(IMCI) Integrated Management of Childhood Illness
34
description
Integrated Management of Childhood Illness in the Philippines
Transcript of (IMCI) Integrated Management of Childhood Illness


~-~~~~U1l~l1lJt~-'''''lJJ~lJJ-'lJJ~iJJ~~~
SICK CHILD AGED 2 MONTHS TO 5 YEARS- -~-
ASSESS AND CLASSIFY THE SICK CHILD
Assess, Classify, and Identify the TreatmentCheck for General Danger Signs ..................Then Ask About the Main Symptoms:
Does the child have cough or difficult breathing? 2Doesthe childhavediarrhea? 3 .
Does the child have fever? 4Classify malaria 4Classify measles 4Classify dengue 4
Does the child have an ear problem? 5Then Check for Malnutrition and Anemia 6Then Check the Child's Immunization Status 6Then Check the Child's Vitamin A Status 6Assess Other Problems 6
TREA T THE CHILD
Teach the Mother How to Give Oral Drugs at HomeOral Antibiotics.Oral AntimalarialParacetamolVitamin AIron .........Mebendazole
Teach the Mother How to TreatLocal Infections at Home
Treat Eye Infection with Tetracycline Eye Ointment 9Dry the Ear by Wicking 9Treat Mouth Ulcers with Gentian Violet 9Soothe the Throat and Relieve Cough with
a Safe Remedy
Give These Treatments in the Health Center OnlyIntramuscular Antibiotic 10Quinine for Severe Malaria 10Prevent Low Blood Sugar 11
--- ~-
TREAT THE CHILD, continued
2Give Extra Fluid for Diarrhea and Continue Feeding
Plan A: Treat Diarrhea at Home 12
Plan B: Treat Some Dehydration with ORS 12Plan C 13
Immunize Every Sick Child, as Needed 13Give Every Sick Child Vitamin A, as Needed 13
788888
Give Follow-up CarePneumonia 14Persistent Diarrhea , 14Dysentery 14Malaria 15
Fever: Malaria Unlikely 15Fever: No Malaria 15Measles with Eye or Mouth Complications 16Fever: Dengue Hemorrhagic Fever Unlikely 16Ear Infection 16Feeding Problem 17Anemia 17Very Low Weight 17
COUNSEL THE MOTHER
Food
Assess the Child's FeedingFeeding RecommendationsCounsel about Feeding Problems
Fluid
Increase Fluid during Illness9
When to ReturnAdvisethe MotherWhento Returnto the HealthWorker
Counsel the Mother about Her Own Health 22
SICK YOUNG INFANTAGED 1 WEEK TO 2 MONTHSASSESS, CLASSIFY, AND TREAT THE SICK YOUNG INFANT
Assess, Classify, and Identify the TreatmentCheck for Possible Bacterial Infection 23
Then Ask: Does the Young Infant have Diarrhea? 24Then Check for Feeding Problems or Low Weight 25Check the Young Infant's Immunization Status 26Assess Other Problems 26
Treat the Young Infant and Counsel the MotherOral Antibiotics 27Intramuscular Antibiotics 27To Treat Diarrhea, See TREAT THE CHILD Chart 28Immunize Every Sick Young Infant, as Needed 28Treat Umbilical Infections in the Health Center 28Treat Local Infections at Home 28Correct Positioning and Attachment for Breastfeeding 29Home Care for the Young Infant 29
Give Follow-up Care for the Sick Young InfantLocal Bacterial InfectionFeeding ProblemLow WeightThrush
30313131
181920
RECORDING FORMSSICK YOUNG INFANTSICK CHILD
3353
WEIGHT-FOR-AGE CHART on the back cover
21 -'- ~ ~ n8
eftlfi~~ .1. ~WORLD HEALTH U IC
..
.~I 11 ORGANIZATION
~ '"",,',:' i""4"'~'"Association of Deans t"""
of Philippine Colleges . "
.of Nursing,Inc. . .'. .'
~.DEPARTMENTOF HEALTHRepublicof the Philippines ECD Project
21

2
ASSESS AND CLASSIFY THE SICK CHILD AGED 2 MONTHS UP TO 5 YEARS
ASSESS CLASSIFY IDENTIFYTREATMENT
ASK THE MOTHER WHAT THE CHILD'S PROBLEMS ARE
Determine if this is an initial or follow-up visit for this problem.if follow-up visit, use the follow-up instructions on the TREAT THE CHILD chart.
if initial visit, assess the child as follows:
USE ALL BOXES THAT MATCH THECHILD'S SYMPTOMS AND PROBLEMS TO
CLASSIFY THE ILLNESS.
ASK:. Is the child not able to drink orbreastfeed?. Does the child vomit everything?. Has the child had convulsions? (during the present illness)
LOOK:. See if the child is abnormally
sleepy or difficult to awaken.
IF YES, ASK:. For how long?LOOK, LISTEN:. Count the breaths in one minute.
}. Look for chest indrawing.
. Look and listen for stridor.
CHILDMUSTBE CALM.
AnYr&£e1'l e raJsignor .. Chestlndrawing ~(
. Stridor';i'nc~lmcbll:Q "..
~ Givefirsl dqse of anapprop~ Give VitarhjJt A.
~ Treatthe;~hildtopre.;erillo~ Refer URG~TL Y to hQ$pita
. Fastbreathing PNEUMONIA ~ Give an appropriate antibiotic for 5 days.~ .Soothe the throat and relieve the cough with
a safe remedy.~ Advise mother when to return immediately.~ Follow up in 2 days.
If the child is:2 months up to 12 months old
12 months up
Fast breathing is:. 50 breaths per minute or more
. 40 breaths per minute or more. No signs of pneumonia
or very severedisease.
NO PNEUMONIACOUGH OR COLD
~ If coughing for more than 30 days, refer forassessment.
~ Soothe the throat and relieve the cough withsafe remedy.
~ Advise mother when to return immediately.
~ Follow up in 5 days if not improving.
\7fiJ {ij'j! ~J R'J ",'J 'T{'I Ilf'l 'ff'J 'if' I ~"'I ff.j Pf'J R'J ft') fi" fT'J . ff'! ~J rfiJ frl fj'l

-., ---,II---"II--'I~--, "1--'''--, "1"""~ ,~--t.~-"-,1""'" II, , , ,."""~-"II-' , ,~-
.I.J ~ £JI ~ UI III ~ UW Uu ~ It UJ UJ ~ 1;1 fA (jt LJ ~ ~
Does Jhe child have diarrhea?
IF YES, ASK: LOOK AND FEEL: forDEHYDRATION. Forhowlong? . Lookat thechild'sgeneralcondition.
Is the child:
- Abnormally sleepy or difficult toawaken?
- Restlessand irritable?
. Is there blood inthestool?
. Lookforsunkeneyes.Twoof the followingsigns:. Restless,irritable.Sunkeneyes. Drinks eagerly, thirsty. Skinpinchgoesback
veryslowly
SOMEDEHYDRATION
. Offerthe childfluid. Is the child:- Notabletodrinkor drinkingpoorly?- Drinkingeagerly,thirsty?
. Pinchtheskinoftheabdomen.Doesitgoback:- Veryslowly(longerthan2 seconds)?- Slowly?
. Not enough signs toclassify as some orseveredehydration
NODEHYDRATION
. Dehydrationpresent
II
. No dehydration PERSISTENTDIARRHEA
and if bloodin stool
. Blood in the stool DYSENTERY
*If referral is not possible, manage the child as described in Management of Childhood Illness, Treat the Child,Annex: Where Referral is Not Possible, and WHO guidelines for inpatient care.
3DANGER SIGNS, COUGH,
DIARRHEA
ASSESS AND CLASSIFY_LY, FEVER: NO MALARIA .,~\;I"E:~VIVIIVIE:I'\IU/"\IIVI';:>
3SESSAND CLASSIFYAT FOLLOW-UP UNSEL THE MOTHERs
~ Givefluid andfoodfor somedehydration(PlanB).~ If child also has another severe classification:
- ReferURGENTLYto hospital, with mother givingfrequent sips of ORSon the way.
- Advise mother to continue breastfeeding.~ Advisethe motherwhento returnimmediately.~ Followup in 5 days if not improving.
~ Givefluid and foodto treatdiarrheaat home(PlanA).~ GiveZincsupplements.~ Advisemotherwhento returnimmediately.~ Followupin 5 daysif not improving.
~ Treatdehydrationbeforereferralunlessthe child hasanothersevereclassification.
~ GiveVitamin A.~ ijf!fer to hospital.
~ Advise the mother on feeding a child who hasPERSISTENTDIARRHEA.
~ Give Vitamin A.~ Followup in 5.days.~ Advisemotherwhento returnimmediately.
~ Treat for 5 days with an oral antibioticrecommended for Shigella in your area.
~ Follow up in 2 days.
~ Advise motherwhen to return immediately.
,OIVII~;:>
FOllOW-UP

