Imaging of the adrenal glands
96
IMAGING OF THE ADRENAL GLANDS
-
Upload
satish-naga -
Category
Health & Medicine
-
view
674 -
download
3
Transcript of Imaging of the adrenal glands

IMAGING OF THE ADRENAL GLANDS

ANATOMY
•Normal size: 2-4 cm CC,smooth limbs without nodularity, max thickness 10 mm.
•Inverted Y, V or L configuration.

Lambda-shaped body and 2 limbs.
Inverted Y-shaped body with 2 limbs that point posteriorly.
Normal CT appearance

NORMAL ADRENALNORMAL ADRENAL
Right – Suprarenal– Posterior to IVC– Lateral to right crus– Medial to right lobe of the liver
Left– Lateral to left crus and aorta– Posterior to pancreas and splenic vessels

II. Imaging characterization of adrenal masses
II. Imaging characterization of adrenal masses

The Hormonally Active Mass
Cortex:• Functional adenomas (Cushing syndrome, Conn
syndrome, or hyperandrogenism).• Carcinomas ( Majority Cushing’s syndrome).
Medulla: • Pheochromocytomas (hypersecretes
cathecolamines)

The Hormonally Active Mass
• The work-up of a suspected hyperfunctioning adrenal mass (pheochromocytoma and aldosteronoma) should start with appropriate biochemical screening tests followed by thin-collimation computed tomography (CT).
• Unilateral mass Conn’s syndrome (aldosterolonoma), Pheochromocytoma.
• Bilateral masses Hyperplasia (Cushing’s diseasePituitary adenoma)

• CT has become the study of choice to differentiate a benign adenoma from a metastasis in the oncology patient.
The oncology patient with an adrenal mass

NCCT
HU < 10
Benign
HU > 10
Delayed CECT (10 min)
Washout > 50%HU < 30
Benign
Washout < 50%HU > 30
Chemical Shift MRI
Signal drop-out
Benign
No signal drop-out
PETBiopsy

Incidentalomas:
Two main concerns exist with incidentalomas:
• The first is whether it is hormonally active, and the second is whether it is malignant.
• The treatment for a hormonally active adrenal tumor is surgery.
• The treatment for a malignancy depends on the cell type, spread, and location of the primary tumor.

From: eMedicine.com, Inc.


Adrenal mass characterization- MRI
• In phase and out of phase gradient echo MR sequences are used to diagnose adrenal adenomas.
• The signal intensity of the adrenal adenoma decreases on out of phase imaging.
• Precession frequencies of protons found in intracellular fat and protons in water cancel out each other's signal at the time the echo is acquired.
• The signal intensity of the adenoma follows that of the of bone marrow, because bone marrow also contains small amounts of adipose tissue.
• The spleen is used as organ of reference on OP images for subjective evaluation.
***Lipid-poor adenomas if an adrenal mass fails to exhibit signal drop out on out of phase imaging it could still be an adenoma.

Adrenal mass characterization
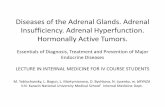
On the chemical shift imaging, signal intensity index, calculated as:
Signal intensity (SI) indexes (D)= [SI in-phase - SI opposed-phase] x 100 (SI in-phase)
A signal intensity index defined as D superior to 25% is used as positive diagnosis criteria for adenoma.

1.5 T
Chemical shift Imaging (CSI)
Schematic shows lipid and water protons precessing in and out of phase with respect to each other over time at 1.5 T. The sine wave depicts the signal intensity within a voxel over time as the water and lipid protons oscillate between in phase and out of phase after the radio-frequency excitation pulse is delivered.

Adrenomedullary tumors :• Pheochromocytoma • Ganglioneuroblastoma • Neuroblastoma • Neuroendocrine
carcinoma
Adrenocortical carcinomas:-Functional
-Nonfunctional -Well differentiated
-Intermediate -Poorly differentiated to
anaplastic
Adrenocortical adenomas:-Functional- Cortisol, aldosterone,androgens-Non-functional
Primary neoplasms

From: eMedicine.com, Inc.

