Imaging studies in patients with heart failure: Current and ......two-dimensional and M-mode imaging...
12
Imaging studies in patients with heart failure: Current and evolving technologies Helene Glassberg, MD; James Kirkpatrick, MD; Victor A. Ferrari, MD N ew technological advances continue to expand the clin- ical role of echocardiography (echo) in the intensive care unit (ICU), particularly in patients with heart failure. Despite rapid growth in other advanced imaging methods, echo retains many advantages over tomo- graphic techniques such as cardiac mag- netic resonance imaging and cardiac computed tomography. As the most com- mon cardiac noninvasive imaging tech- nology, echo is readily available in most hospitals. Echo can provide rapid bedside cardiac assessment and facilitate emer- gent decision-making for critically ill pa- tients. Major indications for echo in the ICU patient with heart failure include hy- potension of uncertain etiology, suspi- cion of left or right ventricular dysfunc- tion, myocardial infarction, significant valvular disease, prosthetic valve dysfunc- tion, pericardial disease, and unexplained hemodynamic alterations. Perhaps the most basic and useful information ob- tained from echo in patients with heart failure are measures of ventricular func- tion and anatomy. In addition, other im- portant parameters include diastolic and valvular function, hemodynamic mea- surements, and a variety of prognostic and therapeutic markers (Table 1). A re- cent editorial described echo as “the sin- gle most useful diagnostic test in the evaluation of patients with unexplained heart failure” (1). This section will review the vital role of echocardiography in the management of heart failure in the crit- ical care setting. DEFINITION OF ETIOLOGY (SYSTOLIC VS. DIASTOLIC DYSFUNCTION) Echocardiographic Findings of Di- lated Cardiomyopathy. In dilated cardio- myopathy, the left ventricle (LV) becomes more spherical in shape, overall LV sys- tolic function is reduced, wall thickness is normal or reduced, and systolic wall thickening is impaired. On M-mode echo- cardiography, additional features of sys- tolic dysfunction are increased separation of the mitral leaflet E point from the septum, poor mitral and aortic valve opening, and early closure of the aortic valve due to reduced stroke volume (2). In addition, images often reveal left atrial en- largement and/or four-chamber dilation. Right ventricular (RV) dysfunction, either secondary to increased pulmonary pres- sures or to direct involvement of the RV in the pathologic process, may be seen. Doppler echocardiography is used in di- lated cardiomyopathy to assess stroke vol- ume and contractile function; acceleration or deceleration of the mitral regurgitant jet can be used as an analog of dP/dt (the change in LV pressure over time) (3). In a study of patients with LV dysfunction, a dP/dt 600 mm Hg/sec and dP/DT 450 mm Hg/sec predicted worsened survival in patients with heart failure (4). Viral Myocarditis. Evidence suggests that both immune- and viral-mediated cardiac damage occurs in this form of dilated cardiomyopathy (5). There is an extensive list of viral infections impli- cated in the cause of myocarditis; the most common is Coxsackie B. The clini- cal manifestations are variable; however, the majority have antecedent flulike symptoms. Some patients may present with chest pain, LV dysfunction, and ECG changes that may mimic myocardial in- farction. Arrhythmias and conduction disturbances can occur. Echocardiogra- phy is often helpful, but usually not di- agnostic. Severe, diffuse myocarditis can result in dilation of all cardiac chambers. LV dysfunction is usually seen, and may be segmental, reflecting the focal nature of myocarditis. A trabeculated pattern of wall thickening may be seen if inflamma- tion is substantial (6, 7). Echocardiography also can detect in- tracardiac thrombi, functional mitral or tricuspid regurgitation, and pericardial involvement. Patients with fulminant myocarditis usually have near normal LV diastolic dimensions and increased septal thickness, while those with acute myo- carditis tend to have increased LV dia- stolic dimensions and normal septal thickness (8). Familial Dilated Cardiomyopathy. This diagnosis generally is made when From the Cardiovascular Medicine Division, Hospital of the University of Pennsylvania, Philadelphia, PA. Drs. Kirkpatrick and Ferrari have not disclosed any potential conflicts of interest. For information regarding this article, E-mail: [email protected] Copyright © 2007 by the Society of Critical Care Medicine and Lippincott Williams & Wilkins DOI: 10.1097/01.CCM.0000297163.25900.63 Technological advances continue to expand the clinical role of echocardiography in the intensive care unit, particularly in pa- tients with heart failure. It has many advantages over tomo- graphic techniques such as echo cardiac magnetic resonance imaging and cardiac computed tomography, can provide rapid bedside cardiac assessment, and facilitate emergent decision- making for critically ill patients. Image quality problems in the intensive care setting have largely been overcome by the use of harmonic imaging, contrast opacification, and when indicated, transesophageal echocardiography. Newer techniques promise to advance the scope and prognostic power of echocardiography, and to expand the portability and availability of this tool. (Crit Care Med 2008; 36[Suppl.]:S28–S39) S28 Crit Care Med 2008 Vol. 36, No. 1 (Suppl.)
Transcript of Imaging studies in patients with heart failure: Current and ......two-dimensional and M-mode imaging...

Imaging studies in patients with heart failure: Current andevolving technologies
Helene Glassberg, MD; James Kirkpatrick, MD; Victor A. Ferrari, MD
New technological advancescontinue to expand the clin-ical role of echocardiography(echo) in the intensive care
unit (ICU), particularly in patients withheart failure. Despite rapid growth inother advanced imaging methods, echoretains many advantages over tomo-graphic techniques such as cardiac mag-netic resonance imaging and cardiaccomputed tomography. As the most com-mon cardiac noninvasive imaging tech-nology, echo is readily available in mosthospitals. Echo can provide rapid bedsidecardiac assessment and facilitate emer-gent decision-making for critically ill pa-tients. Major indications for echo in theICU patient with heart failure include hy-potension of uncertain etiology, suspi-cion of left or right ventricular dysfunc-tion, myocardial infarction, significantvalvular disease, prosthetic valve dysfunc-tion, pericardial disease, and unexplainedhemodynamic alterations. Perhaps themost basic and useful information ob-tained from echo in patients with heartfailure are measures of ventricular func-tion and anatomy. In addition, other im-portant parameters include diastolic and
valvular function, hemodynamic mea-surements, and a variety of prognosticand therapeutic markers (Table 1). A re-cent editorial described echo as “the sin-gle most useful diagnostic test in theevaluation of patients with unexplainedheart failure” (1). This section will reviewthe vital role of echocardiography in themanagement of heart failure in the crit-ical care setting.
DEFINITION OF ETIOLOGY(SYSTOLIC VS. DIASTOLICDYSFUNCTION)
Echocardiographic Findings of Di-lated Cardiomyopathy. In dilated cardio-myopathy, the left ventricle (LV) becomesmore spherical in shape, overall LV sys-tolic function is reduced, wall thicknessis normal or reduced, and systolic wallthickening is impaired. On M-mode echo-cardiography, additional features of sys-tolic dysfunction are increased separationof the mitral leaflet E point from theseptum, poor mitral and aortic valveopening, and early closure of the aorticvalve due to reduced stroke volume (2). Inaddition, images often reveal left atrial en-largement and/or four-chamber dilation.Right ventricular (RV) dysfunction, eithersecondary to increased pulmonary pres-sures or to direct involvement of the RV inthe pathologic process, may be seen.
Doppler echocardiography is used in di-lated cardiomyopathy to assess stroke vol-ume and contractile function; accelerationor deceleration of the mitral regurgitant jetcan be used as an analog of dP/dt (the
change in LV pressure over time) (3). In astudy of patients with LV dysfunction, adP/dt �600 mm Hg/sec and �dP/DT �450mm Hg/sec predicted worsened survival inpatients with heart failure (4).
Viral Myocarditis. Evidence suggeststhat both immune- and viral-mediatedcardiac damage occurs in this form ofdilated cardiomyopathy (5). There is anextensive list of viral infections impli-cated in the cause of myocarditis; themost common is Coxsackie B. The clini-cal manifestations are variable; however,the majority have antecedent flulikesymptoms. Some patients may presentwith chest pain, LV dysfunction, and ECGchanges that may mimic myocardial in-farction. Arrhythmias and conductiondisturbances can occur. Echocardiogra-phy is often helpful, but usually not di-agnostic. Severe, diffuse myocarditis canresult in dilation of all cardiac chambers.LV dysfunction is usually seen, and maybe segmental, reflecting the focal natureof myocarditis. A trabeculated pattern ofwall thickening may be seen if inflamma-tion is substantial (6, 7).
Echocardiography also can detect in-tracardiac thrombi, functional mitral ortricuspid regurgitation, and pericardialinvolvement. Patients with fulminantmyocarditis usually have near normal LVdiastolic dimensions and increased septalthickness, while those with acute myo-carditis tend to have increased LV dia-stolic dimensions and normal septalthickness (8).
Familial Dilated Cardiomyopathy.This diagnosis generally is made when
From the Cardiovascular Medicine Division, Hospitalof the University of Pennsylvania, Philadelphia, PA.
Drs. Kirkpatrick and Ferrari have not disclosed anypotential conflicts of interest.