4
THEN ASK: Does the child have feve.r?(by history, or feels hot Or if temperature is 37.5°C** or abov~)
Decide Malaria Risk
Ask:. Does the child live in a malaria area?. Has the child visited/travelled or stayed overnight in a malaria area
in the past 4 weeks?
If Yes to either, obtain a blood smear.THEN ASK: LOOK AND FEEL:. Forhowlong hasthechild had' Lookor feel for stiff neck.
fever? . Lookfor runny nose.. If more than 7 days, has thefever beenpresenteveryday?. Has the child had measleswithin the last 3 months?
. Lookfor signsof MEASLES:- Generalrashesand- One of these: cough, runny
nose, or redeyes
.If the child has measles now orwithin the last three months:
. Lookfor mouthulcers.Are they deepand extensive?. Lookforpusdrainingfromtheeyes.. Lookfor cloudingof thecornea.
.. .......Assess DengueHemorrhagic FeverASK: LOOKAND FEEL:. Hasthe childhadany bleeding' Look for bleeding from nose or
fromthenoseor gums,or inthe gums.vomitusor stools? . Look for skin petechiae.. Hasthe child hadblack . Feel for cold and clammyvomitus? extremities.
. Hasthe child hadblack . Check for slow capillary refill. Ifstools? noneof theaboveASK,LOOK,and
. Hasthe child had persistent FEELsignsare present& the childabdominalpain? is 6 monthsor older &fever present. Has the childhad persistent for morethan 3 days.vomiting? . Performthe tourniquettest.
MalariaRisk(including travelorovernightstay inmalariaarea)
NoMalariaRisk
Assess DENGUEHemorrhagic Fever
. Bloodsmear(+)If bloodsmearnotdone:. NOrunnynose,andNOmeasles,andNOothercausesof fever
. Bloodsmear(-)or. Runnynoseor. Measlesor. Othercausesoffever
. Nosignsof averyseverefebriledisease
. Cloudingof the corneaor
. Deepor extensi~emouthulcers. Anydangersign
. Pusdrainingfromthe eye or. Mouthulcers
. Measlesnow or within thelast 3 months
. Bleedingfromnoseor gumsor. Bleedinginstoolsor vomitusor. BlackIIItoolsor vomitusor. S~inpetechiaeor. Coldandclammyextremitiesor. Capillaryrefillmorethan3 secondsor. Persistentabdominalpainor. Persistentvomitingor. Tourniquettest positive
. No signsofseveredengueilemorrhaglcfever
MALARIA
FEVER:MALARIAlINLIKELY
VERYSEVEREFEBRILEDISEASE
FEVER:NO MALARIA
aSEVERE,
COMPLICATEDMEASLES***
MEASLESWITHEYEOR MOUTH
COMPLICATIONS'"
MEASLES
SEVEREDENGUE
HEMORRHAGICFEVER
FEVER:DENGUEHEMORRHAGIC
FEVERUNLIKELY
~ Treatthe child with an oral antimalarial. ,~ Giveonedoseof paracetamolin healthcenterfor high fever (38.5°Cor above).~ Advisemotherwhento returnimmediately.~ Followup in 2daysif fever persists.~ If fever is presenteverydayfor morethan7 days,referfor assessment.
~ Giveonedoseof paracetamolin health centerfor high fever(38.5°cor above).~ Advisemotherwhento returnimmediately.~ Followup in 2 daysif feverpersists.~ If feveris presenteverydayfor morethan7days,referfor assessment.~ Treatothercausesof fever.
~ Giveonedose of an appropriateantibiotic. a~ Treatthe child to prevent low blood sl1gar.~ Giveonedoseof par.acetamolin healthcenterfor high fever (38.5°cor above).~ Refer URGENTLYto hospital.
~ Giveonedoseof paracetamolin health centerfor high fever(38.5°cor above).~ Advisemotherwhento returnimmediately.~ Followup in 2 daysif the feverpersists.~ If feveris presenteverydayfor morethan7 days,referfor assessment.~ Treatothercausesof fever. ~
~ Give VitaminA.~ Give first dose of an appropriate antibiotic.~ If clouding of the cornea or pus draining from the eye, apply tetracycline
eye ointment.~ Refer URGENTLYto hospital.
~ Give Vitamin A.~ If pus draining from the eye, apply tetracycline eye ointment.~ If mouthulcers, teachthe mother to treatwith gentian "iolet.~ Followup in 2 days.~ Advise motherwhen to return immediately.
~ Give Vitamin A.~ Advise motherwhen to return immediately.
~ If persistent vomiting or persistent abdominal pain or skin petechiae orpositive tourniquet test are the only positive signs, give ORS(Plan B).
~ If any other signs of bleeding is positive, give fluids rapidly, as in Plan C.~ Treat the child to prevent low blood sugar.~ Refer all children URGENTLYto hospital.~ DO NOTGIVEASPIRIN.
~ Advise motherwhen to return immediately.~ Followup in 2 days if fever persistsor childshowssignsof bleeding.~ DO NOTGIVEASPIRIN.
* If referral is not possible, see manage the child as described in Management of Childhood Illness, Treat the Child, Annex: When Referral is Not Possible, and WHO guidelines for inpatient care.** These temperatures are based on axillary temperature. Rectal temperature readings are approximately a.5°C higher.
*** Other important complications of measles-pneumonia, stridor, diarrhea, ear infection, and malnutrition-are classified in other tables.
~ ~ ,~ ~ ~.t\1I11 ~ ~ ~ ~ ~ ¥f ~ ~ Jf¥ ~ ff f1¥f Iff ~~

~ lli ill Ijj w II . -1 I-;~~~1:-1."~'--" "~"~"'--'~~-:.~-'~l--r.~-~ L.u W LUW ,Jj LlJ W LlJ UJ tlJ LU W LL LU W
Other Causes of Fever:. pneumonia. dysentery. severecomplicatedmeasles. measleswith eye or mouthcomplications. measles
. severe dengue hemorrhagic fever. mastoiditis. acute ear infection
. abscess, cellulites, osteomyelites
. severe pneumonia or very severe disease
5
FEVER, MALARIA,MEASLES, EAR PROBLEM
_I, r-I:.VI:.K: I'IV MALAKI'" ,~'" I"\I:.I."UIVIIVII:.I'IIU1"\IIVh;:>
,~FOLLOW-UP
3SESS AND CLASSIFYFOLLOW-UP.AT
UNSEL THE MOTHER

UJ ~ w---lJil1L1l1l1u;/JJIJ;/1I1;t1I1I1[1I1t1(1~
TREAT THE CHILDCARRY OUT THE TREATMENT STEPS IDENTIFIED ON THE ASSESS AND CLASSIFY CHART
MOTHER TO GIVE ORAL
~
[
MALNUTRITIONandANEMIA,IMMUNIZATIONAND VITAMINA STATUS
ANTIBIOTICS
, _LY, FEVER: NO MALARIA
TREAT FOLLOW-UP"
Give an Appropriate Oral Antibiotics~ FOR PNEUMONIA, ACUTE EAR INFECTION, VERY SEVERE DISEASE, MASTOIDITIS:
FIRST-LINEANTIBIOTIC COTRIMOXAZOLESECOND-LINE ANTIBIOTIC: AMOXYCILLIN
FOR DYSENTERY:
Give antibiotic recommended for Shigella in your area for 5 days.FIRST-LINE ANTIBIOTIC FOR SHIGELLA. COTRIMOXAZOLESECOND-LINE ANTIBIOTIC FOR SHIGELLA NALIDIXIC ACID
~ FOR CHOLERA:
Give an antibiotic recommended for Cholera in your area for 3 days.FIRST-LINEANTIBIOTIC FOR SHIGELLA TETRACYCLINESECOND-LINE ANTIBIOTIC FOR SHIGELLA COTRIMOXAZOLE
7
.~ 1"\E:I."UIVIIVIE:I'IIU/,\IIVI"v .CIVllv,:))SESS AND CLASSIFY
FOLLOW-UPJNSEl THE MOTHER
COTRIMOXAZOLE AMOXYCILLIN(trimethoprim + sulphamethoxazole) Give three times
Give two times daily for 5 days. dailyfor 5 days.AGE OR WEIGHT
ADULT TABLET SYRUP TABLET SYRUP80 mg trimethoprim 40 mg trimethoprim 250 mg 125 mg per
+ 400 mg sulphamethoxazole + 200 mg sulphamethoxazole per 5 ml 5 ml
2 months up to 12 months 1/2 5.0 ml 1/2 5ml(4 - <10 kg)
12 months up to 5 years 1 10.0 ml 1 10 ml(10-19 kg)
COtRIMOXAZOLE NALIDIXIC ACID
(trimethoprim + sulphamethoxazole)Give two times daily for 5 days. Give four times daily for 5 days.
AGE OR WEIGHTSYRUP 250 mg/5 ml
2 months up to 4 months (4-<6 kg) 1.25 ml (1/4 tsp)See doses Above.
4 months up to 12 months (6 - <10 kg) 2.5 ml (1/2 tsp)
12 months up to 5 years(10- 19kg) 5 ml (1 tsp)
TETRACYCLINE COTRIMOXAZOLE(trimethoprim + sulphamethoxazole)
Give four times daily for 3 days. Give two times daily for 5 days.
AGE OR WEIGHT CAPSULE (250 mg)
2 months up to 4 months (4 - <6 kg)
4 months up to 12 months (6 - <10 kg) 1/2 See doses Above.
12 months up to 5 years (10 - <19 kg) 1