Adenomas
• The prevalence of adrenal adenoma is age related. 0.14%for patients aged 20–29 years and 7% in those older than 70 years
• The majority of lesions are not functioning
• the presence of contralateral adrenal atrophy suggests that a lesion may be functioning, because ACTH secretion is suppressed by elevated cortisol levels

LIPID-RICH ADENOMA
• 70 % are lipid-rich– Clear cells have abundant intracytoplasmic fat
• CT – Low attenuation on nonenhanced CT– Threshold of < 10 HU is 71% sens, 98% spec [1]– Spec approaches 100% when considering other
features (size, shape, stability)– < 30 HU on delayed CECT also diagnostic
[1] Boland et al. AJR 1998; 171:201-4

LIPID-RICH ADENOMA
• MRI– Chemical shift imaging is the most sensitive way to
differentiate adenoma – Relies on the different resonance frequencies of
protons in fat and water molecules– Use spleen as internal standard– Look for signal drop-off (20%) on out-of-phase
images due to intra-voxel signal cancellation of the lipid and water protons
– 81-100% sens, 94-100% spec

LIPID-POOR ADENOMA
• 30% are lipid-poor and do not have low attenuation on CT
• Adenomas enhance rapidly and wash out rapidly (independent of lipid content)
• Reflects physiologic differences in perfusion between adenoma and other lesions

The precontrast attenuation varies according
to the presence or absence of lipid, with
mean attenuation in the range of
−2 to 16 HU in lipid-rich adenomas
20 to 25 HU in lipid-poor adenomas

ADENOMA
-3.0 HU

Adenomas
• Non-functioning adenomas (most common) Incidentalomas.
• Functional adenomas **15%-20% of all Cushing’s syndromes cases are
caused by adenomas or carcinomas .
** 80% of all Conn syndromes cases are caused by small adenomas (the remaining 20% are caused
essentially by adrenal hyperplasia rarely by carcinomas).

ADENOMA
T1W OPT1W IP

ADENOMA
T2W
T1W IP
T1W OP

ADENOMA

The lipid-poor adenoma
• Although representing a minority of adrenal adenomas (30%) the lipid-poor variety cannot be accurately identified on unenhanced CT or chemical shift MR imaging.
• “..lipid-poor adrenal adenomas show enhancement and enhancement washout features nearly identical to lipid-rich adenomas and can be distinguished from nonadenomas on the basis of a percentage washout threshold value of 60% and a relative percentage washout of 40%.”
AJR Am J Roentgenol. 2000 Nov;175(5):1411-5.

Percentage of enhancement washout
[E-D/E-U] x 100 = % ICM washout after 10 min.
E= enhanced attenuation value
U= Unenhanced attn value
D= Delayed enhanced value (15 min)
E= 90 HU
U= 40 HU
D= 50 HU
[90-50/90-40] x 100 = 80% washout

Relative % washout
If unenhanced CT has not been performed:
(E-D) / E x 100
Optimal threshold 40% washout (sens 96%, Spec 100%)
• if threshold used is 50% then sens and spec= 100%

40 HU
114 HU
65 HU
[114-65/114-40] x 100 = 49/74 x 100 = 66% washout (>60 %)
Lipid poor adenoma
AJR:179, September 2002
[E-D/E-U] x 100
U
E
D

32 HU
83 HU
57 HU[83-57/83-32] x 100 = 26/51x 100 = 50% washout (<60 %)
Lung mets
AJR:179, September 2002
U
E
D
[E-D/E-U] x 100

Conn’s disease
Hypertension and hypokalemia
Causes: Adrenal adenoma 80%, adrenal hyperplasia 20%

Adrenal hyperplasia
Truncal obesity and elevated plasma Cortisol
**Hyperplasia- 70%•Cushing’s disease- 90%•Ectopic ACTH- 10%
**Adenoma 20%**Carcinoma 10%
Cushing’s syndrome is caused by:

NCCT
HU < 10
Benign
HU > 10
Delayed CECT (10 min)
Washout > 50%HU < 30
Benign
Washout < 50%HU > 30
Chemical Shift MRI
Signal drop-out
Benign
No signal drop-out
PETBiopsy

METASTASESMETASTASES
Common site for mets Variable appearance
– Any size– Round or lobulated– Homogeneous or inhomogeneous– Calcified– Necrotic
Even in pt with known malignancy, 50% of adrenal masses may be adenomas

METASTASESMETASTASES
Features that favor mets include:– Size > 3 cm– Poorly defined margins– Thick, enhancing rim– Inhomogeneous– Invasion of adjacent structures– Mets elsewhere



METASTASES
Metastatic adrenal tumors - Most common potential primaries include the following:
• Lung • Breast • Melanoma • Renal cell carcinoma • Extra-adrenal lymphoma • Leukemias • Pancreatic carcinoma • Colonic carcinoma • Ovarian carcinoma