For information regarding this article, E-mail:[email protected]
Copyright © 2007 by the Society of Critical CareMedicine and Lippincott Williams & Wilkins
DOI: 10.1097/01.CCM.0000297163.25900.63
Technological advances continue to expand the clinical role ofechocardiography in the intensive care unit, particularly in pa-tients with heart failure. It has many advantages over tomo-graphic techniques such as echo cardiac magnetic resonanceimaging and cardiac computed tomography, can provide rapidbedside cardiac assessment, and facilitate emergent decision-making for critically ill patients. Image quality problems in the
intensive care setting have largely been overcome by the use ofharmonic imaging, contrast opacification, and when indicated,transesophageal echocardiography. Newer techniques promise toadvance the scope and prognostic power of echocardiography,and to expand the portability and availability of this tool. (Crit CareMed 2008; 36[Suppl.]:S28–S39)
S28 Crit Care Med 2008 Vol. 36, No. 1 (Suppl.)

idiopathic dilated cardiomyopathy isfound in two or more closely related fam-ily members. Epidemiologic studies re-port variable rates of inheritance, rangingfrom 20% to �50% (9–11). The weight ofevidence in the literature supports theefficacy (class IIa indication in 2005American College of Cardiology/Ameri-can Heart Association guidelines) ofscreening asymptomatic first-degree rel-atives with an electrocardiogram andechocardiography (12). A prospective co-hort study evaluated �700 asymptomaticfirst- and second-degree relatives of 189patients with idiopathic dilated cardiomy-opathy (13). Echocardiography identified
patients with dilated cardiomyopathy asthose with LV enlargement and systolicdysfunction as defined by a fractionalshortening �25%. Twenty-three percentof relatives had abnormal findings: 4.6%had dilated cardiomyopathy, 15.5% hadLV enlargement without systolic dysfunc-tion, and 2.7% had decreased fractionalshortening �25% without LV enlarge-ment (13).
Left Ventricular Noncompaction. LVnoncompaction, also called LV hypertra-beculation or spongy myocardium, is anuncommon cause of dilated cardiomyop-athy that results from arrest of compac-tion of the loose interwoven meshwork
during fetal development. This diagnosisshould be suspected when heavy LV tra-beculation is noted, particularly at theapex (14, 15). Characteristically, there isa normally compacted epicardial layerand a very thickened (noncompacted) en-docardial layer with trabeculations anddeep recesses (16, 17). Echocardiographiccriteria for diagnosis include the absenceof coexisting cardiac abnormalities and aratio of noncompacted to compactedmyocardium �2:1 at end-systole (Fig. 1).
Other findings on echocardiographyinclude reduced LV systolic function, di-astolic dysfunction, LV thrombi, and ab-normal papillary muscle structure (17).Contrast echocardiography may aid in es-tablishing the diagnosis (18).
Ischemic Cardiomyopathy. The ma-jority of patients with ischemic cardiomy-opathy have known coronary heart dis-ease; however, it may present as an occultdilated cardiomyopathy. Ischemic cardio-myopathy can be difficult to differentiatefrom idiopathic dilated cardiomyopathyby echocardiography. In both forms, LVwall motion abnormalities can be seg-mental. In most patients, ischemic car-diomyopathy is associated with regionalremodeling, and ischemic cardiomyopathyalso tends to exhibit areas of endocardialscarring in the areas of infarction (19).
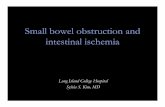
Takotsubo Cardiomyopathy. Takot-subo cardiomyopathy, also called stress-induced or transient LV apical balloon-ing, is an increasingly recognized cardiacdisorder. It is typically triggered by in-tense physical or emotional stress, andpresents similarly to an acute myocardialinfarction. Coronary angiography revealsno significant obstructive disease. Echo-cardiography reveals the characteristicfinding of transient apical dysfunction,with compensatory hyperdynamic func-tion of the base, producing apical bal-looning (20–25) (Fig. 2).
Echocardiographic Features of Hy-pertrophic Cardiomyopathy. Hypertro-phic cardiomyopathy is characterized byincreased LV mass. When present with-out apparent etiology, it is considered tobe a primary hypertrophic cardiomyopa-thy, most frequently genetic in origin.The hypertrophy is typically asymmetricin primary hypertrophic cardiomyopathyand symmetric in secondary disease, suchas hypertensive-mediated hypertrophy(26, 27).
Primary Hypertrophic Cardiomyopa-thy. The most characteristic finding onechocardiography is asymmetric septalhypertrophy, with increased wall thick-
Table 1. Commonly used echocardiographic parameters for the assessment of heart failure in theintensive care setting
Exam Assessments to Be Made During Exam
LV systolic function LV ejection fraction (load dependent)Strain rate (load independent)—in validation process
LV diastolic function Pulsed wave Doppler of the mitral inflowPulmonary venous flowTissue Doppler of the mitral annulusColor M-mode of mitral inflow
Hemodynamics Pulmonary artery pressure (determined using the tricuspid regurgitant jet)Pulmonary artery mean and diastolic pressures from pulmonic
regurgitation jetLV filling pressure (estimated)Inferior vena caval collapsibility index
Prognosis Reduced LV systolic function (LV ejection fraction)Right ventricular enlargement and dysfunctionRestrictive filling pattern
LV, left ventricular.
Figure 1. Noncompaction of the left ventricular myocardium. Parasternal short axis view, just apicalto the papillary muscles, shows intense trabeculation. The depth of the intratrabecular recesses (Crypt)is greater than twice the width of the compacted myocardium (Compacted).
S29Crit Care Med 2008 Vol. 36, No. 1 (Suppl.)

ness localized to the basal septum (26–28). In an uncommon variant of asym-metric septal hypertrophy, the apex is thesite of the most intensive hypertrophy,so-called apical hypertrophy (29). This issometimes difficult to identify by echo-cardiography, because the apex tends tobe more difficult to image, and in somecircumstances it may be helpful to use acontrast agent. The echocardiographicdiagnosis of hypertrophic cardiomyopa-thy is based upon the findings of a hyper-trophied LV with a wall thickness �15mm that is not associated with systemichypertension (30). Classic hypertrophicobstructive cardiomyopathy has the fol-lowing features: asymmetric septal hy-pertrophy, systolic anterior motion of themitral valve, crowding of the LV outflowtract by the mitral apparatus, and partialmidsystolic closure of the aortic valve.When obstructive hypertrophic cardio-myopathy is suspected, it is useful to per-form some sort of provocation during theechocardiogram; the most frequentlyused maneuver is the Valsalva maneuverand, less commonly, a pharmacologicintervention is used, such as amyl ni-
trate inhalation. Provocation can dem-onstrate the dynamic nature of the out-flow tract obstruction and even determineits severity.
Use of Doppler techniques, particu-larly continuous wave, is necessary. Thesystolic flow velocity is measured in theLV outflow tract and midcavity at rest andduring maneuvers (31). Doppler also willrecognize dynamic mitral regurgitationthat often appears in conjunction withoutflow tract obstruction. Systolic ante-rior movement of the mitral valve ontwo-dimensional and M-mode imagingprovides independent evidence of dy-namic obstruction (31, 32) (Fig. 3). Ifobstruction worsens with provocativetesting, the systolic anterior motion ofthe mitral valve also will worsen. Assess-ment of the aortic valve during the prov-ocation will provide secondary evidenceof obstruction by demonstrating midsys-tolic closure. The Valsalva maneuver usu-ally is performed first, and if this fails toprovoke changes, provocation by amyl ni-trate inhalation may be performed.
Hypertensive Cardiomyopathy. Sec-ondary LV hypertrophy is most often a
complication of hypertension. Echocardi-ography is the procedure of choice foridentification, because the sensitivity ofthe various ECG criteria may be as lowas 7% to 35% with mild LV hypertrophyand only 10% to 50% with moderate tosevere disease (33). Current criteria forthe diagnosis of LV hypertrophy on M-mode echocardiography are an LV massindex �134 and �110 g/m2 body sur-face area in men and women, respec-tively (34, 35).
Echocardiographic Features of Re-strictive Cardiomyopathies. Restrictivecardiomyopathies are more difficult to di-agnose with echocardiography and can bedifficult to distinguish from constrictivepericarditis. Restrictive LV filling is char-acterized by a low diastolic volume, nor-mal or only mildly reduced LV ejectionfraction, and abnormal diastolic function.Frequently, the atrial dilation is out ofproportion to the degree of valvular dis-ease (regurgitation or stenosis).
Amyloid Cardiomyopathy. Cardiac in-volvement can occur in primary or sec-ondary amyloidosis or as an isolated car-diac condition in patients with senileamyloidosis. The rigid amyloid fibrils leadto relaxation abnormalities; therefore, di-astolic dysfunction is the most commonand earliest echocardiographic abnormal-ity in cardiac amyloidosis (36). Ulti-mately, systolic dysfunction can develop.