J
8
aTeACH THe MOTHeR TO Give ORAL DRUGS AT HOMe
Followthe instructions belowfor every oral drug to be given at home.Also followthe instructions listed with each drug's dos
~ Give an Oral AntimalarialFIRST-LINE ANTIMALARIAL:SECOND-LINE ANTIMALARIAL:
CHLOROQUINE, PRIMAQUINE, SULFADOXINE AND PYRIMETHAMINEARTEMETER-LUMEFRANTIN E
~ IF CHLOROQUINE:
. Explain to the mother that she should watch her child carefully for 30 minutes after giving a dose of chloroquine. If thechild vomits within 30 minutes, she should repeat the dose and return to the health center for additional tablets.. Explain that itching is a possible side effect of the drug, but is not dangerous.
~ IF SULFADOXINE + PYRIMETHAMINE: Give a single dose in the health center 2 hours before intake of Choroquine.
~ IF PRIMAQUINE: Give single dose on Day 4 for P. falciparum
~ IF ARTEMETER-LUMEFRANTINE combination: Give for 3 days.
See additional handout for drug table on second line antibiotics.
~ Give Paracetamol for High Fever (38.5°C or above) or Ear Pain
~ ~ ~ ~ 'iif1 ~~ ~ ",~ ~ ~
~ Give VitaminATREATMENT~ Give one dose in the health center.
SUPPLEMENT ATlON~ Give one dose in health center if:
- child is six months of age or older,- child has not received a dose of Vitamin A in the
past six months.
~ Give Iron~ Give one dose daily for 14 days.
AGEORWEIGHTIRON/FOLATETABLET
Ferroussulfate200mg+250mcgFolate
(60mgelementaliron)
IRONSYRUP
I
IRONDROPS
Ferroussulfate150mg Ferroussulfateper5 ml 25 mg
(6 mgelementalironperml) (25mgelementalironperml)
3 monthsupto 4 months(4- <6kg)
4 monthsupto12months(6-<10kg)
4 ml (3/4tsp) 1.0ml
2.5ml(1/2tsp) 0.6ml
12monthsupto 3 years(10-<14kg)
3 yearsupto 5years(14-19 kg)
1/2tablet 1.5ml5 ml(1tsp)
1 tablet 10ml(1112tsp) 2.0ml
~ Give Mebendazole/Albendazole~ Give 500 mg Mebendazole/400 mg Albendazole as a single dose in the health center if the
chileJis 12 months up to 59 months and has not had a dose in the previous 6 months, with
the following dose.
fI1f11
f11 ~ ~ ff1 '"' f'",
PRIMAQUINE PRIMAQUINE SULFADOXINE +CHLOROQUINE
Give single dose in Give daily for PYRIMETHAMINEGive for 3 days health center for 14 days for Give single dose in
P. falciparum P. vivax health center
TABLET TABLET TABLET TABLET(150 mg base) (15 mg base) (15 mg base) (500 mg sulfadoxine)
AGE DAY 1 DAY 2 DAY 3 25 mg pyrimethamine
2 months up to 5 months y"
(4 - <7 kg)
5 months up to 12 months(7 - <10 kg)
12 months up to 3 years 1 1 y" %
(10-<14kg)
3 years up to 5 years 1 1 1 % 1
(14 - <19 kg)
PARACETAMOL
AGE OR WEIGHT TABLET (500 mg) SYRUP (120 mg/5 ml)
2 months up to 3 years (4 - <14 kg) y" 5 ml (1 tsp)
3 years to 5 years (14 - <19 kg) 10 ml (2 tsp)
AGE VITAMIN A CAPSULES
100,0001U 200,000 IU
6 months up to 12 months 1 1/2 capsule
12 months.up to 5 years - 1 capsule
AGE OR WEIGHT Albendazole 400 mg tablet Mebendazole500 mg tablet
12 months up to 23 months }2 1
24 months up to 59 months 1 1

lJiJ]iJ]~]I2]j!JJ!lJ~1~1~]~1J:!L~1~1~11!1~1J1J111---ni
TEACHTHE MOTHE.R TO TREAT LOCAL INFECTIONS AT HOM.E
~ to the mother what the treatment is and why it should begiven.
~
~
~ Treat Eye Infection with Tetracycline Eye Ointment
~ Clean both eyes 3 times daily. Wash hands.. Ask child to close eyes.. Use clean cloth and water to gently wipe away pus.
~ Then apply tetracycline eye ointment in both eyes 3 times daily.. Ask the child to look up.. Squirt a small amount of oitment on the inside of the lower lid.. Wash hands again.
~ Treat until redness is gone.
~ Do not use other eye ointments or drops, or put anything else in the eye.
9
\ \cL Y, FEVER: NO MALARIA .,'Il:i KI:.\,,;UMMI:.NUAIIUI\i::)
ORAL DRUGSLOCALINFECTIONS FOLLOW-UP UNSEL THE MOTHER
~ Dry the Ear by Wicking
~ Dry the ear at least 3 times daily.. Roll clean absorbent cloth or soft, strong tissue paper into awick.. Place the wick in the child's ear.
. Remove the wick when wet.. Replace the wick with a clean one and repeat these stepsuntil ear is dry.
Treat Mouth Ulcers with Gentian Violet
~ Treat the mouth ulcers twice daily.. Wash hands.. Wash child's mouth clean using soft cloth wrapped around thefinger and wet with salt water.. Paint'the mouth with half-strength gentian violet, using cottonbud.
. Wash hands again.
~ Soothe the Throatand Relieve Coughwith a Safe Remedy
~ Safe remedies to recommend:. Breastmilk for exclusively breastfed infant. Tamarind, Calamansi and Ginger
~ Harmful remedies to discourage:. Codeine cough syrup. Other cough syrups. Oral and nasal decongestants
,CIU I Iv;:)iSESS AND CLASSIFY
FOLLOW-UPL

J J
10
GIVE THESE TREATMENTS IN HEALTH CENTER ONLY
~ lain to the mother why the drug is given.
.
.
~ Give an IntramuscularAntibioticFOR CHILDREN BEING REFERRED WHO CANNOT TAKE ORAL ANTIBIOTIC:
~ Give the first dose of intramuscular chloramphenicol and refer child urgently tohospital.
IF REFERRAL IS NOT POSSIBLE:~ Repeat the chloramphenicol injection every 12 hours for 5 days.~ Then change to an appropriate oral antibiotic to complete 10 days of treatment.
IJ "IJ WI rrJ 1'111 Mil ,,!I"IJ rJll"11
~ Give Quinine for Severe Malaria
FOR CHILDREN BEING REFERRED WITH A VERY SEVERE FEBRILE DISEASE/MALARIA:
~ Give first dose of intramuscular QUININE and refer urgently to hospital.
IF REFERRAL IS NOT POSSIBLE:~ Give first of intramuscular QUININE.~ The child should remain lying down for one hour.~ Repeat the QUININE injection at 4 and 8 hours later,and then every 12 hours until the child is
able to take an oral antimalarial. Do not continue QUININE injections for more than 1 week.~ DO NOT GIVE QUININE TOA CHILD LESS THAN 4 MONTHS OFAGE.
*quinine salt
rI'J ,,'J rf~1 n-j rf~J rrJ rrJ ITJrr~J~) [7')
CHLORAMPHENICOL
AGE OR WEIGHT Dose: 40 mg per kgAdd 5.0ml sterilewaterto vialcontaining
1,000mg= 5.6ml at 180mg/ml
2 months up to 4 months (4 - <6 kg) 1.0 ml = 180 mg
4 months up to 9 months (6 - <8 kg) 1.5 ml = 270 mg
9 months up to 12 months (8 -<10 kg) 2 ml = 360 mg
12 months to 3 years (10 - <14 kg) 2.5 ml = 450 mg
3 to 5 years (14 -19 kg) 3.5 ml = 630 mg
INTRAMUSCULAR QUININEAGE OR WEIGHT
300 mg/ml* (in ml ampoules)
4 months up to 12 months (6 - <10 kg) 0.3 ml
12 months up to 2 years (10- <12 kg) 0.4 ml
2 years up to 3 years (12 - <14 kg) 0.5 ml
3 years up to 5 years (14 -19 kg) 0.6 ml