METASTASES

METASTASES
[E-D/E-U] x 100
33% washout

METASTASES

METASTASES
PET CT
FDG
FDG

METASTASES
Melanoma
T1W
T2W FS

ADRENAL CARCINOMAADRENAL CARCINOMA
Rare Cortex 10% bilateral 50% functional Usually large at
presentation (4-10 cm)

ADRENAL CARCINOMAADRENAL CARCINOMA
Heterogeneous, irregular contour
Calcification in 30% Large areas of internal
hemorrhage and necrosis in most

ADRENAL CARCINOMAADRENAL CARCINOMA
Look for invasion of adjacent organs and veins

Adrenocortical carcinomas

Adrenocortical carcinomasAdrenocortical carcinomas
Left renal vein

Adrenocortical carcinoma
68-year-old woman with right upper quadrant palpable mass.

Precocious puberty in a child.
Adrenocortical carcinoma

PHEOCHROMOCYTOMAPHEOCHROMOCYTOMA
Neoplasm of chromafin cells in medulla (10% extra adrenal)
Capacity to store and release catecholamines
0.1% of causes of HTN

PheochromocytomaPheochromocytoma
"10-percent rule"
10% bilateral
10% malignant
10% extra-adrenal
associated syndromes:
neurofibromatosis
von-Hippel-Lindau
multiple endrocine neoplasia: MEN-2 and MEN-1
extra-adrenal sites:
detected with MIBG ( I 131-MIBG-NE analog)
Organ of Zuckerkandl (most common)

PHEOCHROMOCYTOMAPHEOCHROMOCYTOMA
Size determines imaging features
< 4 cm– Well defined and
homogeneous
Larger tumors more likely to have central necrosis

PHEOCHROMOCYTOMAPHEOCHROMOCYTOMA
Classically hyperintense on T2
Enhance avidly


Pheochromocytoma

Pheochromocytoma

Pheochromocytoma

Pheochromocytoma
T1W T2W

T1W T2W
T1W POSTGAD
Pheochromocytoma

Paragangliomas
• Extra-adrenal paragangliomas, as the name implies, can occur anywhere along the paraganglionic chain, but are most commonly found in the superior para-aortic region. between the diaphragm and the lower poles of the kidneys.
• Patients often present with headaches, palpitations, sweating, and hypertension.
• Clinical suspicion for extra-adrenal paraganglioma is usually confirmed by elevated urinary catecholamines and their metabolites.


Paraganglioma of the Organ of Zuckerkandl

Von-Hippel-Lindau
VHL- pheochromocytoma, carotid body tumor and islet cell tumor of the pancreas.
T2W

MYELOLIPOMAMYELOLIPOMA
Rare benign tumor (0.2%)Composed of myeloid, erythroid, fat
– Causes heterogeneous appearanceOccasionally calcifyPresence of pure fat on imaging is diagnosticThe primary complication-->retroperitoneal
hemorrhageClinically silent unless very large or
hemorrhage do not undergo malignant transformation

Adrenal myelolipoma

Adrenal myelolipoma

Adrenal myelolipoma

LYMPHOMALYMPHOMA
NHL more commonly than Hodgkin’s– 4% have adrenal involvement
Adrenal infiltration most often occurs with retroperitoneal lymphoma
50% bilateralMass or diffuse enlargement of gland


ADRENAL HEMORRHAGEADRENAL HEMORRHAGE
Causes– Trauma (80%)– Systemic anticoagulant therapy– Sepsis (Waterhouse-Friedrichson syndrome)– Stress– Neoplasm
20% bilateral – Adrenal insufficiency rare

ADRENAL HEMORRHAGEADRENAL HEMORRHAGE
Acute– Round or oval mass, 1-5 cm– Increased attenuation or isodense to liver,
kidney, or muscle on NCCT– Typical signal patterns of blood products on
MRI


Adrenal hemorrhage

ADRENAL HEMORRHAGEADRENAL HEMORRHAGE
Chronic– Will shrink over 6 months– “Ring pattern” on MRI– Pseudocyst– Residual calcification


s/p Adrenal hemorrhage
DDX:
•Neuroblastoma
•TB
•Carcinoma

Granulomatous (TB) disease
• Usually caused by hematogenous spread of systemic infection, resulting in bilateral enlargement and replacement of both the adrenal cortex and medulla by caseous necrosis.
• This may cause adrenal failure by total or near-total destruction of both glands.
• Calcification of the glands can be detected in about half the cases.
• Imaging findings of adrenal tuberculosis are nonspecific and consist often of normal or small size adrenal glands, containing scattered calcifications. Findings are best detected on CT.