Echocardiography in patients withovert cardiac amyloidosis demonstratessymmetric thickening of the LV wall (of-ten with low voltage noted on electrocar-diography, which is in contrast to thick-ening seen with LV hypertrophy due toprimary hypertrophic or hypertensivecardiomyopathy with high voltage onelectrocardiography), a granular “spar-kled” appearance of the myocardium (thissign is less useful when harmonic imag-ing is performed), small ventricularchambers, thickening of the atrial sep-tum, and dilated atria (37, 38). IncreasedRV wall thickness also may be presentand can be associated with RV diastolicdysfunction (38). Disproportionate RVenlargement also may occur (39, 40). Notuncommonly, there is thickening and re-gurgitation of all valves, and a pericardialeffusion may be present. Although thesparkled appearance is relatively nonspe-cific (39–41), the combination of thisfinding and atrial septal thickening arehighly suggestive of cardiac amyloid (40,41). Valvular abnormalities, such as“functional” mitral regurgitation, mayarise from ventricular dilation.
Figure 2. “Takotsubo” stress-induced cardiomyopathy, apical four-chamber views: (a) end-diastole; and(b) end-systole in the initial echocardiogram showed normal contraction at the base of the heart withakinesis from the midventricle to apex (arrows). Two weeks later, the (c) end-diastolic; and (d)end-systolic frames demonstrated normal contraction of the apex.
S30 Crit Care Med 2008 Vol. 36, No. 1 (Suppl.)

Echocardiographic Findings of Com-plications of Myocardial Infarction.There are three major mechanical com-plications of acute myocardial infarction(MI): rupture of the LV free wall; ruptureof the interventricular septum; and thedevelopment of mitral regurgitation, fre-quently due to partial or complete papil-lary muscle rupture. Echocardiography isthe initial test of choice in detecting eachdisorder. Delayed hospitalization (�24hrs) and postinfarction angina increasethe risk of ventricular rupture in predis-posed patients (42). Rupture occurswithin the first five days after MI in aboutone half of cases and within 2 wks in�90% of cases (42–45). Echocardiogra-phy reveals hemopericardium and find-ings of cardiac tamponade. Subacute rup-ture of the LV free wall can occur whenthrombus forms and the pericardiumseals the perforation. This can develop
into frank rupture with cardiac tampon-ade, or may develop into an aneurysm(44–46). In one study, echocardiographicand hemodynamic indices of cardiac tam-ponade were present in 85% of patients(44). The diagnosis of subacute rupture isconfirmed by transthoracic echocardiog-raphy (47).
Ventricular Septal Rupture. Ventricu-lar septal rupture typically occurs 3–5days after an acute MI. It may, however,develop within the first 24 hrs or as lateas 2 wks. Septal rupture occurs equally inanterior and nonanterior infarctions (48).With anterior MI, the defect is most com-monly found in the apical septum, andwith inferior MI, most often occurs at thebase of the heart. Patients with a rup-tured septum usually present with hypo-tension, biventricular failure, and a newmurmur. The defect can be diagnosed by2-dimensional transthoracic echocardi-
ography with color flow Doppler imaging(42, 49, 50). One small study evaluated 43patients with a post-MI ventricular septaldefect and found that 2-D echocardiogra-phy alone visualized the defect in only40% of the patients (49). The addition ofDoppler color flow demonstrated an areaof turbulent transseptal flow and systolicflow abnormality within the RV in allpatients. Transesophageal echocardiogra-phy may occasionally be necessary (51).
Acute Mitral Regurgitation. . The causesof mitral regurgitation after acute MI in-clude ischemic papillary muscle dysfunc-tion, LV dilation or aneurysm, and papil-lary muscle or chordal rupture (50, 52,53). Papillary muscle rupture is a life-threatening complication of acute MIthat usually occurs within 1 wk after theinfarct (52, 53). The rupture may be par-tial or complete. The diagnosis of papil-lary muscle rupture should be consideredwhen there is hemodynamic compromiseand a new systolic murmur in the settingof an acute myocardial infarction. In asmall echocardiographic study, 43 of 50patients studied had a ventricular septaldefect and seven had papillary muscle rup-ture or severe dysfunction (50). Transtho-racic echocardiography often demonstratesa flail mitral valve segment, and within theLV cavity a highly mobile papillary muscleor chordae can be seen. Not infrequently,because of tachycardia and limited imagequality in acutely ill patients, transesopha-geal echocardiography is required to estab-lish the diagnosis.
RV Infarction. Another important rolefor echocardiography in the setting of anacute myocardial infarction is identifyingRV infarction. Evidence of RV infarctionshould be sought in patients with inferiorST-elevation infarction, particularlythose with the triad of hypotension, clearlungs, and elevated jugular venous pres-sure. Echocardiography may show RV di-lation, abnormal interventricular septalmotion, and RV dysfunction (54).
Echocardiography and UnexplainedHypotension. There are various findingson the echocardiogram that may be help-ful in identifying the etiology of hypoten-sion in the ICU patient. A small ventric-ular cavity with hypercontractilefunction is usually consistent with hypovo-lemia or vasodilation (e.g., sepsis, anaphy-lactic shock). In hypotension due to cardio-genic shock, the LV ejection fraction isusually severely reduced, and the LV sizemay be normal or dilated, depending on theetiology of the dysfunction. In chronic isch-emic heart disease, the LV is often dilated,
Figure 3. Asymmetric septal hypertrophy with obstructive cardiomyopathy: (a) apical five- and (b)apical long-axis views of the left ventricle demonstrating severe systolic anterior motion of the mitralvalve apparatus resulting in obstruction of the left ventricular outflow tract (LVOT; white arrows). c,continuous wave Doppler technique quantifies a peak systolic gradient of 104 mm Hg across theobstruction during a Valsalva (VALS) maneuver.
S31Crit Care Med 2008 Vol. 36, No. 1 (Suppl.)

whereas in acute regional or global isch-emia (“stunning”), the LV may remain nor-mal in size, but with reduced contractilefunction. Further assessment can be madewith a variety of Doppler-echo hemody-namic measures.
HEMODYNAMIC ASSESSMENT
Many studies have demonstrated thelimitations of the physical examinationfor assessment of volume status (55, 56).Others have shown that invasive moni-toring with central venous and pulmo-nary artery catheters, while accurate,sometimes carries significant risk withlittle or no demonstrable benefit (57). Arecent report demonstrated increased in-hospital adverse events and no benefitregarding mortality or duration of hospi-
talization using pulmonary artery cathe-ters to guide therapy in heart failure pa-tients (58). Doppler echocardiographycan measure hemodynamic status withgreater accuracy than the physical exam-ination and less risk than invasive tech-niques. In selected patients, Doppler echotechniques effectively can function as an“echo Swan,” estimating cardiac output(59–61); right atrial pressure (62, 63);pulmonary artery systolic, mean, and di-astolic pressures (64–66); and LV fillingpressure (67–69) (Table 2), (Fig. 4).
ASSESSING PROGNOSIS/GUIDING THERAPY
Important prognostic information canbe obtained from echocardiography inmany cardiac disorders. In dilated cardio-
myopathy, it had been shown that thereis a considerably worsened prognosiswhen there is RV dilation and/or a re-duced RV ejection fraction (70, 71). Apotentially useful measurement of RVfunction is the tricuspid annular planesystolic excursion (descent of the base).In one report, an excursion �14 mmadded significant prognostic informationto the other clinical and echocardio-graphic findings (72). Mitral inflow pat-terns can identify restrictive physiologybecause of advanced grade diastolic dys-function. Grade 3 diastolic dysfunctiondescribes a restrictive filling pattern thatimproves with maneuvers to reduce leftatrial pressure (Valsalva) and/or heartfailure therapy, while grade 4 diastolicdysfunction is characterized by persis-
Figure 4. The mitral E/e’ ratio for left ventricular filling: (left) the E velocity is obtained as the peak of the early diastolic blood flow velocity from the spectralDoppler signal at the mitral valve leaflet tips; (right) the e’ velocity is obtained as the peak of the early diastolic myocardial relaxation velocity from the tissueDoppler signal at the septal annulus of the mitral valve. The ratio shown in this figure is 60/8 � 7.5, consistent with normal filling pressures.
Table 2. Echocardiographically determined hemodynamic parameters
Measurement Doppler Echo Technique Doppler Echo Measurement or Formula Limitations
CO 1. PW Doppler in LVOT for VTI CO � VTI � (d/2)2 � � � HR 1. Overestimated in AI2. LVOT diameter (d) 2. Measurement errors of LVOT diameter
RAP Inferior vena caval size (cm) and% collapsibility
1. �1.7 cm and �50% � RAP �5 mm Hg Limited application in mechanicallyventilated patients2. 1.7–2.0 cm and �50% � RAP 5–10 mm Hg
3. 1.7–2.0 cm and �50% � RAP �10 mm Hg4. �2 cm and �50% � RAP 15–20 mm Hg
PA systolic pressure Maximum tricuspid regurgitantvelocity by CW Doppler
4 � velocity2 � RAP 1. Not valid in pulmonic stenosis2. Requires tricuspid regurgitation3. Nonparallel alignment of CW jet leads
to underestimationPA mean pressure Maximum pulmonary regurgitant
velocity by CW Doppler4 � velocity2 1. Requires pulmonic valve regurgitation
2. Nonparallel alignment of CW jet leadsto underestimation
PA diastolicpressure
End diastolic pulmonary regurgitantvelocity by CW Doppler
4 � velocity2 � RAP 1. Requires pulmonic valve regurgitation2. Nonparallel alignment of CW jet leads
to underestimationPCWP Multiple techniques 1. E/e� �8 � PCWP �15 mm Hg E/e� 8–15 � PCWP indeterminate
Ratio of maximum early mitralinflow velocity (E) by PW Dopplerto maximum early diastolic mitralannular velocity by tissue Doppler (e�)
2. E/e� �15 � PCWP �15 mm Hg
CO, cardiac output; PW, pulse wave; LVOT, left ventricular outflow tract; VTI, velocity time integral; HR, heart rate; AI, aortic insufficiency; RAP, rightatrial pressure; PA, pulmonary artery; Max, maximum; CW, continuous wave; PCWP, pulmonary capillary wedge pressure.