L1--1Jr~1~1~1~1~:.JJ~:L~~~~~t~t~1~1~1~1~1-:!Ll1u~
I
Ii
!
--- --
~ Treat the Child to Prevent Low Blood Sugar Level~ If the child is able to breastfeed:
Ask the mother to breastfeed the child.
~ If the child is not able to breastfeed but is able to swallow:
Give expressed breastmilk or a breastmilk substitute.If neither of these is available, give sugar water.Give 30-50 ml of milk or sugar water before departure.
To make sugar water: Dissolve 4 level teaspoons of sugar (20 grams)in a 2QO-mlcup of clean water. .
~ If the child is not able to swallow:
Give 50 ml of milk or sugar water by nasogastric tube.
~ If the child is difficult to awaken or unconscious, start IV infusion:
Give5 mllkgof 10%of dextrosesolution(D10)overa few minutesOr give 1 mllkgof 50% (D50)by slowpush
11
,INTRAMUSCULARANTIBIOTIC
INTRAMUSCULARQUININELOW BLOODSUGAR LEVEL UNSEl THE MOTHER
~ Y, rtVER: NO MALARIJ.\ .,>jl;j KtL;UMMt:NUAIIU~::) ~IVllvv
iSESS AND CLASSIFYFOllOW-UP FOLLOW-UP

f f12
- ---~
E EXTRA FLUID FOR DIARRHEA AND CONTINUE FEEDING:See FOODadvice on COUNSEL THE MOTHE,
~ Plan A: Treat Diarrheaat HomeCounsel the Mother on the 4 Rules of Home Treatment:Give Extra Fluid, Give Zinc Supplements, Continue Feeding, When to Return
1. GIVE EXTRA FLUID (as much as the child will take)
~ Plan B: Treat Some Dehydration with ORSGive in health center recommended amount of ORS over 4-hour period
DETERMINE AMOUNT OF ORS TO GIVE DURING THE FIRST 4 HOURS.
* Use the child's age only when you do not know the weight. The approximate amount of ORS required(in ml) can also be calculated by multiplying the child's weight (in kg) times 75.
If the child wants more ORS than shown, give more.For infants under 6 months of age who are not breastfed, also give 100-200 ml cleanwater during this period.
SHOW THE MOTHER HOW TO GIVE ORS SOLUTION.
Give frequent small sips from a cup.If the child vomits, wait 10 minutes. Then continue, but more slowly.
Continue breastfeecHng whenever the child wants.
AFTER 4 HOURS.Reassess the child and classify the child for dehydration.Select the appropriate plan to continue treatment.Begin feeding the child in health center.
IF THE MOTHER MUST LEAVE BEFORE COMPLETING TREATMENT:Show her how to prepare ORS solution at home.Show her how much ORS to give her child to finish 4-hour treatment at home.Give her enough ORS packets to complete rehydration. Also give her 2 packets,as recommended in Plan A.Explain the 4 rules of home treatment:
1.2.3.4.
GIVE EXTRA FLUID
}GIVE ZINC SUPPLEMENTS See Plan A for the recommended fluidsCONTINUE FEEDING and .KNOW WHEN TO RETURN See the COUNSEL THE MOTHER chart.
1 .~ W ~ ,~ J~ JT 1T ,~ 'T 'T .~~~.
~ TELL THE MOTHER:
Breastfeed frequently and longer at each feeding.If the child is exclusively breastfed, give ORS or clean water in addition tobreastmilk.
If the child is not exclusively breastfed, give one or more of the following:ORS solution, food-based fluids (such as soup, rice water, or "buko juice"),or clean water.
It is especially important to give ORS at home when:the child has been treated with Plan B or Plan C during the visit, orthe child cannot return to a health center if the diarrhea gets worse.
~ TEACH THE MOTHER HOWTO MIX AND GIVE ORS. GIVE THE MOTHER 2PACKETS OF ORS TO USEAT HOME.
~ SHOW THE MOTHER HOW MUCH FLUID TO GIVE IN ADDITION TO THEUSUAL FLUID INTAKE: '
Up to 2 years2 years or more
50 to 100 ml after each loose stool100 to 200 ml after each loose stool
Tell the mother:- Give frequent small sips from a cup.- If the child vomits, wait 10 minutes. Then continue, but more slowly.- Continue qivinq extra fluid until the diarrhea stoDS.
2. GIVE ZINC SUPPLEMENTS. 10 mg per day in infants - < 6 mos. for 10-14 days
}. 20 mg per day in
.
children 6 mos. - 5 years old for 10-14 days See COUNSELTHE MOTHER
CONTINUE FEEDING chart
WHEN TO RETURN
3.4.
AGE Up to 4 months 4 months up to 12 months up to 2 years up to'12 months 2 years 5 years
WEIGHT <6 kg 6 to -<10 kg 10 to -<12 kg 12 to19 kg
AMOUNT (ml) 200-400 400-700 700-900 900-1400

l1J n~jj]jjJJj1J]J]Jl]lJjl]jj]IJ]I1]I1]IJ]Jl]j"J]IJ],IJ]jj1J
EXTRA FLUID FOR DIARRHEA AND CONTINUE FEE.DINGOhOOI1NSEL THlZlVIOTHER chart.
Plan C: Treat Severe Dehydration QuicklyFOLLOW THE ARROWS. IF ANSWER IS "YES," GO ACROSS. IF "NO," GO DOWN.
START HERE
Can you give intravenous (IV)fluid immediately?
YES.. Start IV fluid immediately. If the child can drink, give ORS by mouth while the drip is
set up. Give 100 ml/kg Ringer's Lactate Solution (or, if not available, normal saline),divided as follows:
NO) * Repeat once if radial pulse is still very weak or not detectable.
. Reassess the child every 1-2 hours. If hydration status is not improving, give the IVdrip more rapidly.. Also give ORS (about 5 mllkg/hr) as soon as the child can drink: usually after 3-4hours (infants) or 1-2 hours (children).. Reassess an infant after 6 hours and a child after 3 hours. Classify the dehydration.Then choose the appropriate plan (A, S, or C) to continue treatment.
Is IV treatment availablenearby (within 30 minutes)? YES. . Refer URGENTLY to hospital for IV treatment.. If the child can drink, provide the mother with ORS solution and show her how to
give frequent sips during the trip.NO
Are you trained to use anasogastric (NG) tube forrehydration?
. Start rehydration by tube (or mouth) with ORS solution: give 20 mllkg/hr for 6 hours(total of 120 mllkg).. Reassess the child every 1-2 hours:- If there is repeated vomiting or increasing abdominal ditension, give more fluid
slowly.- If hydration status is not improving after 3 hours, send the child for IV therapy.
. After 6 hours, reassess the child. Classify dehydration. Then choose the appropriateplan (A, S, or C) to continue treatment.
NO"
Can the child drink?
YESI.
NO"
Refer urgently to a hospitalfor IV or NG treatment.
NOTE:. If possible, observe the child at least 6 hours after rehydration to be sure that the
mother can maintain hydration, giving the child ORS solution by mouth.
13
\ PLANA, PLANS, PLAN C
UNLIKELY, FEVER: NO MALARIA
FOllOW-UP
,,'OJ\,:!~~vVMM~I'OjUI-\IIVI~;)
,SESS AND CLASSIFYJUNSElTHE MOTHER
.OIV I Iv;;)
FOLLOW-UP
AGE First give Then give30 ml/kg in: 70 ml/kg in:
Infants (under 12 months) 1 hour* 5 hours
Children (12 months up to 5 years) 30 minutes* 2 1/2 hours

J If
f;lt
14
,~FO~LI-OW-UPCARE
~ PNEUMONIA
After 2 days:
Check the child for general danger signs.
}Assess the child for cough or difficult breathing. See the ASSESS AND CLASSIFY chart.
Ask:
- Is the child's breathing slower?- Is there less fever?
- Is the child eating better?
Treatment:
. Ifchest indrawing ora general danger sign, give a dose of second-line antibioticor intramuscularchloramphenicol. Then refer URGENTLYto hospital.
. If breathing rate, fever, and eating are the same, change to the second-line antibiotic andadvise the mother to return in 2 days or refer. (If this child had measles within the last 3 months,refer.)
. If breathing slower, less fever, or eating better, complete the 5 days of antibiotic.
. If cough is more than 30 days, refer for assessment.
~ PERSISTENT DIARRHEA
After 5 days:
Ask:
- Has the diarrhea stopped?- How many loose stools is the child having per day?
Treatment:
. If the diarrhea has not stopped (child is still having less than 3 or more loose stools perday), do a full reassessment of the child. Give any treatment needed. Then refer to hospital.
Ifthe diarrhea has stopped (child having less than 3 loose stools per day), tell the motherto follow the usual recommendations for the child's age.
011'11I I '~I' ~" ""III I 1
'.'1I I 1
',..qI I ,{~'1 ~"'''11 ~~'1
~ DYSENTERY
After 2 days:
Assess the child for diarrhea. > See Assess & Classify chart
Ask:- Are there fewer stools?- Is there less blood in the stool?- Is there less fever?
- Is there less abdominal pain?- Is the child eating better?
Treatment:. If the child is dehydrated, treat dehydration.
If number of stools, amount of blood in stools, fever, abdominal pain, oreating is the same or worse:Change to second-line oral antibiotic recommended for Shigella in your area.Give it for 5 days. Advise the mother to return in 2 days.
Exceptions -if the child:
- is less than 12 months old, or } Refer to hospital- was dehydrated on the first visit, or- had measles within the last 3 months
. If fewer stools, less blood in the stools, less fever, less abdominal pain,and eating better, continue giving the same antibiotic until finished.
~, ~, rI'1 11' r;'J r7'1~i, 1rn rT' rI'