Adrenal histoplasmosis

Adrenal histoplasmosis

Adrenal TB

ADRENAL CYSTADRENAL CYST
True cyst (45%)– Epithelial lining– Looks like a simple cyst
Pseudocyst (39%)– Results from old hemorrhage– May see a calcified rim
Parasitic (< 10%)– Echinococcosus



Lung carcinoma necrotic mets
Cysts?
Irregular thick wall

SUMMARY
• Adrenal Embryology , Anatomy and Histology.• Physiology of the Adrenal Gland (endocrine gland).• Clinical importance of adrenal masses characterization.• Imaging Techniques (CT, MRI).• Non-hyperfunctioning Lesions of the Adrenal Cortex
(incidentaloma) and their clinical significance for the oncology patience.
• Hyperfunctioning Lesions of the Adrenal Cortex and endocrinologic clinical presentations.
• Neoplasms of the adrenal cortex.• Neoplasms of the Adrenal Medulla -pheochromocytoma• Metastatic Neoplasms to the Adrenal Glands.
Miscellaneous Conditions of the Adrenals (infection, trauma, cyst)

CT Scan - DDx By appearance:
Diameter less than 2 cm: consider Conn’s syndrome (recommend thinner cuts to better visualize)
Diameter greater than 5 cm: consider carcinoma
Bilateral: consider metastasis, infection, hyperplasia
Calcifications: consider pheochromocytoma, carcinoma, cyst (peripheral), infection, myelolipoma, hemangioma, ganglioneuroma
Heterogeneous appearance: consider adenoma, myelolipoma, hemangioma
Central area of necrosis: consider pheochromocytoma, carcinoma, granulomatous infection
Nodularity:, metastasis

By Attenuation:
-115 to -30 HU: consider myelolipoma (lower than adenoma)
Less than 10 HU: consider adenoma
50 to 90 HU: consider acute to subacute hematoma

By enhancement and contrast washout characteristics
• If the attenuation of the adrenal gland is over 10 HU on nonenhanced CT, contrast material–enhanced CT should be performed and washout calculated.
• Over 50%-60% washout of contrast material on a 15-minute delayed CT scan is diagnostic of an adenoma.

thanku

• Fat-containing adrenal masses can be classified into two main types: those that contain intracellularfat (eg, adenoma) and those with macroscopicfat (eg, myelolipoma). Adrenal masses that contain intracellular fat have been shown to lose signal intensity on chemical shift out-of-phase images compared with in-phase images owing to the presence of intracellular lipid. Adrenal lesions that contain macroscopic fat demonstrate a loss of signal intensity on fat-saturated images.

For patients in whom a pheochromocytoma issuspected and an adrenal mass is not identified atCT or MR imaging, nuclear medicine imagingcan be used. I-131 MIBG and In-111 octreotideare the two radiopharmaceuticals used to evaluatefor a pheochromocytoma. I-131 MIBG is a structuralanalog of norepinephrine, which is stored inneurosecretory granules of the adrenal medulla.Abdominal imaging is performed 24–72 hoursafter administration of the agent, and whole-bodyimaging should be performed to detect extraadrenallesions. If there is a high clinical suspicion of aperivesicular paraganglioma, bladder catheterizationmay be necessary as the agent is excretedin the urine. When pheochromocytoma is suspected,

any focal uptake of I-131 MIBG in theadrenal gland is abnormal (Fig 6). The reportedsensitivity of I-131 MIBG for detection of a pheochromocytomais 80%–90%, with a specificity of90%–100% (7–9). I-131 MIBG scintigraphy isuseful to detect the 10% of pheochromocytomasthat are extraadrenal and to document metastaticdisease or residual tumor after surgery.In-111 octreotide, the second agent used todetect pheochromocytomas, is a synthetic octapeptideanalog of somatostatin that shows uptakein a variety of tumors that contain somatostatinreceptors. A total of 5 mCi (185 MBq) ofIn-111 octreotide is administered intravenously,and whole-body imaging is performed at 4 and 24hours after injection. In-111 octreotide has a sensitivityof 75%–90% for detection of pheochro

There is a complementary rolefor In-111 octreotide and I-131 MIBG, since25% of pheochromocytomas are seen only withI-131 MIBG and another 25% are seen only withIn-111 octreotide. The remaining 50% of pheochromocytomasare visualized with both agents