S32 Crit Care Med 2008 Vol. 36, No. 1 (Suppl.)

tence of the restrictive filling pattern de-spite these interventions. The advanceddiastolic dysfunction patterns predict apoor prognosis and can be useful in guid-ing therapy (73, 74).
An analysis of one study was con-ducted to identify echocardiographic pre-dictors of survival among patients withnonischemic cardiomyopathy and heartfailure, and to assess the potential addi-tional prognostic significance of theseechocardiographic findings as comparedwith clinical predictors. Seven of ten rou-tine echocardiographic findings were sig-nificantly associated with death. Theseincluded mitral regurgitation, LV ejec-tion fraction �20%, LV size, and restric-tive filling pattern. The study concludedthat these echocardiographic parameters,when added to the clinical examination,significantly improve the ability to deter-mine prognosis among patients withnonischemic cardiomyopathy and heartfailure (75).
Therapeutic Guidance
Echo also is useful in guiding therapy,by selecting patients who may benefitfrom an assist device or surgical interven-tion for the various complications out-lined above. Serial echocardiography as-sists in the evaluation of efficacy of thetherapy. Echo also may provide helpfulclues as to whether a patient with heartfailure should be anticoagulated, as is in-dicated when a thrombus is detected.
Harmonic Imaging andMicrobubble Contrast
Echo in ICU patients is limited by anumber of technical problems, includinglung disease, body habitus, subcutaneousemphysema, mechanical ventilation, ban-dages, chest tubes and other treatmentdevices, inability to cooperate, and sub-optimal positioning. The percentage ofICU studies that lack adequate ultrasoundimages when performed by trainedsonographers using full feature echocar-diographic platforms is 26% to 30% (76,77). Harmonic imaging and echocardio-graphic contrast agents for chamberopacification are now standard measuresthat make LV and RV imaging possible inalmost all patients.
Harmonic imaging is the default im-aging mode on most echocardiographicmachines. Echocardiographic transduc-ers emit ultrasound at a specific, “funda-mental” frequency. When the beam
strikes a cardiac structure, reflected sig-nals are produced at the fundamental fre-quencies and also multiples of the funda-mental frequencies, termed harmonics.By listening for these harmonic frequen-cies, the ultrasound transducer receivesmuch more information from which toconstruct echocardiographic images, re-sulting in improved definition of cardiacstructures, especially the blood–endocar-dial interface (78).
Echocardiographic contrast agentsinitially were developed for use with har-monic imaging (79). These agents arecomposed of an inert gas enclosed in lipidspheres, which are smaller than red bloodcells. The spheres reflect ultrasoundwaves much more intensely than bloodand tissue. The microbubbles cross thepulmonary circulation, and can thereforebe used to opacify the LV, improving en-docardial definition. Several studies havedemonstrated an important role for con-trast echocardiography in the ICU forevaluation of cardiac function (80) anddetection of wall motion abnormalities(76) (Fig. 5).
TRANSESOPHAGEALECHOCARDIOGRAPHY
Although transthoracic echocardiog-raphy, aided by harmonic imaging andcontrast administration, may answermany of the clinical questions that arisein the ICU patient, there are still patientsand indications for which transthoracicimaging is inadequate. One study demon-strated that a new diagnosis was estab-lished or another excluded by transesoph-ageal echocardiography (TEE) in 45% ofpatients after cardiac surgery, and thatTEE had an impact on management in73% of cases (81). Dr. Costachescu andcolleagues (82) reported the diagnosticsuperiority of TEE compared with con-ventional monitoring with pulmonary ar-tery catheters in determining the etiologyof hemodynamic instability in the earlypostoperative period in cardiac surgerypatients.
Indications. TEE may be useful inmany circumstances, including LVand/or RV failure, tamponade, hypovole-mia, and valvular dysfunction (83). In oneseries, the clinical indications for TEEwere: cardiac sources of embolism (36%);endocarditis (14%); prosthetic heartvalve function (12%); native valvular dis-ease, aortic dissection or aneurysm, orintracardiac tumor, mass, or thrombus(6% to 8% each); and congenital heart
disease (4%) (84). In another study exam-ining the utility of TEE in the ICU, un-explained hypotension accounted for 40%of cases, suspected endocarditis 27%, as-sessment of ventricular function 15%,pulmonary edema 5%, cardiac source ofembolism 4%, and assessment of theaorta and others 5% (85). In this study,TEE revealed the cause of instability in67% of hypotensive patients, leading to achange in management, including rec-ommending surgery in 22%. Overall,TEE led to a significant change in man-agement in 32% of cases. TEE is a uniquediagnostic modality, in that it also can beperformed during elective or emergentsurgery to assess LV and RV function oradequacy of valve repair/replacement,guide placement of an atrial or ventricu-lar septal patch, and assess the adequacyof defect closure. It is frequently used toassess the etiology of intraoperative he-modynamic instability in noncardiac sur-gery, and for guiding management duringdifficulty in separating from cardiopulmonarybypass in cardiac surgery. Emergent bed-side procedures in the ICU, such as theinstitution of extracorporeal membraneoxygenation or percutaneous LV assistdevice placement, also are aided by TEE.
Infective endocarditis is a commonpresenting diagnosis or complication inICU patients. Infective endocarditis hasbeen reported to be the second mostcommon indication for performance ofechocardiography in the ICU (85, 86).Certainly, endocarditis and its complica-tions can be an important cause of heartfailure, and the consequences of un-treated endocarditis can be devastating.Prompt recognition and treatment is ofutmost importance. The typical echocar-diographic features of infective endocar-ditis include: a mobile intracardiac masson a valve or on a catheter, pacing wire,or other device; new valvular regurgita-tion; intracardiac abscess; or dehiscenceof a prosthetic valve (87). Sensitivity forthe echocardiographic diagnosis of infec-tive endocarditis has been reported to be58% to 62% and 88% to 98% for transtho-racic and TEE studies, respectively (88). Inthe ICU, transthoracic sensitivity for infec-tive endocarditis is often poorer, as imagesare frequently technically limited. TEE issuperior to transthoracic echo in diagnos-ing complications of endocarditis such asabscess, fistula, and chordal rupture of themitral valve. TEE in the ICU for evaluationof infective endocarditis is indicated incases where the clinical suspicion is highand a transthoracic study is nondiagnostic,
S33Crit Care Med 2008 Vol. 36, No. 1 (Suppl.)

where prosthetic valve endocarditis orcomplications of known endocarditis aresuspected, and in the setting of Staphylo-coccus aureus bacteremia with an un-known source or persistent bacteremia onantibiotic therapy (83, 89).
Caveats. There are several importantlimitations that must be kept in mindwhen employing TEE in the ICU setting.TEE does not provide all of the same
views obtainable from transthoracic im-aging. It is often difficult to obtain paral-lel alignment from which to accuratelymeasure Doppler velocities, particularlythrough the aortic and pulmonic valves.Stenosis of these valves may therefore beunderestimated. It may be preferable(and more diagnostic) to assess the pul-monic valve and LV apex using transtho-racic echo, since these structures are in
the “far field” of the TEE probe. TEE alsois limited in the assessment of hemody-namic variables, because patients are fre-quently sedated for the procedure, lead-ing to alterations in loading conditions.
Guidelines for TEE competence havebeen published by the American Societyof Echocardiography (90). Generally, TEEis safe when performed by an experiencedoperator (91, 92). Contraindications toTEE examination include: esophagealstricture or malignancy, recent esopha-geal ulcer or hemorrhage, Zenker’s diver-ticulum, unevaluated odynophagia ordysphagia, and altered mental status oran uncooperative patient. In the traumapatient, TEE is not used when there isesophageal orofacial or oropharyngealtrauma, or other disorders that precludeplacement of the TEE probe.
EMERGING TECHNOLOGIES
New Doppler echo techniques havebeen developed to improve cardiac imag-ing and may become clinically importantfor heart failure patients admitted to acritical care unit. Real-time 3-dimen-sional echocardiography (RT3DE) andhand-carried ultrasound (HCU) technol-ogy, in particular, hold promise to im-prove heart failure patient managementin the ICU setting.