L1~l111~J.1~11~~~~~~7l1u.~~~u.~
FOllOW-UP CARE
~ MALARIA
If fever persists after 2 days, or returns within 14 days:
Do a full assessment of the child. > See ASSESS & CLASSIFY chart.
Treatment:
~ If the child has any general danger sign or stiff neck, treat as VERYSEVERE FEBRILE DISEASE/MALARIA.
~ If the child has any cause of fever other than malaria, providetreatment.
~ If malaria is the only apparent cause of fever.
- Take a blood smear
- Give second-line oral antimalarial without waiting for result of bloodsmear.
- Advise mother to return if fever persists.- If fever persists after 2 days treatment with second-line oral
antimalarial, refer with blood smear for reassessment.- If fever has been present for 7 days, refer for assessment.
,
PNEUMONIA, PERSISTENTDIARRHEA, DYSENTERY,
MALARIA, FEVER: MALARIA
UNLIKELY, FEVER: NO MALARIA
FOLLOW-UP
If fever persists after 2 days:
~ FEVER-MALARIA UNLIKELY
Do a full assessment of the child. > See ASSESS & CLASSIFY chart.Assess for other causes of fever.
Treatment:
~ If the child has any general danger sign or stiff neck, treat as VERY SEVERE FEBRILEDISEASE/MALARIA.
~ If malaria is the only apparent cause of fever.- Take a blood smear.- Treat with the first-line oral antimalarial. Advise the mother to return again in 2 days if
the fever persists.- If fever has been present for 7 days, refer for assessment.
~ FEVER (NO MALARIA)If fever persists after 2 days:
Do a full assessment of the child. > See ASSESS & CLASSIFY chart.Make sure that there has been no travel to malarious area and overnight stay in malaria area.If there has been travel and overnight stay take blood smear, if possible.
Treatment:~ If there has been travel and overnight stay to a malarious area and the blood smear is posi-
tive or there is no blood smear - classify according to Fever with Malaria Risk and treat
accordingly.~ If there has been no travel to mfllarious area or blood smear is negative:
- If the child has any general danger sign or stiff neck, treat as VERY SEVEREFEBRILE DISEASE.
- If the child has any apparent cause of1ever, provide treatment.- If no apparent cause of fever, advise the mother to return again in 2 days if fever
persists.- If fever has been present for 7 days, refer for assessment.
15
,~l:; Kt:t;UMMt:NUAIIUI'i':) .:IIUllv;:'»SESS AND CLASSIFY
FOLLOW-UPUNSEL THE MOTHER

f If f
\i1
EFO OW-UP CARE
~
~ MEASLES WITH EYE OR MOUTHCOMPLICATIONS
After 2 days:
Look for red eyes and pus draining from the eyes.Look at mouth ulcers.Smell the mouth.
Treatment for Eye Infection:~ If pus is draining from the eye, ask the mother to describe how
she has treated the eye infection. If treatment has been correct,refer to hospital. If treatment has not been correct, teach mothercorrect treatment.
~ If pus is gone but redness remains, continue the treatment.
~ If no pus or redness, stop the treatment.
Treatment for Mouth Ulcers:
~ If mouth ulcers are worse, or there is a very foul smell fromthe mouth, refer to hospital.
~ If mouth ulcers are the same or better, continue using half-strength gentian violet for a total of 5 days.
rf1 ~ ~iI r11 ~11~~ ri1 ~
16
~ FEVER: DENGUE HEMORRHAGIC FEVER UNLIKELY
If fever persists after 2 days:
Do a full assessment of the child. > See ASSESS & CLASSIFY chart.
Do a tourniquet test.Assess for the other causes of fever.
Treatment:
~ Ifthe child has any signs of bleeding, including skin petechiae or apositive tourniquettest, or signs of shock, or persistent abdominal pain or persistent vomiting.If the child has any other apparent cause of fever, provide treatment.If fever has been present for 7 days, refer for assessment.If no apparent cause of fever, advise the mother to return daily until the child has had nofever for least 48 hours.
~ Advise mother to make sure child is given more fluids and is eating.
~
~
~
~ EAR INFECTION
After 5 days:Reassess for ear problem. > See ASSESS & CLASSIFY chart.Measure the child's temperature.
Treatment:
~ If there is tender swelling behind the ear or high fever (38.5°C or above), treat asMASTOIDITIS.
~ Acute earinfection:if earpain ordischargepersists,treatwith5 moredaysof thesameantibiotic. Continue wicking to dry the ear. Follow-up in 5 days.
~ Chronic ear infection: Check that the mother is wicking the ear correctly. Encourage herto continue.
~ If no ear pain or discharge, praise the mother for her careful treatment. If she has not yetfinished the 5 days of antibiotic, tell her to use all of it before stopping.
r;..1 1~ rf' rT1 ~ r7' ~~ ~ ri' D~rt1

l1J1I1L1l1l1L1I1I1I1!1l1l1lli!1l1I1I1l1l1U;-....
VE FOLLOW-UP CARE
. ~ ANEMIA
After 14 days:
~ Give iron. Atlvise mother to return in 14 days for more iron.IFANY MORE FOllOW-UP VISITS ARE NEEDED BASED ON THE
INITIAL VISIT OR THIS VISIT, ADVISE THE MOTHER OF THENEXT FOllOW-UP VISIT.
0~ Continue giving iron every day for 2 months with follow-up every 14 days.
~ If the child has any palmar pallor after 2 months, refer for assessment.ALSO, ADVISE THE MOTHERWHEN TO RETURN IMMEDIATELY.
(See the COUNSEL THE MOTHER chart.)
17
\MEASLES,FEVER:DENGUE
HEMORRHAGICFEVERUNLIKELY,EARINFECTION,
FEEDINGPROBLEM,ANEMIA,VERYLOWWEIGHT, l
ING RECOMMENDATIONS
SESS AND CLASSIFYFOllOW-UPUNSEL THE MOTHER

rf1
f JjJ
18
COUNSEL THE MOTHER
~ Assess the Child's Feeding
Ask questions about the child's usual feeding and feeding duringthis illness. Compare the mother's answers to the FeedingRecommendations for the child's age in the box below.
ASK: ~ Do you breastfeed your child?- How many times during the day?- Do you also breastfeed during the night?
~ Does the child take any other food or fluids?- What food or fluids?- How many times per day?- What do you use to feed the child?- If very low weight for age: How large are servings?
Does the child receive his own serving?Who feed the child and how?
~ During this illness, has the child's feeding changed?If yes, how?
111 ill r~ IIIft1 rpr~ r~
~ Assess the Child's Care for Development
Ask questions about how mother cares for her child. Compare themother's answers to the Recommendations for Care forDevelopment.
ASK: - How do you play with your child?- How do you communicate with your child?
Sample Feeding Problem
1. difficulty in breastfeeding2. child less than 4 months taking other milk/food3. use of breastmilk substitute/cow's milk/evap milk4. use of feeding bottles5. lack of active feeding6. not feeding well during illness7. complementary food not enough in quantity/quality/variety8. child 6 months above not yet given complementary foods9. infant not exclusively breastfed
10. improper handling and use of breastmilk substitute
{ll ~ f1l rTl fI1III f11 f11 fl1fl1ill f1l

l111J1l1l1J111l1l111I111J1l111l1l1lJ;J1l1l1-
Recommendations for Feeding and Care for DevelopmentBirth up to 6 Months
. Exclusively breastfeed as often as the childwants, day and night, at least 8 times in 24hours.
. Do not give other foods or fluids.
Play:. Provide an area where the child could move, play,and develop his senses of sight, touch, andhearing.
" Have large, colorful things for your child to reachfor and new things to see.
Communicate:
. Look into your child's eyes andsmile at him or her.
When you arebreastfeeding, it isa good time to talkto your child andget a conversationgoing with sounds orgestures.
6 months to 12 months
. Breastfeed as often as the child wants.
. Add any of the following:
. Lugawwith addedoil, mashedvegetablesorbeans, steamed tokwa, flaked fish,
pulverized roasted dilis, finely ground meat,egg yolk, bite-size fruits
. 3 times per day ifbreastfed. 5 times per day if notbreastfed
Play:. Give your child clean, safe householdthings to handle, bang, and drop.
Feeding Recommendations for a child who has PERSISTENT DIARRHEA~ If still breastfeeding, give more frequent, longer breastfeeds, day and night.~ If taking other milk such as milk supplements;
Replace these with increased breastfeeding, or
I
12 months to 2 years
. Breastfeed as often as the child wants.. Give adequate amount of family foods, suchas: rice, camote, potato, fish, chicken, meat,monggo, steamed tokwa, pulverized roasteddilis, milk and eggs, dark-green, leafy andyellow vegetables (malunggay,squash), fruits (papaya,banana)
. Add oil or margarine.
. 5 times per day
. Feed the baby nutritioussnacks like fruits.
Play:. Give your child things to stack up, and to put
into containers, and take out.
Communicate: b. Askyour childsimple
,,
'.
.
' . '''
.
'
questions. Respond
to your child'sattempts to talk. ,Playgames like ~ ~
,
~,
-"bye." e.~@
2 years and older
/. Give adequate amount of family foods at 3
meals every day.. Give twice daily nutritious foods, betweenmeals such as: Boiled
yellow camote,boiled yellow corn,peanuts, boiledsaba, banana, taho,fruits, and fruit
juices.
Play:. Help your child count,name, and comparethings.
. Make simple toys foryour child.
Communicate:. Encourageyourchildto talk, and answer
your child's questions.Teach your child stories,songs, and games.
Replace half the milk with nutrient-rich, semi-solid foods.Do not use condensed or evaporated filled milk.For other foods, follow the feeding recommendations for the child's age.
19
~
ASSESS FEEDING,FEEDINGRECOMMENDATIONS
iSESS AND CLASSIFYCOUNSEL THE MOTHER L FOLLOW-UP

