virusBorrelia burgdorferi
Schistosoma mansoniHerpes simplex virus
Kidney diseaseVascular deposits
GlomerulonephritisKidney demage
in secondary syphilisTransient renal deposits
Rheumatic feverHemolytic anaemia
TuberculosisTuberculoid leprosyAseptic meningitis
Lyme arthritisSchistosomiasis
Herpes stromal keratitis
MECHANISMS OF TISSUE DEMAGE INDUCED BY PATHOGENS
DISEASE
INFLAMMATORY RESPONSES TO INFECTIOUS AGENTS
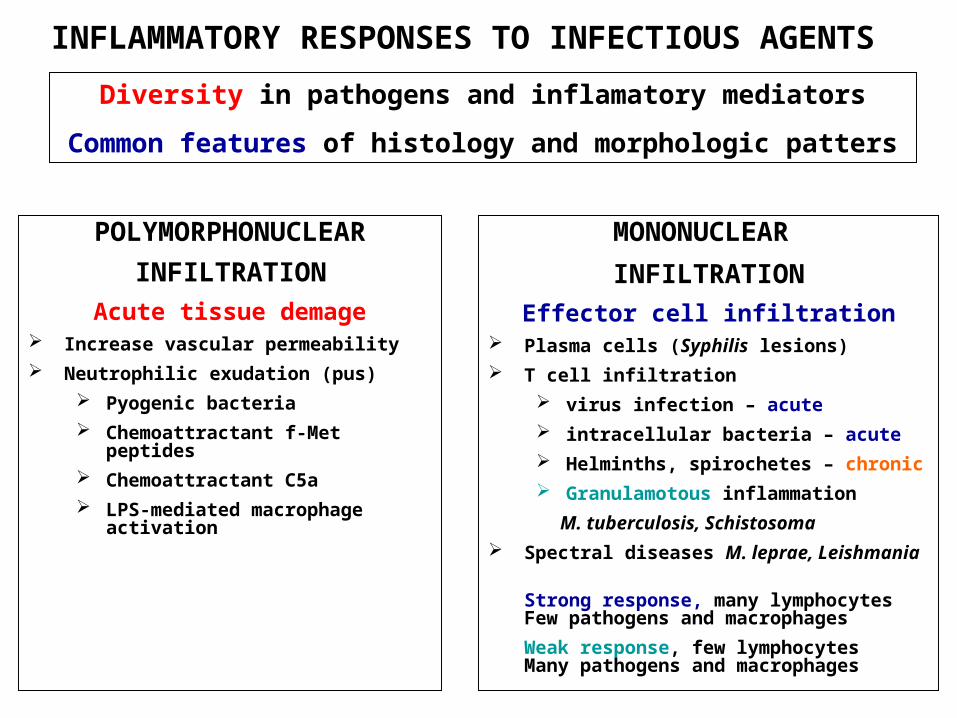
Diversity in pathogens and inflamatory mediators
Common features of histology and morphologic patters
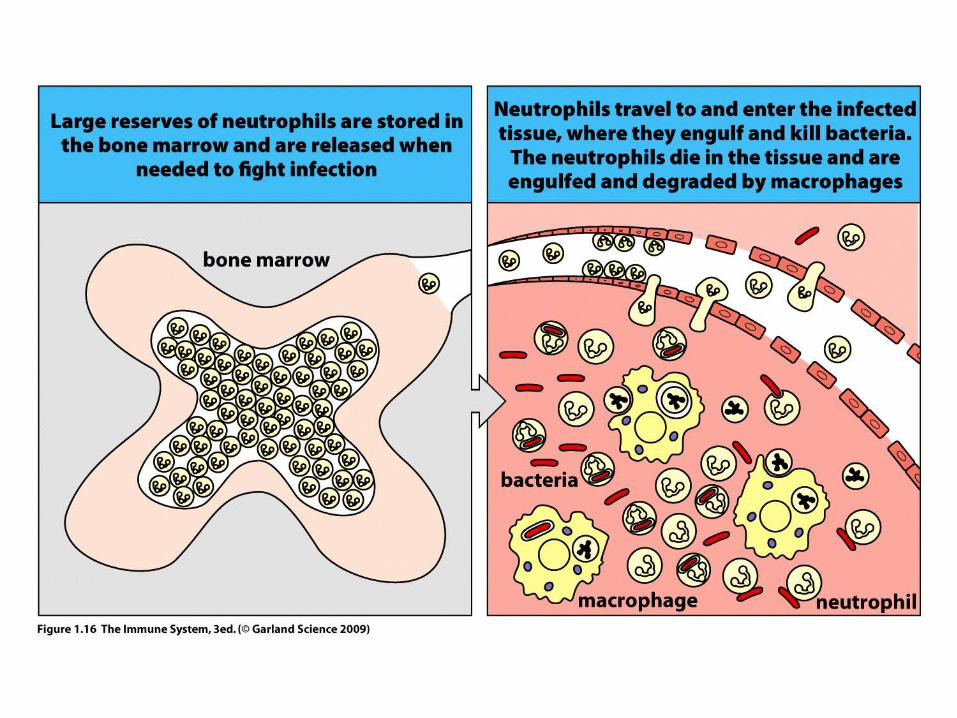
POLYMORPHONUCLEAR
INFILTRATION
Acute tissue demage Increase vascular permeability
Neutrophilic exudation (pus)
Pyogenic bacteria
Chemoattractant f-Met peptides
Chemoattractant C5a
LPS-mediated macrophage activation
MONONUCLEAR
INFILTRATION
Effector cell infiltration Plasma cells (Syphilis lesions)
T cell infiltration
virus infection – acute
intracellular bacteria – acute
Helminths, spirochetes – chronic
Granulamotous inflammation