Real-time 3-DimensionalEchocardiography
LV Assessment. Three-dimensionalechocardiography traditionally has beenhampered by the requirements for te-dious reconstruction of multiple 2-D im-ages. The development of new matrix ar-ray transducers allows collection of fullvolume data sets from a single view (Fig.6). RT3DE has multiple clinical applica-tions for the heart failure patient, includ-ing several studies that have demon-strated increased precision and lowerinter- and intraobserver variability in themeasurement of LV volumes and LV ejec-tion fraction compared with 2-D echocar-diography (93, 94, 95).
The concurrent imaging of all ventric-ular walls may help improve and auto-mate the detection of wall motion abnor-malities. Traditional techniques rely onsubjective assessment of wall motion andthickening, but tracking of segmentalmotion from 3-D data sets allows for gen-eration of regional displacement curvesthat may result in less variability thanconventional wall motion analysis. Dr.
Figure 5. Microbubble contrast for left ventricular opacification: (a) 2-dimensional imaging in theapical four-chamber view with extremely poor endocardial definition limits global (ejection fraction)and regional myocardial function assessment in a patient with limited echocardiographic windows; (b)the addition of microbubble contrast dramatically improves endocardial definition.
S34 Crit Care Med 2008 Vol. 36, No. 1 (Suppl.)

Corsi and colleagues (96) recently haveshown the feasibility of an automated 3-Dendocardial border detection method thatfurther improves reproducibility of wallmotion assessment and volume and ejec-tion fraction calculations.
Mitral Valve Assessment. RT3DE alsoimproves mitral valve assessment. Tradi-tional 2-D evaluation has significant lim-itations because the mitral valve annulusis saddle-shaped and cannot be fully im-aged in a single 2-D plane (97). As aresult, mitral regurgitant jets often areinadequately characterized by 2-D imag-ing, especially when eccentric. The cur-rent Doppler and color Doppler methodsfor calculating regurgitant severity in-volve geometric assumptions that pro-duce substantial errors in noncentral jets(98, 99). Misclassification of mitral regur-gitation severity can lead to significantmissteps in clinical management, and adeleterious outcome for patients, partic-ularly those in an ICU setting.
Three-dimensional echocardiographycan improve the assessment of annularmorphology and may prove especiallybeneficial in facilitating anatomical defi-nition of leaflet prolapse and flail leafletsegments (100, 101). RT3DE data sets canbe manipulated to show mitral anatomyfrom an atrial or ventricular perspective,potentially improving preoperative plan-
ning, and identify important structuralcharacteristics for cardiac surgeons (102,103). Semiautomated techniques for themeasurement of mitral valve leaflet tent-ing and annular size may one day predictwhether patients will benefit from mitralvalve replacement or repair, ventricularreconstruction strategies, or medicaltherapy alone (104). Three-dimensionalimaging of the mitral regurgitant jet mayallow more accurate quantification of re-gurgitation severity (105). RT3DEplanimetry of the mitral valve area alsomay be superior to invasive methods forassessing the severity of mitral stenosis(105, 106).
Limitations. There are significant lim-itations to transthoracic RT3DE. The ob-tainable frame rate, and therefore imagequality, is significantly reduced comparedwith conventional 2-D echocardiography,and tachycardic patients may thereforehave reduced image quality. Patients withpoor acoustic windows on 2-D imagingare likely to have even poorer 3-D images.Current generation 3-D systems requirethe integration of several cardiac cyclesto produce a full-volume rendering;therefore, arrhythmias and respiratory ortranslational motion can introduce sig-nificant artifacts. The 3-D transducer isconsiderably larger than conventional2-D transducers and does not always fit
well into intercostal spaces or betweentubes and dressings, thereby limiting itsapplicability for many ICU patients. Fur-ther developments in transthoracicRT3DE, including contrast-enhancedRT3DE (107, 108) as well as real-time 3-DTEE (109, 110), hold significant promiseto overcome these difficulties. There willremain, however, an important learningcurve for both the sonographer perform-ing RT3DE studies and the physician whointerprets them.
Hand-Carried Ultrasonography
The recent development of high qual-ity miniaturized echocardiographic plat-forms has created new ways to applyechocardiography to the detection andmanagement of heart failure in the ICU.
Applications. The findings from severalstudies (111–113) suggest that applicationof HCU in the ICU setting should be specif-ically targeted. Attempts to perform fullechocardiographic examinations can leadto unacceptable rates of false negatives, es-pecially when assessing valvular function.RV and LV function and effusions can beadequately imaged with HCU in limited,screening examinations. Full feature echo-cardiography is preferable, when available,but during periods when echo availabilitymight be limited, HCU can extend the abil-ity of the physical examination to definecardiac status and guide important deci-sions. Furthermore, the repeated use offull-feature echocardiography to track clin-ical status may not be feasible or cost-effective. HCU has the potential to providefrequent, serial, and rapid noninvasivemeasures of the response to interventions.
HCU Operators. Who performs thetargeted HCU exam is of paramount im-portance. Studies have tested use by op-erators at many different levels of train-ing—from medical students to attendingcardiologists—and parameters from fullechocardiographic examinations to lim-ited estimation of right atrial pressurefrom collapse of the inferior vena cava.While the official recommendations fromthe American Society of Echocardiogra-phy recognize the potential of miniatur-ized technology to provide adequate im-age quality to constitute a fullexamination (if performed and inter-preted by appropriately trained imagers[level 2 echocardiographic training �150 examinations and 300 interpreta-tions]) (114), many experts regard the
Figure 6. In real-time 3-dimensional echocardiographic assessment of left ventricular size and wallmotion, a full volume acquisition is performed and the endocardium is semiautomatically traced in the(a) apical four-chamber; (b) apical two-chamber; and (c) short-axis views to yield an endocardial castof the left ventricle, which can be (d) color-coded to demonstrate individual wall segments.
S35Crit Care Med 2008 Vol. 36, No. 1 (Suppl.)

greatest utility of HCU in terms of exten-sion of the physical examination or mea-surement of specific parameters (115). Inother words, HCU does not replace a fullechocardiogram, particularly in a com-plex ICU patient.
The use of sonographers and echocar-diographers for frequent, repeated mea-sures of cardiac status in the ICU duringoff-hour times is not feasible or cost-effective. Intensivists and other physi-cians have demonstrated acceptable accu-racy in the ICU setting, but one study,performed in an outpatient setting, dem-onstrated acceptable sensitivity fornurses in screening patients for occult LVsystolic dysfunction with an HCU device(116). Training in image acquisition andinterpretation is a necessity. A carefullyperformed study that examined a spec-trum of training concluded that adequateskill could be obtained following 20–40practice examinations with one-on-oneinstruction (117).
Limitations. The reduced image qual-ity of HCU devices, especially when oper-ated by nonsonographers, exacerbates theabove-mentioned difficulties in obtainingadequate transthoracic images in ICU pa-tients (118). Furthermore, many of theHCU devices lack many important modal-ities available on standard platforms, in-cluding phased array transducers, fullcolor Doppler (instead of power colorDoppler), harmonic imaging, pulsed andcontinuous wave Doppler, M-mode, andthe ability to export images in a univer-sally-readable format for off-line analysis.The latest generation devices includemost of these features, albeit at consider-ably increased cost.
Other EmergingEchocardiographic Techniques
Several other novel echo techniquesmay prove to be useful for heart failurepatients in the ICU setting. Intracardiacechocardiography currently is used toguide a variety of percutaneous proce-dures, from pulmonary vein ablations tomitral valvuloplasties (119). In the ICUsetting, intracardiac echocardiographymay prove particularly useful for patientsin whom TEE is precluded, such aspostesophagectomy patients with atrialfibrillation in need of cardioversion. Anongoing study is comparing the accuracyof intracardiac echocardiography to thatof TEE for the detection of left atrialappendage thrombi (120).
Recent developments in tissue Dopp-ler imaging and tissue tracking enablethe measurement of longitudinal, cir-cumferential, and torsional cardiac me-chanics. Tissue Doppler imaging mea-sures the velocity of myocardial motionbut is limited by its dependence on aDoppler signal parallel to the direction ofmyocardial motion. Tissue trackingmethods, such as speckle tracking tech-niques, identify unique speckles withinthe myocardium and track their motionin three dimensions throughout the car-diac cycle. These techniques are sensitivemarkers for abnormal wall motion, andcan assess the degree of ventricular dys-synchrony. These applications may proveparticularly useful in the heart failurepopulation, because up to one third ofpatients fail to respond to biventricularpacing, and many patients demonstratedyssynchrony by echocardiographic crite-ria but lack a widened QRS complex—acrucial component of the current indica-tions for biventricular pacemaker place-ment (121). Heart failure patients in theICU may benefit from echocardiographi-cally guided optimization of pacemakertiming intervals to improve ventriculardiastolic filling and cardiac output (122).
CONCLUSION
The use of echocardiography in the ICUsetting provides important diagnostic andprognostic information to guide therapy forthe heart failure patient. Echo is safe, ac-curate, portable, and widely available, andcontinues to have significant advantagesover CT and MRI studies for ICU patients.Limitations in image quality in the ICUsetting have been largely overcome by theuse of harmonic imaging, contrast opacifi-cation, and when indicated, transesopha-geal echocardiography. Newer echo tech-niques promise to advance the scope andprognostic power of echocardiography, andto expand the portability and availability ofthis “single most useful” test.