r f J1 f J
20
@
~ Counsel the MotherAbout Feeding Problems
If the child is not being fed as described in the above recommendations, counsel the mother accordingly. In addition:
~ Ifthe mother reports difficulty with breastfeeding, assess breastfeeding. (See YOUNG INFANT chart.) As needed, showthe mother correct positioning and attachment for breastfeeding.
~ Ifthe child is less than 6 months old and is taking other milk or foods:-Build mother's confidence that she can produce all the breastmilk that the child needs.-Suggest giving more frequent, longer breastfeeding, day and night, and gradually reducing other milk or foods.
If other milk needs to be continued, counsel the mother to:
- Breastfeed as much as possible, including at night.- Make sure that other milk is a locally appropriate breastmilk substitute, give only when necesarry.- Make sure other milk is correctly and hygienically prepared and given in adequate amounts.- Prepare only an amount of milk which the child can consume within an hour. If there is some left-over milk, discard.
~If the mother is using a bottle to feed the child:- Recommend substituting a cup for bottle.
- Show the mother how to feed the child with a cup.
~ Ifthe child is not being fed actively, counsel the mother to:-Sit witbthechild and encourage eating.- Give the child an adequate serving in a separate plate or bowl.- Observe what the child likes and consider this in the preparation of his/her food.
~ Ifthe child is not feeding well during illness, counsel the mother to:- Breastfeed more frequently and longer if possible.
- Use soft, varied, appetizing, favorite foods to encourage the child to eat as much as possible, and offer frequent small feeding.- Clear a blocked nose if it interferes with feeding.- Expect that appetite will improve as child gets better.
~ Follow up any feeding problem in 5 days.
-- -- - ----
ft1 ~ " ,~
- - -- - -- --- -----------
1~ 111 111 111 11f 111 111 'i1 ~i11 Ii~l1l ,~ '111 ~" ~ r1

il. 1~ 11J li lj .il li U]j-illJll11--11 11 llJII u il lJJ il il
~ Advise the Mother to Increase Fluid During IllnessFOR ANY SICK CHILD:
~Breastfeed more frequently and longer at each feed.~ Increase fluid. For example, give soup, rice water, buko juice or clean water.
FOR CHILD WITH DIARRHEA:~Giving an extra fluid can be lifesaving. Give fluid according to Plan A or Plan B on TREAT THE CHILD chart.
Advise the Mother When to Return to Health Worker
FOLLOW-UP VISITAdvisethe motherto comefor follow-upat the earliesttime listedfor the child'sproblems.
21FEEDING AND CARE FOR
DEVELOPMENT,FEEDING PROBLEMS,
FLUID, WHEN TO RETURN,
WHEN TO RETURN IMMEDIATELY
.,)IVllvv I nn.vvl I
SSESS AND CLASSIFYFOLLOW-UP
If the child has: Return for follow-up in:
PNEUMONIA 2 daysDYSENTERYMALARIA,if the fever persistsFEVER-MALARIAUNLIKELY,if the fever persistsFEVER(NO MALARIA)if the fever persistsMEASLESWITH EYEOR MOUTHCOMPLICATIONSDENGUEHEMORRHAGICFEVERUNLIKELY,if the fever persists
PERSISTENTDIARRHEA 5 daysACUTE EARINFECTIONCHRONICEAR INFECTIONFEEDINGPROBLEMSMANYOTHERILLNESSES,if not improving
ANEMIA 14 days
VERY LOWWEIGHT FORAGE 30 days
Advise the mother to return immediately if the child has any of these signs:
Any sick child . Not able to drink or breastfeed. Becomes sicker. Develops a fever
Ifthe childhas NOPNEUMONIA: . Fast breathingCOUGHORCOLD,also returnif: . Difficultbreathing
If the child has Diarrhea, also return if: . Bloodinstool. Drinkingpoorly
If the childhasFEVER:DENGUE . Any sign of bleedingHEMORRHAGICFEVERUNLIKELY, . Persistent abdominal painalso return if: . Persistentvomiting. Skinpetechiae. Skin rash

r If f f
22
~ Counsel the Mother about Her Own Health
~ If the mother is sick, provide care for her, or refer her for help.
If she has a breast problem (such as engorgement, sore nipples, breast infection), provide care for her or refer her for help.
Advise her to eat well to keep her own strength and health.
Check the mother's immunization status and give her Tetanus Toxoid if needed.
Make sure she has access to:
. Family Planning
. Counseling on STD and AIDS prevention.
~ 1~ ,~ ;~ ~" ~ t}1 ~~ ft1 ~" 111 111 111 )11 111 ft1 )11 If1 111 " ",

U-l1wiJil11111L1111111L1L111J111L1 UI1-Ul1-- ~-
~
..
~ - ~ -
~l
ASSESS, CLASSIFY, AND TREAT THE SICK INFANTAGE 1 WEEK TO 2 MONTHS
IASSESS
ASK THE MOTHER WHAT THE YOUNG INFANT'S PROBLEMS ARE
Determine if this is an initial or follow-up visit for this problem.If follow-up visit, use the follow-up instructions in the follow-up section.If initial visit, assess the young infant as follows:
CHECK FOR POSSIBLE BACTERIAL INFECTION
ASK:
Has the infant
ClassifyALLYOUNGINFANTS
had convulsions?
LOOK, LISTEN:
. Count the breaths in one minute.
}
Repeat the count if elevated.
Look for chest indrawing.
Look for nasal flaring.
Look and listen for grunting.
. Look and feel for bulging fontanelle.
. Look for pus draining from the ear.
. Look at the umbilicus. Is it red or draining pus?
Does the redness extend to the skin?
CHILDMUSTBECALM.
. Measure temperature (or feel for fever or low body temperature).
. Look for skin pustules. Are there many or severe pustules?
. See if the young infant is abnormally sleepy or
difficult to awaken.
. Look at the young infant's movements.
Are they less than normal?
.These thresholds are based on axillary temperature. The thresholds for rectal temperature readings are approximately a.sac higher.
.. If referral is not possible, manage the child as described in Management of Childhood Illness.Treat the Child, Annex: Where Referral is Not Possible.
l.-
CLASSIFY IDENTIFYTREATMENT
USE All BOXES THAT MATCH THEINFANT'S SYMPTOMS AND PROBLEMS
TO CLASSifY THE IllNESS.
SIGNS CLASSIFY AS TREATMENT
23MOTHER'SHEALTH
BACTERIALINFECTION
,\ ASSESS AND CLASSIFY l FOLLOW-UP
,.. Con""Jlsions or . Give ,first dose of intramt1scalarFast breatbing (60 breClths;per minute or antibiotics.more)or
.Severe ch indrawing or POSSIBLE . Treat the chirtJto prevent low bloodNasal flaring or SERIOUS sugar.Grunting or BACTERIAL
Bulging fontanelle or INFECTION . Advise m,pther how to keep thePus draining from the ear or infant warm on the way to theUmbilical rednes§ extending to the skin or hospital. I
Fever (37.5°C*or above, or feels hot) or lowbodytemperature (less than 35.5°8*,or . Refer URGENTLY to the hospital. **
feels cold)or I!IMany or severe skin pustules orAbnormly; sleepy or diffcUlt to awaken or .Less Ulan normal movement.
Red umbilicus or draining pus or LOCAL . Givean appropriate oral antibiotic.Skin pustules BACTERIAL . Treat the local infection in the health
INFECTION center, and teach the mother to treatlocal infections at home.
. Advise mother how to give home carefor young infant.
. Follow up in 2 days.