M. tuberculosis, Schistosoma
Spectral diseases M. leprae, Leishmania
Strong response, many lymphocytesFew pathogens and macrophages
Weak response, few lymphocytesMany pathogens and macrophages
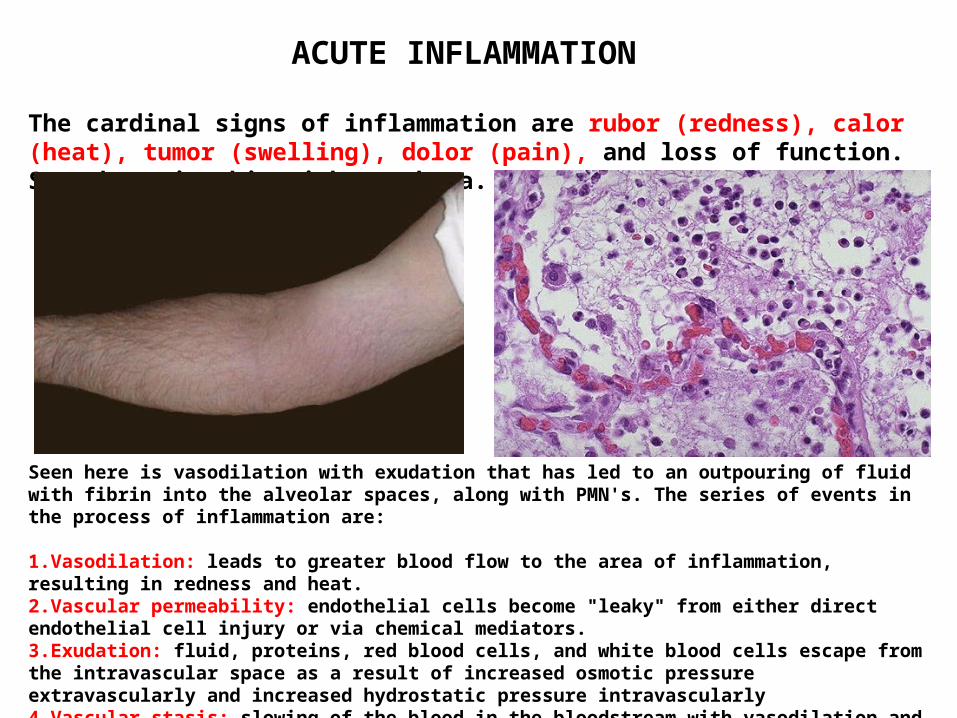
Seen here is vasodilation with exudation that has led to an outpouring of fluid with fibrin into the alveolar spaces, along with PMN's. The series of events in the process of inflammation are:
1.Vasodilation: leads to greater blood flow to the area of inflammation, resulting in redness and heat.2.Vascular permeability: endothelial cells become "leaky" from either direct endothelial cell injury or via chemical mediators.3.Exudation: fluid, proteins, red blood cells, and white blood cells escape from the intravascular space as a result of increased osmotic pressure extravascularly and increased hydrostatic pressure intravascularly4.Vascular stasis: slowing of the blood in the bloodstream with vasodilation and fluid exudation to allow chemical mediators and inflammatory cells to collect and respond to the stimulus.