REFERENCES
1. Dec WG Jr: [various articles on AmericanCollege of Cardiology 52nd Annual Scien-tific Session] Medscape Cardiology March2003. Available at: http://www.medscape.com/cardiology?src�mp
2. Gardin JM, Tommaso CL, Talano JV: Echo-graphic early systolic partial closure (notch-ing) of the aortic valve in congestive cardio-myopathy. Am Heart J 1984; 107:135–142
3. Loutfi H, Nishimura RA: Quantitative eval-uation of left ventricular systolic function
by Doppler echocardiographic techniques.Echocardiography 1994; 11:305–314
4. Kolias TJ, Aaronson KD, Armstrong WF:Doppler-derived dP/dt and �dP/dt predictsurvival in congestive heart failure. J AmColl Cardiol 2000; 36:1594–1599
5. Kawai C: From myocarditis to cardiomyop-athy: Mechanisms of inflammation and celldeath. Learning from the past for the fu-ture. Circulation 1999; 99:1091–1100
6. Chandraratna PAN, Nimalasuriya A, ReidCL, et al: Left ventricular asynergy in acutemyocarditis. JAMA 1983; 250:1428–1430
7. Ferdeghini EM, Pinamonti B, Picano E, etal: Quantitative texture analysis in echocar-diography: Application to the diagnosis ofmyocarditis. J Clin Ultrasound 1991; 19:263–270
8. Felker GM, Boehmer JP, Hruban RH, et al:Echocardiographic findings in fulminantand acute myocarditis. J Am Coll Cardiol2000; 36:227–232
9. Burkett EL, Hershberger RE: Clinical andgenetic issues in familial dilated cardiomy-opathy. J Am Coll Cardiol 2005; 45:969–981
10. Codd MB, Sugrue DD, Gersh BJ, et al: Ep-idemiology of idiopathic dilated and hyper-trophic cardiomyopathy: A population-based study in Olmsted County, Minnesota,1975–1984. Circulation 1989; 80:564–572
11. Michels VV, Moll PP, Miller FA, et al: Thefrequency of familial dilated cardiomyopa-thy in a series of patients with idiopathicdilated cardiomyopathy. N Engl J Med 1992;326:77–82
12. Hunt SA, Abraham WT, Chin MH, et al:ACC/AHA 2005 guideline update for the di-agnosis and management of chronic heartfailure in the adult: a report of the Ameri-can College of Cardiology/American HeartAssociation Task Force on Practice Guide-lines (Writing Committee to Update the2001 Guidelines for the Evaluation andManagement of Heart Failure): developed incollaboration with the American College ofChest Physicians and the International So-ciety for Heart and Lung Transplantation:endorsed by the Heart Rhythm Society. Cir-culation 2005; 112:e154–e235
13. Mahon NG, Murphy RT, MacRae CA, et al:Echocardiographic evaluation in asymp-tomatic relatives of patients with dilatedcardiomyopathy reveals preclinical disease.Ann Intern Med 2005; 143:108–115
14. Ritter M, Oechslin E, Sutsch G, et al: Iso-lated noncompaction of the myocardium inadults. Mayo Clin Proc 1997; 72:26–31
15. Weiford BC, Subbarao VD, Mulhern KM:Noncompaction of the ventricular myocar-dium. Circulation 2004; 109:2965–2971
16. Jenni R, Oechslin E, Schneider J, et al:Echocardiographic and pathoanatomicalcharacteristics of isolated left ventricularnon-compaction: A step towards classifica-tion as a distinct cardiomyopathy. Heart2001; 86:666–671
17. Frischknecht BS, Jost CH, Oechslin EN, etal: Validation of noncompaction criteria in
S36 Crit Care Med 2008 Vol. 36, No. 1 (Suppl.)

dilated cardiomyopathy, and valvular andhypertensive heart disease. J Am Soc Echo-cardiogr 2005; 18:865–872
18. De Groot-de Laat LE, Krenning BJ, ten CateFJ, et al: Usefulness of contrast echocardi-ography for diagnosis of left ventricularnoncompaction. Am J Cardiol 2005; 95:1131–1134
19. Felker CM, Thompson RE, Hare JM, et al:Underlying causes and long-term survivalin patients with initially unexplained car-diomyopathy. N Engl J Med 2000; 342:1077–1122
20. Tsuchihashi K, Ueshima K, Uchida T, et al:Transient left ventricular apical ballooningwithout coronary artery stenosis: A novelheart syndrome mimicking acute myocar-dial infarction. Angina Pectoris-MyocardialInfarction Investigations in Japan. J AmColl Cardiol 2001; 38:11–18
21. Abe Y, Kondo M, Matsuoka R, et al: Assess-ment of clinical features in transient leftventricular apical ballooning. J Am CollCardiol 2003; 41:737–742
22. Desmet WJ, Adriaenssens BF, Dens JA: Api-cal ballooning of the left ventricle: Firstseries in white patients. Heart 2003; 89:1027–1031
23. Bybee KA, Prasad A, Barsness GW, et al:Clinical characteristics and thrombolysis inmyocardial infarction frame counts inwomen with transient left ventricular apicalballooning syndrome. Am J Cardiol 2004;94:343–346
24. Dec GW: Recognition of the apical balloon-ing syndrome in the United States. Circu-lation 2005; 111:388–390
25. Aurigemma GP, Tighe DA: Echocardiogra-phy and reversible left ventricular dysfunc-tion. Am J Med 2006; 119:18–21
26. Maron BJ, Nichols PF 3rd, Pickle LW, et al:Patterns of inheritance in hypertrophiccardiomyopathy: Assessment by M-modeand two-dimensional echocardiography.Am J Cardiol 1984; 53:1087–1094
27. Ciro E, Nichols PD, Maron BJ: Heteroge-neous morphologic expression of geneti-cally transmitted hypertrophic cardiomyop-athy. Two-dimensional echocardiographicanalysis. Circulation 1983; 67:1227–1233
28. Nair CK, Kudesia V, Hansen D, et al: Echo-cardiographic and electrocardiographiccharacteristics of patients with hypertro-phic cardiomyopathy with and without mi-tral annular calcium. Am J Cardiol 1987;59:1428–1430
29. Maron BJ, Bonow RO, Seshagiri TN, et al:Hypertrophic cardiomyopathy with ventric-ular septal hypertrophy localized to the api-cal region of the left ventricle (apical hyper-trophic cardiomyopathy). Am J Cardiol1982; 49:1838–1848
30. Maron BJ, Gardin JM, Flack JM, et al: As-sessment of the prevalence of hypertrophiccardiomyopathy in a general population ofyoung adults: Echocardiographic analysis of4111 subjects in the CARDIA study. Circu-lation 1995; 92:785–789
31. Panza JA, Petrone RK, Fananapazir L, et al:Utility of continuous wave Doppler echocar-diography in the non-invasive assessment ofleft ventricular outflow tract pressure gra-dient in patients with hypertrophic cardio-myopathy. J Am Coll Cardiol 1992; 19:91–99
32. Pollick C, Morgan CD, Gilbert BW, et al:Muscular subaortic stenosis: The temporalrelation between systolic anterior motion ofthe anterior mitral valve leaflet and thepressure gradient. Circulation 1982; 66:1087–1094
33. Devereux RB: Is the electrocardiogram stilluseful for detection of left ventricular hy-pertrophy? Circulation 1990; 81:1144–1146
34. Abergel E, Tase M, Bohlender J, et al: Whichdefinition for echocardiographic left ven-tricular hypertrophy? Am J Cardiol 1995;75:498–502
35. Devereux RB, Lutas EM, Casale PN, et al:Standardization of M-mode echocardio-graphic left ventricular anatomic mea-surements. J Am Coll Cardiol 1984;4:1222–1230
36. Roberts WC, Waller BF: Cardiac amyloidosiscausing cardiac dysfunction: Analysis of 54necropsy patients. Am J Cardiol 1983; 52:137–146
37. Siqueira-Filho AG, Cuhna CLP, Tajik AJ, etal: M-mode and two-dimensional echocar-diographic features in cardiac amyloidosis.Circulation 1981; 63:188–196
38. Klein AL, Hatle LK, Burstow DJ, et al: Com-prehensive Doppler assessment of rightventricular diastolic function in cardiacamyloidosis. J Am Coll Cardiol 1990; 15:99–108
39. Falk RH, Plenn JF, Deering T, et al: Sensi-tivity and specificity of echocardiographicfeatures of cardiac amyloidosis. Am J Car-diol 1987; 59:418–422
40. Nicolosi GL, Pavan D, Lestuzzi C, et al:Prospective identification of patients withamyloid heart disease by two-dimensionalechocardiography. Circulation 1984; 70:432–437
41. Bhandari AK, Nanda NC: Myocardial texturecharacterization by two-dimensional echo-cardiography. Am J Cardiol 1983; 51:817–825