J if I r f
24
rrhea'? Two of the following signs:. Abnormally sleepy ordifficult to awaken. Sunkeneyes
. SkJ,npinchgoes backveryslowly
IF YES, ASK:. For how long?. Is there blood in
the stool?
LOOK AND FEEL:
. Look at the young infant's generalcondition. Is the young infant:- Abnormally sleepy or difficult to
awaken?- Restless or irritable?
forDEHYDRATION
. Look for sunken eyes.
. Pinch the skin of the abdomen.Does it go back:- Very slowly (longer than 2
seconds )?- Slowly?
Two of the following signs:. Restless, irritable
. Sunken eyes
. Skin pinch goes backslowly
. Not enough signs toclassify as some orseveredehydration
. Diarrhea lasting for 14 daysor more
seveREDEHYDRATION
..
SOMEDEHYDRATION
NODEHYDRATION
SEVERE,PERSISTENTDIARRHEA
. If infant does not have POSSIBLE SERIOUSBACTERIALINFECTION.nor DYSENTER){:- Giv~fluid for severedehydration(PlanC)
ORIf infant also has a POSSIBLE SERIOUSBACTERIAL INFECTIONor DYSENTERY:- Refer URGENTLYto hospital, with mother
giving frequent sips of ORS on the way.- Advise mother to continue breastfeeding.- Advise mother how to keep the young.
infant warm on the way to the hospital.
. Give fluid for somedehydration(Plan B).
. If infant also has POSSIBLE SERIOUSBACTERIAL INFECTIONor DYSENTERY:
Refer URGENTLYto hospital with mothergiving frequent sips of ORSon the way.Advise mother to continue breastfeeding.
. Give fluid to treat diarrhea at home (Plan A).
. If the young infant has dehydration, treatdehydration bW'orereferral unless the infanthas also POSSIBLE SERIOUS BACTERIALINFECTION.
. Refer to hospital.
and if bloodin stool
1 T~ 11' 11' 11' 11' 11' 11'11' 11' 11'11' 11' 11' 11' 11' 11' 11' Il~ 11' Il~ rP
. Refer URGENTLY to hospital, withamother. Bloodinthe stool DYSENTERY giving frequent sips of ORS on the way.
. Advise mother to continue breastfeeding.

r111l1l1lj;--?1lIuJ ~~~uJl.1~~~
THEN CHECK. FOR FEEDING PROBLEMS OR LOW WEIGHT:
IF YES, ASK: LOOK and FEEL:
Is there any difficulty feeding? Determine weight for age.
Is the infant breastfed? If yes,how many times in 24 hours?
Does the infant usually receiveany other food or drink? If yes,how often?
What do you use to feed the infant?---------------------------------------IF AN INFANT: Has any difficulty feeding.
Is breastfeeding less than 8 times in 24 hours,Is taking any other foods or drinks, or
Is low weight for age,AND
Has no indications to refer urgently to hospital:
ASSESS THE INFANT'S BREASTFEEDING:
Has the infant breastfed
in the previous hour?If the infant has not fed in the previous hours, ask the mother toput her infant to the breast. Observe the breastfeed for 4 minutes.
(If the infant was fed during the last hour, ask the mother if shecan wait, and to tell you when the infant is willing to feed again.)
Is the infant able to attach?
no attachment at all not well attached good attachment
TO CHECK ATTACHMENT, LOOK FOR:Chin touching the breastMouth wide openLower lip turned outwardMore areola visible above than below the mouth
(All these signs shouldbe present if the attachment is good.)
Is the infant sucking effectively (that is, slow, deep sucks,sometimes pausing)?
not sucking at all not sucking effectively good effectively
Clear a blocked nose if it interferes with breastfeeding.
Look for ulcers or white patches in the mouth (thrush).
ClassifyFEEDING
WP
.
.8<
25
@
. Not well attached tobreast or
. Not sucking effectivelyor. Less than 8 breastfeedsin 24 hours or. Receives other foods ordrinks or
. Low weight for age or. Thrush (ulcers or whitepatches in the mouth)
.
. Not low weight for age,and no other signs ofinadequate feeding.
\ DIARRHEAFEEDING PROBLEMS
FEEDINGPROBLEM
ORLOWWEIGHT
NO FEEDINGPROBLEM
~ Advise the mother to breastfeed as often and
for as long as the infant wants, day and night.
. If not well attached or not sucking effectively,teach correct positioning and attachment.
. If breastfeeding less than 8 times in 24hours, advise to increase frequency ofbreastfeeding.
~ If receiving other foods or drinks, counselmother about breastfeeding more, reducingother foods and drinks, and using a cup:
If not breastfeeding at all:
Refer to breastfeeding counseling andpossible relactation.
Advise about the correct preparing ofbreastmilk substitutes, and using acup.
~ If thrush, teach the mother to treat thrush athome. .
~ Advise the mother to give home care for theyoung infant.
~ Follow up any feeding problem or thrush in 2days.
~ Follow up low weight for age in 14 days.
~ Advise mother to give home care for the younginfant.
~ Praise the mother for feeding the infant well.
...IVII\.,,':' IHKU~H
FOLLOW-UP

/ ]J f r J
26
;'fl '11/ 1111 1111 11') 11') 11'1 "11 111) t1" lfl 11'1 1111 11'] TII' 11'J 11" rt'J ITI iT] IT]

llJ !lj-!1uJL]Jl111JllJl]Jl1!J~L1UJl]~il1 u.I1---u.~
~'"~ '-- ~ ~,- ---- - - ~ '* ,,<m - =-~
T :r THE YOUNG INFANT AND COUNSEL THE MOTHER
~ Give an Appropriate OralAntibioticFor local bacterial infection:First-line antibiotic:Second-line antibiotic:
COTRIMOXAZOLEAMOXICILLIN
COTRIMOXAZOLE
(trimethoprim + sulphamethoxazole)~ Give two times daily for 5 days
AMOXYCILLIN
~ Give three times daily for 5 days
AGE OR WEIGHT
2.5 ml
SYRUP40 mg trimethoprim + 200 mgsulphamethoxazole per 5 ml
ADULT TABLETsingle strength (80 mg trimethoprim +
400 mg sulphamethoxazole)
TABLET
250 mg
SYRUP
125 mg per 5 ml
Birth up to 1 month «3 kg) 1.25 ml* 1.25 ml
1 to 2 months (3-4 kg) 2.5 ml
* Avoid cotrimoxazole in infants less than 1 month of age who are premature or jaundiced.
~ Give First Dose of Intramuscular Antibiotics~ Give the first dose of both benzylpenicillin and gentamicin intramuscular.
* Avoid using undiluted 40 mg/ml gentamicin.
Referral is the best option for a young infant classified with POSSIBLE SERIOUS BACTERIAL INFECTION. If referral is not possible, givebenzylpenicillin and gentamicin for at least 5 days. Give benzylpenicillin every 6 hours plus gentamicin one dose daily.
27
\IMMUNIZATION STATUS ANTIBIOTICS
TREAT AND COUNSEL
THRUSH
FOLLOW-UP
GENTAMICIN BENZYLPENICILLIN
Dose: 5 mg per kg Dose: 50,000 units per kg
WEIGHT Undiluted 2 ml or Add 6 ml sterile water To a vial of 600 mg (1,000,000 units):vial containing to 2 ml vial containing Add 2.1 ml sterile water = OR Add 3.6 ml sterile water =
20 mg = 2 ml at 10 mg/ml 80 mg* = 8 ml at 10 mg/ml 2.5 ml at 400,000 units/ml 4.0 ml at 250,000 units/ml
1 kg 0.5 ml* 0.1 ml 0.2 ml
2 kg 1.0 ml* 0.2 ml 0.4 ml
3 kg 1.5 ml* 0.4 ml 0.6 ml
4 kg 2.0 ml* 0.5 ml 0.8 ml
5 kg 2.5 ml* 0.6 ml 1.0 ml

J j J J r"' I
28
T THE YOUNG INFANTAND COU L THE MO
1~1~1~j]~J~]~j]'~]~1'J]I~]~~]~
~ To treat Diarrhea, See TREAT THE CHILD chart.
~ Teach the Mother How to Treat Local Infections at Home
~ Explain how the treatment is given.~ Watch her as she does the first treatment in the health center.
~ Tell her to do the treatment twice daily. She should return to the health center if the infection worsens.
To Treat Skin Pustules
The mother should:
~ Wash hands.
~ Gently wash off pus and
crusts with soap and water.
~ Dry the area.
~ Paint with gentian violet.~ Wash hands.
To Treat Oral Thrush (ulcers or white patches in mouth)
The mother should:
~ Wash hands.
~ Wash mouth with clean soft cloth wrapped around the fingerand wet with salt water.
~ Paint the mouth with half-strength gentian violet.
~ Wash hands.
To Treat Umbilical InfectionThe mother should:
~ Wash hands.
~ Clean with 70% ethyl alcohol
~ Paint with gentian violet.
~ Wash hands.