The cardinal signs of inflammation are rubor (redness), calor (heat), tumor (swelling), dolor (pain), and loss of function. Seen here is skin with erythema.
ACUTE INFLAMMATION
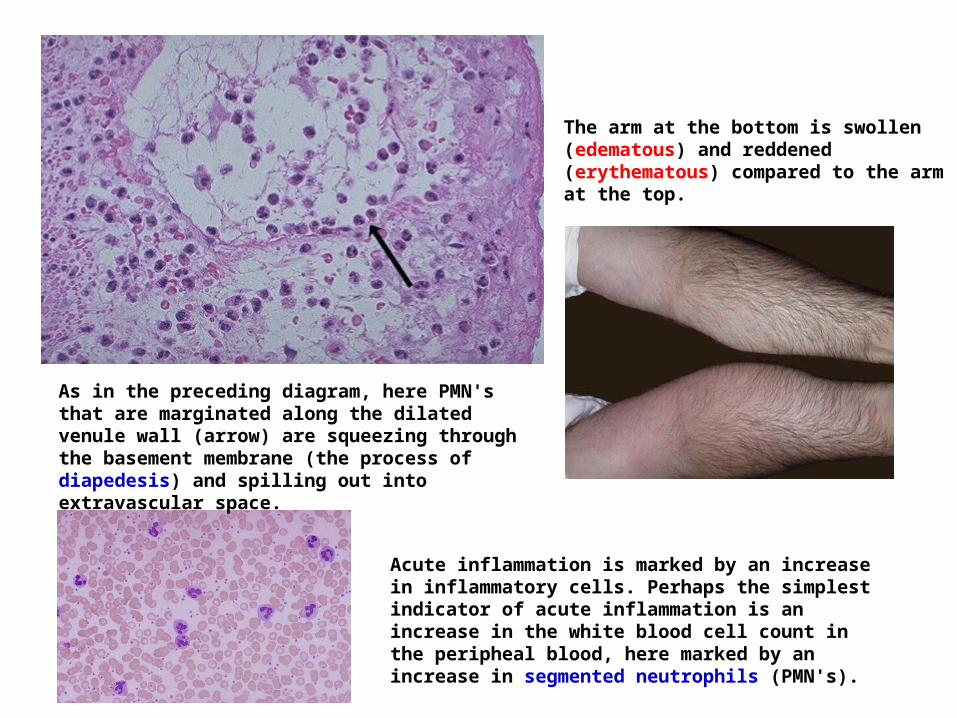
The arm at the bottom is swollen (edematous) and reddened (erythematous) compared to the arm at the top.
Acute inflammation is marked by an increase in inflammatory cells. Perhaps the simplest indicator of acute inflammation is an increase in the white blood cell count in the peripheal blood, here marked by an increase in segmented neutrophils (PMN's).
As in the preceding diagram, here PMN's that are marginated along the dilated venule wall (arrow) are squeezing through the basement membrane (the process of diapedesis) and spilling out into extravascular space.