42. Reeder GS: Identification and treatment ofcomplications of myocardial infarction.Mayo Clin Proc 1995; 70:880–884
43. Figueras J, Cortadellas J, Calvo F, et al:Relevance of delayed hospital admission ondevelopment of cardiac rupture duringacute myocardial infarction: Study in 225patients with free wall, septal, or papillarymuscle rupture. J Am Coll Cardiol 1998;32:135–139
44. Purcaro A, Costantini C, Ciampani N, et al:Diagnostic criteria and management of sub-acute ventricular free wall rupture compli-cating acute myocardial infarction.Am J Cardiol 1997; 80:397–405
45. Oliva PB, Hammill SC, Edwards WD: Car-diac rupture: A clinically predictable com-
plication of acute myocardial infarction; re-port of 70 cases with clinicopathologiccorrelations. J Am Coll Cardiol 1993; 22:720–726
46. Lopez-Sendon J, Gonzalez A, Lopez de Sa E,et al: Diagnosis of subacute ventricular wallrupture after acute myocardial infarction:Sensitivity and specificity of clinical, hemo-dynamic, and echocardiographic criteria.J Am Coll Cardiol 1992; 19:1145–1153
47. McMullan MH, Maples MD, Kilgore TL Jr, etal: Surgical experience with left ventricularfree wall rupture. Ann Thorac Surg 2001;71:1894–1898
48. Radford MJ, Johnson RA, Daggett EM Jr, etal: Ventricular septal rupture: A review ofclinical and physiologic features and ananalysis of survival. Circulation 1981; 64:545–553
49. Bishop HL, Gibson RS, Stamm RB, et al:Role of two-dimensional echocardiographyin the evaluation of patients with ventricu-lar septal rupture postmyocardial infarc-tion. Am Heart J 1981; 102:965–971
50. Smyllie JH, Sutherland GR, Geusken R, etal: Doppler color flow mapping in the diag-nosis of ventricular septal rupture andacute mitral regurgitation after myocardialinfarction. J Am Coll Cardiol 1990; 15:1449–1455
51. Moursi MH, Bhatnagar SK, Vilacosta I, et al:Transesophageal echocardiographic assess-ment of papillary muscle rupture. Circula-tion 1996; 94:1003–1009
52. Lavie CJ, Gersh BJ: Mechanical and electri-cal complications of acute myocardial in-farction. Mayo Clin Proc 1990; 65:709–730
53. Picard MH, Davidoff R, Sleeper LA, et al:Echocardiographic predictors of survivaland response to early revascularization incardiogenic shock. Circulation 2003; 107:279–284
54. Cheitlan MD, Armstrong WF, AurigemmaGP, et al: ACC/AHA/ASE 2003 guideline up-date for the clinical application of echocar-diography: A report of the American Collegeof Cardiology/American Heart AssociationTask Force on Practice Guidelines (ACC/AHA/ASE Committee to Update the 1997Guidelines for the Clinical Application ofEchocardiography). American College ofCardiology Web Site. Available at: www.acc.org/clinical/guidleines/echo/index.pdf. Ac-cessed August 1, 2007
55. Eisenberg PR, Jaffe AS, Schuster DP: Clin-ical evaluation compared to pulmonary ar-tery catheterization in the hemodynamicassessment of critically ill patients. CritCare Med 1984; 12:549–553
56. Demeria DD, MacDougall A, Spurek M, etal: Comparison of clinical measurement ofjugular venous pressure versus measuredcentral venous pressure. Chest 2004; 126:747S.
57. Connors AF Jr, Speroff T, Dawson NV, et al:The effectiveness of right heart catheteriza-tion in the initial care of critically ill pa-
S37Crit Care Med 2008 Vol. 36, No. 1 (Suppl.)

tients. SUPPORT Investigators. JAMA 1996;276:889–897
58. Binanay C, Califf RM, Hasselblad V, et al.Evaluation study of congestive heart failureand pulmonary artery catheterization effec-tiveness: The ESCAPE trial. JAMA 2005;294:1625–1633
59. Lewis JF, Kuo LC, Nelson JG, et al: PulsedDoppler echocardiographic determinationof stroke volume and cardiac output: Clin-ical validation of two new methods usingthe apical window. Circulation 1984; 70:425–431
60. Dubin I, Wallerson DC, Codv RJ, et al: Com-parative accuracy of Doppler echocardio-graphic methods for clinical stroke volumedetermination. Am Heart J 1990; 120:ll6–123
61. Dabaghi SF, Rokey R, Rivera JM, et al: Com-parison of echocardiographic assessment ofcardiac hemodynamics in the intensive careunit with right-sided cardiac catheteriza-tion. Am J Cardiol 1995; 76:392–395
62. Ommen SR, Nishimura RA, Hurrell DG, etal: Assessment of right atrial pressure with2-dimensional and Doppler echocardiogra-phy: A simultaneous catheterization andechocardiographic study. Mayo Clin Proc2000; 75:24–29
63. Kircher BJ, Himelman RB, Schiller NB:Noninvasive estimation of right atrial pres-sure from the inspiratory collapse of theinferior vena cava. Am J Cardiol 1990; 66:493–496
64. Currie PJ, Seward JB, Chan KL, et al: Con-tinuous wave Doppler determination ofright ventricular pressure: A simultaneousDoppler-catheterization study in 127 pa-tients. J Am Coll Cardiol 1985; 6:750–756
65. Stephen B, Dalal P, Berger M, et al: Nonin-vasive estimation of pulmonary artery dia-stolic pressure in patients with tricuspidregurgitation by Doppler echocardiography.Chest 1999; 116:73–77
66. Lee RT, Lord CP, Plappert T, et al: Prospec-tive Doppler echocardiographic evaluationof pulmonary artery diastolic pressure inthe medical intensive care unit. Am J Car-diol 1989; 64:1366–1370
67. Nagueh SF, Lakkis NM, Middleton KJ, et al:Doppler estimation of left ventricular fillingpressures in patients with hypertrophiccardiomyopathy. Circulation 1999; 99:254–261
68. Nagueh SF, Middleton KJ, Kopelen HA, etal: Doppler tissue imaging: A noninvasivetechnique for evaluation of left ventricu-lar relaxation and estimation of fillingpressures. J Am Coll Cardiol 1997; 30:1527–1533
69. Nagueh SF, Mikati I, Kopelen HA, et al:Doppler estimation of left ventricular fillingpressure in sinus tachycardia. A new appli-cation of tissue doppler imaging. Circula-tion 1998; 98:1644–1650
70. Sun JP, James KB, Yang XS, et al: Compar-ison of mortality rates and progression ofleft ventricular dysfunction in patients with
idiopathic dilated cardiomyopathy and di-lated versus nondilated right ventricularcavities. Am J Cardiol 1997; 80:1583–1587
71. De Groote P, Millaire A, Foucher-Hossein C,et al: Right ventricular ejection fraction isan independent predictor of survival in pa-tients with moderate heart failure. J AmColl Cardiol 1998; 32:948–954
72. Ghio S, Recusani F, Klersy C, et al: Prog-nostic usefulness of the tricuspid annularplane systolic excursion in patients withcongestive heart failure secondary to idio-pathic or ischemic dilated cardiomyopathy.Am J Cardiol 2000; 85:837–842
73. Rihal CS, Nishimura RA, Hatle LK, et al:Systolic and diastolic dysfunction in pa-tients with clinical diagnosis of dilated car-diomyopathy. Relation to symptoms andprognosis. Circulation 1994; 90:2772–2779
74. Temporelli PL, Corra U, Imparto A, et al:Reversible restrictive left ventricular dia-stolic filling with optimized oral therapypredicts a more favorable prognosis in pa-tients with chronic heart failure. J Am CollCardiol 1998; 31:1591–1597
75. Cabell CH, Trichon BH, Velazquez EJ, et al:Importance of echocardiography in patientswith severe nonischemic heart failure: Thesecond prospective randomized amlodipinesurvival evaluation (PRAISE-2) echocardio-graphic study. Am Heart J 2004; 147:151–157
76. Reilly JP, Tunick PA, Timmermans RJ, et al:Contrast echocardiography clarifies unin-terpretable wall motion in intensive careunit patients. J Am Coll Cardiol 2000; 35:485–490
77. Lang RM, Mor-Avi V, Zoghbi WA, et al: Therole of contrast enhancement in echocar-diographic assessment of left ventricularfunction. Am J Cardiol 2002; 90:28J–34J.