.]J:}JIJJl}J1J1!1!1~;!1!.1;!];U~;-!1lJ~-u.L1!.1L1~~
TREAT THE YOUNG INFANT AND COUNSEL THE MOTHER
~ Teach Correct Positioning and Attachment for Breastfeeding
~ Show the mother how to hold her infant.
- with the infant's head and body straight.
- facing her breast, with infant's nose opposite her nipples
- with infant's body close to her body
- supporting infant's whQle body, not just neck and shoulders.
~ Show her how to help the infant to attach. She should:
- touch her infant's lips with her nipple
- wait until her infant's mouth is opening wide
- move her infant quickly onto breast, aiming the infant's lower lip well below the nipple.
~ Look for signs of good attachment and effective sucking. If the attachment or sucking is good, try again.
~ Advise Mother to Give Home Care for the Young Infant~
~
FOOD
FLUID } Breastfeed frequently, as often and for as long as the infant wants,
day and night, during sickness and health.
~ WHEN TO RETURN
Follow-up Visit When to Return Immediately:
Advise the mother to return immediately ifthe younginfant has any of these signs:
Breastfeeding or drinking poorlyBecomes sicker
Develops a feverFast breathingDifficult breathingBlood in stool
~ MAKE SURE THE YOUNG INFANT STAYSWARM AT ALL TIMES.In cool weather, cover the infant's head and feet, and dressthe infant with extra clothing.
29
\LOCAL INFECTIONSBREASTFEEDING
HOME CARETHRUSH
FOLLOW-UP
Ifthe infant has: Return for follow-up in:
LOCAL BACTERIAL INFECTIONANY FEEDING PROBLEM 2 daysTHRUSH
LOW WEIGHT FORAGE 14days

pJ j J ] J ] f
,
30
GIVE FOLLOW-UPCARE FOR THE SICK YOUNG IN NT
~ LOCAL BACTERIAL INFECTION
After 2 days:Look at the umbilicus. Is red or draining pus? Does redness extend to the skin?Look at the skin pustules. Are there many or severe pustules?
Treatment
~ If the pus or redness remains or is worse, refer to hospital.
~ If the pus and redness are improved, tell the mother to continue giving the 5 days of antibioticand continue treating the local infection at home.
~I~J~]~]~]'~]I~]~]~jl~]I~]~]~]~~]~]~]~]~]~~

III J1\ 1Jl 111 11, 11; 1'\- 111 l]~1 1"j; rJ~
J'I'. -1
l' ,.. J~ I'll ]j1 Ij~ ]]~
GIVE-FOLLOW UP CARE FOR THE SICK YOUNG INFANT
~ FEEDING PROBLEM
After 2 days:
Reassess feeding. > See "Then Check for Feeding Problem or Low Weight" above.Ask about any feeding problems found on the initial visit.~ Counsel the mother about any new or continuing feeding problems. If you counsel the mother to make significant changes in feeding, ask her to
bring the young infant back again.
If the young infant is low weight for age, ask mother to return in 14 days after the initial visit to measure the young infant's weight gain.
Exception:If you do not think that feeding will improve, or if young infant has loss weight, refer the child.
~ LOW WEIGHTAfter 14 days:Weigh the young infant and determine if the infant is still low weight for age.Reassess feeding. > See "Then Check for Feeding Problem or Low Weight" above.
JJj ! ]1
If the infant is no longer low weight for age, praise the mother and encourage her to continue.If the young infant is still low weight for age, but is feeding well, praise mother. Ask her to come again within a month or when she returns for immunization.If the young infant is still low weight for age and still has a feeding problem, counsel the mother about the feeding problem. Ask the mother to return again in 14 days(or when she returns for immunization, if this is within 2 weeks).Continue to see the young infant every few weeks until infant is feeding well and gaining weight regularly or is no longer low weight for age.
Exception:If you do not think that feeding will improve, or if young infant has lost weight, refer to hospital.
~ ORAL THRUSH
After 2 days:Look for ulcers or white patches in the mouth (thrush).Reassess feeding. > See "Then Check for Feeding Problem or Low Weight" above.~ If thrush is worse, or if the infant has problems with attachment or sucking, refer to hospital.~ If thrush is the same or better, and if the infant is feeding well, continue half-strength gentian violet for a total of 5 days.
31
1 JI ! I,
\FEEDING PROBLEM,
LOW WEIGHT FOR AGE,THRUSH
FOLLOW~UP

I
r-,!
66rF
FF.-~
666rr-:=!
[,
r~r.,
l~r-~
r.l
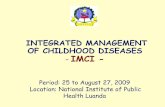
MANAGEMENTOFTHESICKYOUNGINFANTAGE 1 WEEKUPTO 2 MONTHS
Date:
Child'sName:
ASK:Whataretheinfant'sproblems?
ASSESS(Circleallsignspresent)
kg . Temperature:
Follow-upvisit:Age:- Sex:- Weight:
Initialvisit:
CHECK FOR POSSIBLE BACTERIAL INFECTION. Has the infant had convulsions? . Count the breaths in one minute.
per minute. Repeat ifelevated-Fast Breathing?. Look for severe chest indrawing.. Look for nasal flaring.
. Look and listen for grunting.. Look and feel for bulging fontanelle.. Look for pus draining from the ear.. Look at the umbilicus. Is it red or draining pus?Does the redness extend to the skin?. Fever (temperature 37.5°C or above or feels hot)or low body temperature (below 35.5°C or feels cool)
. Look for skin pustules. Are there many or severe pustules?. See if the young infant is abnormally sleepy ordifficult to awaken.
. Look at the young infant's movements. Less than normal?
YES_NO-. Look at the young infant's general condition. Is the infant:Abnormally sleepy or difficult to awakenRestless or irritable?. Look for sunken eyes.. Pinch the skin of the abdomen. Does it go back:Very slowly (longer than 2 seconds)?Slowly?
THEN CHECK FOR FEEDING PROBLEM OR LOW WEIGHT. Is there difficulty feeding Yes - No - .Determine weight for age. Low - Not low -. Is the infant breastfed? Yes - No-If Yes, how many times in 24 hours?- times. Does the infant usually receive any other foods or drinks? Yes -If Yes, how often?
. What do you use to feed the child?-----------------------------------If the infant has any difficulty feeding, is feeding less than 8 times in 24 hours, is taking any other food ordrinks, or is low weight for age AND has no indications to refer urgently to hospital:
breaths
DOES THE YOUNG INFANT HAVE DIARRHEA?. For how long? days. Is there blood in the stool?
No-
ASSESS BREASTFEEDING:Has the infant breastfed in the previous hour? If infant has not fed in the previous hour, ask the mother to put her
infant on her breast.Observe the breastfeed for 4 minutes.. Is the infant able to attach? To check attachment, look for:
- Chin touching breast Yes - No-- Mouth wide open Yes - No-- Lower lip turned outward Yes - No-- More areola above than below the mouth Yes - No-
no attachment at all not well attached good attachment
. Is the infant sucking effectively (that is, slow deep sucks,sometimes pausing)?
L:! not sucking at all not sucking effectively sucking effectively
. Look for ulcers or white patches in the mouth (thrush)
~1-... CHECK THE YOUNG INFANT'S IMMUNIZATION STATUS Circle immunization needed today.
- - -BCG DPT1 OPV1 HEPB1
"
r-.1-.. ASSESS OTHER PROBLEMS
~~
::E"
°C
~~0LL
C)z2i~0UW~
CLASSIFY
('f)
('f)
-----
Return for nextimmunization on:
(Date)
j~

r
1---------
1.--------...
~
~
'---~
-----
I.
TREAT_I
~E:j
;::"E::=
..-:'9'8
t!::::
nI'!'-'"'-
~!:::
=-~
.;:".--
-;.;~
=-!:::
-q-('i)
-;:.-
~~
p:"!Z:
p;"~
~~
Returnfor follow-upin:
Advisemotherwhento returnimmediately.
Giveany immunizationsneededtoday:
1="~
I='!!::
~.-----;:::0~--
...,.r-
--...r-r-

~ -idJ-fU.allbtaJ~Mad1~-"43.jd1d3Jd1~~EI1 a1d3J~~-.
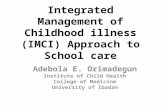
GROWTH CHARTRecord the information along the month-of-weighing line using the symbols below:
FBCCF -D01AH1
weightfever
breastfeedingcough/cold
complementary foods introduceddiarrheaother illnesses
Vitamin A givenhospitalized
sign of injuries such asabrasions/hematoma
4
2019
14
13
12
1110
9
8
7
6
5
4
3
2
1
00 1 2 3 4 5 6 7 8 9 10 11 12I 1 I 1 1 I I 1 1 I I 1 I
Cebu
I 10321254-3487
Distributed by-
e & E PublisJUni, Inc.
1672 Quezon Avenue, South Triangle. Quezon Cit)'
Tel. NO's.929-1344/928-7298 E-mail: infQ.~cebookshop.com
Website: www.cebookshop.com
Showroom & Branches:
IlO'-ilo(0331320-5079
Cagayan de Oro108821272-2094
Davao(082) 225-0159
4-5years
5-6 years+2S0 Boys+250 Girls
.2S0 Boy.
-280 Girts
A child who is...
not gaining weight has a plotted growthcurve that flattens off or looks like a flatline between the "reference" curves;
The child's weight should be betweenthe ~reference~ curves.
The plotted growth curve should go inan upward direction
III A child who is...
. losing weight has a
.
plott edgrDWt
.
h curvethat goes in a downward/decliningdirection between the ~reference" curves.
Asa cfildgelsolder, ~helsheshoUdgainweigl'l.~
Quezon Ave Quezon Ave. Ext Baguio UE-Recto1021928-7298Ioc.132 (021927-6878 1074)446-6543 1021735-3007
Dagupan Tuguegarao Naga BacO'lod1075)522-3034 10781844-9583 1054)811-2107 1034)433-0187