78. Senior R, Soman P, Khattar RS, et al: Im-proved endocardial visualization with secondharmonic imaging compared with fundamen-tal two-dimensional echocardiographic imag-ing. Am Heart J 1999; 138:163–168
79. Spencer KT, Bednarz J, Mor-Avi V, et al: Therole of echocardiographic harmonic imag-ing and contrast enhancement for improve-ment of endocardial border delineation.J Am Soc Echocardiogr 2000; 13:131–138
80. Yong Y, Wu D, Fernandes V, et al: Diagnos-tic accuracy and cost-effectiveness of con-trast echocardiography on evaluation ofcardiac function in technically very difficultpatients in the intensive care unit.Am J Cardiol 2002; 89:711–718
81. Schmidlin D, Schuepbach R, Bernard E, etal: Indications and impact of postoperativetransesophageal echocardiography in car-diac surgical patients. Crit Care Med 2001;29:2143–2148
82. Costachescu T, Denault A, Guimond JG, etal: The hemodynamically unstable patientin the intensive care unit: Hemodynamic vs.transesophageal echocardiographic moni-toring. Crit Care Med 2002; 30:1214–1223
83. Colreavy FB, Donovan K, Lee KY, et al:
Transesophageal echocardiography in criti-cally ill patients. Crit Care Med 2002; 30:989–996
84. Heidenreich PA: Transesophageal echocar-diography (TEE) in the critical care patient.Cardiol Clin 2000; 18:789–805
85. Chenzbraun A, Pinto FJ, Schnittger I:Transesophageal echocardiography in theintensive care unit: Impact on diagnosisand decision-making. Clin Cardiol 1994; 17:438–444
86. Bonow RO, Carabello B, de Leon AC Jr, etal: Guidelines for the management of pa-tients with valvular heart disease: Executivesummary; a report of the American Collegeof Cardiology/American Heart AssociationTask Force on Practice Guidelines (Com-mittee on Management of Patients WithValvular Heart Disease). Circulation 1998;98:1949–1984
87. Oh JK, Seward JB, Tajik AJ: The Echo Man-ual. Second Edition. Philadelphia, Lippin-cott-Raven, 1999
88. Shively BK, Gurule FT, Roldan CA, et al:Diagnostic value of transesophageal com-pared with transthoracic echocardiographyin infective endocarditis. J Am Coll Cardiol1991; 18:391–397
89. Karalis DG, Bansal RC, Hauck AJ, et al:Transesophageal echocardiographic recog-nition of subaortic complications in aorticvalve endocarditis: Clinical and surgical im-plications. Circulation 1992; 86:353–336
90. Pearlman AS, Gardin DIM, Martin RP, et al:Guidelines for physician training in trans-esophageal echocardiography: Recommen-dations of the American Society of Echocar-diography Committee for PhysicianTraining in Echocardiography. J Am SocEchocardiogr 1992; 5:187–194
91. Pearson AC, Castello R, Labovitz AJ: Safetyand utility of transesophageal echocardiog-raphy in the critically ill patient. Am Heart J1990; 119:1083–1089
92. Daniel WG, Erbel R, Kasper W, et al: Safetyof transesophageal echocardiography: Amulticenter survey of 10,419 examinations.Circulation 1991; 83:817–821
93. Jenkins C, Bricknell K, Hanekom L, et al:Reproducibility and accuracy of echocardio-graphic measurements of left ventricularparameters using real-time three dimen-sional echocardiography. J Am Coll Cardiol2004; 44:878–886
94. Lee D, Fuisz AR, Fan PH, et al: Real-time3-dimensional echocardiographic evalua-tion of left ventricular volume: Correlationwith magnetic resonance imaging: A valida-tion study. J Am Soc Echocardiogr 2001;14:1001–1009
95. Sugeng L, Weinert L, Lang RM: Left ven-tricular assessment using real time threedimensional echocardiography. Heart 2003;89(Suppl 3):iii29 –iii36
96. Corsi C, Lang RM, Veronesi F, et al: Volu-metric quantification of global and regionalleft ventricular function from real-time
S38 Crit Care Med 2008 Vol. 36, No. 1 (Suppl.)

three-dimensional echocardiographic im-ages. Circulation 2005; 112:1161–1170
97. Jimenez JH, Soerensen DD, He Z, et al:Effects of a saddle shaped annulus on mitralvalve function and chordal force distribu-tion: An in vitro study. Ann Biomed Eng2003; 31:1171–1181
98. Khanna D, Miller AP, Nanda NC, et al:Transthoracic and transesophageal echo-cardiographic assessment of mitral regurgi-tation severity: Usefulness of qualitative andsemiquantitative techniques. Echocardiog-raphy 2005; 22:748–769
99. Quere JP, Tribouilloy C, Enriquez-SaranoM: Vena contracta width measurement:Theoretic basis and usefulness in the assess-ment of valvular regurgitation severity.Curr Cardiol Rep 2003; 5:110–115
100. Delabays A, Jeanrenaud X, Chassot PG, et al:Localization and quantification of mitralvalve prolapse using three-dimensionalechocardiography. Eur J Echocardiogr2004; 5:422–429
101. Macnab A, Jenkins NP, Bridgewater BJ, etal: Three-dimensional echocardiography issuperior to multiplane transoesophagealecho in the assessment of regurgitant mi-tral valve morphology. Eur J Echocardiogr2004; 5:212–222
102. Sugeng L, Spencer KT, Mor-Avi V, et al:Dynamic three-dimensional color flowDoppler: An improved technique for the as-sessment of mitral regurgitation. Echocar-diography 2003; 20:265–273
103. Fabricius AM, Walther T, Falk V, et al:Three-dimensional echocardiography forplanning of mitral valve surgery: Currentapplicability? Ann Thorac Surg 2004; 78:575–578
104. Ryan LP, Salgo IS, Gorman RC, et al: Theemerging role of three-dimensional echo-cardiography in mitral valve repair. SeminThorac Cardiovasc Surg 2006; 18:126–134
105. Valocik G, Kamp O, Visser CA: Three-dimensional echocardiography in mitralvalve disease. Eur J Echocardiogr 2005;6:443–454
106. Perez de Isla L, Casanova C, Almeria C, et al:Which method should be the referencemethod to evaluate the severity of rheu-matic mitral stenosis? Gorlin’s method ver-sus 3D-echo. Eur J Echocardiogr Availableon-line October 11, 2006.
107. Zamorano J, Cordeiro P, Sugeng L, et al:Real-time three-dimensional echocardiog-raphy for rheumatic mitral valve stenosisevaluation: An accurate and novel approach.J Am Coll Cardiol 2004; 43:2091–2096
108. Caiani EG, Coon P, Corsi C, et al: Dualtriggering improves the accuracy of leftventricular volume measurements by con-trast-enhanced real-time 3-dimensionalechocardiography. J Am Soc Echocardiogr2005; 18:1292–1298
109. Corsi C, Coon P, Goonewardena S, et al:Quantification of regional left ventricularfunction from real-time 3D echocardiog-raphy in patients with poor acoustic win-dows: Effects of contrast enhancementtested against cardiac magnetic reso-nance. J Am Soc Echocardiogr 2006; 19:886 – 893
110. Handke M, Heinrichs G, Moser U, et al:Transesophageal real-time three-dimen-sional echocardiography methods and ini-tial in vitro and human in vivo studies. J AmColl Cardiol 2006; 48:2070–2076
111. Goodkin GM, Spevack DM, Tunick PA, et al:How useful is hand-carried bedside echo-cardiography in critically ill patients? J AmColl Cardiol 2001; 37:2019–2022
112. Vignon P, Frank MBJ, Lesage J, et al: Hand-held echocardiography with doppler capa-bility for the assessment of critically ill pa-tients: Is it reliable? Intensive Care Med2004; 30:718–723
113. Manasia AR, Nagaraj HM, Kodali RB, et al:Feasibility and potential clinical utility ofgoal-directed transthoracic echocardiogra-phy performed by noncardiologist intensiv-ists using a small hand-carried device (So-noHeart) in critically ill patients.J Cardiothorac Vasc Anesth 2005; 19:155–159
114. Seward JB, Douglas PS, Raimund E, et al:Handcarried ultrasound (HCU) device: Rec-ommendations regarding new technology.A report from the echocardiography taskforce on new technology of nomenclatureand standards committee of the AmericanSociety of Echocardiography. J Am SocEchocardiogr 2002; 15:369–373
115. DeCara JM, Lang RM, Spencer KT: Thehand-carried echocardiographic device asan aid to the physical examination. Echo-cardiography 2003; 20:477–485
116. Kirkpatrick JN, Furlong K, Mugica VL, et al:Effectiveness of echocardiographic imagingby nurses to identify left ventricular systolicdysfunction in high-risk patients. Am J Car-diol 2005; 95:1271–1272
117. Hellmann DB, Whiting-O’Keefe Q, ShapiroEP, et al: The rate at which residents learnto use hand-held echocardiography at thebedside. Am J Med 2005; 118:1010–1018
118. Schiller NB: Hand-held echocardiography:Revolution or hassle? J Am Coll Cardiol2001; 37:2023–2024
119. Maloney JD, Burnett JM, Dala-Krishna P, etal: New directions in intracardiac echocar-diography. J Interv Card Electrophysiol2005; 13(Suppl 1):23–29
120. Rao HB, Saksena S, Mitruka R, et al. Intra-cardiac echocardiography guided cardiover-sion to help interventional procedures(ICE-CHIP) study: Study design and meth-ods. J Interv Card Electrophysiol 2005;13(Suppl 1):31–36
121. Achilli A, Sassara M, Ficili S, et al: Long-term effectiveness of cardiac resynchroniza-tion therapy in patients with refractoryheart failure and “narrow” QRS. J Am CollCardiol 2003; 42:2117–2124
122. Vanderheyden M, De Backer T, Rivero-Ayerza M, et al: Tailored echocardiographicinterventricular delay programming furtheroptimizes left ventricular performance aftercardiac resynchronization therapy. HeartRhythm 2005; 2:1066–1072
S39Crit Care Med 2008 Vol. 36, No. 1 (Suppl.)